


Kinesio Taping as an Adjunct Therapy in Postoperative Care after Extraction of Impacted Third Lower Molars—A Randomized Pilot Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
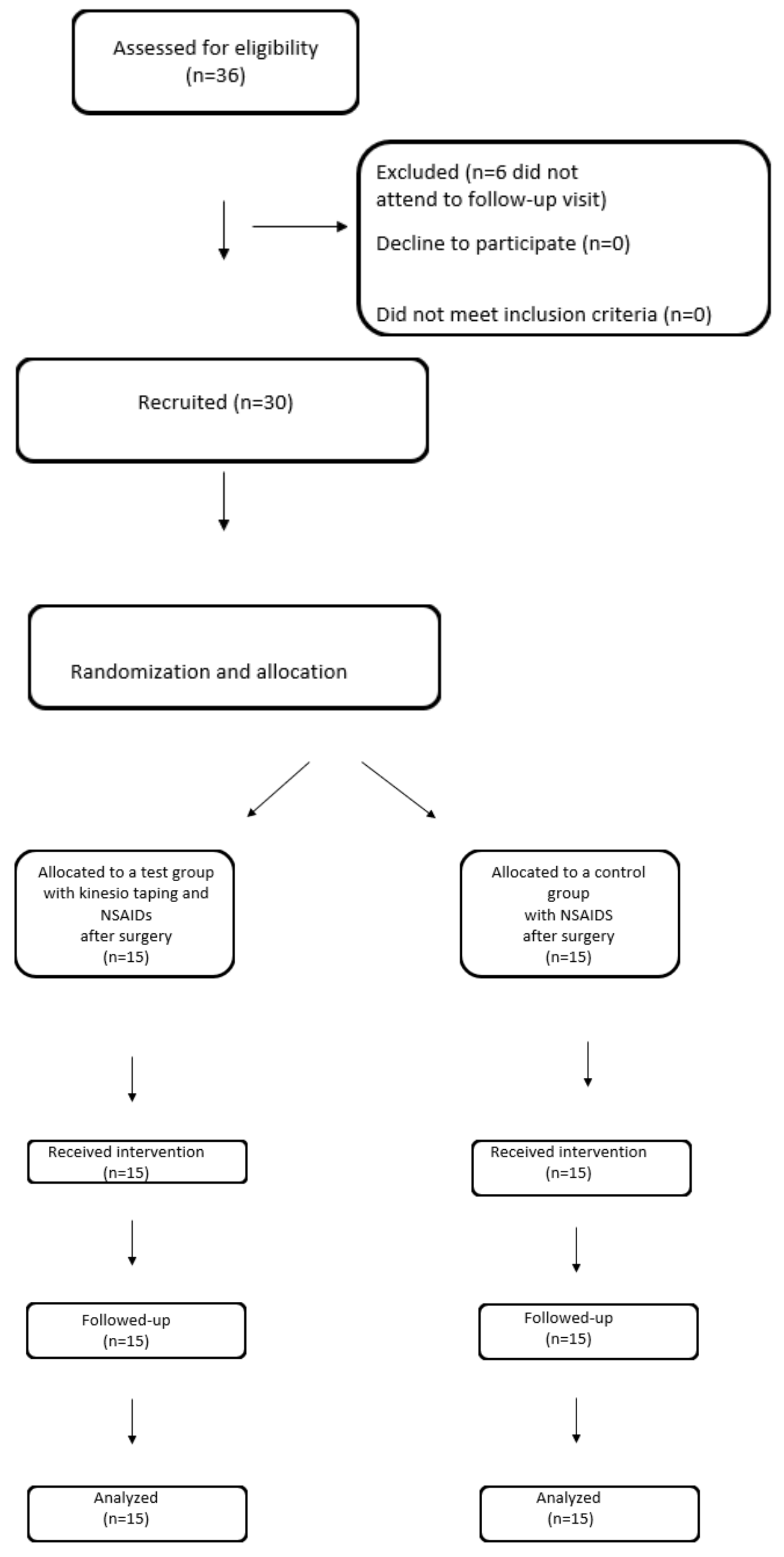
2.1. Participants
2.2. Procedures
2.2.1. Numerical Determination of the Degree of Swelling
2.2.2. Jaw Opening Degree
2.2.3. Assessment of Pain on the VAS Scale
2.2.4. Application of the Kinesio Tape
2.2.5. Post-Surgical NSAID’s Administration
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zandi, M.; Amini, P.; Keshavarz, A. Effectiveness of cold therapy in reducing pain, trismus, and edema after impacted mandibular third molar surgery: A randomized, self-controlled, observer-blind, split-mouth clinical trial. J. Oral. Maxillofac. Surg. 2015, 45, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Poveda Roda, R.; Bagán, J.V.; Jiménez Soriano, Y.; Gallud Romero, L. Use of nonsteroidal antiinflammatory drugs in dental practice: A review. Med. Oral. Patol. Oral. Cir. Bucal. 2007, 12, 10–18. [Google Scholar]
- Woron, J.; Wordliczek, J.; Dobrogowski, J. Comparison of NSAIDs. Med. Po Dyplomie 2020, 6, 55–63. [Google Scholar]
- Crescente, G.; Minervini, G.; Spagnuolo, C.; Moccia, S. Cannabis Bioactive Compound-Based Formulations: New Perspectives for the Management of Orofacial Pain. Molecules 2022, 28, 106. [Google Scholar] [CrossRef] [PubMed]
- di Francesco, F.; Lanza, A.; di Blasio, M.; Vaienti, B.; Cafferata, E.A.; Cervino, G.; Cicciù, M.; Minervini, G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Appl. Sci. 2022, 12, 12409. [Google Scholar] [CrossRef]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic Applications of the Kine-Sio Taping Method, 2nd ed.; Ken Ikai Co. Ltd.: Tokyo, Japan, 2003. [Google Scholar]
- Kase, K.; Hashimoto, T.; Tomoki, O. Development of kinesio taping perfect manual. Kinesio Taping Assoc. 1996, 6, 117–118. [Google Scholar]
- Saavedra-Hernández, M.; Castro-Sánchez, A.M.; Arroyo-Morales, M.; Cleland, J.A.; Lara-Palomo, I.C.; Fernández-de-Las-Peñas, C. Short-term effects of kinesiotaping versus cervical thrust manipulation in patients with mechanical neck pain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2012, 42, 724–730. [Google Scholar] [CrossRef]
- Morris, D.; Jones, D.; Ryan, H.; Ryan, C.G. The clinical effects of Kinesio® Tex taping: A systematic review. Physiother Theory Pract. 2013, 29, 259–270. [Google Scholar] [CrossRef]
- Giray, E.; Karadag-Saygi, E.; Mansiz-Kaplan, B.; Tokgoz, D.; Bayindir, O.; Kayhan, O. A randomized, single-blinded pilot study evaluating the effects of kinesiology taping and the tape application techniques in addition to therapeutic exercises in the treatment of congenital muscular torticollis. Clin. Rehabil. 2017, 31, 1098–1106. [Google Scholar] [CrossRef]
- Medrek, A.; Krol, T.; Michalek-Krol, K.; Dąbrowska-Galas, M. Kinesiotaping and the effect placebo. Med. Rodz. 2017, 4, 304–309. [Google Scholar]
- Wu, W.T.; Hong, C.Z.; Chou, L.W. The Kinesio Taping Method for Myofascial Pain Control. Evid.-Based Complement. Altern. Med. 2015, 2015, 950519. [Google Scholar] [CrossRef] [Green Version]
- Al-Khateeb, T.H.; Nusair, Y. Effect of the proteolytic enzyme serrapeptase on swelling, pain and trismus after surgical extraction of mandibular third molars. Int. J. Oral. Maxillofac. Surg. 2008, 37, 264–268. [Google Scholar] [CrossRef]
- Kim, K.; Brar, P.; Jakubowski, J.; Kaltman, S.; Lopez, E. The use of cortico-steroids and nonsteroidal antiinflammatory medication for the management of pain and inflammation after third molar surgery: A review of the literature. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2009, 107, 630–640. [Google Scholar] [CrossRef]
- Ristow, O.; Pautke, C.; Victoria Kehl Koerdt, S.; Schwärzler, K.; Hahnefeld, L.; Hohlweg-Majert, B. Influence of kinesiologic tape on postoperative swelling, pain and trismus after zygomatico-orbital fractures. J. Craniomaxillofac. Surg. 2014, 42, 469–476. [Google Scholar] [CrossRef]
- Tozzi, U.; Santagata, M.; Sellitto, A.; Tartaro, G.P. Influence of kinesiologic tape on post-operative swelling after orthognathic surgery. J. Maxillofac. Oral. Surg. 2016, 15, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Lietz-Kijak, D.; Kijak, E.; Krajczy, M.; Bogacz, K.; Łuniewski, J.; Szczegielniak, J. The impact of the use of kinesio taping method on the reduction of swell-ing in patients after orthognathic surgery: A pilot study. Med. Sci. Monit. 2018, 24, 3736–3743. [Google Scholar] [CrossRef]
- Coskun Benlidayi, I.; Salimov, F.; Kurkcu, M.; Guzel, R. Kinesio taping for temporomandibular disorders: Single-blind, randomized, controlled trial of effectiveness. J. Back Musculoskelet. Rehabil. 2016, 29, 373–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, Y. Change the myofascial pain and range of motion of the tem-poromandibular joint following kinesio taping of latent myofascial trigger points in the sternocleidomastoid muscle. J. Phys. Ther. Sci. 2014, 26, 1321–1324. [Google Scholar] [CrossRef] [Green Version]
- Keskinruzgar, A.; Kucuk, A.O.; Yavuz, G.Y.; Koparal, M.; Caliskan, Z.G.; Utkun, M. Comparison of kinesio taping and occlusal splint in the management of myofascial pain in patients with sleep bruxism. J. Back Musculoskelet Rehabil. 2019, 32, 1–6. [Google Scholar] [CrossRef]
- Firoozi, P.; Souza, M.R.F.; de Souza, G.M.; Fernandes, I.A.; Galvão, E.L.; Falci, S.G.M. Does kinesio taping reduce pain, swelling, and trismus after mandibular third molar surgery? A systematic review and meta-analysis. Oral. Maxillofac. Surg. 2022, 26, 535–553. [Google Scholar] [CrossRef]
- Qi, J.; Yue, H.; Liu, E.; Chen, G.; Liu, Y.; Chen, J. Effects of Kinesio tape on pain and edema following surgical extraction of the third molar: A meta-analysis and systematic review. J. Back Musculoskelet. Rehabil. 2022, 35, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhu, X.; Guo, J.; Sun, J. Can Kinesio taping improve discomfort after mandibular third molar surgery? A systematic review and meta-analysis. Clin. Oral. Investig. 2021, 25, 5139–5148. [Google Scholar] [CrossRef] [PubMed]
- Tatli, U.; Benlidayi, I.C.; Salimov, F.; Guzel, R. Effectiveness of kinesio taping on postoperative morbidity after impacted mandibular third molar surgery: A prospective, randomized, placebo-controlled clinical study. J. Appl. Oral. Sci. 2020, 28, e20200159. [Google Scholar] [CrossRef]
- Available online: https://www.random.org (accessed on 27 March 2023).
- Wrzoł, M.; Morawiec, T.; Zalejska-Fiolka, J.; Kownacki, P.; Chwalińska, E.; Hampel, A.; Rój, R.; Stránský, J.; Pasz, A.; Niedzielska, I. Evaluation of total oxidant stress and total antioxidant capacity in smoking and non-smoking patients undergoing surgical extraction of third molars. Czas. Stomatol. 2012, 5, 202–208. [Google Scholar]
- Hasegawa, Y.; Terada, K.; Kageyama, I.; Tsuchimochi, T.; Ishikawa, F.; Nakahara, S. Influence of third molar space on angulation and dental arch crowding. Odontology 2013, 101, 22–28. [Google Scholar] [CrossRef]
- Alexander, I. Electronic medical records for the orthopaedic practice. Clin. Orthop. Relat. Res. 2007, 457, 114–119. [Google Scholar] [CrossRef]
- Jamison, R.N.; Gracely, R.H.; Raymond, S.A.; Levine, J.G.; Marino, B.; Herrmann, T.J.; Daly, M.; Fram, D.; Katz, N.P. Comparative study of electronic vs. paper VAS ratings: A randomized, crossover trial using healthy volunteers. Pain 2002, 99, 341–347. [Google Scholar] [CrossRef]
- Younger, J.; McCue, R.; Mackey, S. Pain outcomes: A brief review of instruments and techniques. Curr. Pain Headache Rep. 2009, 13, 39. [Google Scholar] [CrossRef]
- da Rocha Heras, A.C.T.; de Oliveira, D.M.S.; Guskuma, M.H.; de Araújo, M.C.; Fernandes, K.B.P.; da Silva Junior, R.A.; Andraus, R.A.C.; Maia, L.P.; Fernandes, T.M.F. Kinesio taping use to reduce pain and edema after third molar extraction surgery: A randomized con-trolled split-mouth study. J. Craniomaxillofacial Surg. 2020, 48, 127–131. [Google Scholar] [CrossRef]
- Ristow, O.; Hohlweg-Majert, B.; Stürzenbaum, S.R.; Kehl, V.; Koerdt, S.; Hahnefeld, L.; Pautke, C. Therapeutic elastic tape reduces morbidity after wisdom teeth removal–a clinical trial. Clin. Oral. Investig 2014, 18, 1205–1212. [Google Scholar] [CrossRef]
- Ristow, O.; Pautke, C.; Kehl, V.; Koerdt, S.; Hahnefeld, L.; Hohlweg-Majert, B. Kinesiologic taping reduces morbidity after oral and maxillofacial surgery: A pooled analysis. Physiother. Theory Pract. 2014, 30, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Jaroń, A.; Preuss, O.; Grzywacz, E.; Trybek, G. The Impact of Using Kinesio Tape on Non-Infectious Complications after Impacted Mandibular Third Molar Surgery. Int. J. Environ. Res. Public Health 2021, 18, 399. [Google Scholar] [CrossRef] [PubMed]
- Al-Shamiri, H.M.; Shawky, M.; Hassanein, N. Comparative Assessment of Preoperative versus Postoperative Dexamethasone on Postoperative Complications following Lower Third Molar Surgical Extraction. Int. J. Dent. 2017, 2017, 1350375. [Google Scholar] [CrossRef] [Green Version]
- Yurttutan, M.E.; Sancak, K.T. The effect of kinesio taping with the web strip technique on pain, edema, and trismus after impacted mandibular third molar surgery. Niger. J. Clin. Pract. 2020, 23, 1260–1265. [Google Scholar] [CrossRef]
- Gözlüklü, Ö.; Ulu, M.; Gözlüklü, H.Ö.; Yilmaz, N. Comparison of Different Kinesio Taping Techniques After Third Molar Surgery. J. Cranio-Maxillofac. Surg. 2020, 78, 695–704. [Google Scholar] [CrossRef]
- Genc, A.; Cakarer, S.; Yalcin, B.K.; Kilic, B.B.; Isler, S.C.; Keskin, C. A comparative study of surgical drain placement and the use of kinesiologic tape to reduce postoperative morbidity after third molar surgery. Clin. Oral. Investig. 2019, 23, 345–350. [Google Scholar] [CrossRef]
- Erdil, A.; Akbulut, N.; Altan, A.; Demirsoy, M.S. Comparison of the effect of therapeutic elastic bandage, submucosal dexamethasone, or dexketoprofen trometamol on inflammatory symptoms and quality of life following third molar surgery: A randomized clinical trial. Clin. Oral Investig. 2020, 25, 1–9. [Google Scholar] [CrossRef]
- Frank, S. Comparative Analysis of Local Methods of Hypothermia in the Postoperative Period in Dental Surgery. Ph.D. Thesis, Medical University of Warsaw, Warsaw, Poland, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Ganss (A/B/C) | Control | Study | p-Value |
|---|---|---|---|
| A | 3 | 4 | 0.89 |
| B | 6 | 6 | |
| C | 6 | 5 |
| Control Group | Study Group | p-Value | |
|---|---|---|---|
| Age, years, mean ± std | 29.73 ± 13.66 | 22.93 ± 5.02 | 0.235 |
| Gender, female, n (%) | 12 (80%) | 9 (60%) | 1.0 |
| male | 3 (20%) | 6 (40%) |
| Study Group | Control Group | p-Value | |
|---|---|---|---|
| MMO before surgery | 46.86 ± 5.64 | 50.50 ± 6.57 | 0.128 |
| MMO percentage change after 2 days | −0.40 ± 0.19 | −0.52 ± 0.13 | 0.073 |
| MMO percentage change after 7 days | −0.02 ± 0.05 | −0.10 ± 0.09 | 0.0101 |
| Study Group | Control Group | p-Value | |
|---|---|---|---|
| VAS 1 day after surgery | 5.64 ± 2.37 | 7.71 ± 2.16 | 0.0114 |
| VAS after 2 days | 3.07 ± 1.64 | 3.64 ± 1.82 | 0.391 |
| VAS after 7 days | 0.43 ± 0.65 | 0.71 ± 0.91 | 0.405 |
| Sum | Study Group Mean ± sd | Control Group Mean ± sd | p-Value |
|---|---|---|---|
| Sum before surgery | 466.57 ± 23.69 | 463.64 ± 27.50 | 0.765 |
| Sum percentage change after 2 days | 0.08 ± 0.03 | 0.07 ± 0.04 | 0.227 |
| Sum percentage change after 2 days | 0.02 ± 0.02 | 0.01 ± 0.01 | 0.963 |
| Med (Number of Tablets/100 mg Ketoprofenum) | Study Group Mean ± sd | Control Group Mean ± sd | p-Value |
|---|---|---|---|
| Med 1 day after surgery | 0.86 ± 0.95 | 1.79 ± 0.80 | 0.0102 |
| Med 2 days after surgery | 0.50 ± 1.61 | 0.93 ± 1.00 | 0.0131 |
| Med 7 days after surgery | 0.07 ± 0.27 | 0.00 ± 0.00 | 0.317 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pławecki, P.; Pierwocha, K.; Terlecki, W.; Kawulok, A.; Bogacz, M.; Balicz, A.; Jędrusik-Pawłowska, M.; Dąbrowska-Galas, M.; Morawiec, T. Kinesio Taping as an Adjunct Therapy in Postoperative Care after Extraction of Impacted Third Lower Molars—A Randomized Pilot Study. J. Clin. Med. 2023, 12, 2694. https://doi.org/10.3390/jcm12072694
Pławecki P, Pierwocha K, Terlecki W, Kawulok A, Bogacz M, Balicz A, Jędrusik-Pawłowska M, Dąbrowska-Galas M, Morawiec T. Kinesio Taping as an Adjunct Therapy in Postoperative Care after Extraction of Impacted Third Lower Molars—A Randomized Pilot Study. Journal of Clinical Medicine. 2023; 12(7):2694. https://doi.org/10.3390/jcm12072694
Chicago/Turabian StylePławecki, Piotr, Karolina Pierwocha, Wojciech Terlecki, Anna Kawulok, Mateusz Bogacz, Agnieszka Balicz, Magdalena Jędrusik-Pawłowska, Magdalena Dąbrowska-Galas, and Tadeusz Morawiec. 2023. "Kinesio Taping as an Adjunct Therapy in Postoperative Care after Extraction of Impacted Third Lower Molars—A Randomized Pilot Study" Journal of Clinical Medicine 12, no. 7: 2694. https://doi.org/10.3390/jcm12072694
APA StylePławecki, P., Pierwocha, K., Terlecki, W., Kawulok, A., Bogacz, M., Balicz, A., Jędrusik-Pawłowska, M., Dąbrowska-Galas, M., & Morawiec, T. (2023). Kinesio Taping as an Adjunct Therapy in Postoperative Care after Extraction of Impacted Third Lower Molars—A Randomized Pilot Study. Journal of Clinical Medicine, 12(7), 2694. https://doi.org/10.3390/jcm12072694