

Neuro–Immuno–Psychological Aspects of Chronic Urticaria


Abstract
1. Introduction
1.1. Characteristics and Epidemiology of Chronic Urticaria
1.2. Current Insight into the CSU Mechanism
1.3. Urticaria affects the Quality of Life and Psychological Functioning
2. Psychological and Biological Aspects of Stress Reaction
2.1. Neurobiology of Stress Reaction
2.2. Stress as a Transaction; Acute and Chronic Stress
2.3. Methods of Stress Level Diagnosis
3. Stress-Induced Skin Reaction in the Course of CSU
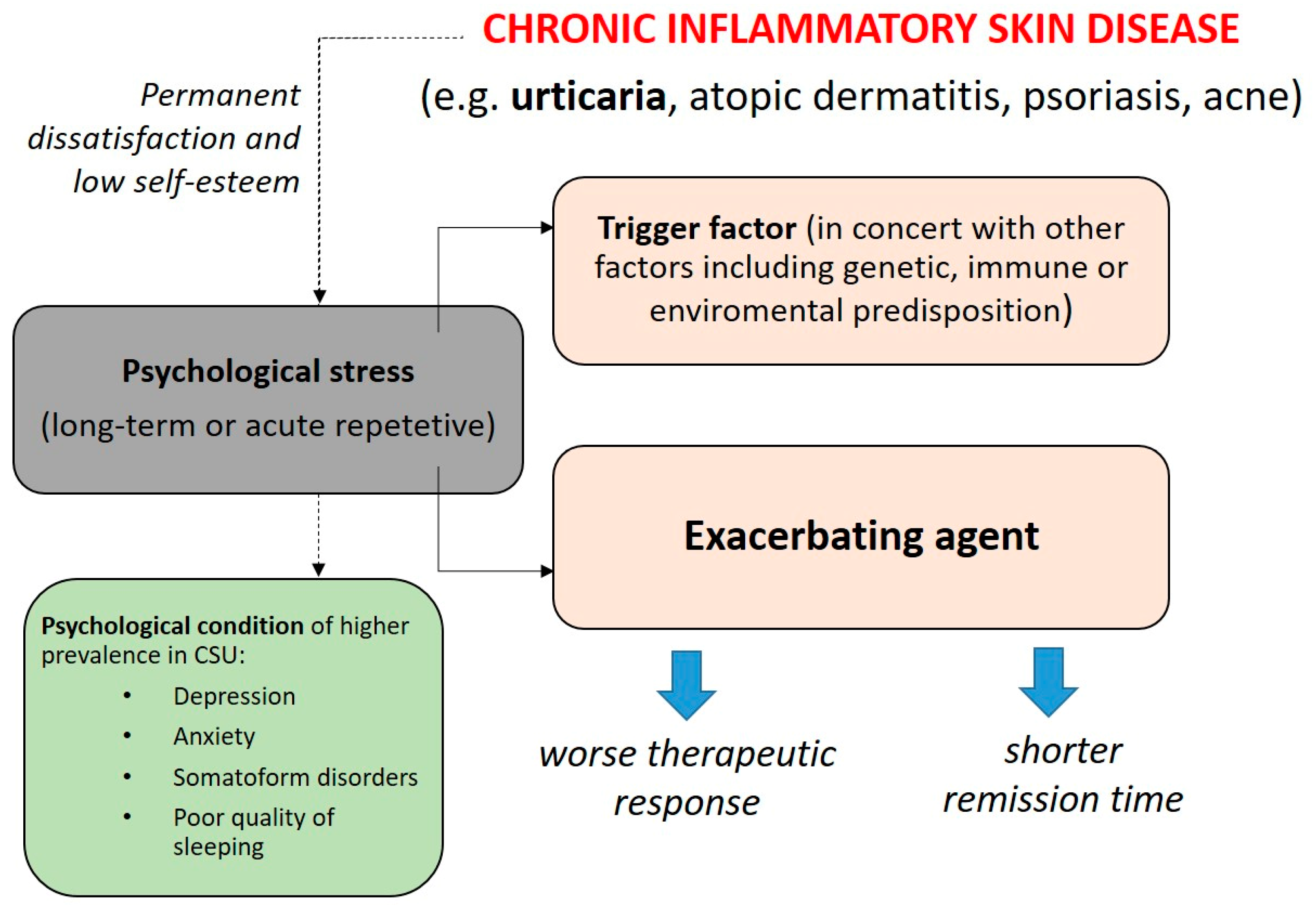
3.1. Stress and Skin Diseases
3.2. HPA Axis and CSU
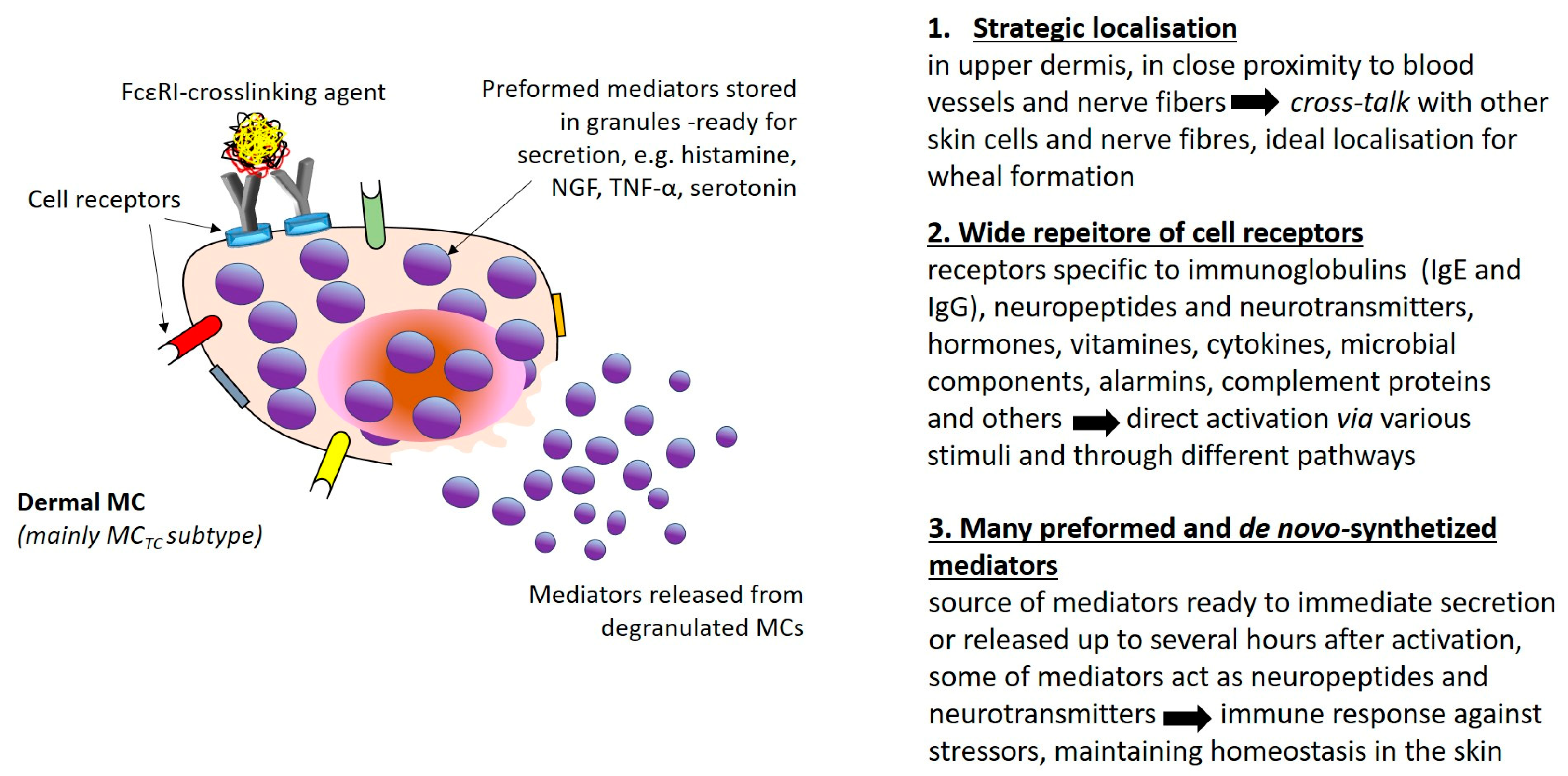
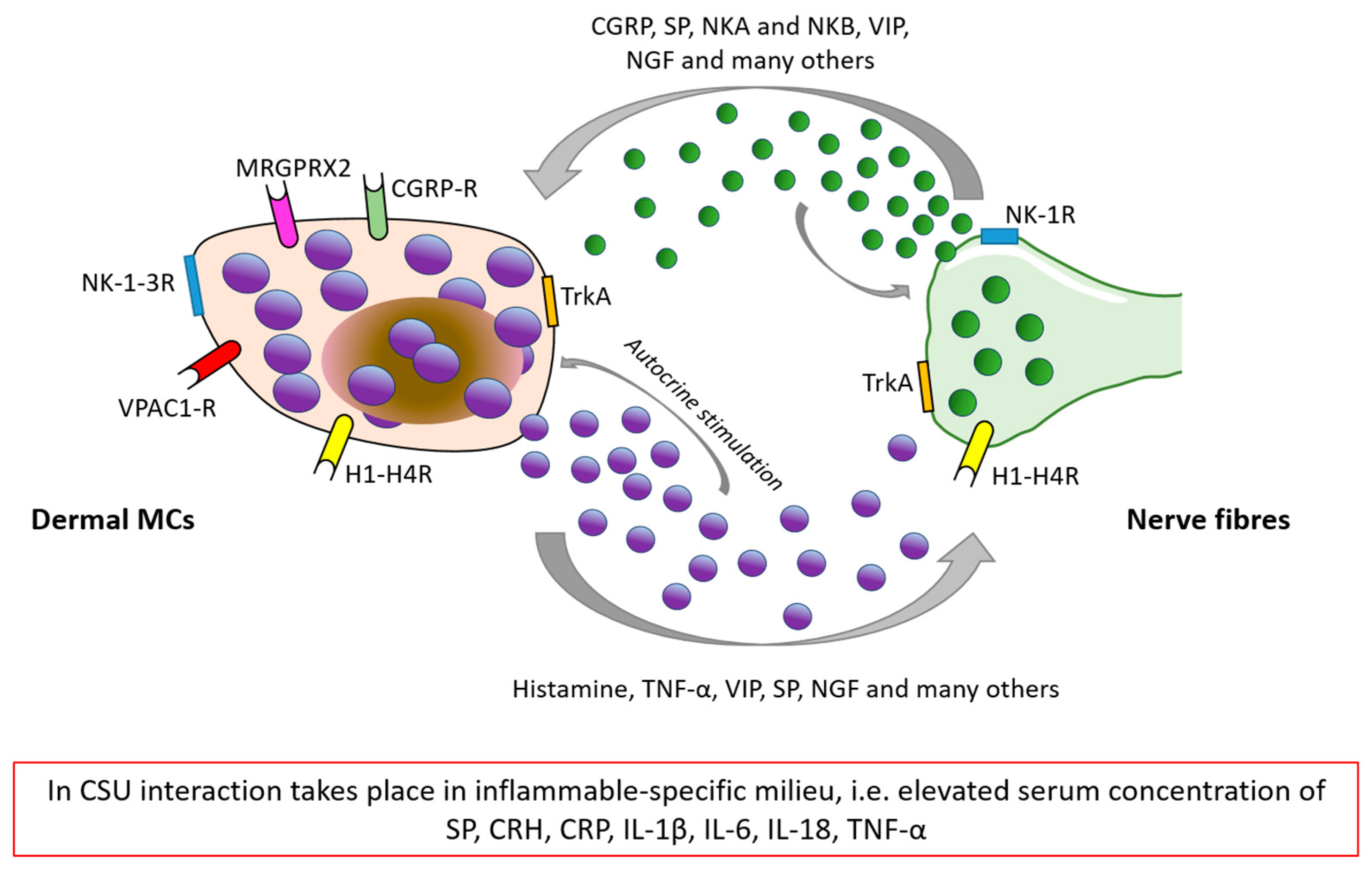
3.3. Neuro–Immuno–Cutaneous Circuit and Its Potential Implication in CSU

4. Recommended Psychological Intervention in Stress-Induced Skin Diseases
5. Conclusions
Funding
Conflicts of Interest
References
- Zuberbier, T.; Abdul Latiff, A.H.; Abuzakouk, M.; Aquilina, S.; Asero, R.; Baker, D.; Ballmer-Weber, B.; Bangert, C.; Ben-Shoshan, M.; Bernstein, J.A.; et al. The International EAACI/GA2LEN/EuroGuiDerm/APAAACI Guideline for the Definition, Classification, Diagnosis, and Management of Urticaria. Allergy 2022, 77, 734–766. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Borges, M.; Ansotegui, I.J.; Baiardini, I.; Bernstein, J.; Canonica, G.W.; Ebisawa, M.; Gomez, M.; Gonzalez-Diaz, S.N.; Martin, B.; Morais-Almeida, M.; et al. The Challenges of Chronic Urticaria Part 1: Epidemiology, Immunopathogenesis, Comorbidities, Quality of Life, and Management. World Allergy Organ. J. 2021, 14, 100533. [Google Scholar] [CrossRef] [PubMed]
- Jain, S. Pathogenesis of chronic urticaria: An overview. Dermatol. Res. Pract. 2014, 2014, 674709. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, G.N.; Riedl, M.A.; Valent, P.; Podder, I.; Maurer, M. Urticaria and angioedema: Understanding complex pathomechanisms to facilitate patient communication, disease management, and future treatment. J. Allergy Clin. Immunol. Pract. 2023, 11, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Church, M.K.; Kolkhir, P.; Metz, M.; Maurer, M. The role and relevance of mast cells in urticaria. Immunol. Rev. 2018, 282, 232–247. [Google Scholar] [CrossRef]
- Elieh Ali Komi, D.; Wöhrl, S.; Bielory, L. Mast cell biology at molecular level: A comprehensive review. Clin. Rev. Allergy Immunol. 2020, 58, 342–365. [Google Scholar] [CrossRef]
- Choi, J.E.; Di Nardo, A. Skin neurogenic inflammation. In Seminars in Immunopathology; Springer: Berlin/Heidelberg, Germany, 2018; pp. 249–259. [Google Scholar] [CrossRef]
- Xu, H.; Shi, X.; Li, X.; Zou, J.; Zhou, C.; Liu, W.; Shao, H.; Chen, H.; Shi, L. Neurotransmitter and neuropeptide regulation of mast cell function: A systematic review. J. Neuroinflammation 2020, 17, 356. [Google Scholar] [CrossRef]
- Kay, A.B.; Clark, P.; Maurer, M.; Ying, S. Elevations in T-helper-2-initiating cytokines (interleukin-33, interleukin-25 and thymic stromal lymphopoietin) in lesional skin from chronic spontaneous (‘idiopathic’) urticaria. Br. J. Dermatol. 2015, 172, 1294–1302. [Google Scholar] [CrossRef]
- Ferrer, M. Immunological events in chronic spontaneous urticaria. Clin. Transl. Allergy 2015, 5, 30. [Google Scholar] [CrossRef]
- Konstantinou, G.N.; Konstantinou, G.N. Psychological stress and chronic urticaria: A neuro-immuno-cutaneous crosstalk. A systematic review of the existing evidence. Clin. Ther. 2020, 42, 771–782. [Google Scholar] [CrossRef]
- Bansal, C.J.; Bansal, A.S. Stress, pseudoallergens, autoimmunity, infection and inflammation in chronic spontaneous urticaria. Allergy Asthma Clin. Immunol. 2019, 15, 56. [Google Scholar] [CrossRef] [PubMed]
- Kocatürk, E.; Salman, A.; Cherrez-Ojeda, I.; Criado, P.R.; Peter, J.; Comert-Ozer, E.; Abuzakouk, M.; Agondi, R.C.; Al-Ahmad, M.; Altrichter, S.; et al. The global impact of the COVID-19 pandemic on the management and course of chronic urticaria. Allergy 2020, 76, 816–830. [Google Scholar] [CrossRef] [PubMed]
- Beyaz, S.; Demir, S.; Oztop, N.; Karadag, P.; Coskun, R.; Colakoglu, B.; Buyukozturk, S.; Gelincik, A. Psychological burden of COVID-19 on mild and moderate chronic spontaneous urticaria. Allergy Asthma Proc. 2021, 42, e107–e115. [Google Scholar] [CrossRef]
- Ben-Shoshan, M.; Blinderman, I.; Raz, A. Psychosocial factors and chronic spontaneous urticaria: A systematic review. Allergy 2013, 68, 131–141. [Google Scholar] [CrossRef]
- Ferrer, M. Epidemiology, healthcare, resources, use and clinical features of different types of urticaria. J. Investig. Allergol. Clin. Immunol. 2009, 19 (Suppl. 2), 21–26. [Google Scholar] [PubMed]
- Delong, L.K.; Culler, S.D.; Saini, S.S.; Beck, L.A.; Chen, S.C. Annual direct and indirect health care costs of chronic idiopathic urticaria: A cost analysis of 50 nonimmunosuppressed patients. Arch. Dermatol. 2008, 144, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Consoli, S.G. Les facteurs psychologiques dans l’urticaire chronique [Psychological factors in chronic urticaria]. Ann. Dermatol. Venereol. 2003, 130, 1S73–1S77. [Google Scholar] [PubMed]
- Barbosa, F.; Freitas, J.; Barbosa, A. Chronic idiopathic urticaria and anxiety symptoms. J. Health Psychol. 2011, 16, 1038–1047. [Google Scholar] [CrossRef]
- Özkan, M.; Oflaz, S.B.; Kocaman, N.; Özşeker, F.; Gelincik, A.; Büyüköztürk, S.; Özkan, S.; Çolakoğlu, B. Psychiatric morbidity and quality of life in patients with chronic idiopathic urticaria. Ann. Allergy Asthma Immunol. 2007, 99, 29–33. [Google Scholar] [CrossRef]
- Malhotra, S.K.; Mehta, V. Role of stressful life events in induction or exacerbation of psoriasis and chronic urticaria. Indian J. Dermatol. Venereol. Leprol. 2008, 74, 594–599. [Google Scholar] [CrossRef]
- Tawil, S.; Irani, C.; Kfoury, R.; Abramian, S.; Salameh, P.; Weller, K.; Maurer, M.; Ezzedine, K. Association of Chronic Urticaria with Psychological Distress: A Multicentre Cross-sectional Study. Acta Derm. Venereol. 2022, 103, adv00865. [Google Scholar] [CrossRef] [PubMed]
- Kaaz, K.; Szepietowski, J.C.; Matusiak, Ł. Sleep quality among adult patients with chronic dermatoses. Postepy Dermatol Alergol. 2019, 36, 659–666. [Google Scholar] [CrossRef]
- Ates, H.; Firat, S.; Buhari, G.K.; Keren, M.; Cifci, B.; Erkekol, F.Ö. Relationships between quality of life, sleep problems, and sleep quality in patients with chronic idiopathic urticaria. J. Cosmet. Dermatol. 2022, 21, 4072–4079. [Google Scholar] [CrossRef] [PubMed]
- Alatas, E.T.; Unal, Y.; Demir Pektas, S.; Kutlu, G. Obstructive sleep apnea syndrome in patients with chronic idiopathic urticaria. Dermatol. Ther. 2020, 33, e14060. [Google Scholar] [CrossRef]
- Mikulska, J.; Juszczyk, G.; Gawrońska-Grzywacz, M.; Herbet, M. HPA Axis in the Pathomechanism of Depression and Schizophrenia: New Therapeutic Strategies Based on Its Participation. Brain Sci. 2021, 11, 1298. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L. Hypothalamic–Pituitary–Adrenocortical Axis Regulation. Endocrinol. Metab. Clin. 2005, 34, 271–292. [Google Scholar] [CrossRef]
- Godoy, L.D.; Rossignoli, M.T.; Delfino-Pereira, P.; Garcia-Cairasco, N.; de Lima Umeoka, E.H. A Comprehensive Overview on Stress Neurobiology: Basic Concepts and Clinical Implications. Front. Behav. Neurosci. 2018, 12, 127. [Google Scholar] [CrossRef]
- Tank, A.W.; Wong, D.L. Peripheral and Central Effects of Circulating Catecholamines. Compr. Physiol. 2015, 5, 1–15. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The Gut-Brain Axis: Interactions between Enteric Microbiota, Central and Enteric Nervous Systems. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2015, 28, 78. [Google Scholar] [CrossRef]
- Farhadi, A.; Fields, J.Z.; Keshavarzian, A. Mucosal Mast Cells Are Pivotal Elements in Inflammatory Bowel Disease That Connect the Dots: Stress, Intestinal Hyperpermeability and Inflammation. World J. Gastroenterol. 2007, 13, 3027. [Google Scholar] [CrossRef]
- Wallon, C.; Yang, P.C.; Keita, Å.V.; Ericson, A.C.; McKay, D.M.; Sherman, P.M.; Perdue, M.H.; Söderholm, J.D. Corticotropin-Releasing Hormone (CRH) Regulates Macromolecular Permeability via Mast Cells in Normal Human Colonic Biopsies in Vitro. Gut 2008, 57, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Krišto, M.; Lugovi´c, L.; Mihi´c, L.-M.; Muñoz, M.; Rupnik, M.; Mahnic, A.; Ozreti´c, O.; Jaganjac, M.; Cesi´c, C.; Kuna, M. Gut Microbiome Composition in Patients with Chronic Urticaria: A Review of Current Evidence and Data. Life 2023, 13, 152. [Google Scholar] [CrossRef] [PubMed]
- Gubert, C.; Kong, G.; Renoir, T.; Hannan, A.J. Exercise, diet and stress as modulators of gut microbiota: Implications for neurodegenerative diseases. Neurobiol. Dis. 2020, 134, 104621. [Google Scholar] [CrossRef] [PubMed]
- Barrio, C.; Arias-Sanchez, S.; Martin-Monzon, I. The gut microbiota-brain axis, psychobiotics and its influence on brain and behaviour: A systematic review. Psychoneuroendocrinology 2022, 137, 105640. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1966. [Google Scholar]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Ogińska-Bulik, N. Zasoby osobiste jako wyznaczniki radzenia sobie ze stresem u dzieci. [Personal resources as determinants of coping with stress in children]. Folia Psychol. 2001, 5, 83–93. [Google Scholar]
- McEwen, B.S. Protection and Damage from Acute and Chronic Stress: Allostasis and Allostatic Overload and Relevance to the Pathophysiology of Psychiatric Disorders. Ann. N. Y. Acad. Sci. 2004, 1032, 1–7. [Google Scholar] [CrossRef]
- Bishop, G.D. Psychologia Zdrowia [Health Psychology]; Astrum: Wroclaw, Poland, 2007. [Google Scholar]
- Juczyński, Z.; Ogińska-Bulik, N. NPSR-Narzędzia Pomiaru Stresu i Radzenia Sobie ze Stresem [Stress and Coping Measurement Tools]; Polskie Towarzystwo Psychologiczne: Warsaw, Poland, 2009. [Google Scholar]
- Endler, N.S.; Parker, J.D. Coping Inventory for Stressful Situations (CISS): Manual; Multi-Health Systems: Toronto, ON, Canada, 1999. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Dalgard, F.J.; Gieler, U.; Tomas-Aragones, L.; Lien, L.; Poot, F.; Jemec, G.B.; Misery, L.; Szabo, C.; Linder, D.; Sampogna, F.; et al. The psychological burden of skin diseases: A cross-sectional multicenter study among dermatological out-patients in 13 European countries. J. Investig. Dermatol. 2015, 135, 984–991. [Google Scholar] [CrossRef]
- Jerković, H.; Bešlić, I.; Ćesić, D.; Šitum, M. The psychosocial burden of urticaria. Rad Hrvat. Akad. Znan. I Umjetnosti. Med. Znan. 2021, 548, 98–103. [Google Scholar] [CrossRef]
- Tat, T.S. Higher levels of depression and anxiety in patients with chronic urticaria. Med. Sci. Monit. 2019, 25, 115. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.S.; Nam, Y.H.; Park, C.S.; Kim, M.Y.; Jo, E.J.; Park, H.K.; Kim, H.K. Anxiety, depression, and stress in Korean patients with chronic urticaria. Korean J. Intern. Med. 2020, 35, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Patella, V.; Zunno, R.; Florio, G.; Palmieri, M.; Palmieri, S.; Brancaccio, R. Omalizumab improves perceived stress, anxiety, and depression in chronic spontaneous urticaria. J. Allergy Clin. Immunol. Pract. 2021, 9, 1402–1404. [Google Scholar] [CrossRef] [PubMed]
- Pondeljak, N.; Lugović-Mihić, L. Stress-induced interaction of skin immune cells, hormones, and neurotransmitters. Clin. Ther. 2020, 42, 757–770. [Google Scholar] [CrossRef]
- Nedoszytko, B.; Sokołowska-Wojdyło, M.; Ruckemann-Dziurdzińska, K.; Roszkiewicz, J.; Nowicki, R. Chemokines and cytokines network in the pathogenesis of the inflammatory skin diseases: Atopic dermatitis, psoriasis and skin mastocytosis. Adv. Dermatol. Allergol. 2014, 31, 84–91. [Google Scholar] [CrossRef]
- Varghese, R.; Rajappa, M.; Chandrashekar, L.; Kattimani, S.; Archana, M.; Munisamy, M.; Revathy, G.; Thappa, D. Association among stress, hypocortisolism, systemic inflammation, and disease severity in chronic urticaria. Ann. Allergy Asthma Immunol. 2016, 116, 344–348. [Google Scholar] [CrossRef]
- Kolkhir, P.; Altrichter, S.; Hawro, T.; Maurer, M. C-reactive protein is linked to disease activity, impact, and response to treatment in patients with chronic spontaneous urticaria. Allergy. 2018, 73, 940–948. [Google Scholar] [CrossRef]
- Kim, J.E.; Cho, B.K.; Cho, D.H.; Park, H.J. Expression of hypothalamic–pituitary–adrenal axis in common skin diseases: Evidence of its association with stress-related disease activity. Acta Derm.-Venereol. 2013, 93, 387–393. [Google Scholar] [CrossRef]
- Papadopoulou, N.; Kalogeromitros, D.; Staurianeas, N.G.; Tiblalexi, D.; Theoharides, T.C. Corticotropin-releasing hormone receptor-1 and histidine decarboxylase expression in chronic urticaria. J. Investig. Dermatol. 2005, 125, 952–955. [Google Scholar] [CrossRef]
- Georgala, S.; Schulpis, K.H.; Papaconstantinou, E.; Varelzidis, A. Raised serum levels of β-endorphin in chronic urticaria. J. Eur. Acad. Dermatol. Venereol. 1994, 3, 27–30. [Google Scholar] [CrossRef]
- Vurgun, E.; Memet, B.; Kocaturk, E.; Guntas, G. Evaluation of serum 25-hydroxyvitamin D levels and cortisol/dehydroepiandrosterone sulfate ratio in chronic spontaneous urticaria. Turk. J. Biochem. 2020, 46, 191–196. [Google Scholar] [CrossRef]
- Huang, X.; Hussain, B.; Chang, J. Peripheral Inflammation and Blood–Brain Barrier Disruption: Effects and Mechanisms. CNS Neurosci. Ther. 2021, 27, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Brzoza, Z.; Kasperska-Zajac, A.; Rogala, B. Serum prolactin concentration and its relationship with dehydroepiandrosterone sulfate concentration in chronic urticaria patients with positive and negative response to autologous serum skin test. Allergy 2007, 62, 566–567. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Singh, K.L.; Boucher, W.; Pang, X.; Letourneau, R.; Webster, E.; Chrousos, G. Corticotropin-Releasing Hormone Induces Skin Mast Cell Degranulation and Increased Vascular Permeability, a Possible Explanation for Its Proinflammatory Effects. Endocrinology 1998, 139, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, G.N.; Konstantinou, G.N.; Koulias, C.; Petalas, K.; Makris, M. Further understanding of Neuro-Immune Interactions in Allergy: Implications in Pathophysiology and Role in Disease Progression. J. Asthma Allergy 2022, 15, 1273–1291. [Google Scholar] [CrossRef] [PubMed]
- Dyke, S.M.; Carey, B.S.; Kaminski, E.R. Effect of Stress on Basophil Function in Chronic Idiopathic Urticaria. Clin. Exp. Allergy 2008, 38, 86–92. [Google Scholar] [CrossRef]
- Basak, P.Y.; Erturan, I.; Yuksel, O.; Kazanoglu, O.O.; Vural, H. Evaluation of serum neuropeptide levels in patients with chronic urticaria. Indian J. Dermatol. Venereol. Leprol. 2014, 80, 483. [Google Scholar] [CrossRef]
- Metz, M.; Krull, C.; Hawro, T.; Saluja, R.; Groffik, A. Substance P is upregulated in the serum of patients with chronic spontaneous urticaria. J. Investig. Dermatol. 2014, 134, 2833–2836. [Google Scholar] [CrossRef]
- Zheng, W.; Wang, J.; Zhu, W.; Xu, C.; He, S. Upregulated expression of substance P in basophils of the patients with chronic spontaneous urticaria: Induction of histamine release and basophil accumulation by substance P. Cell Biol. Toxicol. 2016, 32, 217–228. [Google Scholar] [CrossRef]
- Borici-Mazi, R.; Kouridakis, S.; Kontou-Fili, K. Cutaneous responses to substance P and calcitonin gene-related peptide in chronic urticaria: The effect of cetirizine and dimethindene. Allergy 1999, 54, 46–56. [Google Scholar] [CrossRef]
- Chen, Y.; Lyga, J. Brain-Skin Connection: Stress, Inflammation and Skin Aging. Inflamm. Allergy-Drug Targets (Former. Curr. Drug Targets-Inflamm. Allergy)(Discontin.) 2014, 13, 177. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.; Kotrba, J.; Gaffal, E.; Katsoulis-Dimitriou, K.; Dudeck, A. Mast Cells in the Skin: Defenders of Integrity or Offenders in Inflammation? Int. J. Mol. Sci. 2021, 22, 4589. [Google Scholar] [CrossRef] [PubMed]
- Asadi, S.; Alysandratos, K.D.; Angelidou, A.; Miniati, A.; Sismanopoulos, N.; Vasiadi, M.; Zhang, B.; Kalogeromitros, D.; Theoharides, T.C. Substance P (SP) Induces Expression of Functional Corticotropin-Releasing Hormone Receptor-1 (CRHR-1) in Human Mast Cells. J. Investig. Dermatol. 2012, 132, 324–329. [Google Scholar] [CrossRef]
- Fujisawa, D.; Kashiwakura, J.; Kita, H.; Kikukawa, Y.; Fujitani, Y.; Sasaki-Sakamoto, T.; Kuroda, K.; Nunomura, S.; Hayama, K.; Terui, T.; et al. Expression of Mas-related gene X2 on mast cells is upregulated in the skin of patients with severe chronic urticaria. J. Allergy Clin. Immunol. 2014, 134, 622–633. [Google Scholar] [CrossRef] [PubMed]
- Fok, J.S.; Kolkhir, P.; Church, M.K.; Maurer, M. Predictors of treatment response in chronic spontaneous urticaria. Allergy 2021, 76, 2965–2981. [Google Scholar] [CrossRef] [PubMed]
- Redegeld, F.A.; Yu, Y.; Kumari, S.; Charles, N.; Blank, U. Non-IgE mediated mast cell activation. Immunol. Rev. 2018, 282, 87–113. [Google Scholar] [CrossRef]
- Theoharides, T.C. Neuroendocrinology of mast cells: Challenges and controversies. Exp. Dermatol. 2017, 26, 751–759. [Google Scholar] [CrossRef]
- Zalewska-Janowska, A. (Red.) Psychodermatologia. In Ujęcie Interdyscyplinarne [Psychodermatology. Interdyscyplinary Approach]; PZWL Wydawnictwo lekarskie: Warsaw, Poland, 2022; ISBN 9788301223502. [Google Scholar]
- Tzur Bitan, D.; Berzin, D.; Cohen, A. The association of chronic spontaneous urticaria (CSU) with anxiety and depression: A nationwide cohort study. Arch. Dermatol. Res. 2021, 313, 33–39. [Google Scholar] [CrossRef]
- Berrino, A.M.; Voltolini, S.; Fiaschi, D.; Pellegrini, S.; Bignardi, D.; Minale, P.; Troise, C.; Maura, E. Chronic urticaria: Importance of a medical-psychological approach. Eur. Ann. Allergy Clin. Immunol. 2006, 38, 149–152. [Google Scholar]
- Kronenberger, M. Muzykoterapia. In Podstawy Teoretyczne do Zastosowania Muzykoterapii w Profilaktyce stresu [Music Therapy. Theoretical Basis for the Application of Music Therapy in Stress Prevention]; Mediatour: Szczecin, Poland, 2006. [Google Scholar]
- Błaszczak, A. Wpływ Treningu Redukcji Stresu opartego na uważności (MBSR) na zdrowie fizyczne [Effects of Mindfulness-Based Stress Reduction Training (MBSR) on physical health]. Ann. Univ. Mariae Curie-Skłodowska Sect. J. Paedagog.-Psychol. 2018, 31, 61–73. [Google Scholar] [CrossRef]
- Lindsay, K.; Goulding, J.; Solomon, M.; Broom, B. Treating chronic spontaneous urticaria using a brief 'whole person' treatment approach: A proof-of-concept study. Clin. Transl. Allergy 2015, 5, 40. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Neurohormonal Receptors Expressed on MCs | Receptor Ligands |
|---|---|
| NK-1R-Neurokinin-1 receptor | SP-Substance P |
| TrkA-Tropomyosin receptor kinase A | NGF-Nerve growth factor |
| MRGPRX2/MrgX2-Mas-related G protein coupled X2 receptor | SP, VIP-Vasoactive intestinal peptide |
| CGRP-1R, CGRP-2R-Calcitonin gene-related peptide type 1 and 2 receptor | CGRP-Calcitonin gene-related peptide |
| PAC1- pituitary adenylate cyclase activating peptide type I receptor, VPAC1-R, VPAC2-R-vasoactive intestinal peptide receptor type 1 and 2 | VIP, PACAP-Pituitary adenylate cyclase-activating polypeptide |
| NK-2R, NK-3R- Neurokinin-2 and 3 receptor, respectively | NKA-Neurokinin A (NK-2R), NKB-neurokinin B (NK-3R) |
| Y1R, Y2R, Y3R, Y4R, Y5R | NPY-neuropeptide Y |
| H1R-H4R-Histamine receptor type 1–4 | Histamine |
| CRHR-1 and CRHR-2-Corticotropin-releasing hormone receptor | CRH-Corticotropin-releasing hormone |
| MC1R and MC2R-Melanocortin receptors | ACTH-Adrenocorticotropic hormone |
| GR-Glucocorticoid receptor | Cortisol |
| MOR-Mu opioid receptor | β-endorphin |
| NTSR1-Neurotensin receptor 1 | NT-Neurotensin |
| SSTRs-Somatostatin receptors | SST-Somatostatin |
| Relaxation Technique | Description |
|---|---|
| Visualization | A method of imagining pictures, sensations, tastes, and smells without actual sensory experience. It can be conducted in receptive form, in which the practitioner himself allows the imagination to flow freely through his head, or guided, when the content of the visualization is given, and the patients’ task is to follow the instructions. |
| Jacobson training (Progressive muscle relaxation) | Helps to reach a state of relaxation by noticing the difference between “tensed” and “relaxed.” During its course, the patient alternately tenses and relaxes different muscles, starting with the head and ending with the legs and feet. This allows the person to consciously feel the relaxation of tensed muscles, even if the person exercising was previously unaware of the tension he or she was experiencing. |
| Mindfulness Training | Based on the conscious experience of stimuli coming from the environment or the patient body. It can be practiced in many ways; however, it is worth remembering to focus your attention on the “here and now” during the exercises, observe the stimuli that reach a person, and focus on one’s own feelings, but without trying to fight them or suppress those that are difficult at the moment. Mindfulness training helps one realize the relevance of the stimuli reaching the exercising person, has a calming effect, and aids relaxation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomaszewska, K.; Słodka, A.; Tarkowski, B.; Zalewska-Janowska, A. Neuro–Immuno–Psychological Aspects of Chronic Urticaria. J. Clin. Med. 2023, 12, 3134. https://doi.org/10.3390/jcm12093134
Tomaszewska K, Słodka A, Tarkowski B, Zalewska-Janowska A. Neuro–Immuno–Psychological Aspects of Chronic Urticaria. Journal of Clinical Medicine. 2023; 12(9):3134. https://doi.org/10.3390/jcm12093134
Chicago/Turabian StyleTomaszewska, Katarzyna, Aleksandra Słodka, Bartłomiej Tarkowski, and Anna Zalewska-Janowska. 2023. "Neuro–Immuno–Psychological Aspects of Chronic Urticaria" Journal of Clinical Medicine 12, no. 9: 3134. https://doi.org/10.3390/jcm12093134
APA StyleTomaszewska, K., Słodka, A., Tarkowski, B., & Zalewska-Janowska, A. (2023). Neuro–Immuno–Psychological Aspects of Chronic Urticaria. Journal of Clinical Medicine, 12(9), 3134. https://doi.org/10.3390/jcm12093134