
A Review of Parental Vaccine Hesitancy for Human Papillomavirus in Japan
Abstract
1. Introduction
2. Method
2.1. Search and Selection Procedure
2.2. Analysis
3. Results
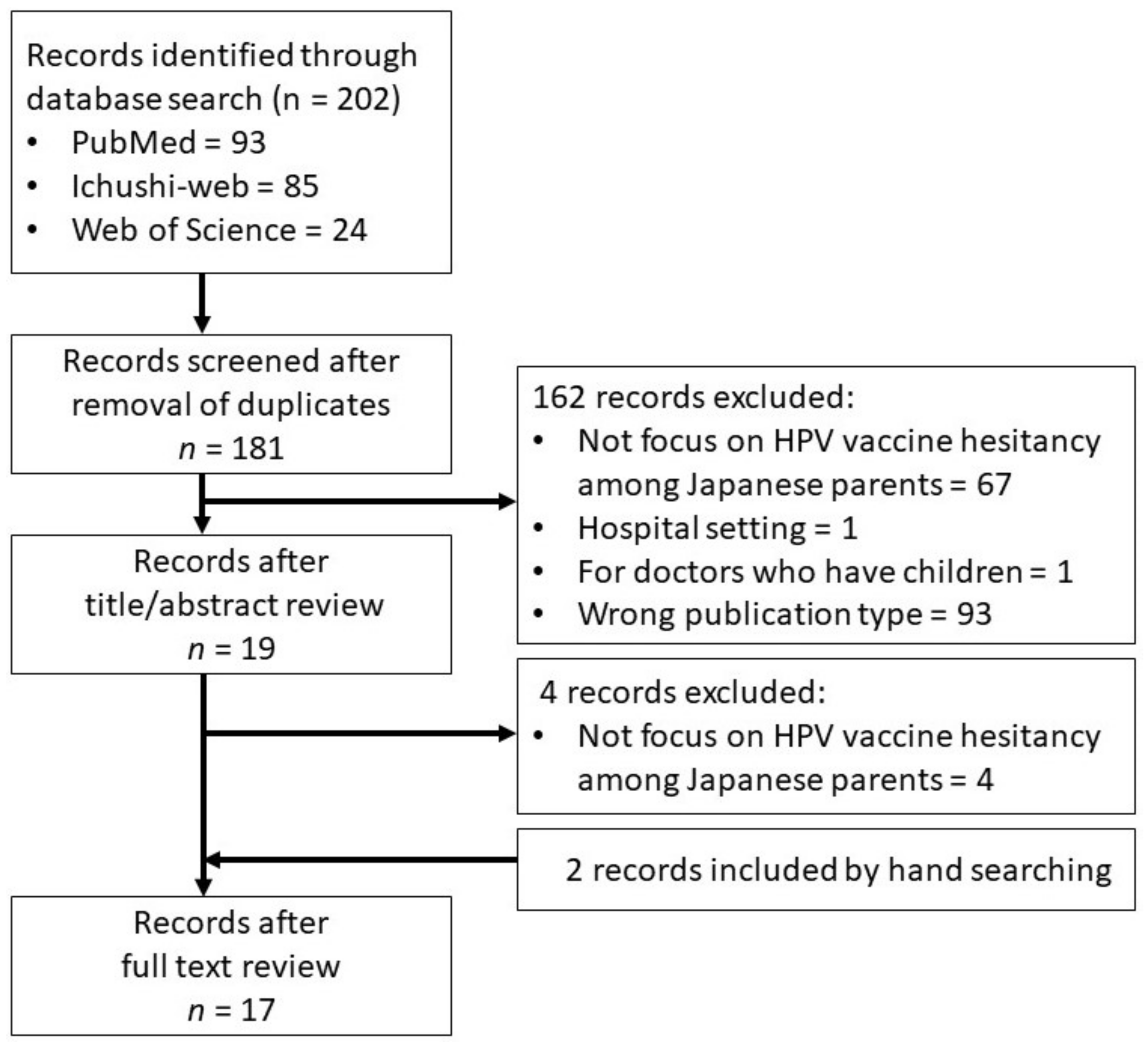
3.1. Search Results and Survey Characteristics
3.2. Perceptions of Risk and Benefits
3.3. Trust and Recommendation
3.4. Information and Knowledge
3.5. Sociodemographic Characteristics
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MacDonald, N.E.; the SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Lee, L.A.; Liu, Y.; Scherpbier, R.W.; Wen, N.; Zhang, G.; Zhu, X.; Ning, G.; Wang, F.; Li, Y.; et al. Vaccine-preventable disease control in the People’s Republic of China: 1949–2016. Vaccine 2018, 36, 8131–8137. [Google Scholar] [CrossRef] [PubMed]
- Roush, S.W.; Murphy, T.V.; Vaccine-Preventable Disease Table Working Group. Historical comparisons of morbidity and mortality for vaccine-preventable diseases in the United States. JAMA 2007, 298, 2155–2163. [Google Scholar] [CrossRef] [PubMed]
- Bagcchi, S. India tackles vaccine preventable diseases. Lancet Infect. Dis. 2015, 15, 637–638. [Google Scholar] [CrossRef]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 7 May 2022).
- Dube, E.; Gagnon, D.; MacDonald, N.; Bocquier, A.; Peretti-Watel, P.; Verger, P. Underlying factors impacting vaccine hesitancy in high income countries: A review of qualitative studies. Expert Rev. Vaccines 2018, 17, 989–1004. [Google Scholar] [CrossRef]
- De Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Shimizu, K.; Sorano, S.; Iwai, K. Vaccine hesitancy in Japan: Is the country well prepared for Tokyo 2020? Travel Med. Infect. Dis. 2020, 34, 101609. [Google Scholar] [CrossRef]
- Oyouni, A.A.A. Human papillomavirus in cancer: Infection, disease transmission, and progress in vaccines. J. Infect. Public Health 2023, in press. [Google Scholar] [CrossRef]
- Wu, J.; Xiao, F.; Zheng, Y.; Lin, Y.; Wang, H.L. Worldwide trend in human papillomavirus-attributable cancer incidence rates between 1990 and 2012 and Bayesian projection to 2030. Cancer 2021, 127, 3172–3182. [Google Scholar] [CrossRef]
- Ueda, Y.; Yagi, A.; Ikeda, S.; Enomoto, T.; Kimura, T. Beyond resumption of the Japanese Government’s recommendation of the HPV vaccine. Lancet Oncol. 2018, 19, 1563–1564. [Google Scholar] [CrossRef]
- Ministry of Health, Labour, and Welfare. 副反応追跡調査結果について [Adverse Effect Follow-Up Survey Results]. Available online: https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou28/chousa/index.html (accessed on 1 June 2022).
- Morimoto, A.; Ueda, Y.; Egawa-Takata, T.; Yagi, A.; Terai, Y.; Ohmichi, M.; Ichimura, T.; Sumi, T.; Murata, H.; Kanzaki, H.; et al. Effect on HPV vaccination in Japan resulting from news report of adverse events and suspension of governmental recommendation for HPV vaccination. Int. J. Clin. Oncol. 2015, 20, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Hanley, S.J.; Yoshioka, E.; Ito, Y.; Kishi, R. HPV vaccination crisis in Japan. Lancet 2015, 385, 2571. [Google Scholar] [CrossRef] [PubMed]
- Simms, K.T.; Hanley, S.J.B.; Smith, M.A.; Keane, A.; Canfell, K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: A modelling study. Lancet Public Health 2020, 5, e223–e234. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Center. がん種別統計情報 子宮頚部 [Statistics by Type of Cancer: Cervix]. Available online: https://ganjoho.jp/reg_stat/statistics/stat/cancer/17_cervix_uteri.html#anchor1 (accessed on 30 January 2022).
- Yagi, A.; Ueda, Y.; Kakuda, M.; Nakagawa, S.; Hiramatsu, K.; Miyoshi, A.; Kobayashi, E.; Kimura, T.; Kurosawa, M.; Yamaguchi, M.; et al. Cervical Cancer Protection in Japan: Where Are We? Vaccines 2021, 9, 1263. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Wilson, R.; Hanley, S.; Parys, A.; Paterson, P. Tracking the global spread of vaccine sentiments: The global response to Japan’s suspension of its HPV vaccine recommendation. Hum. Vaccines Immunother. 2014, 10, 2543–2550. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Santhanes, D.; Wong, C.P.; Yap, Y.Y.; San, S.P.; Chaiyakunapruk, N.; Khan, T.M. Factors involved in human papillomavirus (HPV) vaccine hesitancy among women in the South-East Asian Region (SEAR) and Western Pacific Region (WPR): A scoping review. Hum. Vaccines Immunother. 2018, 14, 124–133. [Google Scholar] [CrossRef]
- Whelan, S.O.; Moriarty, F.; Lawlor, L.; Gorman, K.M.; Beamish, J. Vaccine hesitancy and reported non-vaccination in an Irish pediatric outpatient population. Eur. J. Pediatr. 2021, 180, 2839–2847. [Google Scholar] [CrossRef]
- Cunningham-Erves, J.; Koyama, T.; Huang, Y.; Jones, J.; Wilkins, C.H.; Harnack, L.; McAfee, C.; Hull, P.C. Providers’ Perceptions of Parental Human Papillomavirus Vaccine Hesitancy: Cross-Sectional Study. JMIR Cancer 2019, 5, e13832. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Shuto, M.; Kim, Y.; Okuyama, K.; Ouchi, K.; Ueichi, H.; Nnadi, C.; Larson, H.J.; Perez, G.; Sasaki, S. Understanding confidence in the human papillomavirus vaccine in Japan: A web-based survey of mothers, female adolescents, and healthcare professionals. Hum. Vaccines Immunother. 2021, 17, 3102–3112. [Google Scholar] [CrossRef]
- Miyoshi, A.; Takiuchi, T.; Kimura, T. HPV vaccination in Japan: Can educational intervention promote a father’s intention to encourage his daughter’s vaccination? Int. J. Clin. Oncol. 2020, 25, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Egawa-Takata, T.; Nakae, R.; Shindo, M.; Miyoshi, A.; Takiuchi, T.; Miyatake, T.; Kimura, T. Fathers’ participation in the HPV vaccination decision-making process doesn’t increase parents’ intention to make daughters get the vaccine. Hum. Vaccines Immunother. 2020, 16, 1653–1658. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Sukegawa, A.; Ueda, Y.; Sekine, M.; Enomoto, T.; Miyagi, E. Effect of a Brief Web-Based Educational Intervention on Willingness to Consider Human Papillomavirus Vaccination for Children in Japan: Randomized Controlled Trial. J. Med. Internet Res. 2021, 23, e28355. [Google Scholar] [CrossRef]
- Suzuki, Y.; Sukegawa, A.; Ueda, Y.; Sekine, M.; Enomoto, T.; Melamed, A.; Wright, J.D.; Miyagi, E. The Effect of a Web-Based Cervical Cancer Survivor’s Story on Parents’ Behavior and Willingness to Consider Human Papillomavirus Vaccination for Daughters: Randomized Controlled Trial. JMIR Public Health Surveill. 2022, 8, e34715. [Google Scholar] [CrossRef]
- Hanley, S.J.; Yoshioka, E.; Ito, Y.; Konno, R.; Hayashi, Y.; Kishi, R.; Sakuragi, N. Acceptance of and attitudes towards human papillomavirus vaccination in Japanese mothers of adolescent girls. Vaccine 2012, 30, 5740–5747. [Google Scholar] [CrossRef]
- Shida, J.; Tsuchiya, Y.; Inoue, K.; Maeda, K.; Yamaki, M. Necessary Content of Information Concerning the HPV Vaccine as Assessed by Mothers of Girls. Sch. Health 2015, 11, 1–8. [Google Scholar]
- Hanley, S.J.; Yoshioka, E.; Ito, Y.; Konno, R.; Sasaki, Y.; Kishi, R.; Sakuragi, N. An exploratory study of Japanese fathers’ knowledge of and attitudes towards HPV and HPV vaccination: Does marital status matter? Asian Pac. J. Cancer Prev. 2014, 15, 1837–1843. [Google Scholar] [CrossRef]
- Nishigaki, S.; Wakimizu, R.; Kuroki, H.; Maehara, K.; Saitoh, T.; Fujioka, H.; Uduki, K. Qualitative study of Barriers and Facilitators for Mothers to Consider Immunization of Their Daughters against HPV. J. Ambul. Gen. Pediatr. 2014, 17, 10–17. [Google Scholar]
- Egawa-Takata, T.; Ueda, Y.; Morimoto, A.; Yoshino, K.; Kimura, T.; Nishikawa, N.; Sekine, M.; Horikoshi, Y.; Takagi, T.; Enomoto, T. Survey of Japanese mothers of daughters eligible for human papillomavirus vaccination on attitudes about media reports of adverse events and the suspension of governmental recommendation for vaccination. J. Obstet. Gynaecol. Res. 2015, 41, 1965–1971. [Google Scholar] [CrossRef]
- Nakajima, F. HPV vaccination for adolescent girls and their mothers’ attitudes toward the vaccination. Adolescentology 2015, 33, 259–266. [Google Scholar]
- Egawa-Takata, T.; Ueda, Y.; Tanaka, Y.; Morimoto, A.; Kubota, S.; Yagi, A.; Terai, Y.; Ohmichi, M.; Ichimura, T.; Sumi, T.; et al. Mothers’ attitudes in Japan regarding cervical cancer screening correlates with intention to recommend cervical cancer screening for daughters. Int. J. Clin. Oncol. 2016, 21, 962–968. [Google Scholar] [CrossRef]
- Yagi, A.; Ueda, Y.; Tanaka, Y.; Nakae, R.; Kakubari, R.; Morimoto, A.; Terai, Y.; Ohmichi, M.; Ichimura, T.; Sumi, T.; et al. Time-dependent changes of the intention of mothers in Japan to inoculate their daughters with the HPV vaccine after suspension of governmental recommendation. Hum. Vaccines Immunother. 2018, 14, 2497–2502. [Google Scholar] [CrossRef]
- Kobayashi, K.I.; Chanyasanha, C.; Sujirarat, D. Parental decision-making on human papillomavirus vaccination for daughters in Japan. Int. J. Adolesc. Med. Health 2020, 33, 95–105. [Google Scholar] [CrossRef]
- Ugumori, N.; Ueda, Y.; Yagi, A.; Abe, H.; Shiomi, M.; Nakagawa, S.; Hiramatsu, K.; Miyoshi, A.; Kobayashi, E.; Kimura, T.; et al. A potential means to help the HPV vaccine penetrate the Japanese public while under the continued suspension of governmental recommendation. Hum. Vaccines Immunother. 2021, 17, 3096–3101. [Google Scholar] [CrossRef]
- Imanishi, Y.; Kinoshita, T.; Sakamoto, M.; Ichimiya, M.; Mitsunami, M.; Takahashi, T.; Shigemi, D.; Song, M.; Inaba, K. Importance of human papillomavirus vaccination leaflets focusing on the safety profile targeted pediatricians in Japan. Vaccine 2022, 40, 5010–5015. [Google Scholar] [CrossRef]
- Yagi, A.; Ueda, Y.; Tomine, Y.; Ikeda, S.; Kakuda, M.; Nakagawa, S.; Hiramatsu, K.; Miyoshi, A.; Kobayashi, E.; Kimura, T.; et al. The ‘best friend effect’: A promising tool to encourage HPV vaccination in Japan. Int. J. Clin. Oncol. 2022, 27, 1750–1757. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.E. What are the factors that contribute to parental vaccine-hesitancy and what can we do about it? Hum. Vaccines Immunother. 2014, 10, 2584–2596. [Google Scholar] [CrossRef]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; deHart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.R.; Berenson, A.B. Sources of HPV vaccine hesitancy in parents. Hum. Vaccines Immunother. 2013, 9, 2649–2653. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.M.; Brown, C.J.; Gust, D.A. Vaccine beliefs of parents who oppose compulsory vaccination. Public Health Rep. 2005, 120, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Morino, S.; Tanaka-Taya, K.; Satoh, H.; Arai, S.; Takahashi, T.; Sunagawa, T.; Oishi, K. Descriptive epidemiology of varicella based on national surveillance data before and after the introduction of routine varicella vaccination with two doses in Japan, 2000–2017. Vaccine 2018, 36, 5977–5982. [Google Scholar] [CrossRef]
- Okuhara, T.; Ishikawa, H.; Okada, M.; Kato, M.; Kiuchi, T. Readability comparison of pro- and anti-HPV-vaccination online messages in Japan. Patient Educ. Couns. 2017, 100, 1859–1866. [Google Scholar] [CrossRef]
- Bigaard, J.; Franceschi, S. Vaccination against HPV: Boosting coverage and tackling misinformation. Mol. Oncol. 2021, 15, 770–778. [Google Scholar] [CrossRef]
- Corcoran, B.; Clarke, A.; Barrett, T. Rapid response to HPV vaccination crisis in Ireland. Lancet 2018, 391, 2103. [Google Scholar] [CrossRef]
- Keane, M.T.; Walter, M.V.; Patel, B.I.; Moorthy, S.; Stevens, R.B.; Bradley, K.M.; Buford, J.F.; Anderson, E.L.; Anderson, L.P.; Tibbals, K.; et al. Confidence in vaccination: A parent model. Vaccine 2005, 23, 2486–2493. [Google Scholar] [CrossRef]
- Zimet, G.D. Improving adolescent health: Focus on HPV vaccine acceptance. J. Adolesc. Health 2005, 37, S17–S23. [Google Scholar] [CrossRef]
- Okuhara, T.; Okada, H.; Goto, E.; Tsunezumi, A.; Kagawa, Y.; Kiuchi, T. Encouraging COVID-19 vaccination via an evolutionary theoretical approach: A randomized controlled study in Japan. Patient Educ. Couns. 2022, 105, 2248–2255. [Google Scholar] [CrossRef]
- Okuhara, T.; Okada, H.; Goto, E.; Kiuchi, T. Urgent need for writing education in schools of medicine and public health to address vaccine hesitancy. Int. J. Med. Educ. 2021, 12, 166–168. [Google Scholar] [CrossRef]
- Saitoh, A.; Saitoh, A.; Katsuta, T.; Mine, M.; Kamiya, H.; Miyairi, I.; Ishiwada, N.; Oshiro, M.; Kira, R.; Shimizu, N.; et al. Effect of a vaccine information statement (VIS) on immunization status and parental knowledge, attitudes, and beliefs regarding infant immunization in Japan. Vaccine 2020, 38, 8049–8054. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, K.; Osaka, W.; Togari, T.; Ishikawa, H.; Yonekura, Y.; Sekido, A.; Matsumoto, M. Comprehensive health literacy in Japan is lower than in Europe: A validated Japanese-language assessment of health literacy. BMC Public Health 2015, 15, 505. [Google Scholar] [CrossRef] [PubMed]
- Ueda, N.; Yokouchi, R.; Onoda, T.; Ogihara, A. Characteristics of Articles About Human Papillomavirus Vaccination in Japanese Newspapers: Time-Series Analysis Study. JMIR Public Health Surveill. 2017, 3, e97. [Google Scholar] [CrossRef] [PubMed]
- Daniel-Ulloa, J.; Gilbert, P.A.; Parker, E.A. Human Papillomavirus Vaccination in the United States: Uneven Uptake by Gender, Race/Ethnicity, and Sexual Orientation. Am. J. Public Health 2016, 106, 746–747. [Google Scholar] [CrossRef]


{kind=link}
| #1 vaccine | “vaccin” [Supplementary Concept] OR “vaccin” [All Fields] OR “vaccination” [MeSH Terms] OR “vaccination” [All Fields] OR “vaccinable” [All Fields] OR “vaccinal” [All Fields] OR “vaccinate” [All Fields] OR “vaccinated” [All Fields] OR “vaccinates” [All Fields] OR “vaccinating” [All Fields] OR “vaccinations” [All Fields] OR “vaccination’s” [All Fields] OR “vaccinator” [All Fields] OR “vaccinators” [All Fields] OR “vaccine’s” [All Fields] OR “vaccined” [All Fields] OR “vaccines” [MeSH Terms] OR “vaccines” [All Fields] OR “vaccine” [All Fields] OR “vaccins” [All Fields] |
| #2 parents | “parent’s” [All Fields] OR “parentally” [All Fields] OR “parentals” [All Fields] OR “parented” [All Fields] OR “parenting” [MeSH Terms] OR “parenting” [All Fields] OR “parents” [MeSH Terms] OR “parents” [All Fields] OR “parent” [All Fields] OR “parental” [All Fields] |
| #3 children | “child” [MeSH Terms] OR “child” [All Fields] OR “children” [All Fields] OR “child’s” [All Fields] OR “children’s” [All Fields] OR “childrens” [All Fields] OR “childs” [All Fields] |
| #4 Japan | “japan” [MeSH Terms] OR “japan” [All Fields] OR “japan’s” [All Fields] OR “japans” [All Fields] |
| #5 HPV | “HPV” [All Fields] |
| #6 human papilloma virus | “papillomaviridae” [MeSH Terms] OR “papillomaviridae” [All Fields] OR (“human” [All Fields] AND “papilloma” [All Fields] AND “virus” [All Fields]) OR “human papilloma virus” [All Fields] |
| #1 AND (#2 OR #3) AND #4 AND (#5 OR #6) | |
| Author, Year | Study Characteristics | Objective | Key Findings (Theme #) | |||
|---|---|---|---|---|---|---|
| Period | Design | Methodology | Sample | |||
| Hanley et al., 2012 [30] | 2010 | Cross-sectional | Paper questionnaire | 862 participants; all mothers who had a daughters | To determine acceptance of and preferences for the HPV vaccine, examine attitudes toward HPV and its vaccine, and identify sociodemographic and attitudinal predictors. |
|
| Shida et al., 2015 [31] | 2012 | Qualitative | Content analysis of free text writing in a questionnaire | 272 participants; parents/guardians who had a daughter | To explore what kind of information parents seek for their decision-making. |
|
| Hanley et al., 2014 [32] | 2010 | Cross-sectional | Paper questionnaire | 27 participants; all fathers who had a daughters | To investigate differences in vaccine acceptance in public funding programs and marital status. |
|
| Nishigaki et al., 2014 [33] | 2011–2012 | Qualitative | Interview | 20 participants; mother-daughter dyads | To examine vaccine uptake factors for mothers who have adolescent daughters. |
|
| Egawa-Takata et al., 2015 [34] | Not provided | Cross-sectional | Internet survey | 1000 participants; all mothers who had a daughter | To investigate the frequency of continuing/discontinuing HPV vaccination, how mothers influenced the decision, and mothers’ thoughts about a future HPV vaccination. |
|
| Nakajima et al., 2015 [35] | 2010–2011 | Cross-sectional | Paper questionnaire | 224 participants; all mothers who had a daughter | To identify awareness and decision-making factors. |
|
| Egawa-Takata et al., 2016 [36] | 2015 | Cross-sectional | Internet survey | 618 participants; all mothers who had a daughter | To examine the social factors for advising daughters about the HPV vaccine and cervical cancer screening. |
|
| Yagi et al., 2018 [37] | 2014, 2015, and 2016 | Cross-sectional | Internet survey in three phases | 200 (1st survey), 2060 (2nd survey), and 2000 (3rd survey) participants; all mothers who had a daughter | To examine the time-dependent relationship between the mothers’ willingness to vaccinate their daughters and government recommendations. |
|
| Shuto et al., 2021 [25] | 2019 | Cross-sectional | Internet survey | 1646 participants; all mothers who had a daughter | To understand HPV vaccine confidence and willingness among mothers with at least one daughter aged 12–16, female adolescents, and healthcare providers. |
|
| Kobayashi et al., 2020 [38] | 2017 | Cross-sectional | Paper questionnaire | 246 participants; parents/guardians who had a daughter | To analyze how government policy influenced parental HPV vaccine acceptance for their daughters and associated factors. |
|
| Miyoshi et al., 2020 [26] | 2017 | Interventional | Internet survey | 1648 participants; all fathers who had a daughter | To identify fathers’ role in a young girl’s vaccination decision-making and the effectiveness of an educational intervention to change their attitude towards the HPV vaccine. |
|
| Egawa-Tanaka et al., 2020 [27] | 2018 | RCT | Via Internet | 1499 participants; all mothers who had a daughter | To determine whether mothers’ willingness would change intervention by a letter recommending talking with their husbands about HPV vaccination and/or an educational leaflet.To identify the mothers’ decision-making process. |
|
| Suzuki et al., 2021 [28] | 2018 | RCT | Via Internet | 1660 participants; parents who had a daughter or son | To assess the effectiveness of a web-based educational intervention for parental decision-making. |
|
| Ugumori et al., 2021 [39] | 2020 | Cross-sectional and follow-up | Questionnaire | 59 participants; all mothers who had a daughter | To investigate the mothers’ attitudes before and after the doctor’s explanation about the information leaflet. |
|
| Imanishi et al., 2022 [40] | 2021 | Cross-sectional | Paper questionnaire | 161 participants; all mothers who had a daughter | To clarify the effectiveness of doctors’ explanation about vaccine safety by the leaflet. |
|
| Suzuki et al., 2022 [29] | 2020 | RCT | Via Internet | 2175 participants; parents who had a daughter | To investigate the effect of a cervical cancer survivor’s story on parents’ decision-making based on examining the rate of parents’ vaccine acceptance and vaccination rate at three months. |
|
| Yagi et al., 2022 [41] | 2021 | Cross-sectional | Internet survey | 1576 participants; all mothers who had a daughter | To examine the mothers’ willingness to vaccinate themselves and their daughters against HPV and their reasons. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lelliott, M.; Sahker, E.; Poudyal, H. A Review of Parental Vaccine Hesitancy for Human Papillomavirus in Japan. J. Clin. Med. 2023, 12, 2004. https://doi.org/10.3390/jcm12052004
Lelliott M, Sahker E, Poudyal H. A Review of Parental Vaccine Hesitancy for Human Papillomavirus in Japan. Journal of Clinical Medicine. 2023; 12(5):2004. https://doi.org/10.3390/jcm12052004
Chicago/Turabian StyleLelliott, Madoka, Ethan Sahker, and Hemant Poudyal. 2023. "A Review of Parental Vaccine Hesitancy for Human Papillomavirus in Japan" Journal of Clinical Medicine 12, no. 5: 2004. https://doi.org/10.3390/jcm12052004
APA StyleLelliott, M., Sahker, E., & Poudyal, H. (2023). A Review of Parental Vaccine Hesitancy for Human Papillomavirus in Japan. Journal of Clinical Medicine, 12(5), 2004. https://doi.org/10.3390/jcm12052004