
Comparing the Effects of Differential and Visuo-Motor Training on Functional Performance, Biomechanical, and Psychological Factors in Athletes after ACL Reconstruction: A Randomized Controlled Trial


 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
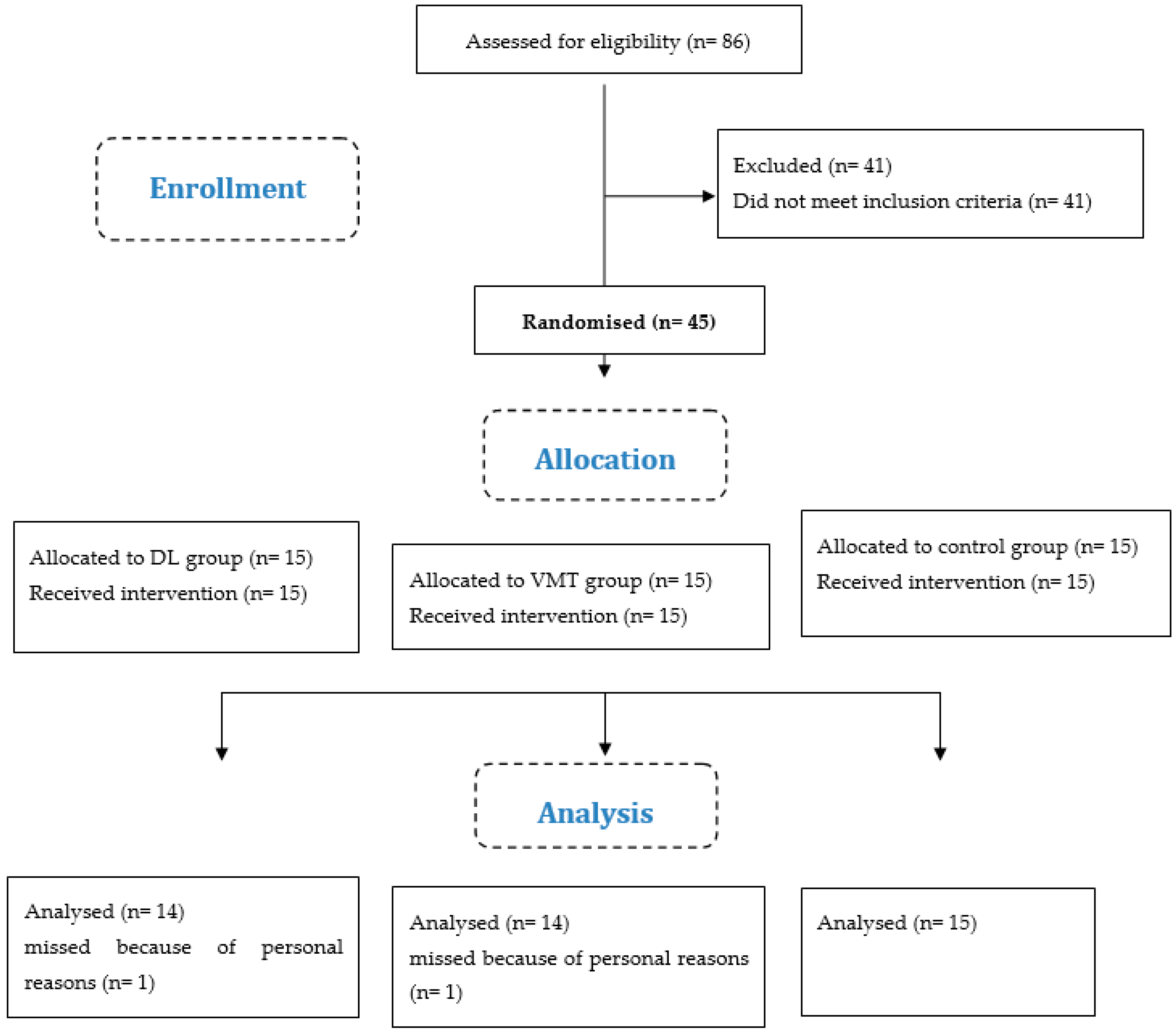
2.1. Study Design
2.2. Participants Recruitment and Eligibility Criteria
2.3. Demographic and Health Data
2.4. Randomization, Allocation, and Implementation
2.5. Sample Size Calculation
2.6. Procedures
3. Primary Outcome Measure
Functional Performance (Triple Hop Test)
4. Secondary Outcome Measures
4.1. Dynamic Balance (Star Excursion Balance Test)
4.2. Biomechanics during Single-Leg Drop-Landing Task
4.3. Data Collection
4.4. Kinesiophobia (TSK)
5. Interventions
5.1. Differential Learning (DL)
5.2. Visual-Motor Training (VMT)
5.3. Control
5.4. Statistical Analysis
6. Results
6.1. Functional Performance
6.2. Dynamic Balance
6.3. Biomechanics
6.4. Kinesiophobia
7. Discussion
8. Limitations
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gokeler, A.; Dingenen, B.; Hewett, T.E. Rehabilitation and return to sport testing after anterior cruciate ligament reconstruction: Where are we in 2022? Arthrosc. Sport. Med. Rehabil. 2022, 4, e77–e82. [Google Scholar] [CrossRef]
- Wiggins, A.J.; Grandhi, R.K.; Schneider, D.K.; Stanfield, D.; Webster, K.E.; Myer, G.D. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Am. J. Sport. Med. 2016, 44, 1861–1876. [Google Scholar] [CrossRef] [PubMed]
- Lie, M.M.; Risberg, M.A.; Storheim, K.; Engebretsen, L.; Øiestad, B.E. What’s the rate of knee osteoarthritis 10 years after anterior cruciate ligament injury? An updated systematic review. Br. J. Sport. Med. 2019, 53, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Thomee, P.; Währborg, P.; Börjesson, M.; Thomee, R.; Eriksson, B.I.; Karlsson, J. Self-efficacy, symptoms and physical activity in patients with an anterior cruciate ligament injury: A prospective study. Scand. J. Med. Sci. Sport. 2007, 17, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Gokeler, A.; Schmalz, T.; Knopf, E.; Freiwald, J.; Blumentritt, S. The relationship between isokinetic quadriceps strength and laxity on gait analysis parameters in anterior cruciate ligament reconstructed knees. Knee Surg. Sport. Traumatol. Arthrosc. 2003, 11, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.V.; Ford, K.R.; Myer, G.D.; Heyl, R.; Hewett, T.E. Limb asymmetries in landing and jumping 2 years following anterior cruciate ligament reconstruction. Clin. J. Sport Med. 2007, 17, 258–262. [Google Scholar] [CrossRef]
- Gokeler, A.; Hof, A.L.; Arnold, M.P.; Dijkstra, P.U.; Postema, K.; Otten, E. Abnormal landing strategies after ACL reconstruction. Scand. J. Med. Sci. Sport. 2010, 20, e12–e19. [Google Scholar] [CrossRef]
- Salgarello, M.; Visconti, G.; Barone-Adesi, L. Interlocking circumareolar suture with undyed polyamide thread: A personal experience. Aesthetic Plast. Surg. 2013, 37, 1061–1062. [Google Scholar] [CrossRef]
- Dingenen, B.; Janssens, L.; Luyckx, T.; Claes, S.; Bellemans, J.; Staes, F.F. Postural stability during the transition from double-leg stance to single-leg stance in anterior cruciate ligament injured subjects. Clin. Biomech. 2015, 30, 283–289. [Google Scholar] [CrossRef]
- Simoneau, G.G.; Wilk, K.E. The Challenge of Return to Sports for Patients Post-ACL Reconstruction; JOSPT, Inc.: Alexandria, VA, USA, 2012. [Google Scholar]
- Øiestad, B.E.; Holm, I.; Aune, A.K.; Gunderson, R.; Myklebust, G.; Engebretsen, L.; Aarsland Fosdahl, M.; Risberg, M.A. Knee function and prevalence of knee osteoarthritis after anterior cruciate ligament reconstruction: A prospective study with 10 to 15 years of follow-up. Am. J. Sport. Med. 2010, 38, 2201–2210. [Google Scholar] [CrossRef]
- Chaudhari, A.M.; Briant, P.L.; Bevill, S.L.; Koo, S.; Andriacchi, T.P. Knee kinematics, cartilage morphology, and osteoarthritis after ACL injury. Med. Sci. Sport. Exerc. 2008, 40, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Gokeler, A.; Neuhaus, D.; Benjaminse, A.; Grooms, D.R.; Baumeister, J. Principles of motor learning to support neuroplasticity after ACL injury: Implications for optimizing performance and reducing risk of second ACL Injury. Sport. Med. 2019, 49, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, N.; Harbourne, R.T.; Cavanaugh, J.T. Optimal movement variability: A new theoretical perspective for neurologic physical therapy. J. Neurol. Phys. Ther. 2006, 30, 120–129. [Google Scholar] [CrossRef]
- Schöllhorn, W.I.; Beckmann, H.; Michelbrink, M.; Sechelmann, M.; Trockel, M.; Davids, K. Does noise provide a basis for the unification of motor learning theories? Int. J. Sport Psychol. 2006, 37, 186. [Google Scholar]
- Kal, E.; Prosée, R.; Winters, M.; Van Der Kamp, J. Does implicit motor learning lead to greater automatization of motor skills compared to explicit motor learning? a systematic review. PLoS ONE 2018, 13, e0203591. [Google Scholar] [CrossRef] [PubMed]
- Ghanati, H.A.; Letafatkar, A.; Shojaedin, S.; Hadadnezhad, M.; Schöllhorn, W.I. Comparing the Effects of Differential Learning, Self-Controlled Feedback, and External Focus of Attention Training on Biomechanical Risk Factors of Anterior Cruciate Ligament (ACL) in Athletes: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 10052. [Google Scholar] [CrossRef]
- Schöllhorn, W.I. Individualität-ein vernachlässigter Parameter. Leistungssport 1999, 29, S5–S12. [Google Scholar]
- Liao, C.-M.; Masters, R.S.W. Analogy learning: A means to implicit motor learning. J. Sport. Sci. 2001, 19, 307–319. [Google Scholar] [CrossRef]
- Maxwell, J.P.; Masters, R.S.W.; Kerr, E.; Weedon, E. The implicit benefit of learning without errors. Q. J. Exp. Psychol. Sect. A 2001, 54, 1049–1068. [Google Scholar] [CrossRef]
- Schöllhorn, W.I.; Horst, F. Effects of complex movements on the brain as a result of increased decision-making. J. Complex. Health Sci. 2019, 2, 40–45. [Google Scholar]
- Schöllhorn, W.I.; Mayer-Kress, G.; Newell, K.M.; Michelbrink, M. Time scales of adaptive behavior and motor learning in the presence of stochastic perturbations. Hum. Mov. Sci. 2009, 28, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Henz, D.; Schöllhorn, W.I. Differential training facilitates early consolidation in motor learning. Front. Behav. Neurosci. 2016, 10, 199. [Google Scholar] [CrossRef] [PubMed]
- Henz, D.; John, A.; Merz, C.; Schöllhorn, W.I. Post-task effects on EEG brain activity differ for various differential learning and contextual interference protocols. Front. Hum. Neurosci. 2018, 12, 19. [Google Scholar] [CrossRef] [PubMed]
- Schöllhorn, W.I.; Rizzi, N.; Slapšinskaitė-Dackevičienė, A.; Leite, N. Always Pay Attention to Which Model of Motor Learning You Are Using. Int. J. Environ. Res. Public Health 2022, 19, 711. [Google Scholar] [CrossRef] [PubMed]
- Schöllhorn, W.I.; Bauer, H.U. Identifying Individual Movement Styles in High Performance Sports by Means of Self-Organizing Kohonen Maps; International Society of Biomechanics in Sports (ISBS); University Press Konstanz: Konstanz, Germany, 1998. [Google Scholar]
- Apidogo, J.B.; Burdack, J.; Schöllhorn, W.I. Learning Multiple Movements in Parallel—Accurately and in Random Order, or Each with Added Noise? Int. J. Environ. Res. Public Health 2022, 19, 10960. [Google Scholar] [CrossRef]
- Nitsch, J.R.; Hackfort, D. Stress in Schule und Hochschule-eine handlungspsychologische Funktionsanalyse. In Stress-Theorien Untersuchungen Müssnahmen; Huber: Bern, Switzerland, 1981; pp. 263–311. [Google Scholar]
- Hackfort, D. Commentary on “Towards a Grand Unified Theory of sports performance”. Hum. Mov. Sci. 2017, 56, 166–168. [Google Scholar] [CrossRef]
- von Cube, F. Kybernetische Grundlagen des Lernens und Lehrens; Klett: Stuttgart, Germany, 1965. [Google Scholar]
- Schöllhorn, W.I.; Beckmann, H.; Davids, K. Exploiting system fluctuations. Differential training in physical prevention and rehabilitation programs for health and exercise. Medicina 2010, 46, 365. [Google Scholar] [CrossRef] [PubMed]
- Repšaitė, V.; Vainoras, A.; Berškienė, K.; Baltaduonienė, D.; Daunoravičienė, A.; Sendžikaitė, E. Results of the pilot study. Neurol. Neurochir. Pol. 2015, 49, 150–155. [Google Scholar] [CrossRef]
- Rosset-Llobet, J.; Fàbregas-Molas, S. Rehabilitation and Plasticity of Task-Specific Focal Hand Dystonia; Treat, D., Dressler, D., Altenmüller, E., Krauss, J.K., Eds.; 2018; pp. 256–260. [Google Scholar]
- Kurz, J.; Gosenheimer, A.; Schumann-Schmid, B.; Steinmetz, F.; Schöllhorn, W.I. Differenzielles Gangtraining in der stationären Rehabilitation bei Knie-oder Hüft-TEP. BG Beweg. Gesundh. 2016, 32, 221–225. [Google Scholar] [CrossRef]
- Quaney, B.M.; He, J.; Timberlake, G.; Dodd, K.; Carr, C. Visuomotor training improves stroke-related ipsilesional upper extremity impairments. Neurorehabil. Neural Repair 2010, 24, 52–61. [Google Scholar] [CrossRef]
- Eng, K.; Siekierka, E.; Pyk, P.; Chevrier, E.; Hauser, Y.; Cameirao, M.; Holper, L.; Hägni, K.; Zimmerli, L.; Duff, A. Interactive visuo-motor therapy system for stroke rehabilitation. Med. Biol. Eng. Comput. 2007, 45, 901–907. [Google Scholar] [CrossRef]
- Bigsby, K.; Mangine, R.E.; Clark, J.F.; Rauch, J.T.; Bixenmann, B.; Susaret, A.W.; Hasselfeld, K.A.; Colosimo, A.J. Effects of postural control manipulation on visuomotor training performance: Comparative data in healthy athletes. Int. J. Sport. Phys. Ther. 2014, 9, 436. [Google Scholar]
- Grooms, D.; Appelbaum, G.; Onate, J. Neuroplasticity following anterior cruciate ligament injury: A framework for visual-motor training approaches in rehabilitation. J. Orthop. Sport. Phys. Ther. 2015, 45, 381–393. [Google Scholar] [CrossRef]
- Wohl, T.R.; Criss, C.R.; Grooms, D.R. Visual perturbation to enhance return to sport rehabilitation after anterior cruciate ligament injury: A clinical commentary. Int. J. Sport. Phys. Ther. 2021, 16, 552. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9. [Google Scholar] [CrossRef]
- Shrestha, B.; Dunn, L. The declaration of Helsinki on medical research involving human subjects: A review of seventh revision. J. Nepal Health Res. Counc. 2019, 17, 548–552. [Google Scholar] [CrossRef]
- Sturgill, L.P.; Snyder-Mackler, L.; Manal, T.J.; Axe, M.J. Interrater reliability of a clinical scale to assess knee joint effusion. J. Orthop. Sport. Phys. Ther. 2009, 39, 845–849. [Google Scholar] [CrossRef]
- Meierbachtol, A.; Yungtum, W.; Paur, E.; Bottoms, J.; Chmielewski, T.L. Psychological and functional readiness for sport following advanced group training in patients with anterior cruciate ligament reconstruction. J. Orthop. Sport. Phys. Ther. 2018, 48, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Padua, D.A.; DiStefano, L.J.; Beutler, A.I.; de la Motte, S.J.; DiStefano, M.J.; Marshall, S.W. The Landing Error Scoring System as a Screening Tool for an Anterior Cruciate Ligament Injury–Prevention Program in Elite-Youth Soccer Athletes. J. Athl. Train. 2015, 50, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Pavan, D.; Morello, F.; Monachino, F.; Rovere, G.; Camarda, L.; Pitarresi, G. Similar biomechanical properties of four tripled tendon graft models for ACL reconstruction. Arch. Orthop. Trauma Surg. 2021, 142, 1155–1165. [Google Scholar] [CrossRef]
- Bosco, F.; Giustra, F.; Crivellaro, M.; Via, R.G.; Lavia, A.D.; Capella, M.; Sabatini, L.; Risitano, S.; Rovere, G.; Massè, A. Is augmentation the best solution in partial anterior cruciate ligament tears? A literature systematic review and meta-analysis. J. Orthop. 2022, 36, 11–17. [Google Scholar] [CrossRef]
- Camarda, L.; Pitarresi, G.; Moscadini, S.; Marannano, G.; Sanfilippo, A.; D’Arienzo, M. Effect of suturing the femoral portion of a four-strand graft during an ACL reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Sheikhi, B.; Letafatkar, A.; Thomas, A.C.; Ford, K.R. Altered trunk and lower extremity movement coordination after neuromuscular training with and without external focus instruction: A randomized controlled trial. BMC Sport. Sci. Med. Rehabil. 2021, 13, 92. [Google Scholar] [CrossRef] [PubMed]
- Dingenen, B.; Truijen, J.; Bellemans, J.; Gokeler, A. Test–retest reliability and discriminative ability of forward, medial and rotational single-leg hop tests. Knee 2019, 26, 978–987. [Google Scholar] [CrossRef]
- Munro, A.G.; Herrington, L.C. Between-session reliability of the star excursion balance test. Phys. Ther. Sport 2010, 11, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Hertel, J. Considerations for normalizing measures of the Star Excursion Balance Test. Meas. Phys. Educ. Exerc. Sci. 2003, 7, 89–100. [Google Scholar] [CrossRef]
- Nagelli, C.V.; Di Stasi, S.; Wordeman, S.C.; Chen, A.; Tatarski, R.; Hoffman, J.; Hewett, T.E. Knee biomechanical deficits during a single-leg landing task are addressed with neuromuscular training in anterior cruciate ligament–reconstructed athletes. Clin. J. Sport Med. 2021, 31, e347–e353. [Google Scholar] [CrossRef]
- Harriman, S.L.; Patel, J. When are clinical trials registered? An analysis of prospective versus retrospective registration. Trials 2016, 17, 187. [Google Scholar] [CrossRef]
- Wilkins, L.; Appelbaum, L.G. An early review of stroboscopic visual training: Insights, challenges and accomplishments to guide future studies. Int. Rev. Sport Exerc. Psychol. 2020, 13, 65–80. [Google Scholar] [CrossRef]
- Welling, W.; Benjaminse, A.; Gokeler, A.; Otten, B. Enhanced retention of drop vertical jump landing technique: A randomized controlled trial. Hum. Mov. Sci. 2016, 45, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Stensrud, S.; Myklebust, G.; Kristianslund, E.; Bahr, R.; Krosshaug, T. Correlation between two-dimensional video analysis and subjective assessment in evaluating knee control among elite female team handball players. Br. J. Sport. Med. 2011, 45, 589–595. [Google Scholar] [CrossRef]
- Oftadeh, S.; Bahram, A.; Yaali, R.; Ghadiri, F.; Schöllhorn, W.I. External Focus or Differential Learning: Is There an Additive Effect on Learning a Futsal Goal Kick? Int. J. Environ. Res. Public Health 2021, 19, 317. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S. Communication and motor skill learning: What we learn from research in the gymnasium. Quest 1994, 46, 345–355. [Google Scholar] [CrossRef]
- Fuchs, P.X.; Fusco, A.; Bell, J.W.; von Duvillard, S.P.; Cortis, C.; Wagner, H. Effect of differential training on female volleyball spike-jump technique and performance. Int. J. Sport. Physiol. Perform. 2020, 15, 1019–1025. [Google Scholar] [CrossRef]
- Newell, K.M. Schema theory (1975): Retrospectives and prospectives. Res. Q. Exerc. Sport 2003, 74, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Dhawale, A.K.; Smith, M.A.; Ölveczky, B.P. The role of variability in motor learning. Annu. Rev. Neurosci. 2017, 40, 479–498. [Google Scholar] [CrossRef]
- Kotsifaki, A.; Korakakis, V.; Whiteley, R.; Van Rossom, S.; Jonkers, I. Measuring only hop distance during single leg hop testing is insufficient to detect deficits in knee function after ACL reconstruction: A systematic review and meta-analysis. Br. J. Sport. Med. 2020, 54, 139–153. [Google Scholar] [CrossRef]
- Tran, A.A.; Gatewood, C.; Harris, A.H.S.; Thompson, J.A.; Dragoo, J.L. The effect of foot landing position on biomechanical risk factors associated with anterior cruciate ligament injury. J. Exp. Orthop. 2016, 3, 13. [Google Scholar] [CrossRef]
- Zebis, M.K.; Andersen, L.L.; Brandt, M.; Myklebust, G.; Bencke, J.; Lauridsen, H.B.; Bandholm, T.; Thorborg, K.; Hölmich, P.; Aagaard, P. Effects of evidence-based prevention training on neuromuscular and biomechanical risk factors for ACL injury in adolescent female athletes: A randomised controlled trial. Br. J. Sport. Med. 2016, 50, 552–557. [Google Scholar] [CrossRef]
- Bosco, F.; Giustra, F.; Giai Via, R.; Lavia, A.D.; Capella, M.; Sabatini, L.; Risitano, S.; Cacciola, G.; Vezza, D.; Massè, A. Could anterior closed-wedge high tibial osteotomy be a viable option in patients with high posterior tibial slope who undergo anterior cruciate ligament reconstruction? A systematic review and meta-analysis. Eur. J. Orthop. Surg. Traumatol. 2022, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ghanati, H.A.; Letafatkar, A.; Almonroeder, T.G.; Rabiei, P. Examining the Influence of Attentional Focus on the Effects of a Neuromuscular Training Program in Male Athletes. J. Strength Cond. Res. 2020, 36, 1568–1575. [Google Scholar] [CrossRef]
- Dobija, L.; Reynaud, V.; Pereira, B.; Van Hille, W.; Descamps, S.; Bonnin, A.; Coudeyre, E. Measurement properties of the Star Excursion Balance Test in patients with ACL deficiency. Phys. Ther. Sport 2019, 36, 7–13. [Google Scholar] [CrossRef]
- Michelbrink, M.; Schöllhorn, W.I. 22.23 Differencial learning and random walk analysis inhuman balance. Gait Posture 2005, 21, S148–S149. [Google Scholar] [CrossRef]
- Wind, J.; Horst, F.; Rizzi, N.; John, A.; Schöllhorn, W.I. Electrical brain activity and its functional connectivity in the physical execution of modern jazz dance. Front. Psychol. 2020, 11, 586076. [Google Scholar] [CrossRef]
- John, A.T.; Barthel, A.; Wind, J.; Rizzi, N.; Schöllhorn, W.I. Acute Effects of Various Movement Noise in Differential Learning of Rope Skipping on Brain and Heart Recovery Analyzed by Means of Multiscale Fuzzy Measure Entropy. Front. Behav. Neurosci. 2022, 16, 20. [Google Scholar] [CrossRef]
- Grooms, D.R.; Chaudhari, A.; Page, S.J.; Nichols-Larsen, D.S.; Onate, J.A. Visual-motor control of drop landing after anterior cruciate ligament reconstruction. J. Athl. Train. 2018, 53, 486–496. [Google Scholar] [CrossRef]
- Appelbaum, L.G.; Schroeder, J.E.; Cain, M.S.; Mitroff, S.R. Improved visual cognition through stroboscopic training. Front. Psychol. 2011, 2, 276. [Google Scholar] [CrossRef]
- Appelbaum, L.G.; Cain, M.S.; Schroeder, J.E.; Darling, E.F.; Mitroff, S.R. Stroboscopic visual training improves information encoding in short-term memory. Atten. Percept. Psychophys. 2012, 74, 1681–1691. [Google Scholar] [CrossRef]
- Dale, R.B.; Gollapalli, R.P.; Price, T.; Megahee, K.; Duncan, M.; Tolstick, N.; Ford, L. The effect of visual perturbation upon femoral acceleration during the single and bilateral squat. Phys. Ther. Sport 2017, 27, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Mitroff, S.R.; Friesen, P.; Bennett, D.; Yoo, H.; Reichow, A.W. Enhancing ice hockey skills through stroboscopic visual training: A pilot study. Athl. Train. Sport. Health Care 2013, 5, 261–264. [Google Scholar] [CrossRef]
- Wilkins, L.; Gray, R. Effects of stroboscopic visual training on visual attention, motion perception, and catching performance. Percept. Mot. Skills 2015, 121, 57–79. [Google Scholar] [CrossRef] [PubMed]
- Hülsdünker, T.; Rentz, C.; Ruhnow, D.; Käsbauer, H.; Strüder, H.K.; Mierau, A. The effect of 4-week stroboscopic training on visual function and sport-specific visuomotor performance in top-level badminton players. Int. J. Sport. Physiol. Perform. 2019, 14, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Scherzer, C.B.; Brewer, B.W.; Cornelius, A.E.; Van Raalte, J.L.; Petitpas, A.J.; Sklar, J.H.; Pohlman, M.H.; Krushell, R.J.; Ditmar, T.D. Psychological skills and adherence to rehabilitation after reconstruction of the anterior cruciate ligament. J. Sport Rehabil. 2001, 10, 165–172. [Google Scholar] [CrossRef]
- Scott, C.E.H.; Howie, C.R.; MacDonald, D.; Biant, L.C. Predicting dissatisfaction following total knee replacement: A prospective study of 1217 patients. J. Bone Joint Surg. Br. 2010, 92, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Culliton, S.E.; Bryant, D.M.; Overend, T.J.; MacDonald, S.J.; Chesworth, B.M. The relationship between expectations and satisfaction in patients undergoing primary total knee arthroplasty. J. Arthroplasty 2012, 27, 490–492. [Google Scholar] [CrossRef]
- Waljee, J.; McGlinn, E.P.; Sears, E.D.; Chung, K.C. Patient expectations and patient-reported outcomes in surgery: A systematic review. Surgery 2014, 155, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Pizzari, T.; McBurney, H.; Taylor, N.F.; Feller, J.A. Adherence to anterior cruciate ligament rehabilitation: A qualitative analysis. J. Sport Rehabil. 2002, 11, 90–102. [Google Scholar] [CrossRef]
- Chaput, M.; Ness, B.M.; Lucas, K.; Zimney, K.J. A Multi-Systems Approach to Human Movement after ACL Reconstruction: The Nervous System. Int. J. Sport. Phys. Ther. 2022, 17, 47–59. [Google Scholar] [CrossRef]
- Swanik, C.B.; Covassin, T.; Stearne, D.J.; Schatz, P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. Am. J. Sport. Med. 2007, 35, 943–948. [Google Scholar] [CrossRef]
- Avedesian, J.M.; Forbes, W.; Covassin, T.; Dufek, J.S. Influence of cognitive performance on musculoskeletal injury risk: A systematic review. Am. J. Sport. Med. 2022, 50, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Michelbrink, M.; Schöllhorn, W.I. Changes in noise structure by learning a balancing tasks. J. Biomech. 2006, 39, S483. [Google Scholar] [CrossRef]
- Halperin, I.; Chapman, D.W.; Martin, D.T.; Abbiss, C.; Wulf, G. Coaching cues in amateur boxing: An analysis of ringside feedback provided between rounds of competition. Psychol. Sport Exerc. 2016, 25, 44–50. [Google Scholar] [CrossRef]
- Porter, J.M.; Nolan, R.P.; Ostrowski, E.J.; Wulf, G. Directing attention externally enhances agility performance: A qualitative and quantitative analysis of the efficacy of using verbal instructions to focus attention. Front. Psychol. 2010, 1, 216. [Google Scholar] [CrossRef]
- Durham, K.; Van Vliet, P.M.; Badger, F.; Sackley, C. Use of information feedback and attentional focus of feedback in treating the person with a hemiplegic arm. Physiother. Res. Int. 2009, 14, 77–90. [Google Scholar] [CrossRef]
- Hunt, C.; Paez, A.; Folmar, E. The impact of attentional focus on the treatment of musculoskeletal and movement disorders. Int. J. Sport. Phys. Ther. 2017, 12, 901. [Google Scholar] [CrossRef]
- Wulf, G.; Lauterbach, B.; Toole, T. The learning advantages of an external focus of attention in golf. Res. Q. Exerc. Sport 1999, 70, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.D.; Thomson, N.; Buchanan, M. Word length and the structure of short-term memory. J. Verbal Learn. Verbal Behav. 1975, 14, 575–589. [Google Scholar] [CrossRef]
- Baddeley, A.D.; Hitch, G.J.; Allen, R.J. From short-term store to multicomponent working memory: The role of the modal model. Mem. Cognit. 2019, 47, 575–588. [Google Scholar] [CrossRef]
- Schollhorn, I.W.; Hegen, P.; Davids, K. The nonlinear nature of learning-A differential learning approach. Open Sport. Sci. J. 2012, 5. [Google Scholar] [CrossRef]
- Holm, I.; Fosdahl, M.A.; Friis, A.; Risberg, M.A.; Myklebust, G.; Steen, H. Effect of neuromuscular training on proprioception, balance, muscle strength, and lower limb function in female team handball players. Clin. J. Sport Med. 2004, 14, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, M.; Letafatkar, A.; Thomas, A.C.; Keyhani, S. Effects of a neuromuscular training program using external focus attention cues in male athletes with anterior cruciate ligament reconstruction: A randomized clinical trial. BMC Sport. Sci. Med. Rehabil. 2021, 13, 49. [Google Scholar] [CrossRef] [PubMed]
- Masters, R.S.W.; Poolton, J.M.; Maxwell, J.P.; Raab, M. Implicit motor learning and complex decision making in time-constrained environments. J. Mot. Behav. 2008, 40, 71–79. [Google Scholar] [CrossRef]
- McNevin, N.H.; Wulf, G.; Carlson, C. Effects of attentional focus, self-control, and dyad training on motor learning: Implications for physical rehabilitation. Phys. Ther. 2000, 80, 373–385. [Google Scholar] [CrossRef]
- Kelso, J.A.S. Dynamic Patterns: The Self-Organization of Brain and Behavior; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Schöllhorn, W.I. Practical consequences of systems dynamic approach to technique and strength training. Acta Acad. Olympique Est. 2000, 8, 25–37. [Google Scholar]
- Schöllhorn, W.I. Practical consequences of biomechanically determined individuality and fluctuations on motor learning. In Conference Proceedings of the International Society of Biomechanics; University Press: Calgary, Canada, 1999. [Google Scholar]
- Singer, W. Development and plasticity of cortical processing architectures. Science 1995, 270, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Schöllhorn, W. Systemdynamische Betrachtung Komplexer Bewegungsmuster im Lernprozeß: Prozeßorientierte Strukturierung der Entwicklung Eines Bewegungsablaufs Mit Hilfe biomechanischer Beschreibungsgrößen; Lang: Frankfurt am Main, Germany, 1998. [Google Scholar]
- Smith, L.B.; Thelen, E.E. A dynamic systems approach to development: Applications. In This Book Grew out of a Workshop,” Dynamic Systems in Development,” Held for the Society for Research in Child Development in Kansas City, KS, April 1989; MIT Press: Cambridge, MA, USA, 1993. [Google Scholar]
- Wade, M.G.; Whiting, H.T.A. Motor Development in Children: Aspects of Coordination and Control; Nijhoff: Leiden, The Netherlands, 1986. [Google Scholar]
- Horst, F.; Janssen, D.; Beckmann, H.; Schöllhorn, W.I. Can individual movement characteristics across different throwing disciplines be identified in high-performance decathletes? Front. Psychol. 2020, 11, 2262. [Google Scholar] [CrossRef]
- Aragonés, D.; Eekhoff, A.; Horst, F.; Schöllhorn, W.I. Fatigue-related changes in technique emerge at different timescales during repetitive training. J. Sport. Sci. 2018, 36, 1296–1304. [Google Scholar] [CrossRef]
- Burdack, J.; Horst, F.; Aragonés, D.; Eekhoff, A.; Schöllhorn, W.I. Fatigue-related and timescale-dependent changes in individual movement patterns identified using support vector machine. Front. Psychol. 2020, 11, 551548. [Google Scholar] [CrossRef]
- Horst, F.; Mildner, M.; Schöllhorn, W.I. One-year persistence of individual gait patterns identified in a follow-up study–A call for individualised diagnose and therapy. Gait Posture 2017, 58, 476–480. [Google Scholar] [CrossRef]
- Horst, F.; Eekhoff, A.; Newell, K.M.; Schöllhorn, W.I. Intra-individual gait patterns across different time-scales as revealed by means of a supervised learning model using kernel-based discriminant regression. PLoS ONE 2017, 12, e0179738. [Google Scholar] [CrossRef] [PubMed]
- Horst, F.; Kramer, F.; Schäfer, B.; Eekhoff, A.; Hegen, P.; Nigg, B.M.; Schöllhorn, W.I. Daily changes of individual gait patterns identified by means of support vector machines. Gait Posture 2016, 49, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Newell, K.M.; McDonald, P.V. Searching for Solutions to the Coordination Function: Learning as Exploratory Behavior; Tutorials in motor behavior: North-Holland, The Netherlands, 1992. [Google Scholar]
- Pacheco, M.M.; Lafe, C.W.; Newell, K.M. Search strategies in the perceptual-motor workspace and the acquisition of coordination, control, and skill. Front. Psychol. 2019, 10, 1874. [Google Scholar] [CrossRef]
- Koffka, K. Perception: An introduction to the Gestalt-Theorie. Psychol. Bull. 1922, 19, 531. [Google Scholar] [CrossRef]
- Newell, K.M. Constraints on the development of coordination. In Motor Development on Children: Aspects of Coordination and Control; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 1986. [Google Scholar]
- Mosston, M. Inclusion and exclusion in education—II. Innov. Curric. Des. Phys. Educ. 1969. [Google Scholar]
- Behzadnia, B.; Mohammadzadeh, H.; Ahmadi, M. Autonomy-supportive behaviors promote autonomous motivation, knowledge structures, motor skills learning and performance in physical education. Curr. Psychol. 2019, 38, 1692–1705. [Google Scholar] [CrossRef]
- Fisher, R. Statistical methods and scientific induction. J. R. Stat. Soc. Ser. B 1955, 17, 69–78. [Google Scholar] [CrossRef]
- Neyman, J.; Pearson, E.S., IX. On the problem of the most efficient tests of statistical hypotheses. Philos. Trans. R. Soc. London. Ser. A Contain. Pap. Math. Phys. Character 1933, 231, 289–337. [Google Scholar]
- Stegmüller, W. Personelle und Statistische Wahrscheinlichkeit [Personal and Statistical Probability] Probleme und Resultate der Wissenschaftstheorie und Analytischen Philosophie [Problems and Results of Philosophy of Science and Analytical Philosophy]; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 1973. [Google Scholar]
- Nuzzo, R. Statistical errors: P values, the’gold standard’of statistical validity, are not as reliable as many scientists assume. Nature 2014, 506, 150–153. [Google Scholar] [CrossRef]
- Gigerenzer, G. Mindless statistics. J. Socio. Econ. 2004, 33, 587–606. [Google Scholar] [CrossRef]
- Weiss, W.M.; Uguento, A.M.; Mahmooth, Z.; Murray, L.K.; Hall, B.J.; Nadison, M.; Rasmussen, A.; Lee, J.S.; Vazzano, A.; Bass, J. Mental health interventions and priorities for research for adult survivors of torture and systematic violence: A review of the literature. Torture J. 2016, 26, 27. [Google Scholar] [CrossRef]


{kind=link}
| Groups | DL (n = 15) | VMT (n = 15) | Control (n = 15) | p-Value * |
|---|---|---|---|---|
| Age (years) | 28.8 (4.6) | 29.1 (3.7) | 27.9 (2.9) | 0.673 |
| Mass (kg) | 78.4 (6) | 77 (4.8) | 79 (4.9) | 0.566 |
| Height (cm) | 175.2 (4.7) | 174 (4.6) | 174.3 (3.9) | 0.710 |
| Body mass index (kg/m2) | 22.4 (1.9) | 22.1 (1.4) | 22.6 (1.5) | 0.649 |
| Time since surgery (months) | 8.5 (1.1) | 8.8 (1.2) | 7.8 (1.5) | 0.392 |
| Internal Variants: | External Variants: |
|---|---|
| Cognition/Coordination-oriented Before jumping: - 2–3 bunny hops - skipping both/left/right leg - high knees both/left/right knee - butt-kicks both/left/right leg - zigzag - shuffle to the left, right - complete turn to left/right before you jump While jumping: - arms crossing in front of the chest, behind the back, - raise both/left/right arm - circle both/left/right arm - head to left/right - close left/right eye While landing: - one arm in front and the other arm behind - landing with a very wide/narrow stance - landing on toes Metabolism/Mentally oriented: Fatigue: - With—Without | With primary stimulations of sensory system (apperception): Visual: - in a virtual reality - environment Somatosensory: - exercise on sand - with or without shoes Proprioceptive: - exercise in dark - with weight vest Acoustic: - loud music - noise from the audience |
| Exercise | Visual Cues | |
|---|---|---|
| Tap-test | Tap the cones Acoustic Cue | The Tap-test requires the athlete to run 10 m to tap a cone, cut to the right or left for 5 m to tap another cone, cut to the opposite direction for 10 m to tap the third cone, return to the center by cutting 5 m to tap the first cone and then run 10 m back to the start position—thereby running in a “T” formation). A modification that increases the difficulty of this task and simulates the cognitive demands of sport is to have the clinician call out “Left” or “Right” to indicate which direction the athlete should cut prior to reaching the first cone, thereby creating an unanticipated cutting task which has been previously associated with increased injury-risk biomechanics compared to anticipated trials. |
| Agility Ladder Drills | The confines of the ladder | Agility ladder drills require athletes to match specific foot-placement patterns within an agility ladder context. |
| Single-leg Deadlifts | Place an object by the cone(s) | Single-leg deadlifts may be modified by requiring athletes to gently place a small object on the ground next to a cone target. To increase the difficulty, multiple cones can be placed at different angles within the athlete’s field of view, set at distances equal to his or her max volitional reaching distance while standing on one leg. For example, if the clinician chooses to use three targets, then he or she may call out “Left”, “Center”, or “Right” to vary the task order and difficulty. |
| Single-leg Stance (on foam) | Hold the bar horizontally | Single-leg stance on a foam surface may be modified by having the participant hold a light-weight bar with an outstretched arm and focus on keeping it steadily horizontal |
| Vertical Jumps | Hit the overhead target | The VERTEC is a therapeutic tool that assesses maximum vertical jump height by requiring athletes to jump and hit an overhead target. While using the VERTEC to have athletes hit the mark equal to 80% of their maximal jump height, clinicians may call out “Left” or “Right” during the initial flight phase of the jump to signal to the athlete to unilaterally land on his or her left or right leg. The use of spontaneous cuing creates an unanticipated landing task, which has been previously associated with increased injury-risk biomechanics compared to anticipated landing. |
| Squat Jumps | Land facing the cones | Jump squats may be modified by placing four cones around the participant at 0, 90, 180, and 270-degree positions. After numbering each cone one through four, the clinician may then rapidly call out cues to the athlete to specify which cone they should face after each jump squat. To increase the difficulty of this cognitive challenge, the clinician can introduce more cones or increase the rapidity of cuing. |
| Exercise | Error Count |
|---|---|
| T-test | Miss a cone Cut to the wrong direction |
| Agility Ladder Drills | Hit the ladder Incorrect foot placement |
| Single-leg Deadlifts | Opposite foot touches ground Either hand touches ground Object placed in wrong location |
| Single-leg Stance (on foam) | Opposite foot touches ground Either hand touches ground |
| Vertical Jumps | Miss the target Land on wrong foot |
| Squat Jumps | Land facing wrong orientation |
| Variable | Group | Pre-Test Mean ± SD | Post-Test Mean ± SD | ES (CI95%) † | p Value | ||
|---|---|---|---|---|---|---|---|
| Main Effect of Time | Main Effect of Group | Group × Time Interaction | |||||
| Triple hop test (cm) | DL | 457.3 ± 51.2 | 531.3 ± 74.4 ‡ § | 1.15 ! (0.06 to 2.25) | F = 16.226 p < 0.001 * | F = 2.609 p < 0.085 | F = 3.861 p < 0.029 * |
| VMT | 456.4 ± 54 | 517.6 ± 78.9 ‡ | 0.90 ! (−0.15 to 1.96) | ||||
| Control | 455.6 ± 51 | 457.4 ± 51.1 | 0.03 (−0.97 to 1.04) | ||||
| Variables (cm) | Group | Pre-Test Mean ± SD | 8-Weeks Mean ± SD | ES (CI95%) † | p Value | ||
|---|---|---|---|---|---|---|---|
| Main Effect of Time | Main Effect of Group | Group × Time Interaction | |||||
| Anterior | DL | 80.6 ± 3.9 | 89.5 ± 1.9 ‡ § | 2.90 ! (1.45 to 4.35) | F = 170.914 p < 0.001 * | F = 13.324 p < 0.001 * | F = 25.849 p < 0.001 * |
| VMT | 80.4 ± 3.2 | 88.8 ± 1.4 ‡ § | 3.40 ! (1.81 to 4.98) | ||||
| Control | 80.1 ± 3 | 81.5 ± 3.2 | 0.45 (−0.57 to 1.47) | ||||
| Anteromedial | DL | 81.8 ± 5 | 90.1 ± 3.4 ‡ § | 1.94 ! (0.71 to 3.16) | F = 48.253 p < 0.001 * | F = 6.221 p < 0.004 * | F = 9.617 p < 0.001 * |
| VMT | 82.2 ± 4.8 | 89.8 ± 3.2 ‡ § | 1.86 ! (0.65 to 3.07) | ||||
| Control | 82.5 ± 4.5 | 83.4 ± 3.9 | 0.21 (−0.80 to 1.22) | ||||
| Medial | DL | 81.8 ± 5 | 90.1 ± 3.4 ‡ | 1.94 ! (0.71 to 3.16) | F = 74.274 p < 0.001 * | F = 3.514 p < 0.039 * | F = 13.337 p < 0.001 * |
| VMT | 82.2 ± 4.8 | 89.8 ± 3.2 ‡ | 1.86 ! (0.65 to 3.07) | ||||
| Control | 82.5 ± 4.5 | 83.4 ± 3.9 | 0.21 (−0.80 to 1.22) | ||||
| Posteromedial | DL | 78.7 ± 3.1 | 89 ± 4.4 ‡ § | 2.70 ! (1.30 to 4.10) | F = 162.347 p < 0.001 * | F = 12.205 p < 0.001 * | F = 31.295 p < 0.001 * |
| VMT | 78.7 ± 3.1 | 87.8 ± 3.2 ‡ § | 2.88 ! (1.44 to 4.33) | ||||
| Control | 78.7 ± 3.1 | 79.6 ± 2.9 | 0.30 (−0.26 to 1.83) | ||||
| Posterior | DL | 82.2 ± 3.3 | 90.1 ± 3.3 ‡ § | 2.39 ! (1.06 to 3.72) | F = 84.773 p < 0.001 * | F = 5.316 p < 0.009 * | F = 16.797 p < 0.013 * |
| VMT | 81.9 ± 3.8 | 89.8 ± 3.3 ‡ § | 2.22 ! (0.93 to 3.50) | ||||
| Control | 82.6 ± 3.7 | 83.2 ± 3.8 | 0.16 (−0.85 to 1.17) | ||||
| Posterolateral | DL | 76.4 ± 3.2 | 87 ± 4 ‡ § | 2.92 ! (1.47 to 4.38) | F = 147.187 p < 0.001 * | F = 10.384 p < 0.001 * | F = 26.928 p < 0.001 * |
| VMT | 76.6 ± 3.3 | 85.9 ± 4 ‡ § | 2.53 ! (1.17 to 3.89) | ||||
| Control | 76.9 ± 3.3 | 78 ± 1.8 | 0.41 (−0.60 to 1.43) | ||||
| Lateral | DL | 74.8 ± 4.6 | 87.6 ± 4.6 ‡ § | 2.78 ! (1.36 to 4.20) | F = 123.620 p < 0.001 * | F = 9.974 p < 0.001 * | F = 23.937 p < 0.001 * |
| VMT | 74.3 ± 4.4 | 85.2 ± 3.7 ‡ § | 2.68 ! (1.28 to 4.07) | ||||
| Control | 75 ± 4 | 76.1 ± 4.6 | 0.25 (−0.76 to 1.27) | ||||
| Anterolateral | DL | 77 ± 4 | 88.6 ± 4 ‡ § | 2.9 ! (1.45 to 4.35) | F = 98.265 p < 0.001 * | F = 10.488 p < 0.001 * | F = 22.583 p < 0.013 * |
| VMT | 78 ± 3.9 | 87.5 ± 4.1 ‡ § | 2.37 ! (1.05 to 3.69) | ||||
| Control | 77.6 ± 4.3 | 78 ± 4.7 | 0.08 (−0.92 to 1.10) | ||||
| Variables | Group | Pre-Test Mean ± SD | 8-Weeks Mean ± SD | ES (CI95%) † | p Value | ||
|---|---|---|---|---|---|---|---|
| Main Effect of Time | Main Effect of Group | Group × Time Interaction | |||||
| Hip flexion (degree) | DL | 55.9 ± 5.5 | 62 ± 6.1 ‡ § | 1.05 ! (−0.29 to 2.13) | F = 31.011 p < 0.001 * | F = 2.979 p < 0.062 | F = 8.386 p < 0.001 * |
| VMT | 50.5 ± 7.7 | 56.6 ± 7.8 ‡ § | 0.78 (−0.26 to 1.83) | ||||
| Control | 51.9 ± 11 | 51.8 ± 11 | −0.00 (−1.02 to 1) | ||||
| KF (degree) | DL | 28.1 ± 7.1 | 39.2 ± 4.5 ‡ § | 1.86 ! (0.65 to 3.08) | F = 55.063 p < 0.001 * | F = 20.632 p < 0.001 * | F = 18.190 p < 0.001 * |
| VMT | 27.8 ± 5.9 | 41.7 ± 3.07 ‡ § | 2.95 ! (1.49 to 4.42) | ||||
| Control | 26.6 ± 4.8 | 25.9 ± 6 | −0.12 (−1.21 to 0.81) | ||||
| AD (degree) | DL | 18.2 ± 1.8 | 23 ± 3.6 ‡ | 1.68 ! (−0.50 to 2.86) | F = 53.829 p < 0.001 * | F = 4.095 p < 0.024 * | F = 8.469 p < 0.001 * |
| VMT | 19.7 ± 1.2 | 25.7 ± 4.3 ‡ | 1.90 ! (0.68 to 3.12) | ||||
| Control | 21.9 ± 2.2 | 22.1 ± 2.2 | 0.09 (−0.61 to 1.43) | ||||
| KV (degree) | DL | −4.9 ± 0.2 | −3.6 ± 0.2 ‡ § | 6.5 ! (3.96 to 9.03) | F = 119.261 p < 0.001 * | F = 53.577 p < 0.001 * | F = 39.136 p < 0.001 * |
| VMT | −5.3 ± 0.4 | −3.8 ± 0.3 ‡ § | 4.24 ! (2.41to 6.06) | ||||
| Control | −5.1 ± 0.4 | −5.2 ± 0.4 | −0.12 (−1.26 to 0.76) | ||||
| VGRF (N) | DL | 3.3 ± 0.2 | 2.8 ± 0.1 ‡ § | −3.16 ! (−4.68 to −1.64) | F = 51.717 p < 0.001 * | F = 8.211 p < 0.001 * | F = 4.870 p < 0.013 * |
| VMT | 3 ± 0.4 | 2.7 ± 0.1 ‡ § | −1.02 ! (−2.10 to 0.04) | ||||
| Control | 3.4 ± 0.4 | 3.3 ± 0.5 | −0.22 (−1.52 to 0.52) | ||||
| Variable | Group | Pre-Test Mean ± SD | 8-Weeks Mean ± SD | ES (CI95%) † | p Value | ||
|---|---|---|---|---|---|---|---|
| Main Effect of Time | Main Effect of Group | Group × Time Interaction | |||||
| TSK test | DL | 37.6 ± 7.3 | 22.6 ± 4.8 ‡ § | −2.42 ! (−3.76 to −1.09) | F = 50.047 p < 0.001 * | F = 3.438 p < 0.029 * | F = 6.154 p < 0.001 * |
| VMT | 38 ± 6.7 | 23.3 ± 4.1 ‡ § | −2.64 ! (−4.03 to −1.26) | ||||
| Control | 37.4 ± 6.5 | 36.2 ± 6.0 | −0.19 (−1.20 to 0.82) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gholami, F.; Letafatkar, A.; Moghadas Tabrizi, Y.; Gokeler, A.; Rossettini, G.; Ghanati, H.A.; Schöllhorn, W.I. Comparing the Effects of Differential and Visuo-Motor Training on Functional Performance, Biomechanical, and Psychological Factors in Athletes after ACL Reconstruction: A Randomized Controlled Trial. J. Clin. Med. 2023, 12, 2845. https://doi.org/10.3390/jcm12082845
Gholami F, Letafatkar A, Moghadas Tabrizi Y, Gokeler A, Rossettini G, Ghanati HA, Schöllhorn WI. Comparing the Effects of Differential and Visuo-Motor Training on Functional Performance, Biomechanical, and Psychological Factors in Athletes after ACL Reconstruction: A Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(8):2845. https://doi.org/10.3390/jcm12082845
Chicago/Turabian StyleGholami, Fatemeh, Amir Letafatkar, Yousef Moghadas Tabrizi, Alli Gokeler, Giacomo Rossettini, Hadi Abbaszadeh Ghanati, and Wolfgang Immanuel Schöllhorn. 2023. "Comparing the Effects of Differential and Visuo-Motor Training on Functional Performance, Biomechanical, and Psychological Factors in Athletes after ACL Reconstruction: A Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 8: 2845. https://doi.org/10.3390/jcm12082845
APA StyleGholami, F., Letafatkar, A., Moghadas Tabrizi, Y., Gokeler, A., Rossettini, G., Ghanati, H. A., & Schöllhorn, W. I. (2023). Comparing the Effects of Differential and Visuo-Motor Training on Functional Performance, Biomechanical, and Psychological Factors in Athletes after ACL Reconstruction: A Randomized Controlled Trial. Journal of Clinical Medicine, 12(8), 2845. https://doi.org/10.3390/jcm12082845