

Brace-Free Rehabilitation after Isolated Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft Is Not Inferior to Brace-Based Rehabilitation—A Randomised Controlled Trial
 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Oversight
2.2. Patients and Recruitment
2.3. Interventions
2.4. Perioperative Management and Rehabilitation
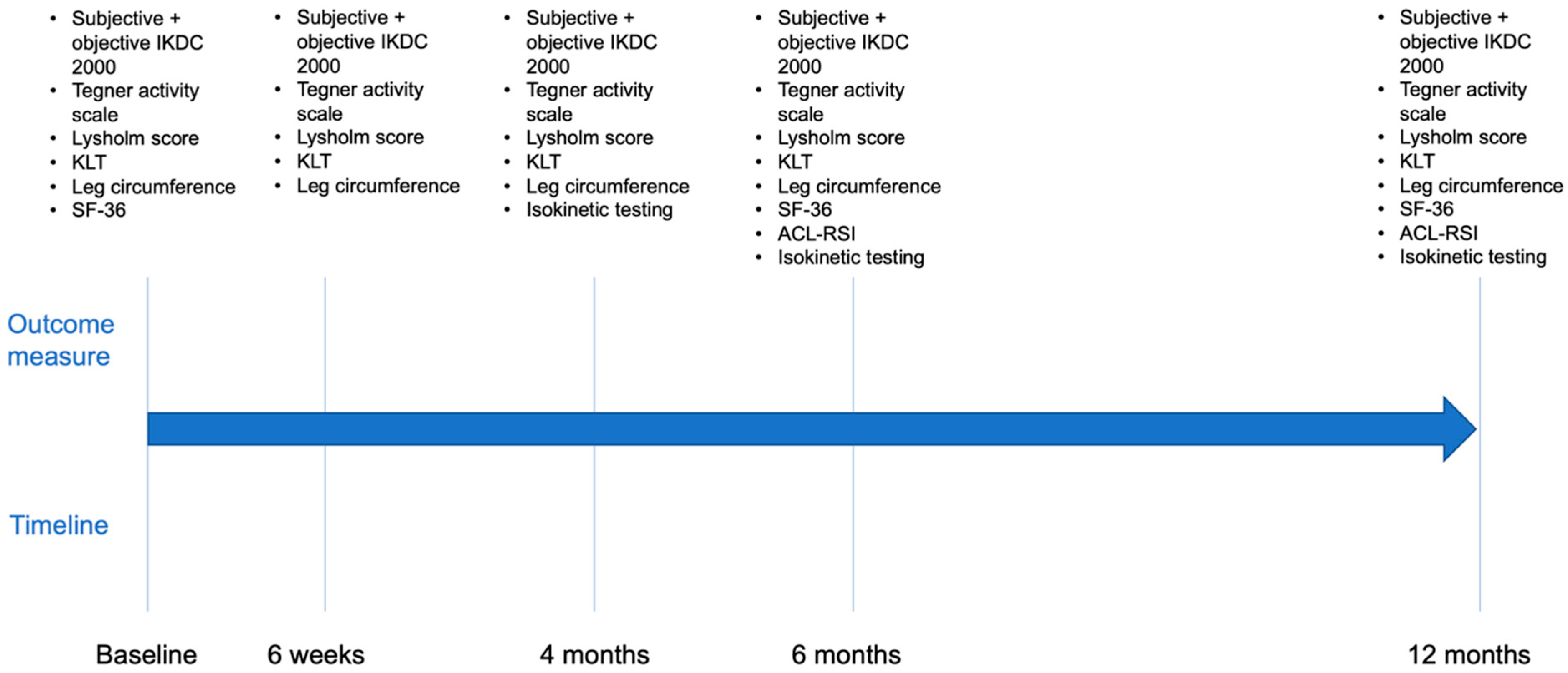
2.5. Outcomes
2.6. Isokinetic Strength Testing
2.7. Statistical Analysis
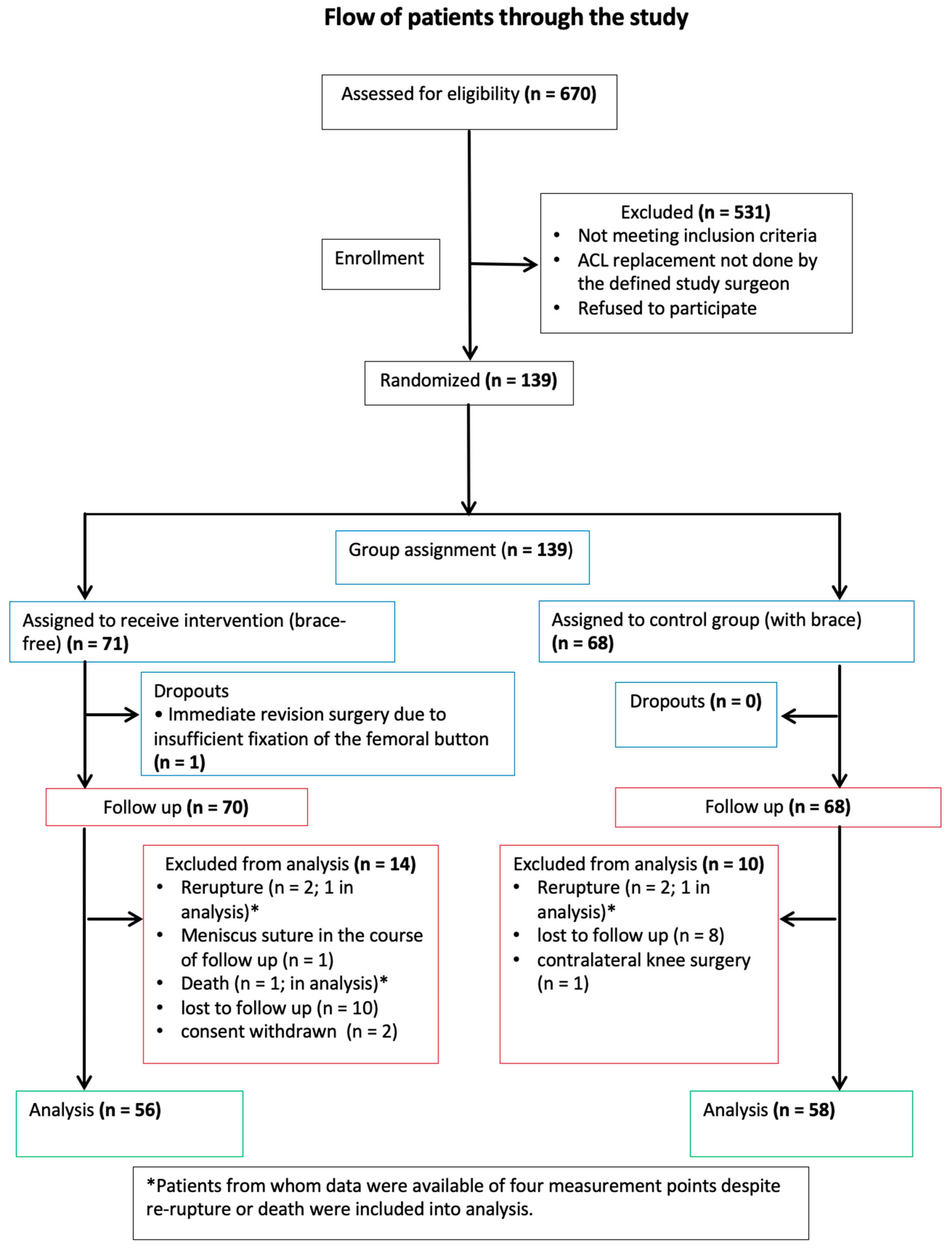
3. Results
3.1. Baseline Data
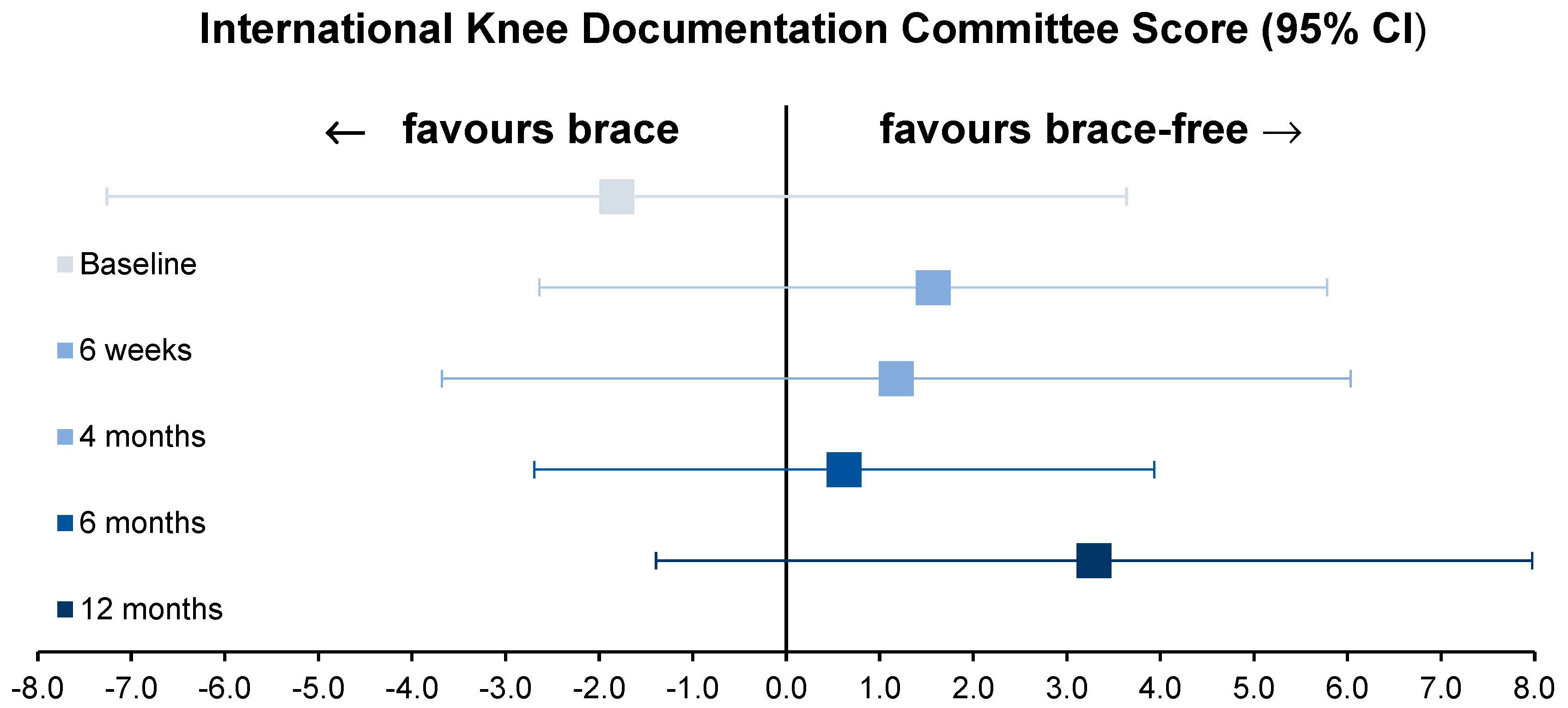
3.2. Primary Outcome Measure
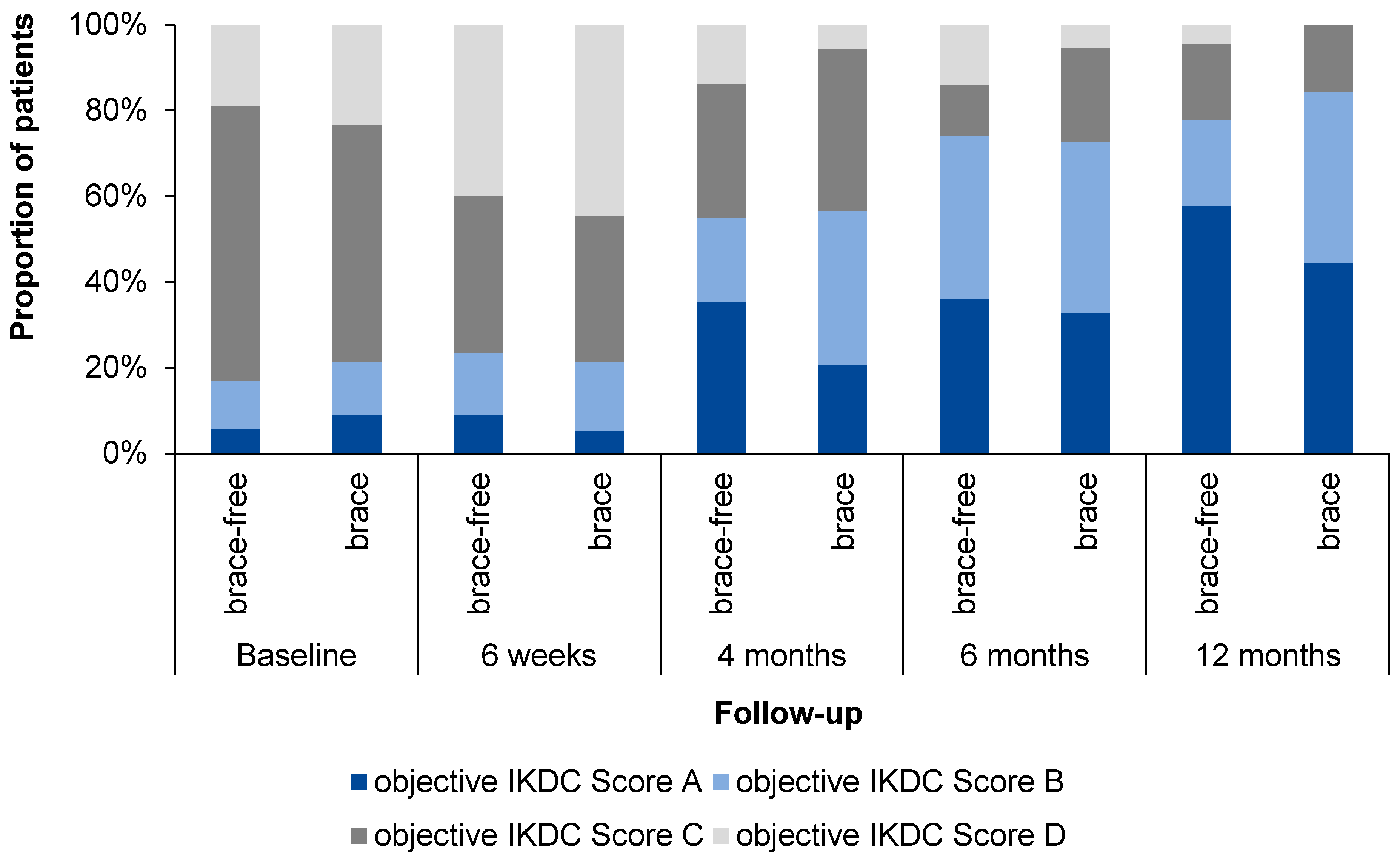
3.3. Secondary Outcome Measures
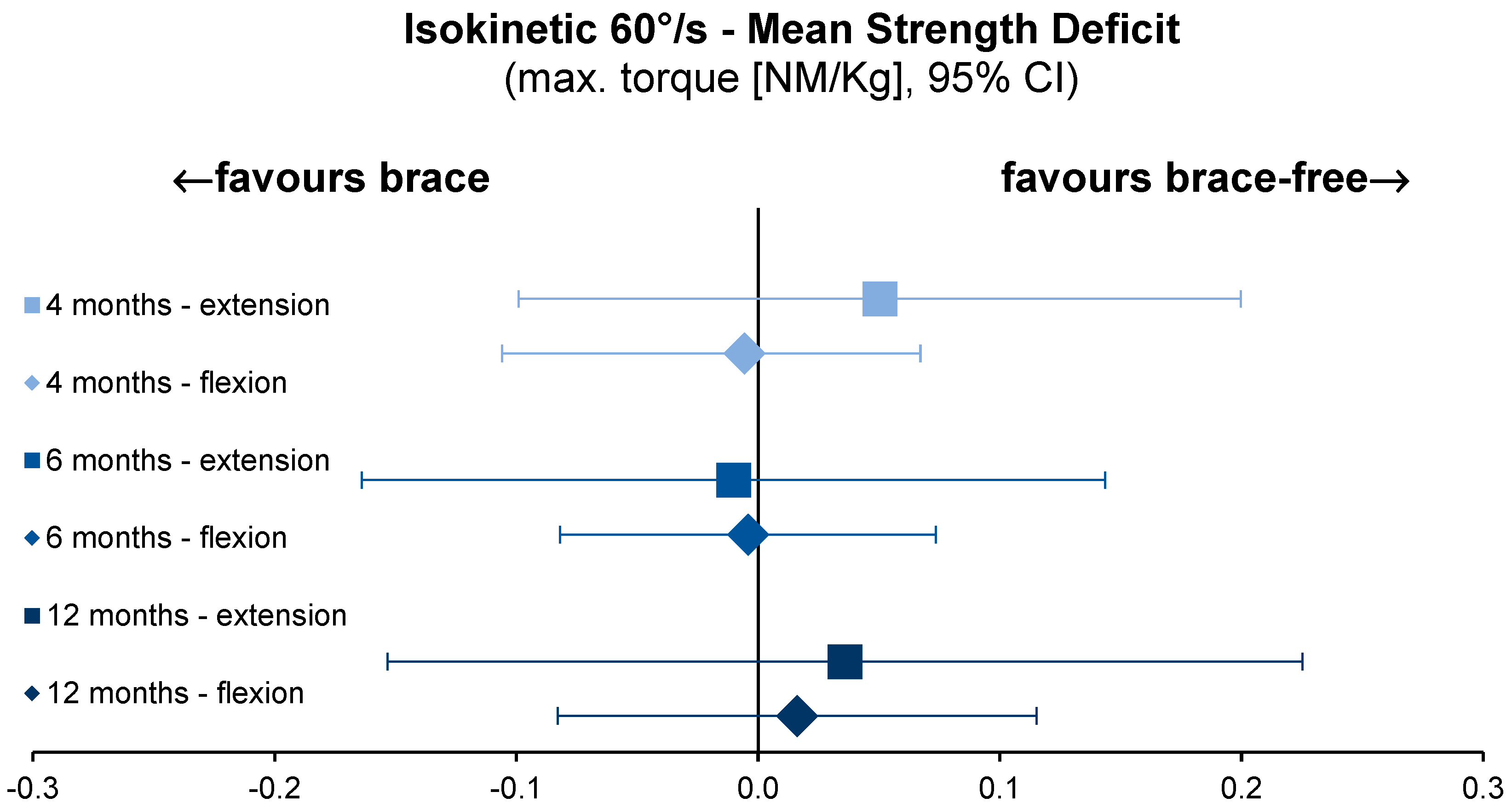
3.4. Isokinetic Strength Testing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Economics
Appendix A.2. In-House Rehabilitation Protocol
| Operating Day | Day 1 | Day 3 | Day 14 | Day 28 | Week 7 | Month 4 | Month 7 | Month 9 | |
| Weight bearing | 20 kg partial load | Load increase pain-adapted | Full weight bearing | ||||||
| Splint/Brace | Rehabilitative four-point hard-frame knee brace | Training off the brace | |||||||
| Physiotherapy | Free mobility in the ankle joint | Motor rail 0-0-90° Muscle stimulation Isometry quadriceps Mobilisation with 2 crutches | Motor rail 0-0-90° Patellar mobilisation Active knee flexion/Passive knee extension | Coordination training Proprioception training | Muscle training | ||||
| Sports/Other | Redon removal if necessary Bandage change | Suture removal | Aqua jogging Crawl swimming Cross trainer Ergometer Nordic walking | Jogging Jump training | Contact sport | Competitive sports High risk sport (Ski Alpine, Squash) |
Appendix A.3. Statistical Analysis


References
- Blom, A.W.; Donovan, R.L.; Beswick, A.D.; Whitehouse, M.R.; Kunutsor, S.K. Common elective orthopaedic procedures and their clinical effectiveness: Umbrella review of level 1 evidence. BMJ 2021, 374, n1511. [Google Scholar] [CrossRef] [PubMed]
- Bram, J.T.; Magee, L.C.; Mehta, N.N.; Patel, N.M.; Ganley, T.J. Anterior Cruciate Ligament Injury Incidence in Adolescent Athletes: A Systematic Review and Meta-analysis. Am. J. Sport. Med. 2021, 49, 1962–1972. [Google Scholar] [CrossRef]
- Ma, R.; Sheth, C.; Fenkell, B.; Buyuk, A.F. The Role of Bracing in ACL Injuries: The Current Evidentiary State of Play. J. Knee Surg. 2022, 35, 255–265. [Google Scholar] [CrossRef]
- Birmingham, T.B.; Kramer, J.F.; Kirkley, A.; Inglis, J.T.; Spaulding, S.J.; Vandervoort, A.A. Knee bracing after ACL reconstruction: Effects on postural control and proprioception. Med. Sci. Sport. Exerc. 2001, 33, 1253–1258. [Google Scholar] [CrossRef]
- McDevitt, E.R.; Taylor, D.C.; Miller, M.D.; Gerber, J.P.; Ziemke, G.; Hinkin, D.; Uhorchak, J.M.; Arciero, R.A.; St Pierre, P. Functional bracing after anterior cruciate ligament reconstruction: A prospective, randomized, multicenter study. Am. J. Sport. Med. 2004, 32, 1887–1892. [Google Scholar] [CrossRef]
- Risberg, M.A.; Beynnon, B.D.; Peura, G.D.; Uh, B.S. Proprioception after anterior cruciate ligament reconstruction with and without bracing. Knee Surg. Sport. Traumatol. Arthrosc. 1999, 7, 303–309. [Google Scholar] [CrossRef]
- Risberg, M.A.; Holm, I.; Steen, H.; Eriksson, J.; Ekeland, A. The effect of knee bracing after anterior cruciate ligament reconstruction. A prospective, randomized study with two years’ follow-up. Am. J. Sport. Med. 1999, 27, 76–83. [Google Scholar] [CrossRef]
- Stanley, C.J.; Creighton, R.A.; Gross, M.T.; Garrett, W.E.; Yu, B. Effects of a knee extension constraint brace on lower extremity movements after ACL reconstruction. Clin. Orthop. Relat. Res. 2011, 469, 1774–1780. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.K.; Ng, G.Y.; Mak, A.F. Effects of knee bracing on the functional performance of patients with anterior cruciate ligament reconstruction. Arch. Phys. Med. Rehabil. 2001, 82, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Branch, T.P.; Hunter, R.E. Functional analysis of anterior cruciate ligament braces. Clin. Sport. Med. 1990, 9, 771–797. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Fleming, B.C.; Churchill, D.L.; Brown, D. The effect of anterior cruciate ligament deficiency and functional bracing on translation of the tibia relative to the femur during nonweightbearing and weightbearing. Am. J. Sport. Med. 2003, 31, 99–105. [Google Scholar] [CrossRef]
- Beynnon, B.D.; Johnson, R.J.; Fleming, B.C.; Peura, G.D.; Renstrom, P.A.; Nichols, C.E.; Pope, M.H. The effect of functional knee bracing on the anterior cruciate ligament in the weightbearing and nonweightbearing knee. Am. J. Sport. Med. 1997, 25, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Cawley, P.W.; France, E.P.; Paulos, L.E. Comparison of rehabilitative knee braces. A biomechanical investigation. Am. J. Sport. Med. 1989, 17, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Wojtys, E.M.; Kothari, S.U.; Huston, L.J. Anterior cruciate ligament functional brace use in sports. Am. J. Sport. Med. 1996, 24, 539–546. [Google Scholar] [CrossRef]
- Birmingham, T.B.; Bryant, D.M.; Giffin, J.R.; Litchfield, R.B.; Kramer, J.F.; Donner, A.; Fowler, P.J. A randomized controlled trial comparing the effectiveness of functional knee brace and neoprene sleeve use after anterior cruciate ligament reconstruction. Am. J. Sport. Med. 2008, 36, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Perrone, G.S.; Webster, K.E.; Imbriaco, C.; Portilla, G.M.; Vairagade, A.; Murray, M.M.; Kiapour, A.M. Risk of Secondary ACL Injury in Adolescents Prescribed Functional Bracing after ACL Reconstruction. Orthop. J. Sport. Med. 2019, 7, 2325967119879880. [Google Scholar] [CrossRef] [PubMed]
- Martinek, V.; Friederich, N.F. To brace or not to brace? How effective are knee braces in rehabilitation? Orthopade 1999, 28, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Rebel, M.; Paessler, H.H. The effect of knee brace on coordination and neuronal leg muscle control: An early postoperative functional study in anterior cruciate ligament reconstructed patients. Knee Surg. Sport. Traumatol. Arthrosc. 2001, 9, 272–281. [Google Scholar] [CrossRef]
- Deppen, R.J.; Landfried, M.J. Efficacy of prophylactic knee bracing in high school football players. J. Orthop. Sport. Phys. Ther. 1994, 20, 243–246. [Google Scholar] [CrossRef]
- Smith, S.D.; Laprade, R.F.; Jansson, K.S.; Aroen, A.; Wijdicks, C.A. Functional bracing of ACL injuries: Current state and future directions. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1131–1141. [Google Scholar] [CrossRef]
- Birmingham, T.B.; Kramer, J.F.; Kirkley, A. Effect of a functional knee brace on knee flexion and extension strength after anterior cruciate ligament reconstruction. Arch. Phys. Med. Rehabil. 2002, 83, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Dai, B.; Butler, R.J.; Garrett, W.E.; Queen, R.M. Anterior cruciate ligament reconstruction in adolescent patients: Limb asymmetry and functional knee bracing. Am. J. Sport. Med. 2012, 40, 2756–2763. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.O.; Hochrein, A.; Hein, W.; Hube, R.; Bernstein, A. Rehabilitation results following anterior cruciate ligament reconstruction using a hard brace compared to a fluid-filled soft brace. Knee 2010, 17, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Mohtadi, N.G.; Chan, D.S.; Dainty, K.N.; Whelan, D.B. Patellar tendon versus hamstring tendon autograft for anterior cruciate ligament rupture in adults. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.L.; Calcei, J.; Ray, T.; Magnussen, R.A.; Musahl, V.; Kaeding, C.C.; Clatworthy, M.; Bergfeld, J.A.; Arnold, M.P. ACL Study Group presents the global trends in ACL reconstruction: Biennial survey of the ACL Study Group. J. ISAKOS 2021, 6, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.G.; Feng, J.T.; He, X.; Wang, F.; Hu, Y.C. The effect of knee bracing on the knee function and stability following anterior cruciate ligament reconstruction: A systematic review and meta-analysis of randomized controlled trials. Orthop. Traumatol. Surg. Res. 2019, 105, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Brandsson, S.; Faxén, E.; Kartus, J.; Eriksson, B.I.; Karlsson, J. Is a knee brace advantageous after anterior cruciate ligament surgery? A prospective, randomised study with a two-year follow-up. Scand. J. Med. Sci. Sport. 2001, 11, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Harilainen, A.; Sandelin, J. Post-operative use of knee brace in bone-tendon-bone patellar tendon anterior cruciate ligament reconstruction: 5-year follow-up results of a randomized prospective study. Scand. J. Med. Sci. Sport. 2006, 16, 14–18. [Google Scholar] [CrossRef]
- Harilainen, A.; Sandelin, J.; Vanhanen, I.; Kivinen, A. Knee brace after bone-tendon-bone anterior cruciate ligament reconstruction. Randomized, prospective study with 2-year follow-up. Knee Surg. Sport. Traumatol. Arthrosc. 1997, 5, 10–13. [Google Scholar] [CrossRef]
- Mayr, H.O.; Stüeken, P.; Münch, E.O.; Wolter, M.; Bernstein, A.; Suedkamp, N.P.; Stoehr, A. Brace or no-brace after ACL graft? Four-year results of a prospective clinical trial. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1156–1162. [Google Scholar] [CrossRef]
- Budny, J.; Fox, J.; Rauh, M.; Fineberg, M. Emerging Trends in Anterior Cruciate Ligament Reconstruction. J. Knee Surg. 2017, 30, 63–69. [Google Scholar] [CrossRef]
- Valle, C.; Hirschmüller, A.; Schmitt-Sody, M.; Haller, B.; Keller, M.; Schoch, W.; Hoffman, H.; Minzlaff, P. Standards in rehabilitation following anterior cruciate ligament reconstruction in the German-speaking world. Sportverletz. Sportschaden 2018, 32, 103–110. [Google Scholar] [PubMed]
- Irrgang, J.J.; Anderson, A.F.; Boland, A.L.; Harner, C.D.; Kurosaka, M.; Neyret, P.; Richmond, J.C.; Shelborne, K.D. Development and validation of the international knee documentation committee subjective knee form. Am. J. Sport. Med. 2001, 29, 600–613. [Google Scholar] [CrossRef] [PubMed]
- van Meer, B.L.; Meuffels, D.E.; Vissers, M.M.; Bierma-Zeinstra, S.M.; Verhaar, J.A.; Terwee, C.B.; Reijman, M. Knee injury and Osteoarthritis Outcome Score or International Knee Documentation Committee Subjective Knee Form: Which questionnaire is most useful to monitor patients with an anterior cruciate ligament rupture in the short term? Arthroscopy 2013, 29, 701–715. [Google Scholar] [CrossRef] [PubMed]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sport. Med. 1982, 10, 150–154. [Google Scholar] [CrossRef]
- Tegner, Y.; Lysholm, J. Derotation brace and knee function in patients with anterior cruciate ligament tears. Arthroscopy 1985, 1, 264–267. [Google Scholar] [CrossRef]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Hefti, F.; Muller, W.; Jakob, R.P.; Staubli, H.U. Evaluation of knee ligament injuries with the IKDC form. Knee Surg. Sport. Traumatol. Arthrosc. 1993, 1, 226–234. [Google Scholar] [CrossRef]
- Drouin, J.M.; Valovich-mcLeod, T.C.; Shultz, S.J.; Gansneder, B.M.; Perrin, D.H. Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements. Eur. J. Appl. Physiol. 2004, 91, 22–29. [Google Scholar]
- Duarte, J.P.; Valente-Dos-Santos, J.; Coelho, E.S.M.J.; Couto, P.; Costa, D.; Martinho, D.; Gonçalves, R.S. Reproducibility of isokinetic strength assessment of knee muscle actions in adult athletes: Torques and antagonist-agonist ratios derived at the same angle position. PLoS ONE 2018, 13, e0202261. [Google Scholar] [CrossRef]
- Pelegrinelli, A.R.M.; Guenka, L.C.; Dias, J.M.; Dela Bela, L.F.; Silva, M.F.; Moura, F.A.; Brown, L.E.; Cardoso, J.R. Isokinetic Muscle Performance after Anterior Cruciate Ligament Reconstruction: A Case-Control Study. Int. J. Sport. Phys. Ther. 2018, 13, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Van Driessche, S.; Van Roie, E.; Vanwanseele, B.; Delecluse, C. Test-retest reliability of knee extensor rate of velocity and power development in older adults using the isotonic mode on a Biodex System 3 dynamometer. PLoS ONE 2018, 13, e0196838. [Google Scholar] [CrossRef] [PubMed]
- Mentiplay, B.F.; Banky, M.; Clark, R.A.; Kahn, M.B.; Williams, G. Lower limb angular velocity during walking at various speeds. Gait Posture 2018, 65, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A.; Wells, R.P.; Orr, G.W. Errors in the use of isokinetic dynamometers. Eur. J. Appl. Physiol. Occup. Physiol. 1981, 46, 397–408. [Google Scholar] [CrossRef]
- Baumgart, C.; Welling, W.; Hoppe, M.W.; Freiwald, J.; Gokeler, A. Angle-specific analysis of isokinetic quadriceps and hamstring torques and ratios in patients after ACL-reconstruction. BMC Sport. Sci. Med. Rehabil. 2018, 10, 23. [Google Scholar] [CrossRef]
- Irrgang, J.; Anderson, A.; Dunn, W.; Kocher, M.; Marx, R.; Mann, B.; Miller, B.; Provencher, M.; Reider, B.; Richmond, J. Summary of Clinical Outcome Measures for Sports-Related Knee Injuries; Final Report; AOSSM Outcomes Task Force. 2012. Available online: https://www.sportsmed.org/AOSSMIMIS/members/downloads/research/ClinicalOutcomeMeasuresKnee.pdf (accessed on 4 January 2023).
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Whitehead, T.S.; Webster, K.E. Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery. Am. J. Sport. Med. 2013, 41, 1549–1558. [Google Scholar] [CrossRef]
- Anderson, K.; Wojtys, E.M.; Loubert, P.V.; Miller, R.E. A biomechanical evaluation of taping and bracing in reducing knee joint translation and rotation. Am. J. Sport. Med. 1992, 20, 416–421. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Goldstein, S.A.; Redfern, M.; Trier, E.; Matthews, L.S. A biomechanical evaluation of the Lenox Hill knee brace. Clin. Orthop. Relat. Res. 1987, 220, 179–184. [Google Scholar] [CrossRef]
- Henriksson, M.; Rockborn, P.; Good, L. Range of motion training in brace vs. plaster immobilization after anterior cruciate ligament reconstruction: A prospective randomized comparison with a 2-year follow-up. Scand. J. Med. Sci. Sport. 2002, 12, 73–80. [Google Scholar] [CrossRef]
- Kartus, J.; Stener, S.; Köhler, K.; Sernert, N.; Eriksson, B.I.; Karlsson, J. Is bracing after anterior cruciate ligament reconstruction necessary? A 2-year follow-up of 78 consecutive patients rehabilitated with or without a brace. Knee Surg. Sport. Traumatol. Arthrosc. 1997, 5, 157–161. [Google Scholar] [CrossRef]
- Melegati, G.; Tornese, D.; Bandi, M.; Volpi, P.; Schonhuber, H.; Denti, M. The role of the rehabilitation brace in restoring knee extension after anterior cruciate ligament reconstruction: A prospective controlled study. Knee Surg. Sport. Traumatol. Arthrosc. 2003, 11, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Möller, E.; Forssblad, M.; Hansson, L.; Wange, P.; Weidenhielm, L. Bracing versus nonbracing in rehabilitation after anterior cruciate ligament reconstruction: A randomized prospective study with 2-year follow-up. Knee Surg. Sport. Traumatol. Arthrosc. 2001, 9, 102–108. [Google Scholar] [CrossRef]
- Andersson, D.; Samuelsson, K.; Karlsson, J. Treatment of anterior cruciate ligament injuries with special reference to surgical technique and rehabilitation: An assessment of randomized controlled trials. Arthroscopy 2009, 25, 653–685. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.W.; Fetzer, G.B. Bracing after ACL reconstruction: A systematic review. Clin. Orthop. Relat. Res. 2007, 455, 162–168. [Google Scholar] [CrossRef]
- Janssen, R.P.; Scheffler, S.U. Intra-articular remodelling of hamstring tendon grafts after anterior cruciate ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Giotis, D.; Paschos, N.K.; Zampeli, F.; Pappas, E.; Mitsionis, G.; Georgoulis, A.D. Bracing can partially limit tibial rotation during stressful activities after anterior crucial ligament reconstruction with a hamstring graft. Orthop. Traumatol. Surg. Res. 2016, 102, 601–606. [Google Scholar] [CrossRef]
- Welling, W.; Benjaminse, A.; Seil, R.; Lemmink, K.; Zaffagnini, S.; Gokeler, A. Low rates of patients meeting return to sport criteria 9 months after anterior cruciate ligament reconstruction: A prospective longitudinal study. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 3636–3644. [Google Scholar] [CrossRef]
- Kohn, L.; Rembeck, E.; Rauch, A. Anterior cruciate ligament injury in adults: Diagnostics and treatment. Orthopade 2020, 49, 1013–1028. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Brace | Brace-Free | p Value |
|---|---|---|---|
| Demographics | n = 58 | n = 56 | |
| Male gender, n (%) | 37 (63.8) | 37 (66.1) | 0.846 * |
| Right knee, n (%) | 28 (48.3) | 26 (46.4) | 0.854 * |
| Age (years), mean (SD) | 33.2 (12.3) | 31.5 (10.8) | 0.429 † |
| Body mass index (kg/m2), mean (SD) | 26.0 (3.1) | 25.9 (4.1) | 0.881 † |
| Smoking, n (%) | 12 (20.7) | 17 (30.4) | 0.285 * |
| Interval between injury and surgery (days), mean (SD) | 109.2 (199.5) | 123.4 (257.4) | 0.744 † |
| Cartilage damage | |||
| Medial femoral, n (%) | 11 (19.3) | 12 (21.43) | 0.819 * |
| Lateral femoral, n (%) | 2 (3.51) | 0 (0.00) | 0.496 * |
| Medial tibial, n (%) | 5 (8.77) | 5 (8.93) | 1.000 * |
| Lateral tibial, n (%) | 3 (5.26) | 2 (3.57) | 1.000 * |
| Meniscal lesion | |||
| Meniscus medial | |||
| Lesion, n (%) | 8 (13.79) | 3 (5.36) | |
| Meniscus lateral | |||
| Lesion, n (%) | 4 (6.9) | 5 (8.93) | |
| Meniscus resection during ACLR, n (%) | 11 (19.3) | 8 (14.29) | 0.799 * |
| Meniscus medial, n (%) | 7 (12.07) | 3 (5.36) | 0.322 * |
| Meniscus lateral, n (%) | 4 (6.9) | 5 (8.93) | 0.74 * |
| Sports Level | n | Brace | Brace-Free |
|---|---|---|---|
| Professional | 4 | n = 0 | n = 4 |
| Activity (%), mean (SD) | 75 (35.36) | ||
| Return to sports (w), mean (SD) | 22 (8.49) | ||
| Amateur | 47 | n = 28 | n = 19 |
| Activity (%), mean (SD) | 73.86 (35.72) | 57.65 (40.04) | |
| Return to sports (w), mean (SD) | 31.95 (36.08) | 28.67 (15.44) | |
| Recreational sports | 52 | n = 27 | n = 25 |
| Activity (%), mean (SD) | 55.23 (45) | 61.25 (40.97) | |
| Return to sports (w), mean (SD) | 31.62 (16.36) | 33.27 (18.03) | |
| No sport | 7 | n = 3 | n = 4 |
| Pre-Existing Injuries and Previous Interventions Contralateral Side | Brace | Brace-Free | Total |
|---|---|---|---|
| none | 58 | 65 | 123 |
| ACL reconstruction | 5 | 4 | 9 |
| ACL rupture, conservative | 1 | 0 | 1 |
| Rupture of the collateral ligaments, conservative | 1 | 1 | 2 |
| Meniscus/cartilage lesion | 1 | 1 | 2 |
| Patella luxation | 1 | 0 | 1 |
| Posttraumatic arthrosis | 1 | 0 | 1 |
| Total | 68 | 71 | 139 |
| Complications | Brace | Brace-Free | Total |
|---|---|---|---|
| none | 62 | 59 | 121 |
| Re-rupture | 2 | 2 | 4 |
| Cyclops, operative treated | 4 | 4 | 8 |
| Postoperative joint lavage, non-infectious hemarthrosis | 0 | 1 | 1 |
| Dislocated screw fragment | 0 | 1 | 1 |
| New Meniscus lesion, operative suture | 0 | 1 | 1 |
| Revision button fixation | 0 | 1 | 1 |
| Plica resection | 0 | 1 | 1 |
| Notchplastic in case of ACL impingement | 0 | 1 | 1 |
| Total | 68 | 71 | 139 |
| Timepoint | Group | Lysholm Score, Mean ± SD | Tegner Score, Mean ± SD | Knee Laxity Measurement [mm], Mean ± SD | SF 36-MCS Scale, Mean ± SD | SF 36-PCS Scale, Mean ± SD |
|---|---|---|---|---|---|---|
| Baseline | Brace | 54.9 ± 4.7 | 3.5 ± 0.6 | −1.0 ± 0.5 | 51.6 ± 2.8 | 38.5 ± 2.3 |
| Brace-free | 56.0 ± 5.1 | 2.7 ± 0.6 | −0.9 ± 0.6 | 49.5 ± 3.2 | 39.2 ± 2.5 | |
| 6 weeks | Brace | 60.9 ± 4.7 | 2.5 ± 0.4 | 0.2 ± 0.5 | 52.8 ± 4.2 | 37.8 ± 3.7 |
| Brace-free | 61.2 ± 5.2 | 2.5 ± 0.4 | −0.4 ± 0.4 | 46.5 ± 6.7 | 36.2 ± 3.9 | |
| 4 months | Brace | 78.3 ± 4.3 | 3.8 ± 0.4 | −0.8 ± 0.5 | 58.3 ± 1.8 | 45.3 ± 4.6 |
| Brace-free | 75.1 ± 5.2 | 3.6 ± 0.5 | −0.4 ± 0.4 | 50.9 ± 5.0 | 45.9 ± 3.9 | |
| 6 months | Brace | 84.3 ± 2.4 | 4.6 ± 0.5 | −0.3 ± 0.5 | 54.8 ± 1.7 | 50.4 ± 1.3 |
| Brace-free | 83.5 ± 2.7 | 4.2 ± 0.5 | −0.8 ± 0.5 | 52.6 ± 2.4 | 51.0 ± 1.4 | |
| 12 months | Brace | 88.3 ± 4.0 | 5.5 ± 0.5 | −0.4 ± 0.5 | 52.9 ± 1.4 | 52.9 ± 1.4 |
| Brace-free | 85.1 ± 3.9 | 5.3 ± 0.6 | −0.6 ± 0.4 | 52.3 ± 2.0 | 52.3 ± 2.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoepp, C.; Ohmann, T.; Martin, W.; Praetorius, A.; Seelmann, C.; Dudda, M.; Stengel, D.; Hax, J. Brace-Free Rehabilitation after Isolated Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft Is Not Inferior to Brace-Based Rehabilitation—A Randomised Controlled Trial. J. Clin. Med. 2023, 12, 2074. https://doi.org/10.3390/jcm12052074
Schoepp C, Ohmann T, Martin W, Praetorius A, Seelmann C, Dudda M, Stengel D, Hax J. Brace-Free Rehabilitation after Isolated Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft Is Not Inferior to Brace-Based Rehabilitation—A Randomised Controlled Trial. Journal of Clinical Medicine. 2023; 12(5):2074. https://doi.org/10.3390/jcm12052074
Chicago/Turabian StyleSchoepp, Christian, Tobias Ohmann, Wolfgang Martin, Arthur Praetorius, Christine Seelmann, Marcel Dudda, Dirk Stengel, and Jakob Hax. 2023. "Brace-Free Rehabilitation after Isolated Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft Is Not Inferior to Brace-Based Rehabilitation—A Randomised Controlled Trial" Journal of Clinical Medicine 12, no. 5: 2074. https://doi.org/10.3390/jcm12052074
APA StyleSchoepp, C., Ohmann, T., Martin, W., Praetorius, A., Seelmann, C., Dudda, M., Stengel, D., & Hax, J. (2023). Brace-Free Rehabilitation after Isolated Anterior Cruciate Ligament Reconstruction with Hamstring Tendon Autograft Is Not Inferior to Brace-Based Rehabilitation—A Randomised Controlled Trial. Journal of Clinical Medicine, 12(5), 2074. https://doi.org/10.3390/jcm12052074