
Practice Patterns of Antithrombotic Therapy during the Early Postoperative Course of Cardiac Surgery

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Online Survey and Periods
2.3. Data Analysis
3. Results
3.1. Respondent Characteristics
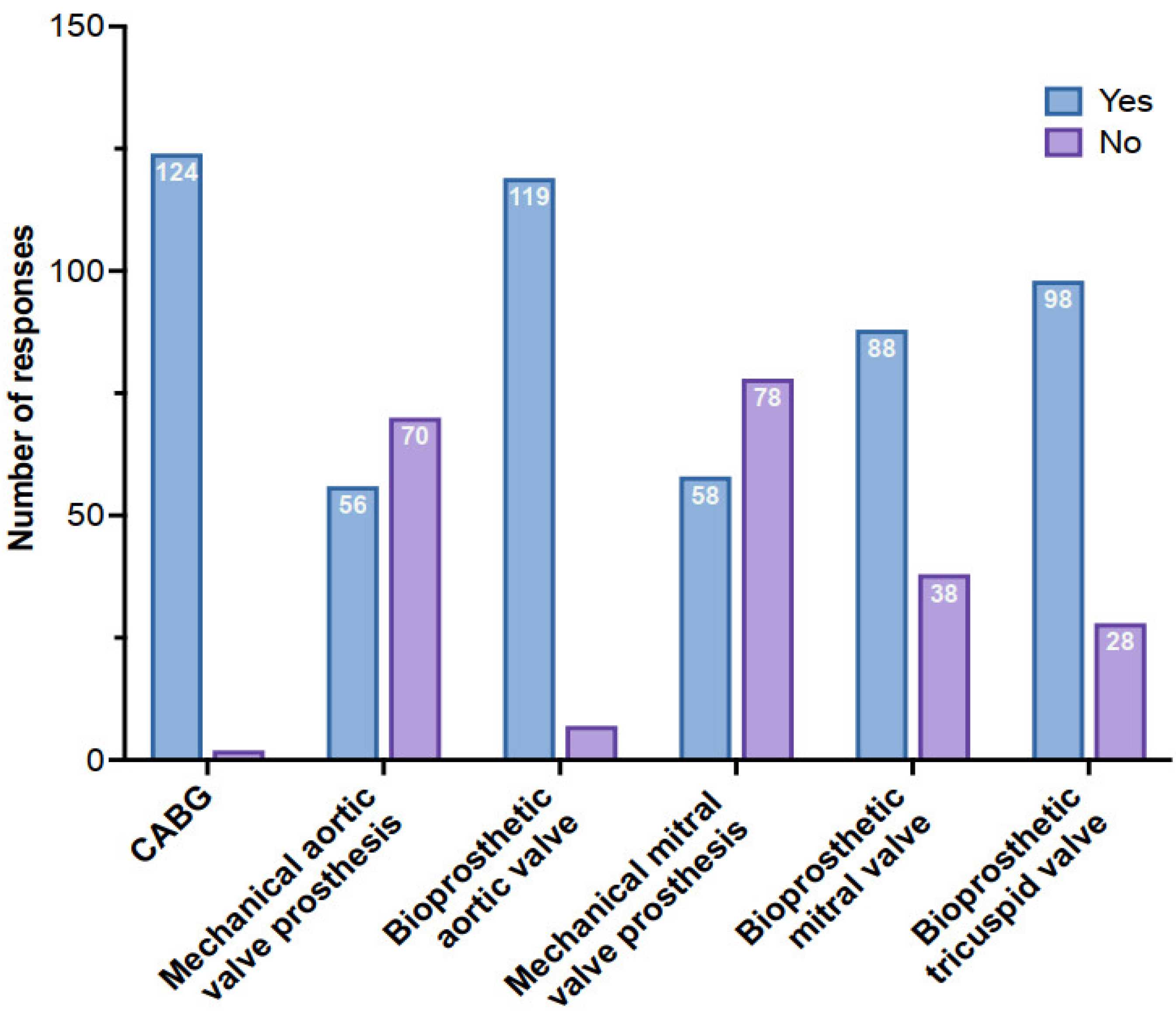
3.2. Early Postoperative Antithrombotic Therapy
3.3. Modalities of LMWH Use
3.4. Management of Chest Drainage and Temporary Epicardial Pacing Wires (TEPWs)
4. Discussion

{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Type | No. of Patients | Type of Cardiac Surgery | Strategy | Time of Start | Follow-Up | TE Rate | TE Event | Bleeding Rate | Mortality |
|---|---|---|---|---|---|---|---|---|---|---|
| Montalescot [11] (2000) | Retrospective CC | 208 adults 106 adults UFH 102 adults LMWH | Single or double mechanical heart valve replacement | UFH group: 3 SC injections a day, at a dose of 500 IU·kg−1·d−1, adjusted to the APTT with a target range of 1.5 to 2.5 times control; LMWH group: 100 anti-Xa IU·kg−1, SC at 12 h intervals for enoxaparin. For Nadroparin, at a dose of 87 anti-Xa IU·kg−1 SC at 12 h intervals. Anti-Xa activity 4 h after the third injection: 0.5 to 1 IU·mL−1 | ~POD + 6 | In-hospital stay (~14 days) | UH: 1/106 (1%) LMWH: 0/102 (0%) | 2 successive transient ischemic strokes (J17) | UH: 2/106 (2%) LMWH: 2/102 (2%) | No death |
| Fanikos [9] (2004) | Retrospective matched CC | 63 adults 34 adults UFH 29 adults LMWH | Mechanical heart valve | UFH dose adjustments left to the discretion of the physician; Enoxaparin 1 mg/kg SC at 12 h interval | POD + 1-2 | 3 months | UFH: 2/34 (6%) LMWH: 0/29 (0%) | 1 bilateral occipital stroke. 1 HIT | UH: 3/34 (9%) LMWH: 3/29 (10%) | UH: 4/34 (11.7%) LMWH: 1/29 (3.4%) |
| Talwar [19] (2004) | Retrospective CC | 538 adults 245 OA 293 OA + LMWH | Mechanical heart valve | OA + enoxaparin SC | 6 h after surgery | 6 months | OA: 15 (6.1%) OA + LMWH: 6 (2.1%) | Prosthetic valve thrombosis | N.D. | N.D. |
| Meurin [12] (2005) | Prospective CS | 250 patients | Mechanical heart valve | Enoxaparin (100 IU·kg−1 twice daily SC) until VKA treatment was fully effective | ~POD + 16 | 3 months | 1/250 (0.4%) | Transient ischemic attack | 2/250 major bleeding (0.8%), 3/250 minor bleeding (1.2%) | No death |
| Jones [25] (2005) | Retrospective CC | 2977 adults 2037 none 579 UFH 361 LMWH | CABG or valve surgeries | Enoxaparin: 1 mg·kg−1 SC twice daily OA not documented | N.D. | In-hospital stay | N.D. | N.D. | Bleeding requiring reoperation: 2.7% for no UFH or LMWH, 7.8% for UFH 8.9% for LMWH | N.D. |
| Rivas-Gándara [20] (2008) | Prospective CS | 140 adults | Mixed heart valve replacement | Enoxaparin 40 mg SC twice daily if BW > 60 kg or 40 mg once daily if BW < 60 kg, then increase to 0.75 mg·kg−1·d−1 at POD + 3 OA started at POD + 1 | POD + 1 | 3 months | 6/140 (4.3%) | 3 strokes, 1 mesenteric ischemia, 1 retinal thrombosis, 1 mitral prosthetic thrombosis | 3/140 (2.1%), 1 mortal intracranial hemorrhage, 1 muscular hematoma, 1 excessive drainage bleeding | 9/140 (6.4%) |
| Puri [21] (2008) | CS | 503 adults 221 OA only 159 OA + LMWH 123 OA + UFH | Mechanical heart valve | LMWH: Enoxaparin 40 mg SC once daily UFH infusion titrated in order to achieve 1.5- to 2-fold that of controls | 6–12 h after surgery | 8 to 64 months | OA only: 1/221 (0.5%); OA + LMWH: 1/159 (0.6%); OA + UFH: 1/123 (0.8%) | Transient ischemic attack, peripheral thromboembolism | 2/221 (OA), 12/159 (OA + LMWH), 9/123 (OA + UFH) required the reinsertion of drains; 0/221 (OA), 7/159 (OA + LMWH), 5/123 (OA + UFH) had tamponade; 0/221 (OA), 5/159 (OA + LMWH), 4/123 (OA + UFH) required re-exploration for excessive drainage at >48 h after surgery | N.D. |
| Steger [33] (2008) | Retrospective CS | 256 adults | Mechanical heart valve | Enoxaparin 40 mg SC twice daily | POD + 4 | Mean follow-up: 38.6 days | 2/256 (0.7%) | Arterial thromboses | 18/256 (7%) minor bleeding | No death |
| Weiss [14] (2013) | Retrospective CC | 402 adults Enoxaparin 201 full dose (FD) 201 half dose (HD) | Mixed cardiac surgeries | FD: Enoxaparin 1 mg·kg−1 HD: Enoxaparin 0.5 mg·kg−1 | POD + 1 | In-hospital stay | FD: 5/201 (2.5%) HD: 9/201 (4.5%) | Cerebral infarction: 1/201 (FD), 5/201 (HD); Myocardial infarction: 3/201 in each group; Mesenteric infarction: 0/201 (FD), 1/201 (HD); Vein thrombosis: 1/201 (FD), O/201 (HD) | FD: 11/201 (5.5%) HD: 5/201 (2.5%) | FD: 1/201 (0.5%) HD: 11/201 (5.5%) |
| Kindo [10] (2014) | Prospective CS | 1063 adults Enoxaparin | Mechanical heart valve | Enoxaparin 4000 IU SC on POD + 1 At POD + 2: 4000 IU SC—BW < 60 kg 6000 IU –SC BW [60–80 kg] 8000 IU SC—BW > 80 kg Twice daily | POD + 1 | 6 weeks | 11/1063 (1%) | 10/11 transient or permanent strokes | 44/1063 (4.1%) 7 were observed before enoxaparin | No death |
| Kolluri [15] (2016) | RCT | 78 adults 41 fondaprinux 37 placebo | On-pump CABG | 2.5 mg SC fondaparinux daily prophylaxis | 12 ± 2 h after surgery or morning of POD + 1 | POD + 11 And POD + 35 | Fondaparinux: 1/41 (2.4%) Placebo: 1/37 (2.7%) | DVT | Fondaparinux: 4/41 (9.8%) Placebo: 0/37 | No death |
| Czerwińska-Jelonkiewicz [13] (2018) | Retrospective CS | 388 adults Enoxaparin | Surgical valve procedure Mechanical 161 (62%) Bioprosthetic 110 (28.35%) Other/combined 117 (30.1%) | 40–60 mg SC enoxaparin on day of surgery and 40–80 mg on POD + 1 | 8–12 h after surgery | In-hospital stay | 7/388 (1.8%) | Strokes or transient ischemic attacks | Severe: 37 (9.6%) Massive: 14 (3.6%) | 4/388 (1.0%) |
| Li [7] (2019) | Retrospective CS with propensity score | 473 adults 257 enoxaparin 216 controls | On-pump minimally invasive cardiac surgery (MICS) | 40 mg SC enoxaparin once daily | 6 h after surgery | In-hospital stay | Enoxaparin: 1/257 (0.4%); Control: 3/216 (1.4%); After PS adjusting Enoxaparin and Control: 0% | DVT and shock (undetermined) | Enoxaparin: 41/257 (16%); Control: 17/216 (7.9%); After PS enoxaparin: 16/257 (14.5%); Control: 6/216 (5.5%) | No death |
| Parviainen [23] (2022) | RCT | 39 adults Enoxaparin 20 CIV 19 SC | On-pump CABG | 40 mg enoxaparin CIV/24 h for 72 h 40 mg SC enoxaparin once daily | 6–10 h after surgery | 72 h postoperative | 0/33 | None in both groups | 3/39 (7.7%) | No death |
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dyke, C.; Aronson, S.; Dietrich, W.; Hofmann, A.; Karkouti, K.; Levi, M.; Murphy, G.J.; Sellke, F.W.; Shore-Lesserson, L.; von Heymann, C.; et al. Universal Definition of Perioperative Bleeding in Adult Cardiac Surgery. J. Thorac. Cardiovasc. Surg. 2014, 147, 1458–1463.e1. [Google Scholar] [CrossRef]
- Vuylsteke, A.; Pagel, C.; Gerrard, C.; Reddy, B.; Nashef, S.; Aldam, P.; Utley, M. The Papworth Bleeding Risk Score: A Stratification Scheme for Identifying Cardiac Surgery Patients at Risk of Excessive Early Postoperative Bleeding. Eur. J. Cardio-Thoracic Surg. 2011, 39, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Close, V.; Purohit, M.; Tanos, M.; Hunter, S. Should Patients Post-Cardiac Surgery Be given Low Molecular Weight Heparin for Deep Vein Thrombosis Prophylaxis? Interact. Cardiovasc. Thorac. Surg. 2006, 5, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Lison, S.; Dietrich, W.; Braun, S.; Boehm, J.; Schuster, T.; Englhard, A.; Perchuc, A.; Spannagl, M.; Busley, R. Enhanced Thrombin Generation After Cardiopulmonary Bypass Surgery. Anesth. Analg. 2011, 112, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, S.; Mehilli, J.; Cassese, S.; Hall, T.S.; Abdelhamid, M.; Barbato, E.; Hert, S.D.; de Laval, I.; Geisler, T.; Hinterbuchner, L.; et al. 2022 ESC Guidelines on Cardiovascular Assessment and Management of Patients Undergoing Non-Cardiac Surgery. Eur. Heart J. 2022, 43, 3826–3924. [Google Scholar] [CrossRef] [PubMed]
- Passaglia, L.G.; Barros, G.M.; Sousa, M.R. Early Postoperative Bridging Anticoagulation after Mechanical Heart Valve Replacement: A Systematic Review and Meta-analysis. J. Thromb. Haemost. 2015, 13, 1557–1567. [Google Scholar] [CrossRef]
- Li, W.; Wang, P.; Le, S.; Xi, W.; Wang, J.; Yin, L.; Wang, Q.; Zhang, Y.; Wang, Z. Benefits May Not Outweigh Risks of Low Molecular Weight Heparin (LMWH) in Early Postoperative Thromboprophylaxis Following Minimally Invasive Cardiac Surgery: A Propensity Score-Matched Analysis. J. Thorac. Dis. 2019, 11, 5266–5273. [Google Scholar] [CrossRef]
- Li, B.-X.; Liu, S.-D.; Qi, L.; Sun, S.; Sun, W.; Li, Y.-M.; Song, B.; Wu, X.-A. Comparison of Different Bridging Anticoagulation Therapies Used after Mechanical Heart Valve Replacement in Chinese Patients—A Prospective Cohort Study. J. Cardiothorac. Surg. 2020, 15, 40. [Google Scholar] [CrossRef]
- Fanikos, J.; Tsilimingras, K.; Kucher, N.; Rosen, A.B.; Hieblinger, M.D.; Goldhaber, S.Z. Comparison of Efficacy, Safety, and Cost of Low-Molecular-Weight Heparin with Continuous-Infusion Unfractionated Heparin for Initiation of Anticoagulation after Mechanical Prosthetic Valve Implantation. Am. J. Cardiol. 2004, 93, 247–250. [Google Scholar] [CrossRef]
- Kindo, M.; Gerelli, S.; Minh, T.H.; Zhang, M.; Meyer, N.; Announe, T.; Bentz, J.; Mansour, Z.; Mommerot, A.; Petit-Eisenmann, H.; et al. Exclusive Low-Molecular-Weight Heparin as Bridging Anticoagulant After Mechanical Valve Replacement. Ann. Thorac. Surg. 2014, 97, 789–795. [Google Scholar] [CrossRef]
- Montalescot, G.; Polle, V.; Collet, J.P.; Leprince, P.; Bellanger, A.; Gandjbakhch, I.; Thomas, D. Low Molecular Weight Heparin After Mechanical Heart Valve Replacement. Circulation 2000, 101, 1083–1086. [Google Scholar] [CrossRef]
- Meurin, P.; Tabet, J.Y.; Weber, H.; Renaud, N.; Driss, A.B. Low-Molecular-Weight Heparin as a Bridging Anticoagulant Early After Mechanical Heart Valve Replacement. Circulation 2006, 113, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Czerwińska-Jelonkiewicz, K.; Cisowski, M.; Bochenek, A.; Buszman, P.; Milewski, K.; Kunik, P.; Mularska, M.; Kocot, K.; Politowski, P.; Brączkowski, J.; et al. Low Molecular Weight Heparin in Surgical Valve Procedures: When and How Much for an Optimal Prophylaxis? Cardiol. J. 2018, 27, 548–557. [Google Scholar] [CrossRef]
- Weiss, A.; Brose, S.; Ploetze, K.; Matschke, K. Half-Dose Enoxaparin vs. Full-Dose Enoxaparin for Postoperative Bridging Therapy in Patients after Cardiac Surgery: Which Dose Regimen Should Be Preferred? Clin. Hemorheol. Microcirc. 2013, 54, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Kolluri, R.; Plessa, A.L.; Sanders, M.C.; Singh, N.K.; Lucore, C. A Randomized Study of the Safety and Efficacy of Fondaparinux versus Placebo in the Prevention of Venous Thromboembolism after Coronary Artery Bypass Graft Surgery. Am. Heart J. 2016, 171, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wilsey, H.A.; Pandya, K.; Beavers, C.; Xiaoshu, L.; Ather, A. Comparison of Venous Thromboembolism Prophylactic Measures Post Coronary Artery Bypass Graft Surgery. Am. J. Cardiovasc. Drug 2019, 19, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.M.; Bham, E.; Pavey, W. Incidence of Venous Thromboembolism and Benefits and Risks of Thromboprophylaxis After Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2015, 4, e002652. [Google Scholar] [CrossRef]
- Nisio, M.D.; Peinemann, F.; Porreca, E.; Rutjes, A.W. Primary Prophylaxis for Venous Thromboembolism in Patients Undergoing Cardiac or Thoracic Surgery. Cochrane Database Syst. Rev. 2015, 89, CD009658. [Google Scholar] [CrossRef]
- Talwar, S.; Kapoor, C.K.; Velayoudam, D.; Kumar, A.S. Anticoagulation Protocol and Early Prosthetic Valve Thrombosis. Indian Hear J. 2004, 56, 225–228. [Google Scholar]
- Rivas-Gándara, N.; Ferreira-González, I.; Tornos, P.; Torrents, A.; Permanyer-Miralda, G.; Nicolau, I.; Arellano-Rodrigo, E.; Vallejo, N.; Igual, A.; Soler-Soler, J. Enoxaparin as Bridging Anticoagulant Treatment in Cardiac Surgery. Heart 2008, 94, 205. [Google Scholar] [CrossRef]
- Puri, D.; Kumar, A.; Basu, R.; Chaudhary, A.; Sarwal, V.; Sahoo, M.; Mahant, T.S. Early Anticoagulation after Mechanical Valve Implantation, and Related Complications. J. Hear Valve Dis. 2008, 17, 418–424; discussion 425. [Google Scholar]
- Kondo, N.I.; Maddi, R.; Ewenstein, B.M.; Goldhaber, S.Z. Anticoagulation and Hemostasis in Cardiac Surgical Patients. J. Card. Surg. 1994, 9, 443–461. [Google Scholar] [CrossRef] [PubMed]
- Parviainen, M.K.; Vahtera, A.; Ånäs, N.; Tähtinen, J.; Huhtala, H.; Kuitunen, A.; Järvelä, K. Anti-factor X Activity Levels with Continuous Intravenous Infusion and Subcutaneous Administration of Enoxaparin after Coronary Artery Bypass Grafting: A Randomized Clinical Trial. Acta Anaesthesiol. Scand. 2022, 66, 1083–1090. [Google Scholar] [CrossRef]
- Kulik, A.; Rubens, F.D.; Wells, P.S.; Kearon, C.; Mesana, T.G.; van Berkom, J.; Lam, B.-K. Early Postoperative Anticoagulation After Mechanical Valve Replacement: A Systematic Review. Ann. Thorac. Surg. 2006, 81, 770–778. [Google Scholar] [CrossRef]
- Jones, H.U.; Muhlestein, J.B.; Jones, K.W.; Renlund, D.G.; Bair, T.L.; Bunch, T.J.; Horne, B.D.; Lappé, D.L.; Anderson, J.L.; Doty, D.B. Early Postoperative Use of Unfractionated Heparin or Enoxaparin Is Associated with Increased Surgical Re-Exploration for Bleeding. Ann. Thorac. Surg. 2005, 80, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Cote, C.L.; Baghaffar, A.; Tremblay, P.; Herman, C. Incidence of Tamponade Following Temporary Epicardial Pacing Wire Removal. J. Card. Surg. 2020, 35, 1247–1252. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; Bonis, M.D.; Paulis, R.D.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart DiseaseDeveloped by the Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, ehab395. [Google Scholar] [CrossRef]
- Beller, J.P.; Krebs, E.D.; Hawkins, R.B.; Mehaffey, J.H.; Quader, M.A.; Speir, A.M.; Kiser, A.C.; Joseph, M.; Yarboro, L.T.; Teman, N.R.; et al. Non–Vitamin K Oral Anticoagulant Use after Cardiac Surgery Is Rapidly Increasing. J. Thorac. Cardiovasc. Surg. 2020, 160, 1222–1231. [Google Scholar] [CrossRef] [PubMed]
- Mannacio, V.A.; Mannacio, L.; Antignano, A.; Mauro, C.; Mastroroberto, P.; Musumeci, F.; Zebele, C.; Iannelli, G. New Oral Anticoagulants Versus Warfarin in Atrial Fibrillation After Early Postoperative Period in Patients With Bioprosthetic Aortic Valve. Ann. Thorac. Surg. 2022, 113, 75–82. [Google Scholar] [CrossRef]
- Myllykangas, M.E.; Kiviniemi, T.O.; Gunn, J.M.; Salomaa, V.V.; Pietilä, A.; Niiranen, T.J.; Aittokallio, J. Anticoagulation Therapy After Biologic Aortic Valve Replacement. Front. Cardiovasc. Med. 2021, 8, 698784. [Google Scholar] [CrossRef] [PubMed]
- Dangas, G.D.; Tijssen, J.G.P.; Wöhrle, J.; Søndergaard, L.; Gilard, M.; Möllmann, H.; Makkar, R.R.; Herrmann, H.C.; Giustino, G.; Baldus, S.; et al. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 120–129. [Google Scholar] [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. Dabigatran versus Warfarin in Patients with Mechanical Heart Valves. N. Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Steger, V.; Bail, D.H.; Graf, D.; Walker, T.; Rittig, K.; Ziemer, G. A Practical Approach for Bridging Anticoagulation after Mechanical Heart Valve Replacement. J. Heart Valve Dis. 2008, 17, 335–342. [Google Scholar] [PubMed]



| Characteristics | Number of Responses (n (%)) |
|---|---|
| Total population | 149 |
| Age (years) | |
| <30 | 3 (2) |
| 30 to 40 | 88 (59.1) |
| 40 to 50 | 31 (20.8) |
| >50 | 27 (18.1) |
| Years of practice in cardiac anesthesia | |
| <5 | 70 (47) |
| 6 to 10 | 29 (19.5) |
| 11 to 15 | 27 (18.1) |
| 16 to 20 | 8 (5.4) |
| >20 | 15 (10.1) |
| Position in the healthcare facility | |
| Professor or associate professor | 10 (6.7) |
| Attending physician | 114 (76.5) |
| Resident | 25 (16.8) |
| Type of hospital | |
| Academic hospital | 116 (77.9) |
| Nonacademic public hospital | 5 (3.4) |
| For-profit private facility | 21 (14.1) |
| Non-profit private facility | 7 (4.6) |
| Minimally invasive cardiac surgery (MICS) in the center | |
| Yes | 106 (71.1) |
| No | 43 (28.9) |
| Minimal extracorporeal circulation (MECC) | |
| Yes | 20 (13.5) |
| No | 128 (86.5) |
| Volume of on-pump heart surgery (cases per year) | |
| 250 to 499 | 26 (17.4) |
| 500 to 749 | 42 (28.2) |
| 750 to 1000 | 34 (22.8) |
| >1000 | 47 (31.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein, T.; Bignolas, H.; Mongardon, N.; Abou-Arab, O.; Guinot, P.G.; Bouglé, A.; Guerci, P. Practice Patterns of Antithrombotic Therapy during the Early Postoperative Course of Cardiac Surgery. J. Clin. Med. 2023, 12, 2029. https://doi.org/10.3390/jcm12052029
Klein T, Bignolas H, Mongardon N, Abou-Arab O, Guinot PG, Bouglé A, Guerci P. Practice Patterns of Antithrombotic Therapy during the Early Postoperative Course of Cardiac Surgery. Journal of Clinical Medicine. 2023; 12(5):2029. https://doi.org/10.3390/jcm12052029
Chicago/Turabian StyleKlein, Thomas, Hugo Bignolas, Nicolas Mongardon, Osama Abou-Arab, Pierre Grégoire Guinot, Adrien Bouglé, and Philippe Guerci. 2023. "Practice Patterns of Antithrombotic Therapy during the Early Postoperative Course of Cardiac Surgery" Journal of Clinical Medicine 12, no. 5: 2029. https://doi.org/10.3390/jcm12052029
APA StyleKlein, T., Bignolas, H., Mongardon, N., Abou-Arab, O., Guinot, P. G., Bouglé, A., & Guerci, P. (2023). Practice Patterns of Antithrombotic Therapy during the Early Postoperative Course of Cardiac Surgery. Journal of Clinical Medicine, 12(5), 2029. https://doi.org/10.3390/jcm12052029