
Refractory Takayasu’s Arteritis with Severe Coronary Involvement—Case Report and Literature Review

 ,
,  ,
, 
Abstract
:1. Introduction
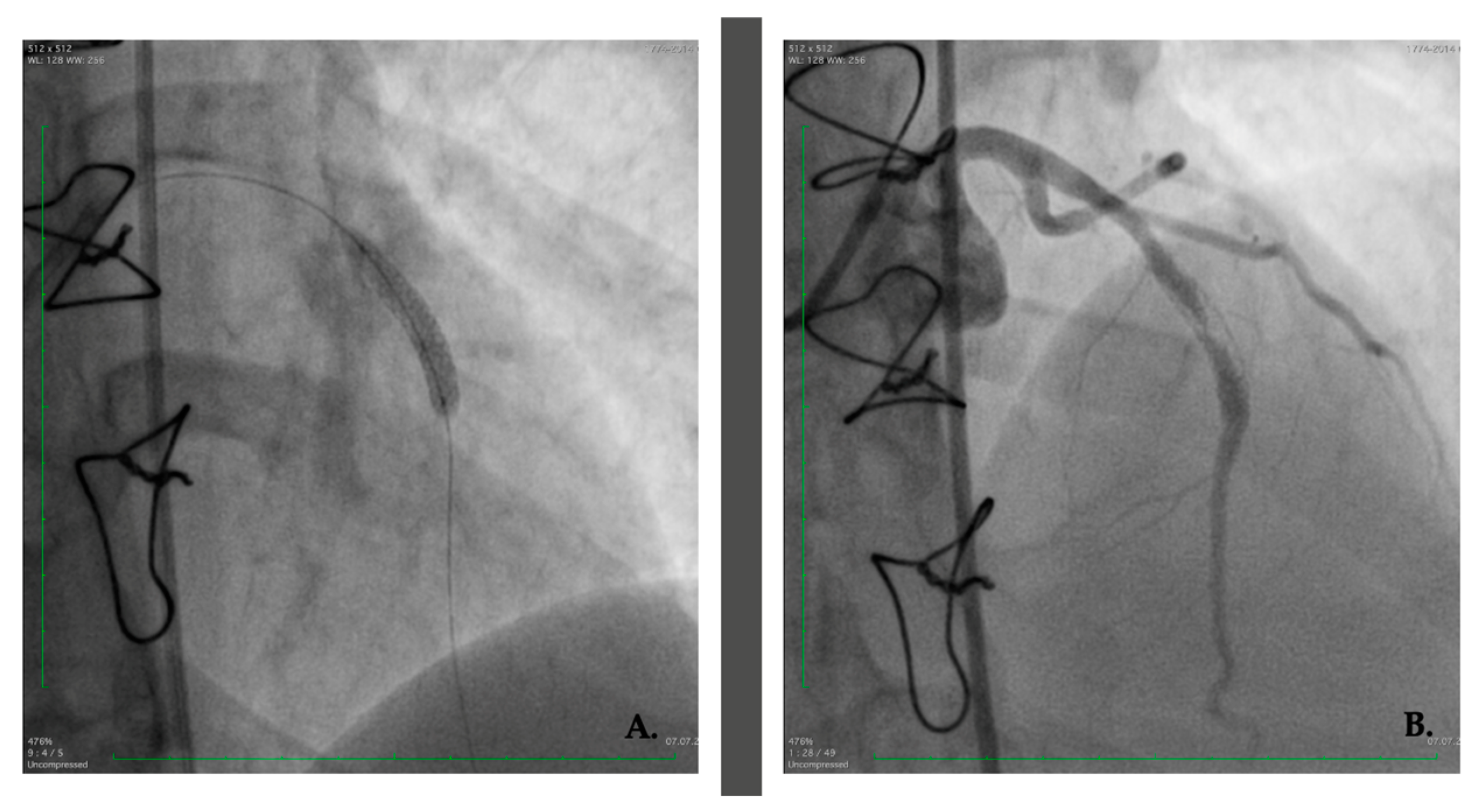
2. Case Presentation
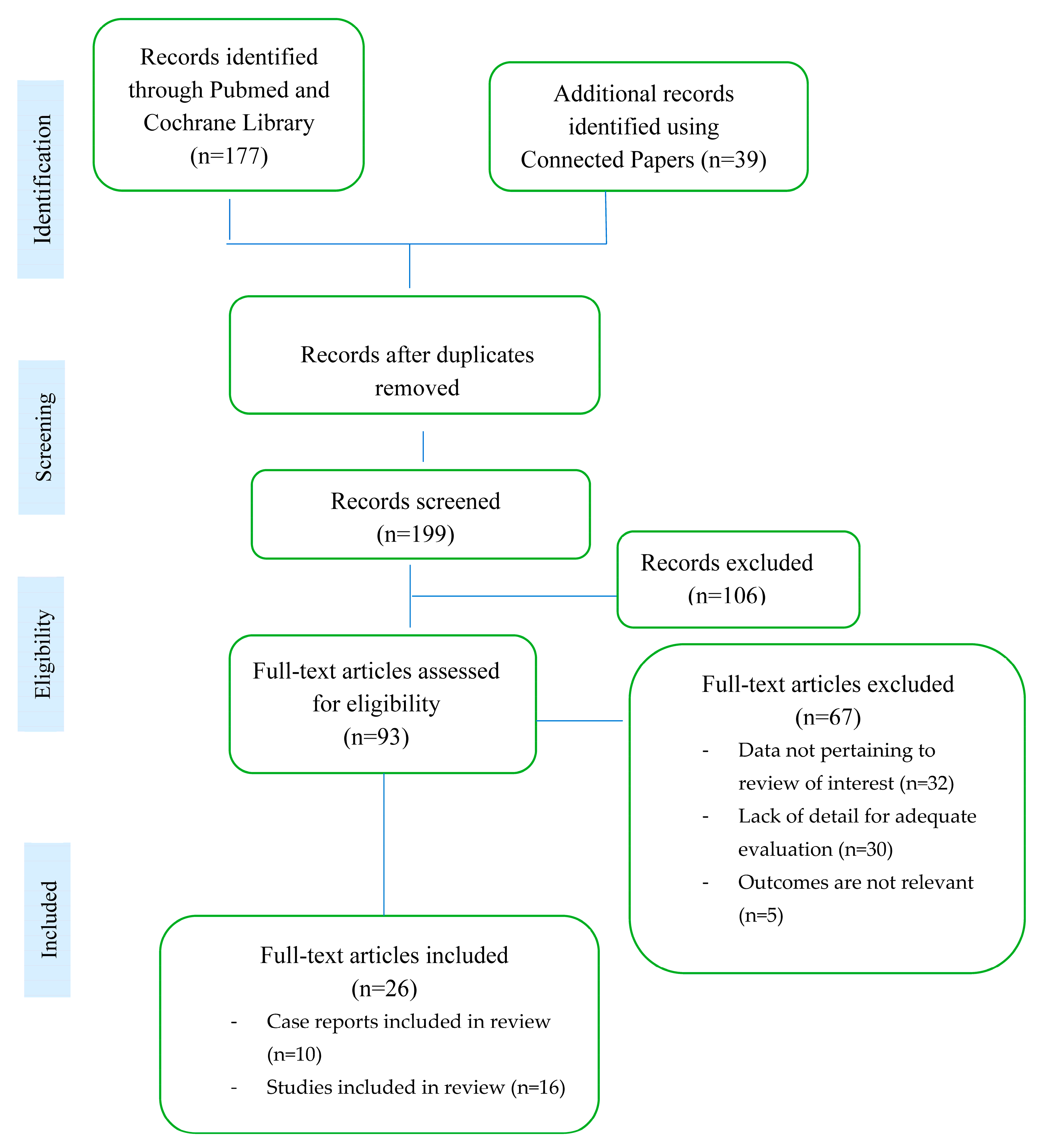
3. Materials and Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Recent Advances in the Diagnosis and Therapy of Large Vessel Vasculitis. Available online: https://www.mp.pl/paim/issue/article/16272 (accessed on 8 May 2023).
- Ponte, C.; Grayson, P.C.; Robson, J.C.; Suppiah, R.; Gribbons, K.B.; Judge, A.; Craven, A.; Khalid, S.; Hutchings, A.; Watts, R.A.; et al. 2022 American College of Rheumatology/EULAR classification criteria for Takayasu arteritis. Ann. Rheum. Dis. 2022, 81, 1647–1653. Available online: https://ard.bmj.com/content/81/12/1654 (accessed on 27 February 2023). [CrossRef] [PubMed]
- Dejaco, C.; Ramiro, S.; Duftner, C.; Besson, F.L.; Bley, T.A.; Blockmans, D.; Brouwer, E.; Cimmino, M.A.; Clark, E.; Dasgupta, B.; et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann. Rheum. Dis. 2018, 77, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Gloor, A.D.; Chollet, L.; Christ, L.A.; Cullmann, J.L.; Bonel, H.M.; Villiger, P.M. Takayasu arteritis: Prevalence and Clinical Presentation in Switzerland. PLoS ONE 2021, 16, e0250025. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0250025 (accessed on 8 May 2023). [CrossRef] [PubMed]
- Le Joncour, A.; Desbois, A.-C.; Leroyer, A.S.; Tellier, E.; Régnier, P.; Maciejewski-Duval, A.; Comarmond, C.; Barete, S.; Arock, M.; Bruneval, P.; et al. Mast cells drive pathologic vascular lesions in Takayasu arteritis. J. Allergy Clin. Immunol. 2022, 149, 292–301.e3. [Google Scholar] [CrossRef]
- Danda, D.P.; Manikuppam, P.; Tian, X.; Harigai, M. Advances in Takayasu arteritis: An Asia Pacific perspective. Front. Med. 2023, 9, 2022. Available online: https://www.frontiersin.org/articles/10.3389/fmed.2022.952972 (accessed on 27 February 2023). [CrossRef]
- Grayson, P.C.; Maksimowicz-McKinnon, K.; Clark, T.M.; Tomasson, G.; Cuthbertson, D.; Carette, S.; A Khalidi, N.; A Langford, C.; Monach, P.; Seo, P.; et al. Distribution of arterial lesions in Takayasu’s arteritis and giant cell arteritis. Ann. Rheum. Dis. 2012, 71, 1329–1334. [Google Scholar] [CrossRef] [Green Version]
- Kumar, G.V.R.; Agarwal, N.B.; Javali, S.; Patwardhan, A.M. Takayasu’s arteritis with ostial and left main coronary artery stenosis. Tex. Heart Inst. J. 2007, 34, 470–474. [Google Scholar]
- Joseph, G.; Goel, R.; Thomson, V.S.; Joseph, E.; Danda, D. Takayasu Arteritis. J. Am. Coll. Cardiol. 2023, 81, 172–186. [Google Scholar] [CrossRef]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; De Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. Update of the EULAR Recommendations for the Management of Large Vessel Vasculitis. Ann. Rheum. Dis. 2020, 71, 19–30. Available online: https://ard.bmj.com/content/79/1/19 (accessed on 3 March 2023). [CrossRef] [Green Version]
- Rav-Acha, M.; Plot, L.; Peled, N.; Amital, H. Coronary involvement in Takayasu’s arteritis. Autoimmun. Rev. 2007, 6, 566–571. [Google Scholar] [CrossRef]
- Park, J.-S.; Lee, H.C.; Lee, S.K.; Kim, S.P.; Kim, Y.D.; Ahn, M.S.; Hong, T.J. Takayasu’s Arteritis Involving the Ostia of Three Large Coronary Arteries. Korean Circ. J. 2009, 39, 551–555. Available online: https://www.semanticscholar.org/paper/Takayasu%27s-Arteritis-Involving-the-Ostia-of-Three-Park-Lee/6bb22fcfc85cd3eaff7a8fe3ff5ff8500d1a511f (accessed on 11 February 2023). [CrossRef] [Green Version]
- Yokota, K.; Shimpo, M.; Iwata, T.; Hirose, M.; Ikemoto, T.; Ohya, K.-I.; Katsuki, T.; Shimada, K.; Kario, K. A Case of Takayasu Arteritis with Repeated Coronary Artery Restenosis after Drug-Eluting Stent Implantation Successfully Treated with a Combination of Steroids. Intern. Med. 2012, 51, 739–743. [Google Scholar] [CrossRef] [Green Version]
- Soni, M.R.; Bohara, A.D.; Mahajan, U.A.; Nathani, J.P. Everolimus eluting stent for critical left main stenosis in Takayasu arteritis. J. Indian Coll. Cardiol. 2012, 2, 93–96. [Google Scholar] [CrossRef]
- Lee, H.K.; Namgung, J.; Choi, W.-H.; Choe, H.; Kwon, S.U.; Doh, J.H.; Lee, S.Y.; Lee, W.R. Stenting of the Left Main Coronary Artery in a Patient with Takayasu’s Arteritis. Korean Circ. J. 2011, 41, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Gao, C.; Li, F. Acute myocardial infarction with left main coronary artery ostial negative remodelling as the first manifestation of Takayasu arteritis: A case report. BMC Cardiovasc. Disord. 2021, 21, 560. [Google Scholar] [CrossRef]
- Zhang, T.; Peng, B.; Tu, X.; Zhang, S.; Zhong, S.; Cao, W. Acute myocardial infarction as the first manifestation of Takayasu arteritis. Medicine 2019, 98, e15143. [Google Scholar] [CrossRef]
- Mihailovici, A.; Donoiu, I. A Case of Severe Advanced Takayasu Arteritis with Acute Myocardial Infarction as First Manifestation. Curr. Health Sci. J. 2018, 44, 80–84. [Google Scholar] [CrossRef]
- Wang, X.; Dang, A.; Lv, N.; Liu, Q.; Chen, B. High-sensitivity C-reactive protein predicts adverse cardiovascular events in patients with Takayasu arteritis with coronary artery involvement. Clin. Rheumatol. 2015, 35, 679–684. [Google Scholar] [CrossRef]
- Saadoun, D.; Lambert, M.; Mirault, T.; Resche-Rigon, M.; Koskas, F.; Cluzel, P.; Mignot, C.; Schoindre, Y.; Chiche, L.; Hatron, P.-Y.; et al. Retrospective Analysis of Surgery Versus Endovascular Intervention in Takayasu Arteritis. Circulation 2012, 125, 813–819. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Zhang, H.; Wang, M.; Yang, W.; Qiao, S.; Hu, F. Revascularization Versus Medical Therapy in Takayasu’s Arteritis Patients with Coronary Artery Involvement. Rheumatol. Ther. 2020, 8, 119–133. [Google Scholar] [CrossRef]
- Kuijer, A.; Van Oosterhout, M.F.M.; Kloppenburg, G.T.L.; Morshuis, W.J. Coronary artery bypass grafting in Takayasu’s disease—Importance of the proximal anastomosis: A case report. J. Med. Case Rep. 2015, 9, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Dang, A. Prognostic Value of Brachial-Ankle Pulse Wave Velocity in Patients with Takayasu Arteritis with Drug-Eluting Stent Implantation. Arthritis Care Res. 2015, 67, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dang, A.; Lv, N.; Cheng, N.; Cheng, X.; Yang, Y.; Song, Y. Long-term outcomes of coronary artery bypass grafting versus percutaneous coronary intervention for Takayasu arteritis patients with coronary artery involvement. Semin. Arthritis Rheum. 2017, 47, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.-M.; Lin, H.-Z. Coronary artery involvements in Takayasu arteritis: Systematic review of reports. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 883–904. [Google Scholar] [CrossRef]
- Al-Hulaimi, N.; Al-Saileek, A.; Ahmed, T.; Al-Zaibag, M.; Pai, R.G.; El-Widaa, H. Mixed aneurysmal and obstructive coronary artery disease causing acute myocardial infarction in a young woman with Takayasu’s arteritis. Can. J. Cardiol. 2001, 17, 602–605. [Google Scholar]
- Cobilinschi, C.; Cobilinschi, C.; Constantinescu, A.; Draniceanu, I.; Ionescu, R. New-Onset ANCA-Associated Vasculitis in a Patient with SARS-COV. Balk. Med. J. 2021, 38, 318–320. [Google Scholar] [CrossRef]
- Xu, Y.; Luo, L.; Su, G.; Zhu, J.; Kang, M.; Zhang, D.; Lai, J.; Li, X. Clinical characteristics and risk factors of coronary artery lesions in Chinese pediatric Takayasu arteritis patients: A retrospective study. Pediatr. Rheumatol. 2023, 21, 42. [Google Scholar] [CrossRef]
- Sun, T.; Zhang, H.; Ma, W.; Yang, L.; Jiang, X.; Wu, H.; Hui, R.; Zheng, D. Coronary Artery Involvement in Takayasu Arteritis in 45 Chinese Patients. J. Rheumatol. 2013, 40, 493–497. [Google Scholar] [CrossRef]
- Ci, W.; Zhao, Y.; Bi, T. Male Patients with Takayasu Arteritis and Coronary Artery Involvement are Prone to have Serious Coronary Stenosis and High Mortality. Curr. Vasc. Pharmacol. 2021, 20, 62–68. [Google Scholar] [CrossRef]
- Yang, Y.; Tian, T.; Yang, K.; Zhang, Y.; Meng, X.; Fan, P.; Feng, L.; Mu, C.; Gao, L.; Zhou, X. Outcomes of percutaneous coronary intervention and coronary artery bypass grafting in patients with Takayasu arteritis. Int. J. Cardiol. 2017, 241, 64–69. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, Y.; Shen, Z.; Fang, L.; Liu, Z.; Zhang, S. Comparing the effects of different management strategies on long-term outcomes for significant coronary stenosis in patients with Takayasu arteritis. Int. J. Cardiol. 2020, 306, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Maz, M.; Chung, S.A.; Abril, A.; Langford, C.A.; Gorelik, M.; Guyatt, G.; Archer, A.M.; Conn, D.L.; Full, K.A.; Grayson, P.C.; et al. American College of Rheumatology/Vasculitis Foundation Guideline for the Management of Giant Cell Arteritis and Takayasu Arteritis. Arthritis Rheumatol. 2021, 73, 1349–1365. [Google Scholar] [CrossRef]
- Laurent, C.; Ricard, L.; Fain, O.; Buvat, I.; Adedjouma, A.; Soussan, M.; Mekinian, A. PET/MRI in Large-Vessel Vasculitis: Clinical Value for diagnosis and Assessment of Disease Activity. Sci. Rep. 2019, 9, 12388. Available online: https://www.nature.com/articles/s41598-019-48709-w (accessed on 21 June 2023). [CrossRef] [Green Version]
- Ćorović, A.; Wall, C.; Nus, M.; Gopalan, D.; Huang, Y.; Imaz, M.; Zulcinski, M.; Peverelli, M.; Uryga, A.; Lambert, J.; et al. Somatostatin Receptor PET/MR Imaging of Inflammation in Patients with Large Vessel Vasculitis and Atherosclerosis. J. Am. Coll. Cardiol. 2023, 81, 336–354. [Google Scholar] [CrossRef]
- O’Connor, T.E.; Carpenter, H.E.; Bidari, S.; Waters, M.F.; Hedna, V.S. Role of inflammatory markers in Takayasu arteritis disease monitoring. BMC Neurol. 2014, 14, 62. [Google Scholar] [CrossRef] [Green Version]
- Pathadan, A.P.; Tyagi, S.; Gupta, M.D.; Girish, M.P.; Mahajan, S.; Kunal, S.; Mahajan, B.; Bansal, A. The study of novel inflammatory markers in takayasu arteritis and its correlation with disease activity. Indian Heart J. 2021, 73, 640–643. [Google Scholar] [CrossRef]
- Joseph, G.; Thomson, V.S.; Attumalil, T.V.; Mathen, P.G.; Anandaraj, A.M.; George, O.K.; George, P.V.; Goel, R.; Kumar, S.; Mathew, J.; et al. Outcomes of Percutaneous Intervention in Patients with Takayasu Arteritis. J. Am. Coll. Cardiol. 2023, 81, 49–64. [Google Scholar] [CrossRef]
- Oliviero, F.; Galozzi, P.; Zanatta, E.; Gatto, M.; Spinella, P.; Doria, A. The Influence of Dietary Intervention in Connective Tissue Diseases: Evidence from Randomized Clinical Trials. Available online: https://www.semanticscholar.org/paper/The-In%EF%AC%82uence-of-Dietary-Intervention-in-Connective-Oliviero-Galozzi/f14a0b8e13d877dcaffb2e30fc710aeca8efffba (accessed on 9 May 2023).
- Byun, J.-W.; Song, H.-J.; Kim, L.; Shin, J.-H.; Choi, G.-S. Predictive Factors of Relapse in Adult with Henoch-Schönlein Purpura. Am. J. Dermatopathol. 2012, 34, 139–144. [Google Scholar] [CrossRef]
- Yin, D.H.; Guo, Y.L.; Cao, T.T.; Pan, C.L.; Zhao, G.J.; Hu, Y. Effect of animal protein diet on the prognosis of children with Henoch-Schönlein purpura. Zhongguo Dang Dai Er Ke Za Zhi 2021, 23, 927–932. [Google Scholar] [CrossRef]
- Ţincu, I.F.; Păcurar, D.; Ţincu, R.C.; Becheanu, C. Influence of Protein Intake During Complementary Feeding on Body Size and IGF-I Levels in 12-Months-Old Infants. Balk. Med. J. 2019, 37, 54–55. [Google Scholar] [CrossRef]
- Koelman, L.; Markova, M.; Seebeck, N.; Hornemann, S.; Rosenthal, A.; Lange, V.; Pivovarova-Ramich, O.; Aleksandrova, K. Effects of High and Low Protein Diets on Inflammatory Profiles in People with Morbid Obesity: A 3-Week Intervention Study. Nutrients 2020, 12, 3636. [Google Scholar] [CrossRef] [PubMed]
- Arbeus, M.; Souza, D.; Geijer, H.; Lidén, M.; Pinheiro, B.; Bodin, L.; Samano, N. Five-year patency for the no-touch saphenous vein and the left internal thoracic artery in on- and off-pump coronary artery bypass grafting. J. Card. Surg. 2021, 36, 3702–3708. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Publication Domain | Author, Year | Article Type (Case Report /Study) | Summary |
|---|---|---|---|
| Clinical | Grayson P. C. et al., 2012, 2022 [2,7] Acha M. R et al., 2007 [11] | Study Study | Coronary artery involvement is common in TA Types of involvement: occlusion or stenosis of the coronary ostia and the proximal segments (type 1), focal or diffuse coronary arteritis (type 2) and coronary aneurysms (type 3) |
| Sun T. et al., 2013 [29] | Study | The most frequent sites involved are the coronary ostium and the proximal segment of the coronary arteries | |
| Yang Y. et al., 2017 [31] | Study | Males tend to have more severe coronary stenosis and a higher risk for long-term mortality | |
| Cobilinschi C. et al., 2021 [27] | Case report | Coronary involvement is linked the atherogenic profile of patients | |
| Xu Y. et al., 2023 [28] | Study | The percentage of coronary lesions is pediatric TA is significantly higher than in the adult population | |
| Park J.S. et al., 2009 [12] Yokota K. et al., 2012 [13] Soni M. R. et al., 2012 [14] Lee H.K. et al., 2011 [15] Zhou S. et al., 2021 [16] Zhang T. et al., 2019 [17] Mihailovici A.R et al., 2018 [18] | Case report Case report Case report Case report Case report Case report Case report | Common symptoms in TA with coronary involvement: angina pectoris, dyspnea on exertion, retrosternal chest pain as acute myocardial infarction | |
| Biological | Wang X. et al., 2016 [19] | Study | HsCRP can predict adverse cardiovascular events in TA with coronary artery involvement |
| Saadoun D. et al., 2012 [20] Wang H. et al., 2020 [32] | Study Study | Biological inflammation at revascularization increases the risk of vascular complications with reinterventions Disease activity predicts progression in patients with TA and coronary stenosis | |
| O’Connor T.E. et al., 2014 [33] | Study | Inflammatory markers are not reliable to distinguish active from inactive disease | |
| Drug therapy | Huang Z. et al., 2021 [21] | Study | Corticosteroids are used in combination with immunosuppressants, preferably before revascularization |
| Surgical therapy | Kuijer A. et al., 2015 [22] Wang X et al., 2015 [23] Wang X et al., 2017 [24] | Case report Study Study | Revascularization techniques for coronary stenosis are PCI, PCI with drug-eluting stents and CABG Coronary angioplasty and drug-eluting stent insertion have a high risk of restenosis PCI is an alternative to CABG after patients reach remission of the disease with medical therapy |
| Yuan S. M., 2020 [25] Al-Hulaimi N. et al., 2001 [26] | Study Case report | Restenosis may occur even in the absence of clinical symptoms | |
| Ci W. et al., 2022 [30] Pathadan A.P et al., 2021 [34] | Study Study | Determining interleukin levels can be of use when initiating biological therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cobilinschi, C.O.; Grădinaru, E.; Săulescu, I.; Cârstea, N.; Caraiola, S.; Bălănescu, A.R.; Opriș-Belinski, D. Refractory Takayasu’s Arteritis with Severe Coronary Involvement—Case Report and Literature Review. J. Clin. Med. 2023, 12, 4394. https://doi.org/10.3390/jcm12134394
Cobilinschi CO, Grădinaru E, Săulescu I, Cârstea N, Caraiola S, Bălănescu AR, Opriș-Belinski D. Refractory Takayasu’s Arteritis with Severe Coronary Involvement—Case Report and Literature Review. Journal of Clinical Medicine. 2023; 12(13):4394. https://doi.org/10.3390/jcm12134394
Chicago/Turabian StyleCobilinschi, Claudia Oana, Elena Grădinaru, Ioana Săulescu, Nicolae Cârstea, Simona Caraiola, Andra Rodica Bălănescu, and Daniela Opriș-Belinski. 2023. "Refractory Takayasu’s Arteritis with Severe Coronary Involvement—Case Report and Literature Review" Journal of Clinical Medicine 12, no. 13: 4394. https://doi.org/10.3390/jcm12134394
APA StyleCobilinschi, C. O., Grădinaru, E., Săulescu, I., Cârstea, N., Caraiola, S., Bălănescu, A. R., & Opriș-Belinski, D. (2023). Refractory Takayasu’s Arteritis with Severe Coronary Involvement—Case Report and Literature Review. Journal of Clinical Medicine, 12(13), 4394. https://doi.org/10.3390/jcm12134394