
Systemic and Local Medical or Surgical Therapies for Ear, Nose and/or Throat Manifestations in ANCA-Associated Vasculitis: A Systematic Literature Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Interventions and Outcomes
2.3. Data-Extraction and Critical Appraisal
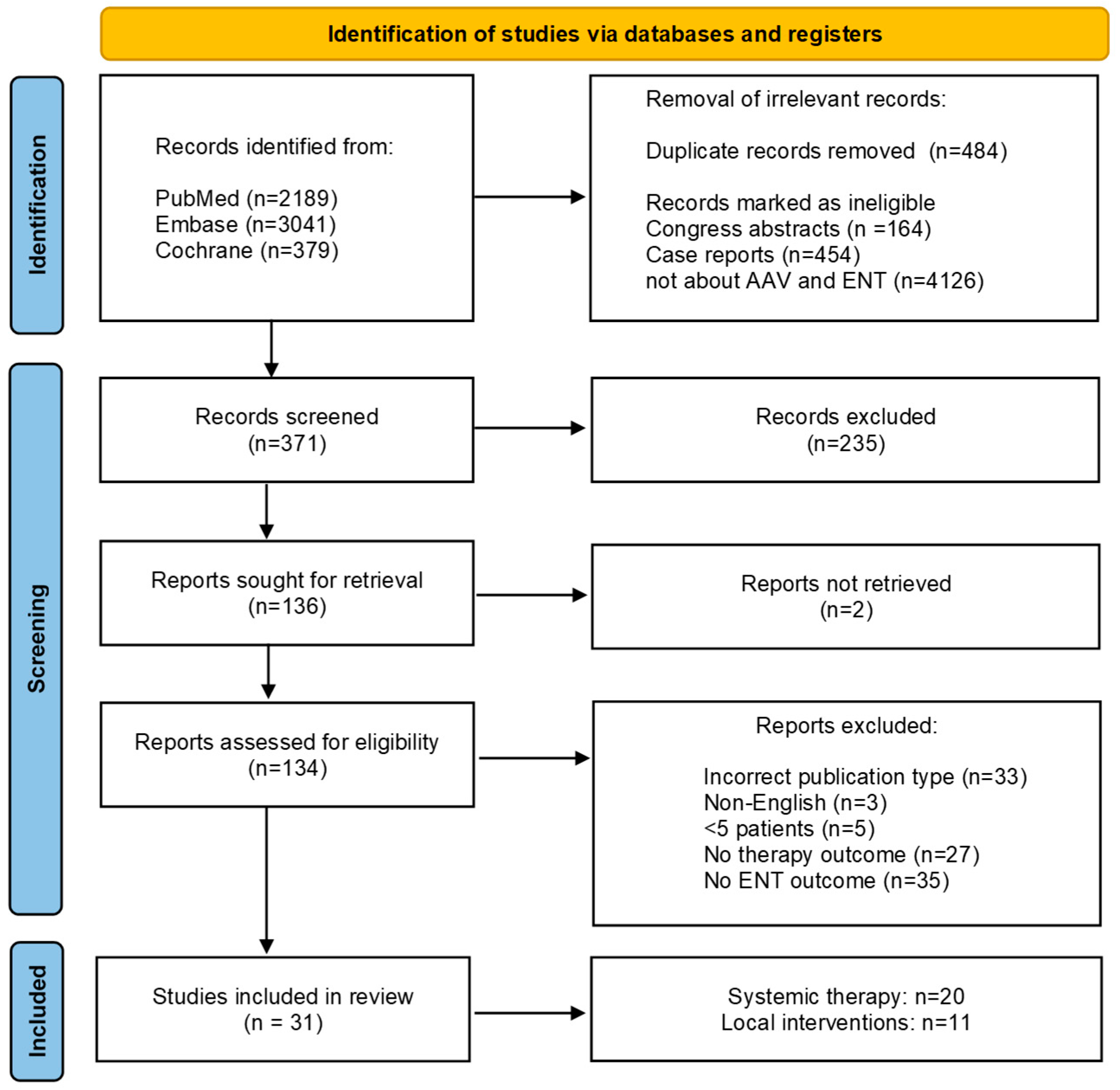
3. Results
3.1. Treatment of Sinonasal Manifestations
3.2. Treatment of Subglottic Manifestations
3.3. Treatment of Otitis and Inner Ear Dysfunction
3.4. Treatment of Non-Specified ENT Manifestations

{kind=link}
| First Author Country | Publication Year | Intervention | Study Design | N of Patients Total/ENT Intervention/ENT Control | AAV Type | Follow-Up | Results | LoE h | Validity h | |
|---|---|---|---|---|---|---|---|---|---|---|
| ENT Disease Activity | ENT Relapse | |||||||||
| Systemic therapy | ||||||||||
| Wechsler [14] International (9 countries) | 2017 | Intervention: MEPO + GC +/− csDMARDs a Control: Placebo + GC +/− csDMARD a | randomized, placebo-controlled, double-blind, parallel-group, phase 3 trial | Total: 151 Intervention: 64 Control: 64 | EGPA | All included pt 60 w | n/r | Relapse Intervention: 35% (n = 24) Control: 51% | 1b | + |
| Rios-Garces [31] Spain | 2021 | Intervention: MEPO + GC +/− csDMARDs b Control: none | Retrospective cohort | Total: 56 Intervention: 11 Control: none | EGPA | Median 3.19 y (3 m–5.6 y) | Response: Nasal polyps 50% (n = 4), Rhinitis 33% (n = 1), Paranasal sinus involvement 33% (n = 1) | n/r | 4 | + |
| Tsurikisawa [32] Japan | 2021 | Intervention: MEPO + GC +/− csDMARDs c Control: none | Retrospective cohort | Total: 59 Intervention: 9 Control: none | EGPA | n/r | Response in 100% of patients (n = 9) | n/r | 4 | − |
| Detoraki [30] Italy | 2021 | Intervention: MEPO + GC d Control: none | Prospective cohort | Total: 8 Intervention: 8 Control: none | EGPA | All included pt 12 m | Decrease mean SNOT-22 49 (t = 0) to 22 (t = 12 m), decrease in mean TENPS 3.4 (t = 0) to 0.8 (t = 12 m) | n/r | 4 | − |
| Holle [18] Germany | 2012 | Intervention: RTX + GC +/− CYC e Control: none | Retrospective cohort | Total: 59 Intervention: 3 Control: none | GPA | Median 7 m (4–58 m) | Response 67% (n = 2) | n/r | 4 | +/− |
| Low [19] United States | 2020 | Intervention: csDMARDs + GCf Control: none | Retrospective cohort | Total: 44 Intervention: 44 Control: none | EGPA | Mean 4.54 y (SD 4.98) | Remission 21% (n = 9), response 32% (n = 14), no response 21% (n = 9) | n/r | 4 | +/− |
| Bacciu [12] Italy | 2008 | Intervention: GC + intranasal GC +/− csDMARDs g Control: none | Retrospective case series | Total: 29 Intervention: 17 Control: none | EGPA | Mean 43 m (12 m–74 m) | Remission 82.3% (n = 14), improvement of symptoms 100% (n = 17) | n/r | 4 | + |
| First Author Country | Publication Year | Intervention | Study Design | N of Patients Total/ENT Intervention/ENT Control | AAV Type | Follow-Up | Results | LoE h | Validity h | |
|---|---|---|---|---|---|---|---|---|---|---|
| ENT Disease Activity | ENT Relapse | |||||||||
| Systemic therapy | ||||||||||
| Holle [18] Germany | 2012 | Intervention: RTX + GC +/− CYC a Control: none | Retrospective cohort | Total: 59 Intervention: 8 Control: none | GPA | Median 7 m (4–58 m) | complete remission 37.5% (n = 3) response 50% (n = 4) refractory 12.5% (n = 1) | n/r | 4 | +/− |
| Local interventions (in combination with systemic therapy) | ||||||||||
| Zammit [33] United Kingdom | 2021 | Intervention: dilatation + GC + i.v. CYC or RTX b Control: none | Retrospective cohort | Total: 20 Intervention:20 Control: none | GPA | Mean 61.2 m (15.7–201.5 m) | Remission 90% (n = 18) | Relapse 10% (n = 2) | 4 | +/− |
| Schokkenbroek [34] Netherlands | 2008 | Intervention: dilatation c Control: none | Retrospective cohort | Total:25 Intervention:9 Control: none | GPA | Mean 25.4 m +/− 41.1 m | n/r | 77.8% (n = 7) | 4 | − |
| Taylor [35] United States | 2013 | Intervention: dilatation +/− local/intralesional GC +/− csDMARD d Control: none | Retrospective cohort | Total: 39 Intervention: 15 Control: none | GPA | Mean 8.2 y, median 9.9 y | n/r | Mean n of procedures/pt 3.53 | 4 | − |
| Wolter [36] Canada | 2010 | Intervention: Dilatation + intralesional GC c Control: none | Retrospective cohort | Total: 12 Intervention: 8 Control: none | GPA | n/r | n/r | Mean n of procedures/pt 3.37, mean symptom control 11.9 months | 4 | − |
| Fijolek [37] Poland | 2016 | Intervention: Dilatation + intralesional GC +/− systemic GC and csDMARD e Control: none | Retrospective cohort | Total: 250 Intervention: 34 Control: none | GPA | Median 7 y (2 w–20 y) | 88.2% (n = 30) response to treatment | Median n of procedures/pt 1, median response interval 34 months Relapse in pt with systemic treatment in 32% (n = 11) | 4 | +/− |
| Nouraei [38] United Kingdom | 2008 | Intervention ± Dilatation + intralesional GC + laser surgery c Control: none | Retrospective cohort | Total: 18 Intervention: 18 Control: none | GPA | 5–38 m | n/r | Median n of procedures/pt 1, mean intervention-free interval 26.1 months | 4 | +/− |
| Carnevale [39] Spain | 2019 | Intervention: Dilatation + laser surgery c Control: none | Retrospective case series | Total: 19 Intervention: 5 Control: none | GPA | n/r | 80.0% (n = 4) response to treatment | n/r | 4 | − |
| Costantino [40] United States | 2018 | Intervention: laryngotracheal resection + reconstruction +/− GC +/− csDMARD/biological f Control: none | Retrospective case series | Total:11 Intervention: 11 Control: none | GPA | Median 10.9 y (4 m–28 y) | 91% (n = 10) response to treatment | 55% (n = 6) required additional local treatment | 4 | +/− |
| Arebro [42] Sweden | 2012 | Intervention: micro larynx surgery c Control: none | Retrospective case series | Total: 13 Intervention: 13 Control: none | GPA | Mean 3.5 y, 1.5 y–6.5 y | 100% (n = 13) response to treatment, 85% (n = 11) higher QoL | 38.5% (n = 5) relapsed | 4 | − |
| Solans-Laque [41] Spain | 2008 | Intervention: Surgery or dilatation + intralesional GC +/− systemic GC +/− csDMARD g Control: none | Retrospective case series | Total: 51 Intervention: 6 Control: none | GPA | Mean 71.3 m, 12 m–180 m | n/r | 83.3% (n = 5) relapsed | 4 | − |
| Chen [43] United States | 2020 | Intervention: dilatation + biological or csDMARD Control: dilatation + different csDMARDs | Retrospective cohort | Total: 39 Intervention: 18 Control: 21 | GPA | n/r | Median dilatation interval RTX maintenance (n = 3) 153 d vs 80 d in non-RTX, MTX (n = 7) 259 d vs. 174 d in non-MTX, AZA (n = 4) 177 d vs. 394 d in non-AZA, LEF (n = 4) 484 d vs. 155 d in non-LEF | n/r | 4 | − |
| First Author Country | Publication Year | Systemic Therapy | Study Design | N of Patients Total/ENT Intervention/ENT Control | AAV Type | Follow- Up | Results | LoE g | Validity g | |
|---|---|---|---|---|---|---|---|---|---|---|
| ENT Disease Activity | ENT Relapse | |||||||||
| Otitis media/Hearing loss | ||||||||||
| Okada [16] Japan | 2019 | Intervention: RTX + GC a Control: GC +/− i.v. CYC, AZA a | Retrospective cohort | Total: n = 23 Intervention: n = 6 Control: n = 17 | AAV | n/r | Response, mean hearing gain AC/BC Intervention: 100%, 22 dB /11 dB Control: 100%, 21 dB / 10 dB | n/r | 2b | +/− |
| Harabuchi [17] Japan | 2017 | Intervention: csDMARDs + GC b Control: GC b | Retrospective cohort | Total: n = 235 Intervention: n = 122 Control: n = 101 | AAV | Median 24 m (Q25–75: 11 m–72 m) | Hearing improvement rate Intervention: 68% Control: 56% | Relapse Intervention: 36% (n = 45) Control: 47% (n = 47) | 4 | − |
| Yoshida [25] Japan | 2014 | Intervention: CYC + GC c Control: none | Retrospective case series | Total: n= 8 Intervention n = 8 Control: none | AAV | 12 m–96 m | Hearing improvement Intervention: 81% (n = 16) ears | Relapse Intervention: 0% (n = 0) | 4 | +/− |
| Sahyouni [13] United States | 2019 | Intervention: MTX + GC + aTNF d Control: none | Retrospective case series | Total: n= 11 Intervention: n = 11 Control: none | GPA | n/r | improvement of otologic symptoms Intervention: 100% (n = 11) | n/r | 4 | − |
| Tsurikisawa [32] Japan | 2021 | Intervention: MEPO + GC +/− csDMARDs e Control: none | Retrospective cohort | Total: n = 59 Intervention: n = 6 Control: none | EGPA | n/r | Response in 83% (n = 5) | n/r | 4 | − |
| Vestibular symptoms | ||||||||||
| Morita [24] Japan | 2017 | Intervention: i.v. CYC + GC f Control: GC f | Retrospective cohort | Total: n = 31 Intervention: n = 3 Control: n = 7 | AAV | Median 26 m (1 m–127 m) | Response Intervention: 100% (n = 3) Control: 57.1% (n = 4) | n/r | 4 | +/− |
| First Author Country | Publication Year | Systemic Therapy | Study Design | N of Patients Total/ENT Intervention/ENT Control | AAV Type | Follow-Up | Results | LoE i | Validity i | |
|---|---|---|---|---|---|---|---|---|---|---|
| ENT Disease Activity | ENT Relapse | |||||||||
| Lally [11] United States | 2014 | Intervention: RTX +/− GC a Control: csDMARDs +/− GC a | Retrospective cohort | Total: 99 Intervention: 51 Control: 48 | GPA | n/r | Absence of ENT activity during % of observational period Intervention: 92.4%, Control: 53.7% More absence of ENT activity in intervention group OR 12.0, p < 0.001 | n/r | 2b | +/− |
| Eriksson [20] Sweden | 2005 | Intervention: RTX + GC +/− csDMARDs b Control: none | Retrospective case series | Total: 9 Intervention: 7 Control: none | AAV | 6 m–25 m | remission 86% (n = 6), partial remission 14% (n = 1), drop in daily GC dose | 28% (n = 2) | 4 | + |
| Malm [21] United States | 2014 | Intervention: RTX + GC c Control: none | Retrospective case series | Total: 11 Intervention: 11 Control: none | GPA | Mean 23.5 m (6 m–48 m) | drop in daily GC dose | n/r | 4 | +/− |
| Teixeira [22] United Kingdom | 2019 | Intervention: RTX + GC d Control: none | Retrospective cohort | Total: 69 Intervention: 61 Control: none | EGPA | In all pt 24 m | n/r | 17.4% (n = 12) | 4 | + |
| Bettiol [45] International (8 countries) | 2021 | Intervention: MEPO 100 mg/4 w + standard care e Control: MEPO 300 mg/4 w + standard care e | Retrospective cohort | Total: 203 Intervention: 121 Control: 17 | EGPA | 3 m–24 m | Intervention: ENT involvement decreased from 76.6% to 20.5% at 24 m Control: ENT involvement decreased from 51.5% to 27.6% at 12 m | Intervention: 15.8% (n = 25) Control: 12.2% (n = 4) | 2b | +/− |
| Ueno [46] Japan | 2021 | Intervention: MEPO 300 mg/4 w + standard care f Control: none | Retrospective cohort | Total: 16 Intervention: 6 Control: none | EGPA | In all pt 12 m | Response 50% (n = 3) | n/r | 4 | + |
| Knopf [15] Germany | 2015 | Intervention: GC +/− csDMARDs g Control: none | Retrospective case series | Total: 28 Intervention: 21 Control: none | GPA | Mean 38 m (8 m–56 m) | Remission 95% (n = 20) | n/r | 4 | − |
| Yilmaz [23] Turkey | 2017 | Intervention: GC +/− csDMARDs h Control: none | Retrospective case series | Total: 15 Intervention: 15 Control: none | EGPA | Mean 1.7 y (0.5 y–2 y) | Remission 100% (n = 15) | n/r | 4 | − |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lazarus, B.; John, G.T.; O’callaghan, C.; Ranganathan, D. Recent advances in anti-neutrophil cytoplasmic antibody-associated vasculitis. Indian J. Nephrol. 2016, 26, 86–96. [Google Scholar] [CrossRef]
- Felicetti, M.; Cazzador, D.; Padoan, R.; Pendolino, A.L.; Faccioli, C.; Nardello, E.; Berti, A.; Silvestrini, M.; Paolazzi, G.; Brunori, G.; et al. Ear, nose and throat involvement in granulomatosis with polyangiitis: How it presents and how it determines disease severity and long-term outcomes. Clin. Rheumatol. 2018, 37, 1075–1083. [Google Scholar] [CrossRef]
- Solans-Laque, R.; Fraile, G.; Rodriguez-Carballeira, M.; Caminal, L.; Castillo, M.J.; Martinez-Valle, F.; Bosch, J.A. Clinical characteristics and outcome of Spanish patients with ANCA-associated vasculitides: Impact of the vasculitis type, ANCA specificity, and treatment on mortality and morbidity. Medicine 2017, 96, e6083. [Google Scholar] [CrossRef]
- Del Pero, M.M.; Chaudhry, A.; Rasmussen, N.; Jani, P.; Jayne, D. A disease activity score for ENT involvement in granulomatosis with polyangiitis (Wegener’s). Laryngoscope 2013, 123, 622–628. [Google Scholar] [CrossRef]
- Kitching, A.R.; Anders, H.-J.; Basu, N.; Brouwer, E.; Gordon, J.; Jayne, D.R.; Kain, R. ANCA-associated vasculitis. Nat. Rev. Dis. Prim. 2020, 6, 71. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J. Small-vessel vasculitis. N. Engl. J. Med. 1997, 337, 1512–1523. [Google Scholar] [CrossRef]
- Sharma, A.; Lakshman, A.; Nampoothiri, R.V.; Verma, R.; Rathi, M.; Naidu, G.; Pinto, B.; Sharma, K.; Dhir, V.; Nada, R.; et al. Pulmonary and Ear, Nose and Throat (ENT) Involvement in ANCA-Associated Vasculitis at Diagnosis-Experience from a Tertiary Care Centre in North India. J. Assoc. Phys. India 2017, 65, 40–47. [Google Scholar]
- Seo, P.; Min, Y.-I.; Holbrook, J.T.; Hoffman, G.S.; Merkel, P.A.; Spiera, R.; Davis, J.C.; Ytterberg, S.R.; Clair, E.W.S.; McCune, W.J.; et al. Damage caused by Wegener’s granulomatosis and its treatment: Prospective data from the Wegener’s Granulomatosis Etanercept Trial (WGET). Arthritis Rheum. 2005, 52, 2168–2178. [Google Scholar] [CrossRef]
- Yates, M.; Watts, R.A.; Bajema, I.M.; Cid, M.C.; Crestani, B.; Hauser, T.; Mukhtyar, C. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann. Rheum. Dis. 2016, 75, 1583–1594. [Google Scholar] [CrossRef]
- Dirikgil, E.; Tas, S.W.; Rutgers, A.; Verhoeven, P.M.J.; Van Laar, J.M.; Hagen, E.C.; Tekstra, J.; Hak, A.E.L.; Van Paassen, P.; Kok, M.; et al. A Dutch consensus statement on the diagnosis and treatment of ANCA-associated vasculitis. Neth. J. Med. 2020, 78, 71–82. [Google Scholar]
- Lally, L.; Lebovics, R.S.; Huang, W.-T.; Spiera, R.F. Effectiveness of rituximab for the otolaryngologic manifestations of granulomatosis with polyangiitis (Wegener’s). Arthritis Care Res. 2014, 66, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Bacciu, A.; Buzio, C.; Giordano, D.; Pasanisi, E.; Vincenti, V.; Mercante, G.; Grasselli, C.; Bacciu, S. Nasal Polyposis in Churg-Strauss Syndrome. Laryngoscope 2008, 118, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Sahyouni, R.; Moshtaghi, O.; Abouzari, M.; Le, P.; Birkenbeuel, J.; Cheung, D.; Lin, H.W.; Djalilian, H.R. A Case Series of Granulomatosis with Polyangiitis Primarily Diagnosed by Otological Manifestations. Ann. Otol. Rhinol. Laryngol. 2019, 128, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, M.E.; Akuthota, P.; Jayne, D.; Khoury, P.; Klion, A.; Langford, C.A.; Merkel, P.A.; Moosig, F.; Specks, U.; Cid, M.C.; et al. Mepolizumab or Placebo for Eosinophilic Granulomatosis with Polyangiitis. N. Engl. J. Med. 2017, 376, 1921–1932. [Google Scholar] [CrossRef] [PubMed]
- Knopf, A.; Chaker, A.; Stark, T.; Hofauer, B.; Lahmer, T.; Thürmel, K.; Bas, M. Clinical aspects of granulomatosis with polyangiitis affecting the head and neck. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 185–193. [Google Scholar] [CrossRef]
- Okada, M.; Suemori, K.; Takagi, D.; Teraoka, M.; Yamada, H.; Ishizaki, J.; Hato, N. The treatment outcomes of rituximab for intractable otitis media with ANCA-associated vasculitis. Auris Nasus Larynx 2019, 46, 38–42. [Google Scholar] [CrossRef]
- Harabuchi, Y.; Kishibe, K.; Tateyama, K.; Morita, Y.; Yoshida, N.; Kunimoto, Y.; Matsui, T.; Sakaguchi, H.; Okada, M.; Watanabe, T.; et al. Clinical features and treatment outcomes of otitis media with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (OMAAV): A retrospective analysis of 235 patients from a nationwide survey in Japan. Mod. Rheumatol. 2017, 27, 87–94. [Google Scholar] [CrossRef]
- Holle, J.U.; Dubrau, C.; Herlyn, K.; Heller, M.; Ambrosch, P.; Noelle, B.; Reinhold-Keller, E.; Gross, W.L. Rituximab for refractory granulomatosis with polyangiitis (Wegener’s granulomatosis): Comparison of efficacy in granulomatous versus vasculitic manifestations. Ann. Rheum. Dis. 2012, 71, 327–333. [Google Scholar] [CrossRef]
- Low, C.M.; Keogh, K.A.; Saba, E.S.; Gruszczynski, N.R.; Berti, A.; Specks, U.; Baqir, M.; Smith, B.M.; Choby, G.; Stokken, J.K.; et al. Chronic rhinosinusitis in eosinophilic granulomatosis with polyangiitis: Clinical presentation and antineutrophil cytoplasmic antibodies. Int. Forum Allergy Rhinol. 2020, 10, 217–222. [Google Scholar] [CrossRef]
- Eriksson, P. Nine patients with anti-neutrophil cytoplasmic antibody-positive vasculitis successfully treated with rituximab. J. Intern. Med. 2005, 257, 540–548. [Google Scholar] [CrossRef]
- Malm, I.-J.; Mener, D.J.; Kim, J.; Seo, P.; Kim, Y.J. Otolaryngological Progression of Granulomatosis with Polyangiitis after Systemic Treatment with Rituximab. Otolaryngol. Head Neck Surg. 2014, 150, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, V.; Mohammad, A.J.; Jones, R.B.; Smith, R.; Jayne, D. Efficacy and safety of rituximab in the treatment of eosinophilic granulomatosis with polyangiitis. RMD Open. 2019, 5, e000905. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, I.; Tutar, N.; Simsek, Z.O.; Oymak, F.S.; Gulmez, I.; Yılmaz, I. Clinical and Serological Features of Eosinophilic and Vasculitic Phases of Eosinophilic Granulomatosis with Poliangiitis: A Case Series of 15 Patients. Turk. Thorac. J. 2017, 18, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Morita, Y.; Takahashi, K.; Izumi, S.; Kubota, Y.; Ohshima, S.; Horii, A. Vestibular Involvement in Patients with Otitis Media with Antineutrophil Cytoplasmic Antibody-associated Vasculitis. Otol. Neurotol. 2017, 38, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Hara, M.; Hasegawa, M.; Matsuzawa, S.; Shinnabe, A.; Kanazawa, H.; Iino, Y. Reversible Cochlear Function with ANCA-Associated Vasculitis Initially Diagnosed by Otologic Symptoms. Otol. Neurotol. 2014, 35, 114–120. [Google Scholar] [CrossRef]
- Exley, A.; Bacon, P.A.; Luqmani, R.; Kitas, G.; Gordon, C.; Savage, C.O.S.; Adu, D. Development and initial validation of the vasculitis damage index for the standardized clinical assessment of damage in the systemic vasculitides. Arthritis Rheum. 1997, 40, 371–380. [Google Scholar] [CrossRef]
- Offringa, M.; Assendelft, W.J.J.; Scholten, R.J.P.M. Inleiding in Evidence-Based Medicine; Bohn Stafleu van Lochem: Houten, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Philips, B.; Ball, C.; Sackett, D.; Badenoch, D.; Straus, S.; Haynes, B.; Howick, J. Last Updated by Howick J. Oxford Centre for Evidence-Based Medicine–Levels of Evidence (March 2009). 2021. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 (accessed on 1 March 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Detoraki, A.; Tremante, E.; Poto, R.; Morelli, E.; Quaremba, G.; Granata, F.; Romano, A.; Mormile, I.; Rossi, F.W.; de Paulis, A.; et al. Real-life evidence of low-dose mepolizumab efficacy in EGPA: A case series. Respir. Res. 2021, 22, 185. [Google Scholar] [CrossRef]
- Ríos-Garcés, R.; Prieto-González, S.; Hernández-Rodríguez, J.; Arismendi, E.; Alobid, I.; Penatti, A.E.; Cid, M.C.; Espígol-Frigolé, G. Response to mepolizumab according to disease manifestations in patients with eosinophilic granulomatosis with polyangiitis. Eur. J. Intern. Med. 2022, 95, 61–66. [Google Scholar] [CrossRef]
- Tsurikisawa, N.; Oshikata, C.; Watanabe, M.; Fukuda, N.; Yamaguchi, T.; Kiyohara, H.; Kaneko, T. Clinical Features of Patients with Active Eosinophilic Granulomatosis with Polyangiitis Successfully Treated with Mepolizumab. Int. Arch. Allergy Immunol. 2021, 182, 744–756. [Google Scholar] [CrossRef]
- Zammit, M.; Dhunnoo, V.; Kinshuck, A.; Hardy, S.; Harper, J.; Panarese, A.; Webb, C. The Liverpool Experience: The Role of Immunosuppression in treating Vasculitic Subglottic Stenosis. Clin. Otolaryngol. 2021, 47, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Schokkenbroek, A.A.; Franssen, C.F.M.; Dikkers, F.G. Dilatation tracheoscopy for laryngeal and tracheal stenosis in patients with Wegener’s granulomatosis. Eur. Arch. Oto-Rhino-Laryngol. 2008, 265, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.C.; Clayburgh, D.R.; Rosenbaum, J.T.; Schindler, J.S. Clinical Manifestations and Treatment of Idiopathic and Wegener Granulomatosis–Associated Subglottic Stenosis. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Wolter, N.E.; Ooi, E.H.; Witterick, I.J. Intralesional corticosteroid injection and dilatation provides effective management of subglottic stenosis in Wegener’s granulomatosis. Laryngoscope 2010, 120, 2452–2455. [Google Scholar] [CrossRef]
- Fijolek, J.; Wiatr, E.; Gawryluk, D.; Martusewicz-Boros, M.M.; Orlowski, T.M.; Dziedzic, D.; Polubiec-Kownacka, M.; Oniszh, K.; Langfort, R.; Roszkowski-Sliz, K. Intratracheal Dilation-injection Technique in the Treatment of Granulomatosis with Polyangiitis Patients with Subglottic Stenosis. J. Rheumatol. 2016, 43, 2042–2048. [Google Scholar] [CrossRef]
- Nouraei, S.A.R.; Obholzer, R.; Ind, P.W.; Salama, A.D.; Pusey, C.D.; Porter, F.; Sandhu, G.S. Results of endoscopic surgery and intralesional steroid therapy for airway compromise due to tracheobronchial Wegener’s granulomatosis. Thorax 2008, 63, 49–52. [Google Scholar] [CrossRef]
- Carnevale, C.; Arancibia-Tagle, D.; Sarría-Echegaray, P.; Til-Pérez, G.; Tomás-Barberán, M. Head and Neck Manifestations of Granulomatosis with Polyangiitis: A Retrospective analysis of 19 Patients and Review of the Literature. Int. Arch. Otorhinolaryngol. 2019, 23, 165–171. [Google Scholar] [CrossRef]
- Costantino, C.L.; Niles, J.L.; Wright, C.D.; Mathisen, D.J.; Muniappan, A. Subglottic Stenosis in Granulomatosis with Polyangiitis: The Role of Laryngotracheal Resection. Ann. Thorac. Surg. 2018, 105, 249–253. [Google Scholar] [CrossRef]
- Solans-Laqué, R.; Bosch-Gil, J.; Canela, M.; Lorente, J.; Pallisa, E.; Vilardell-Tarrés, M. Clinical features and therapeutic management of subglottic stenosis in patients with Wegener’s granulomatosis. Lupus 2008, 17, 832–836. [Google Scholar] [CrossRef]
- Arebro, J.; Henriksson, G.; Macchiarini, P.; Juto, J.-E. New treatment of subglottic stenosis due to Wegener’s granulomatosis. Acta Oto-Laryngol. 2012, 132, 995–1001. [Google Scholar] [CrossRef]
- Chen, L.W.; Lina, I.; Motz, K.; Berges, A.J.; Ospino, R.; Seo, P.; Hillel, A.T. Factors Affecting Dilation Interval in Patients with Granulomatosis with Polyangiitis-Associated Subglottic and Glottic Stenosis. Otolaryngol. Neck Surg. 2021, 165, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Iino, Y. Pathogenesis and Diagnosis of Otitis Media with ANCA-Associated Vasculitis. Allergol. Int. 2014, 63, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Bettiol, A.; Urban, M.L.; Dagna, L.; Cottin, V.; Franceschini, F.; Del Giacco, S.; Schiavon, F.; Neumann, T.; Lopalco, G.; Novikov, P.; et al. Mepolizumab for Eosinophilic Granulomatosis with Polyangiitis: A European Multicenter Observational Study. Arthritis Rheumatol. 2022, 74, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Miyagawa, I.; Nakano, K.; Iwata, S.; Hanami, K.; Fukuyo, S.; Kubo, S.; Miyazaki, Y.; Kawabe, A.; Yoshinari, H.; et al. Effectiveness and Safety of Mepolizumab in Combination with Corticosteroids in Patients with Eosinophilic Granulomatosis with Polyangiitis. Arthritis Res. Ther. 2021, 23, 86. [Google Scholar] [CrossRef] [PubMed]
- Harabuchi, Y.; Kishibe, K.; Tateyama, K.; Morita, Y.; Yoshida, N.; Okada, M.; Kunimoto, Y.; Watanabe, T.; Inagaki, A.; Yoshida, T.; et al. Clinical characteristics, the diagnostic criteria and management recommendation of otitis media with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (OMAAV) proposed by Japan Otological Society. Auris Nasus Larynx 2021, 48, 2–14. [Google Scholar] [CrossRef]
- Robson, J.C.; Dawson, J.; Doll, H.; Cronholm, P.F.; Milman, N.; Kellom, K.; Ashdown, S.; Easley, E.; Gebhart, D.; Lanier, G.; et al. Validation of the ANCA-associated vasculitis patient-reported outcomes (AAV-PRO) questionnaire. Ann. Rheum. Dis. 2018, 77, 1157–1164. [Google Scholar] [CrossRef]
- Chung, S.A.; Langford, C.A.; Maz, M.; Abril, A.; Gorelik, M.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. 2021 American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Antineutrophil Cytoplasmic Antibody-Associated Vasculitis. Arthritis Rheumatol. 2021, 73, 1366–1383. [Google Scholar] [CrossRef]
- Stegeman, C.A.; Tervaert, J.W.; de Jong, P.E.; Kallenberg, C.G. Trimethoprim-sulfamethoxazole (co-trimoxazole) for the prevention of relapses of Wegener’s granulomatosis. Dutch Co-Trimoxazole Wegener Study Group. N. Engl. J. Med. 1996, 335, 16–20. [Google Scholar] [CrossRef]

| Sinonasal manifestations | Local therapy | No information available |
| Systemic therapy | Varying results in patients treated with GC in combination with a csDMARD (remission 21–82%) and patients treated with GC in combination with MEPO (relapse 35%, response in 33–100%) | |
| Subglottic manifestations | Local therapy | Response of 80–100% in patients treated with dilatation therapy, intralesional GC, surgery or a combination of these therapies. Relapses were seen in 38–83% of patients with mean N of procedures per patient up to 3.5 |
| Systemic therapy | One study reporting complete remission in 38% of patients treated with GC and RTX | |
| Otitis and inner ear dysfunction | Local therapy | No information available |
| Systemic therapy | Hearing improvement in 68–100% of patients treated with csDMARDs combined with GC compared to 56–57% in patients treated with GC alone. Hearing gain in 100% of patients treated with GC in combination with either RTX or csDMARDs. Response in 83% of patients treated with MEPO in combination with GC with or without csDMARDs | |
| ENT manifestations not specified | Local therapy | No information available |
| Systemic therapy | Response in 86–100% of patients treated with csDMARDs and glucocorticoids, relapses were observed in 17–28%. Decrease in ENT involvement from 77% to 21% in patients treated with MEPO with or without GC and csDMARDs, relapse in 16% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krol, R.M.; Remmelts, H.H.F.; Klaasen, R.; Frima, A.; Hagen, E.C.; Kamalski, D.M.A.; Heijstek, M.W.; Spierings, J. Systemic and Local Medical or Surgical Therapies for Ear, Nose and/or Throat Manifestations in ANCA-Associated Vasculitis: A Systematic Literature Review. J. Clin. Med. 2023, 12, 3173. https://doi.org/10.3390/jcm12093173
Krol RM, Remmelts HHF, Klaasen R, Frima A, Hagen EC, Kamalski DMA, Heijstek MW, Spierings J. Systemic and Local Medical or Surgical Therapies for Ear, Nose and/or Throat Manifestations in ANCA-Associated Vasculitis: A Systematic Literature Review. Journal of Clinical Medicine. 2023; 12(9):3173. https://doi.org/10.3390/jcm12093173
Chicago/Turabian StyleKrol, Roline M., Hilde H. F. Remmelts, Ruth Klaasen, Annelies Frima, E. Christiaan Hagen, Digna M. A. Kamalski, Marloes W. Heijstek, and Julia Spierings. 2023. "Systemic and Local Medical or Surgical Therapies for Ear, Nose and/or Throat Manifestations in ANCA-Associated Vasculitis: A Systematic Literature Review" Journal of Clinical Medicine 12, no. 9: 3173. https://doi.org/10.3390/jcm12093173
APA StyleKrol, R. M., Remmelts, H. H. F., Klaasen, R., Frima, A., Hagen, E. C., Kamalski, D. M. A., Heijstek, M. W., & Spierings, J. (2023). Systemic and Local Medical or Surgical Therapies for Ear, Nose and/or Throat Manifestations in ANCA-Associated Vasculitis: A Systematic Literature Review. Journal of Clinical Medicine, 12(9), 3173. https://doi.org/10.3390/jcm12093173