
Seasonal Trends in the Prevalence and Incidence of Viral Encephalitis in Korea (2015–2019)

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Viral Surveillance Data
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
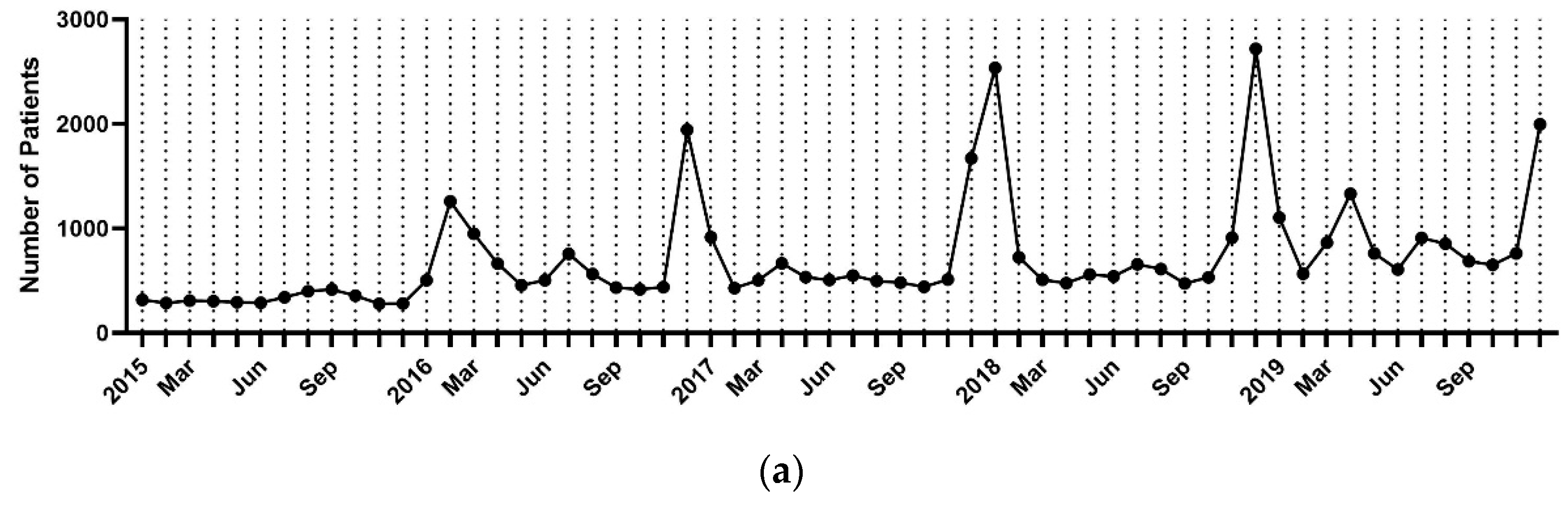
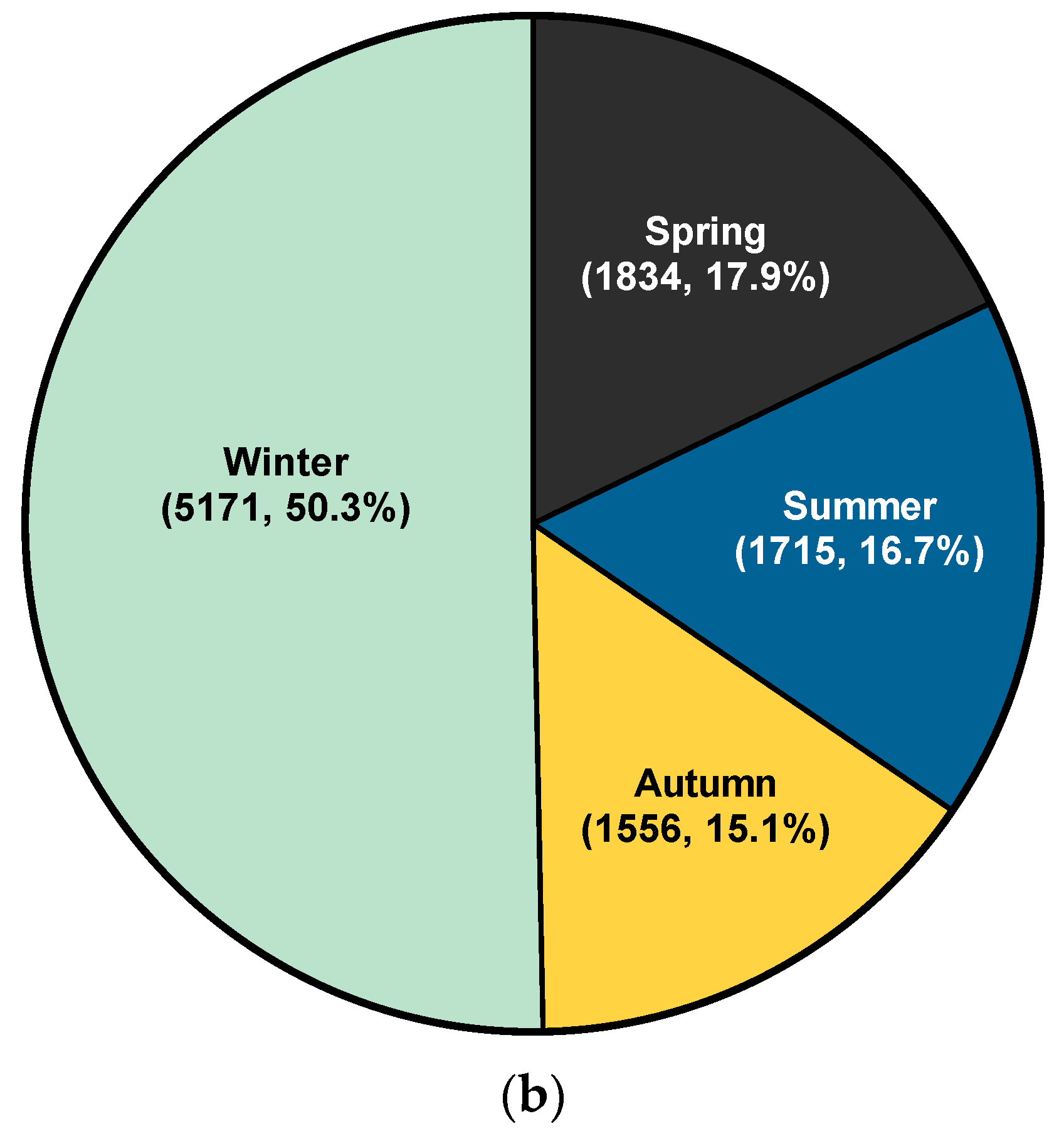
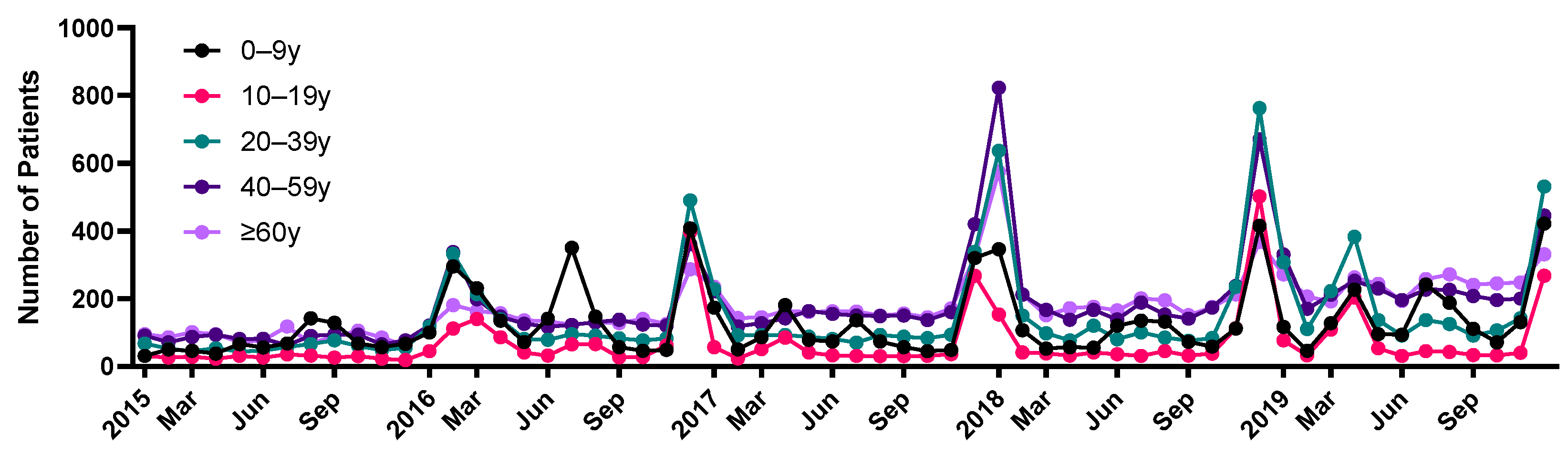
3.2. Encephalitis Trend Analysis
3.3. Viral Positive Detection Rates
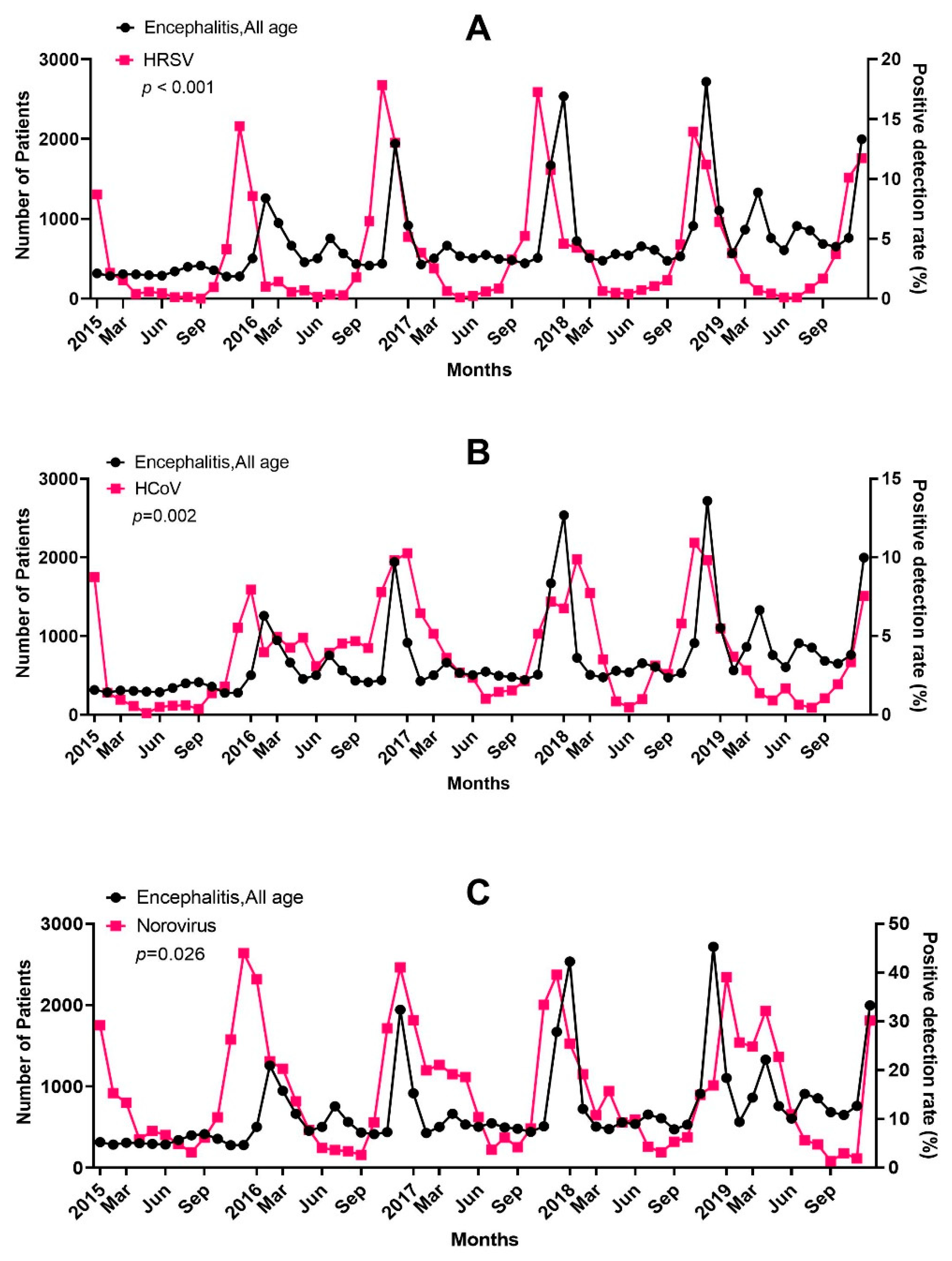
3.4. Causal Associations between Virus Prevalence and Encephalitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simon, D.W.; Da Silva, Y.S.; Zuccoli, G.; Clark, R.S. Acute encephalitis. Crit. Care Clin. 2013, 29, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Ellul, M.; Solomon, T. Acute encephalitis-diagnosis and management. Clin. Med. 2018, 18, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R. Understanding and managing acute encephalitis. F1000Research 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S. Introduction: Health of the health care system in Korea. Soc. Work Public Health 2010, 25, 127–141. [Google Scholar] [CrossRef]
- Kim, D.S. Special issue on the national health care system of South Korea. Soc. Work Public Health 2010, 25, 125–126. [Google Scholar] [CrossRef]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of Health Insurance Review and Assessment Service National Patient Samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef]
- Granger, C.W.J. Investigating Causal Relations by Econometric Models and Cross-spectral Methods. Econometrica 1969, 37, 424. [Google Scholar] [CrossRef]
- Lim, J.H.; Kim, Y.K.; Min, S.H.; Kim, S.W.; Lee, Y.H.; Lee, J.M. Seasonal Trends of Viral Prevalence and Incidence of Kawasaki Disease: A Korea Public Health Data Analysis. J. Clin. Med. 2021, 10, 3301. [Google Scholar] [CrossRef]
- Lim, J.H.; Kim, Y.K.; Min, S.H.; Kim, S.W.; Lee, Y.H.; Lee, J.M. Epidemiology and Viral Etiology of Pediatric Immune Thrombocytopenia through Korean Public Health Data Analysis. J. Clin. Med. 2021, 10, 1356. [Google Scholar] [CrossRef]
- Granerod, J.; Crowcroft, N.S. The epidemiology of acute encephalitis. Neuropsychol. Rehabil. 2007, 17, 406–428. [Google Scholar] [CrossRef]
- Granerod, J.; Cousens, S.; Davies, N.W.; Crowcroft, N.S.; Thomas, S.L. New estimates of incidence of encephalitis in England. Emerg. Infect. Dis. 2013, 19, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, A. Epidemiology and outcomes of acute encephalitis. Curr. Opin. Neurol. 2015, 28, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Khetsuriani, N.; Holman, R.C.; Anderson, L.J. Burden of encephalitis-associated hospitalizations in the United States, 1988–1997. Clin. Infect. Dis. 2002, 35, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Vora, N.M.; Holman, R.C.; Mehal, J.M.; Steiner, C.A.; Blanton, J.; Sejvar, J. Burden of encephalitis-associated hospitalizations in the United States, 1998–2010. Neurology 2014, 82, 443–451. [Google Scholar] [CrossRef] [PubMed]
- George, B.P.; Schneider, E.B.; Venkatesan, A. Encephalitis hospitalization rates and inpatient mortality in the United States, 2000–2010. PLoS ONE 2014, 9, e104169. [Google Scholar] [CrossRef]
- Messacar, K.; Fischer, M.; Dominguez, S.R.; Tyler, K.L.; Abzug, M.J. Encephalitis in US Children. Infect. Dis. Clin. N. Am. 2018, 32, 145–162. [Google Scholar] [CrossRef]
- Bernard, S.; Mailles, A.; Stahl, J.P.; Steering, C.; Investigators, G. Epidemiology of infectious encephalitis, differences between a prospective study and hospital discharge data. Epidemiol. Infect. 2013, 141, 2256–2268. [Google Scholar] [CrossRef]
- Jmor, F.; Emsley, H.C.; Fischer, M.; Solomon, T.; Lewthwaite, P. The incidence of acute encephalitis syndrome in Western industrialised and tropical countries. Virol. J. 2008, 5, 134. [Google Scholar] [CrossRef]
- Wang, H.; Zhao, S.; Wang, S.; Zheng, Y.; Wang, S.; Chen, H.; Pang, J.; Ma, J.; Yang, X.; Chen, Y. Global magnitude of encephalitis burden and its evolving pattern over the past 30 years. J. Infect. 2022, 84, 777–787. [Google Scholar] [CrossRef]
- Stone, M.J.; Hawkins, C.P. A medical overview of encephalitis. Neuropsychol. Rehabil. 2007, 17, 429–449. [Google Scholar] [CrossRef]
- Lewis, P.; Glaser, C.A. Encephalitis. Pediatr. Rev. 2005, 26, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.G.; Carlson, S.; Cheng, A.C.; Chilver, M.B.; Dwyer, D.E.; Irwin, M.; Kok, J.; Macartney, K.; MacLachlan, J.; Minney-Smith, C.; et al. Where has all the influenza gone? The impact of COVID-19 on the circulation of influenza and other respiratory viruses, Australia, March to September 2020. Euro. Surveill. 2020, 25, 2001847. [Google Scholar] [CrossRef] [PubMed]
- Van Brusselen, D.; De Troeyer, K.; Ter Haar, E.; Vander Auwera, A.; Poschet, K.; Van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; Van Herendael, B.; et al. Bronchiolitis in COVID-19 times: A nearly absent disease? Eur. J. Pediatr. 2021, 180, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Nagakumar, P.; Chadwick, C.L.; Bush, A.; Gupta, A. Collateral impact of COVID-19: Why should children continue to suffer? Eur. J. Pediatr. 2021, 180, 1975–1979. [Google Scholar] [CrossRef]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef]
- Agha, R.; Avner, J.R. Delayed Seasonal RSV Surge Observed During the COVID-19 Pandemic. Pediatrics 2021, 148, e2021052089. [Google Scholar] [CrossRef]
- Andrade, C.A.; Kalergis, A.M.; Bohmwald, K. Potential Neurocognitive Symptoms Due to Respiratory Syncytial Virus Infection. Pathogens 2021, 11, 47. [Google Scholar] [CrossRef]
- Rozenberg, F. Acute viral encephalitis. Handb. Clin. Neurol. 2013, 112, 1171–1181. [Google Scholar] [CrossRef]
- Venkatesan, A.; Murphy, O.C. Viral Encephalitis. Neurol. Clin. 2018, 36, 705–724. [Google Scholar] [CrossRef]
- Bohmwald, K.; Galvez, N.M.S.; Rios, M.; Kalergis, A.M. Neurologic Alterations Due to Respiratory Virus Infections. Front. Cell Neurosci. 2018, 12, 386. [Google Scholar] [CrossRef]
- Saravanos, G.L.; King, C.L.; Deng, L.; Dinsmore, N.; Ramos, I.; Takashima, M.; Crawford, N.; Clark, J.E.; Dale, R.C.; Jones, C.A.; et al. Respiratory Syncytial Virus-Associated Neurologic Complications in Children: A Systematic Review and Aggregated Case Series. J. Pediatr. 2021, 239, 39–49.e39. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Soto, J.A.; Andrade-Parra, C.; Fernandez-Fierro, A.; Espinoza, J.A.; Rios, M.; Eugenin, E.A.; Gonzalez, P.A.; Opazo, M.C.; Riedel, C.A.; et al. Lung pathology due to hRSV infection impairs blood-brain barrier permeability enabling astrocyte infection and a long-lasting inflammation in the CNS. Brain Behav. Immun. 2021, 91, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Muhammad Ismail, H.I.; Teh, C.M.; Lee, Y.L.; National Paediatric, H.N.S.G. Neurologic manifestations and complications of pandemic influenza A H1N1 in Malaysian children: What have we learnt from the ordeal? Brain Dev. 2015, 37, 120–129. [Google Scholar] [CrossRef]
- Morishima, T.; Togashi, T.; Yokota, S.; Okuno, Y.; Miyazaki, C.; Tashiro, M.; Okabe, N.; Collaborative Study Group on Influenza-Associated Encephalopathy in Japan. Encephalitis and encephalopathy associated with an influenza epidemic in Japan. Clin. Infect. Dis. 2002, 35, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Meijer, W.J.; Linn, F.H.; Wensing, A.M.; Leavis, H.L.; van Riel, D.; GeurtsvanKessel, C.H.; Wattjes, M.P.; Murk, J.L. Acute influenza virus-associated encephalitis and encephalopathy in adults: A challenging diagnosis. JMM Case Rep. 2016, 3, e005076. [Google Scholar] [CrossRef] [PubMed]
- Newland, J.G.; Laurich, V.M.; Rosenquist, A.W.; Heydon, K.; Licht, D.J.; Keren, R.; Zaoutis, T.E.; Watson, B.; Hodinka, R.L.; Coffin, S.E. Neurologic complications in children hospitalized with influenza: Characteristics, incidence, and risk factors. J. Pediatr. 2007, 150, 306–310. [Google Scholar] [CrossRef]
- Britton, P.N.; Blyth, C.C.; Macartney, K.; Dale, R.C.; Li-Kim-Moy, J.; Khandaker, G.; Crawford, N.W.; Marshall, H.; Clark, J.E.; Elliott, E.J.; et al. The Spectrum and Burden of Influenza-Associated Neurological Disease in Children: Combined Encephalitis and Influenza Sentinel Site Surveillance from Australia, 2013–2015. Clin. Infect. Dis. 2017, 65, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.J.; Park, J.Y.; Choi, J.S.; Choi, S.R.; Kim, D.; Lee, J.H.; Woo, Y.J.; Lee, J.; Kim, Y.J. Influenza-associated Neurologic Complications in Hospitalized Pediatric Patients: A Multicenter Retrospective Study in Republic of Korea. Pediatr. Infect. Dis. J. 2021, 40, e466–e471. [Google Scholar] [CrossRef]
- Espinet-Coll, E.; Nebreda-Duran, J.; Lopez-Nava Breviere, G.; Coordinadores del Grupo Espanol de Trabajo para el Tratamiento Endoscopico del Metabolismo y la Obesidad (GETTEMO). Gastric perforation by intragastric balloon in a patient with Nissen fundoplication. Response of the Spanish Bariatric Endoscopy Group. Gastroenterol. Hepatol. 2018, 41, 583–584. [Google Scholar] [CrossRef]
- Kaida, A.; Iritani, N.; Kubo, H.; Shiomi, M.; Kohdera, U.; Murakami, T. Seasonal distribution and phylogenetic analysis of human metapneumovirus among children in Osaka City, Japan. J. Clin. Virol. 2006, 35, 394–399. [Google Scholar] [CrossRef]
- Sanchez Fernandez, I.; Rebollo Polo, M.; Munoz-Almagro, C.; Monfort Carretero, L.; Fernandez Urena, S.; Rueda Munoz, A.; Colome Roura, R.; Perez Duenas, B. Human Metapneumovirus in the Cerebrospinal Fluid of a Patient With Acute Encephalitis. Arch. Neurol. 2012, 69, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Fok, A.; Mateevici, C.; Lin, B.; Chandra, R.V.; Chong, V.H. Encephalitis-Associated Human Metapneumovirus Pneumonia in Adult, Australia. Emerg. Infect. Dis. 2015, 21, 2074–2076. [Google Scholar] [CrossRef] [PubMed]
- Hazama, K.; Shiihara, T.; Tsukagoshi, H.; Matsushige, T.; Dowa, Y.; Watanabe, M. Rhinovirus-associated acute encephalitis/encephalopathy and cerebellitis. Brain Dev. 2019, 41, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Liu, Y.; Feng, Z.; Feng, Q.; Li, K.; Gao, H.; Qian, S.; Xu, L.; Xie, Z. A fatal case of viral sepsis and encephalitis in a child caused by human adenovirus type 7 infection. Virol. J. 2022, 19, 154. [Google Scholar] [CrossRef]
- Mitui, M.T.; Tabib, S.M.; Matsumoto, T.; Khanam, W.; Ahmed, S.; Mori, D.; Akhter, N.; Yamada, K.; Kabir, L.; Nishizono, A.; et al. Detection of human bocavirus in the cerebrospinal fluid of children with encephalitis. Clin. Infect. Dis. 2012, 54, 964–967. [Google Scholar] [CrossRef]
- Yu, J.M.; Chen, Q.Q.; Hao, Y.X.; Yu, T.; Zeng, S.Z.; Wu, X.B.; Zhang, B.; Duan, Z.J. Identification of human bocaviruses in the cerebrospinal fluid of children hospitalized with encephalitis in China. J. Clin. Virol. 2013, 57, 374–377. [Google Scholar] [CrossRef]
- Mori, D.; Ranawaka, U.; Yamada, K.; Rajindrajith, S.; Miya, K.; Perera, H.K.; Matsumoto, T.; Dassanayake, M.; Mitui, M.T.; Mori, H.; et al. Human bocavirus in patients with encephalitis, Sri Lanka, 2009–2010. Emerg. Infect. Dis. 2013, 19, 1859–1862. [Google Scholar] [CrossRef]
- Lee, K.Y. Rotavirus infection-associated central nervous system complications: Clinicoradiological features and potential mechanisms. Clin. Exp. Pediatr. 2022, 65, 483–493. [Google Scholar] [CrossRef]
- Hellysaz, A.; Hagbom, M. Understanding the Central Nervous System Symptoms of Rotavirus: A Qualitative Review. Viruses 2021, 13, 658. [Google Scholar] [CrossRef]
- Uemura, N.; Okumura, A.; Negoro, T.; Watanabe, K. Clinical features of benign convulsions with mild gastroenteritis. Brain Dev. 2002, 24, 745–749. [Google Scholar] [CrossRef]
- Kasai, M.; Shibata, A.; Hoshino, A.; Maegaki, Y.; Yamanouchi, H.; Takanashi, J.I.; Yamagata, T.; Sakuma, H.; Okumura, A.; Nagase, H.; et al. Epidemiological changes of acute encephalopathy in Japan based on national surveillance for 2014–2017. Brain Dev. 2020, 42, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Takanashi, J.; Miyamoto, T.; Ando, N.; Kubota, T.; Oka, M.; Kato, Z.; Hamano, S.; Hirabayashi, S.; Kikuchi, M.; Barkovich, A.J. Clinical and radiological features of rotavirus cerebellitis. Am. J. Neuroradiol. 2010, 31, 1591–1595. [Google Scholar] [CrossRef] [PubMed]
- Ushijima, H.; Bosu, K.; Abe, T.; Shinozaki, T. Suspected rotavirus encephalitis. Arch. Dis. Child. 1986, 61, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Conway, S.P. Rotavirus encephalitis. Arch. Dis. Child. 1988, 63, 224. [Google Scholar] [CrossRef] [PubMed]
- Shiihara, T.; Watanabe, M.; Honma, A.; Kato, M.; Morita, Y.; Ichiyama, T.; Maruyama, K. Rotavirus associated acute encephalitis/encephalopathy and concurrent cerebellitis: Report of two cases. Brain Dev. 2007, 29, 670–673. [Google Scholar] [CrossRef]
- Kobayashi, S.; Negishi, Y.; Ando, N.; Ito, T.; Nakano, M.; Togari, H.; Wakuda, M.; Taniguchi, K. Two patients with acute rotavirus encephalitis associated with cerebellar signs and symptoms. Eur. J. Pediatr. 2010, 169, 1287–1291. [Google Scholar] [CrossRef]
- Ueda, H.; Tajiri, H.; Kimura, S.; Etani, Y.; Hosoi, G.; Maruyama, T.; Noma, H.; Kusumoto, Y.; Takano, T.; Baba, Y.; et al. Clinical characteristics of seizures associated with viral gastroenteritis in children. Epilepsy. Res. 2015, 109, 146–154. [Google Scholar] [CrossRef]
- Paketci, C.; Edem, P.; Okur, D.; Sarioglu, F.C.; Guleryuz, H.; Bayram, E.; Kurul, S.H.; Yis, U. Rotavirus encephalopathy with concomitant acute cerebellitis: Report of a case and review of the literature. Turk. J. Pediatr. 2020, 62, 119–124. [Google Scholar] [CrossRef]
- Soares-Weiser, K.; Maclehose, H.; Bergman, H.; Ben-Aharon, I.; Nagpal, S.; Goldberg, E.; Pitan, F.; Cunliffe, N. Vaccines for preventing rotavirus diarrhoea: Vaccines in use. Cochrane Database Syst. Rev. 2012, 11, CD008521. [Google Scholar] [CrossRef]
- Becker-Dreps, S.; Bucardo, F.; Vilchez, S.; Zambrana, L.E.; Liu, L.; Weber, D.J.; Pena, R.; Barclay, L.; Vinje, J.; Hudgens, M.G.; et al. Etiology of childhood diarrhea after rotavirus vaccine introduction: A prospective, population-based study in Nicaragua. Pediatr. Infect. Dis. J. 2014, 33, 1156–1163. [Google Scholar] [CrossRef]
- Burnett, E.; Parashar, U.D.; Tate, J.E. Real-world effectiveness of rotavirus vaccines, 2006–2019: A literature review and meta-analysis. Lancet. Glob. Health 2020, 8, e1195–e1202. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Takeshita, S.; Nezu, A.; Aihara, Y.; Usuku, S.; Noguchi, Y.; Yokota, S. Norovirus-associated encephalopathy. Pediatr. Infect. Dis. J. 2006, 25, 651–652. [Google Scholar] [CrossRef] [PubMed]
- Obinata, K.; Okumura, A.; Nakazawa, T.; Kamata, A.; Niizuma, T.; Kinoshita, K.; Shimizu, T. Norovirus encephalopathy in a previously healthy child. Pediatr. Infect. Dis. J. 2010, 29, 1057–1059. [Google Scholar] [CrossRef] [PubMed]
- Kimura, E.; Goto, H.; Migita, A.; Harada, S.; Yamashita, S.; Hirano, T.; Uchino, M. An adult norovirus-related encephalitis/encephalopathy with mild clinical manifestation. BMJ Case Rep. 2010, 2010, bcr0320102784. [Google Scholar] [CrossRef]
- Sanchez-Fauquier, A.; Gonzalez-Galan, V.; Arroyo, S.; Roda, D.; Pons, M.; Garcia, J.J. Norovirus-associated encephalitis in a previously healthy 2-year-old girl. Pediatr. Infect. Dis. J. 2015, 34, 222–223. [Google Scholar] [CrossRef]
- Shima, T.; Okumura, A.; Kurahashi, H.; Numoto, S.; Abe, S.; Ikeno, M.; Shimizu, T.; Norovirus-associated Encephalitis/Encephalopathy Collaborative Study, i. A nationwide survey of norovirus-associated encephalitis/encephalopathy in Japan. Brain Dev. 2019, 41, 263–270. [Google Scholar] [CrossRef]
- Kawano, G.; Oshige, K.; Syutou, S.; Koteda, Y.; Yokoyama, T.; Kim, B.G.; Mizuochi, T.; Nagai, K.; Matsuda, K.; Ohbu, K.; et al. Benign infantile convulsions associated with mild gastroenteritis: A retrospective study of 39 cases including virological tests and efficacy of anticonvulsants. Brain Dev. 2007, 29, 617–622. [Google Scholar] [CrossRef]
- Chen, S.Y.; Tsai, C.N.; Lai, M.W.; Chen, C.Y.; Lin, K.L.; Lin, T.Y.; Chiu, C.H. Norovirus infection as a cause of diarrhea-associated benign infantile seizures. Clin. Infect. Dis. 2009, 48, 849–855. [Google Scholar] [CrossRef]
- Hasbun, R.; Wootton, S.H.; Rosenthal, N.; Balada-Llasat, J.M.; Chung, J.; Duff, S.; Bozzette, S.; Zimmer, L.; Ginocchio, C.C. Epidemiology of Meningitis and Encephalitis in Infants and Children in the United States, 2011–2014. Pediatr. Infect. Dis. J. 2019, 38, 37–41. [Google Scholar] [CrossRef]
- Hasbun, R.; Rosenthal, N.; Balada-Llasat, J.M.; Chung, J.; Duff, S.; Bozzette, S.; Zimmer, L.; Ginocchio, C.C. Epidemiology of Meningitis and Encephalitis in the United States, 2011–2014. Clin. Infect. Dis. 2017, 65, 359–363. [Google Scholar] [CrossRef]
- Chen, B.S.; Lee, H.C.; Lee, K.M.; Gong, Y.N.; Shih, S.R. Enterovirus and Encephalitis. Front. Microbiol. 2020, 11, 261. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.X.; Terasaki, T.; Shiroki, K.; Ohka, S.; Aoki, J.; Tanabe, S.; Nomura, T.; Terada, E.; Sugiyama, Y.; Nomoto, A. Efficient delivery of circulating poliovirus to the central nervous system independently of poliovirus receptor. Virology 1997, 229, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Gromeier, M.; Wimmer, E. Mechanism of injury-provoked poliomyelitis. J. Virol. 1998, 72, 5056–5060. [Google Scholar] [CrossRef]
- Chen, C.S.; Yao, Y.C.; Lin, S.C.; Lee, Y.P.; Wang, Y.F.; Wang, J.R.; Liu, C.C.; Lei, H.Y.; Yu, C.K. Retrograde axonal transport: A major transmission route of enterovirus 71 in mice. J. Virol. 2007, 81, 8996–9003. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.C.; Badmanathan, M.; Devi, S.; Leong, K.L.; Cardosa, M.J.; Wong, K.T. Pathologic characterization of a murine model of human enterovirus 71 encephalomyelitis. J. Neuropathol. Exp. Neurol. 2008, 67, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Rhoades, R.E.; Tabor-Godwin, J.M.; Tsueng, G.; Feuer, R. Enterovirus infections of the central nervous system. Virology 2011, 411, 288–305. [Google Scholar] [CrossRef] [PubMed]
- Quan, P.L.; Wagner, T.A.; Briese, T.; Torgerson, T.R.; Hornig, M.; Tashmukhamedova, A.; Firth, C.; Palacios, G.; Baisre-De-Leon, A.; Paddock, C.D.; et al. Astrovirus encephalitis in boy with X-linked agammaglobulinemia. Emerg. Infect. Dis. 2010, 16, 918–925. [Google Scholar] [CrossRef]
- Vu, D.L.; Cordey, S.; Brito, F.; Kaiser, L. Novel human astroviruses: Novel human diseases? J. Clin. Virol. 2016, 82, 56–63. [Google Scholar] [CrossRef]
- Koukou, G.; Niendorf, S.; Hornei, B.; Schlump, J.U.; Jenke, A.C.; Jacobsen, S. Human astrovirus infection associated with encephalitis in an immunocompetent child: A case report. J. Med. Case Rep. 2019, 13, 341. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N (%) | |
|---|---|---|
| Total number of patients | 42,775 (100.0) | |
| Age group | ||
| 0–9.99 years | 7710 (18.0) | |
| 10~19.99 years | 4224 (9.9) | |
| 20~39.99 years | 8890 (20.8) | |
| 40–59.99 years | 11,233 (26.3) | |
| ≥60 years | 10,718 (25.1) | |
| Sex | ||
| Male | 20,760 (48.5) | |
| Female | 22,015 (51.5) | |
| Location | ||
| Seoul | 11,116 (26.0) | |
| Busan | 3225 (7.5) | |
| Incheon | 1927 (4.5) | |
| Daegu | 1567 (3.7) | |
| Gwangju | 2698 (6.3) | |
| Daejeon | 1077 (2.5) | |
| Ulsan | 582 (1.4) | |
| Gyeonggi | 8656 (20.2) | |
| Gangwon | 1930 (4.5) | |
| Chungbuk | 706 (1.7) | |
| Chungnam | 1492 (3.5) | |
| Jeonbuk | 1594 (3.7) | |
| Jeonnam | 911 (2.1) | |
| Gyeongbuk | 1798 (4.2) | |
| Gyeongnam | 2660 (6.2) | |
| Jeju | 708 (1.7) | |
| Sejong | 128 (0.3) | |
| Insurance type | ||
| Medical insurance | 40,839 (95.5) | |
| Medical aid | 1918 (4.5) | |
| Free | 18 (0.0) |
| Age Group (Years) | Annual Incidence * (Annual Incidence Rate) ** | Overall Incidence Rate | Relative Risk *** | ||||
|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2018 | 2019 | |||
| 0–9 | 818 (17.8) | 2047 (44.5) | 1375 (29.9) | 1779 (38.7) | 2067 (44.9) | 35.1 | 2.79 |
| 10–19 | 331 (5.8) | 1148 (20.1) | 773 (13.5) | 1230 (21.5) | 1119 (19.6) | 16.1 | 1.28 |
| 20–39 | 673 (4.7) | 1894 (13.2) | 1463 (10.2) | 2554 (17.8) | 2468 (17.2) | 12.6 | 1.00 |
| 40–59 | 989 (5.8) | 2039 (11.9) | 2095 (12.2) | 3226 (18.8) | 2916 (17.0) | 13.1 | 1.04 |
| ≥60 | 1054 (10.9) | 1737 (18.0) | 1919 (19.9) | 2377 (24.6) | 2429 (25.2) | 19.7 | 1.56 |
| Total | 3865 (7.5) | 8865 (17.2) | 7625 (14.7) | 11,166 (21.5) | 10,999 (21.2) | 16.4 | 1.30 |
| Year | Jan | Feb | Mar | Apr | May | Jun | Jul | Aug | Sep | Oct | Nov | Dec | Total | Average |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 316 | 285 | 308 | 304 | 294 | 288 | 341 | 399 | 415 | 357 | 278 | 280 | 3865 | 322 |
| 2016 | 503 | 1259 | 948 | 664 | 456 | 503 | 756 | 564 | 433 | 415 | 439 | 1943 | 8883 | 740 |
| 2017 | 917 | 428 | 503 | 665 | 533 | 506 | 549 | 496 | 481 | 442 | 510 | 1672 | 7702 | 642 |
| 2018 | 2535 | 723 | 508 | 476 | 559 | 540 | 656 | 610 | 473 | 530 | 911 | 2718 | 11,239 | 937 |
| 2019 | 1104 | 565 | 864 | 1330 | 760 | 606 | 909 | 854 | 685 | 651 | 761 | 1997 | 11,086 | 924 |
| Total | 5375 | 3260 | 3131 | 3439 | 2602 | 2443 | 3211 | 2923 | 2487 | 2395 | 2899 | 8610 | 42,775 | 3565 |
| Average | 946 | 513 | 488 | 512 | 447 | 466 | 550 | 491 | 391 | 362 | 403 | 917 | 71,341 | 540 |
| Age Group (Years) | HAdV | HPIV | HRSV | IFV | HCoV | HRV | HBoV | HMPV | Rotavirus | Norovirus | Adenovirus | Astrovirus |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0–9 | 0.885 | 0.894 | <0.001 | 0.521 | 0.021 | 0.447 | 0.556 | 0.377 | 0.965 | 0.112 | 0.589 | 0.668 |
| 10–19 | 0.89 | 0.345 | <0.001 | 0.569 | 0.004 | 0.882 | 0.873 | 0.83 | 0.615 | 0.134 | 0.821 | 0.493 |
| 20–39 | 0.93 | 0.485 | <0.001 | 0.572 | <0.001 | 0.263 | 0.895 | 0.658 | 0.985 | 0.046 | 0.646 | 0.932 |
| 40–59 | 0.98 | 0.683 | <0.001 | 0.139 | 0.001 | 0.072 | 0.789 | 0.646 | 0.662 | 0.011 | 0.545 | 0.898 |
| ≥60 | 0.542 | 0.66 | 0.001 | 0.041 | 0.012 | 0.097 | 0.463 | 0.497 | 0.596 | 0.002 | 0.512 | 0.913 |
| total | 0.938 | 0.63 | <0.001 | 0.74 | 0.002 | 0.302 | 0.759 | 0.587 | 0.958 | 0.026 | 0.569 | 0.901 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.J.; Kim, J.M.; Keum, H.R.; Kim, S.W.; Baek, H.S.; Byun, J.C.; Kim, Y.K.; Kim, S.; Lee, J.M. Seasonal Trends in the Prevalence and Incidence of Viral Encephalitis in Korea (2015–2019). J. Clin. Med. 2023, 12, 2003. https://doi.org/10.3390/jcm12052003
Lee SJ, Kim JM, Keum HR, Kim SW, Baek HS, Byun JC, Kim YK, Kim S, Lee JM. Seasonal Trends in the Prevalence and Incidence of Viral Encephalitis in Korea (2015–2019). Journal of Clinical Medicine. 2023; 12(5):2003. https://doi.org/10.3390/jcm12052003
Chicago/Turabian StyleLee, Seon Jin, Jeong Min Kim, Ha Rim Keum, Sang Won Kim, Hee Sun Baek, Jun Chul Byun, Yu Kyung Kim, Saeyoon Kim, and Jae Min Lee. 2023. "Seasonal Trends in the Prevalence and Incidence of Viral Encephalitis in Korea (2015–2019)" Journal of Clinical Medicine 12, no. 5: 2003. https://doi.org/10.3390/jcm12052003
APA StyleLee, S. J., Kim, J. M., Keum, H. R., Kim, S. W., Baek, H. S., Byun, J. C., Kim, Y. K., Kim, S., & Lee, J. M. (2023). Seasonal Trends in the Prevalence and Incidence of Viral Encephalitis in Korea (2015–2019). Journal of Clinical Medicine, 12(5), 2003. https://doi.org/10.3390/jcm12052003