
Non-Invasive Neuromodulation Methods to Alleviate Symptoms of Huntington’s Disease: A Systematic Review of the Literature

 ,
,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Study Selection
2.2. Data Collection and Data Items
2.3. Quality Assessment
3. Results
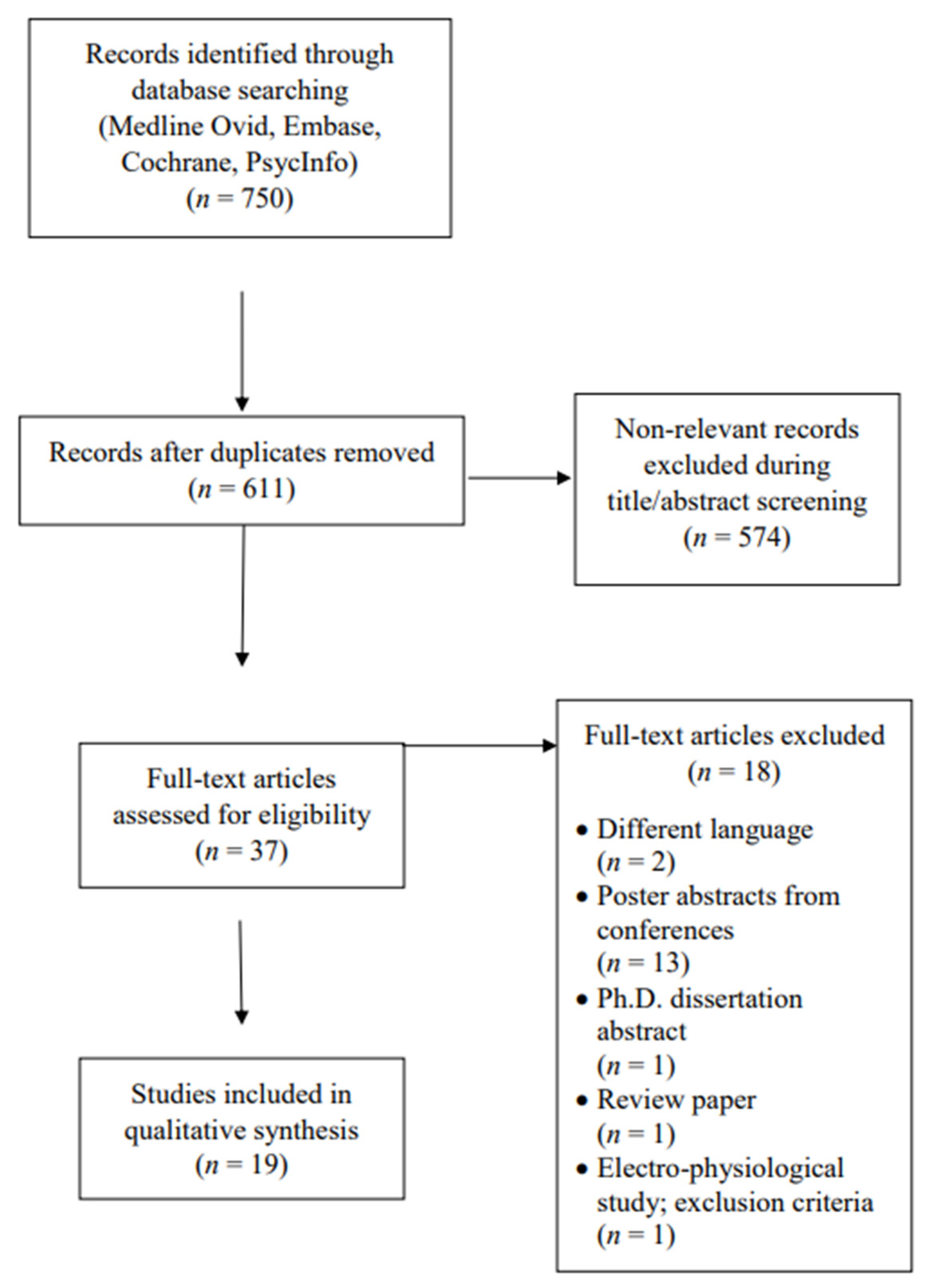
3.1. Study Selection
3.2. Study Characteristics
4. ECT
4.1. Study Design
4.2. Intervention Parameters
4.3. Assessment Tools and Outcomes
5. TMS
5.1. Study Design
5.2. Intervention Parameters
5.3. Assessment Tools and Outcomes
6. tDCS
6.1. Study Design
6.2. Intervention Parameters
6.3. Assessment Tools and Outcomes
7. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tabrizi, S.J.; Leavitt, B.R.; Landwehrmeyer, G.B.; Wild, E.J.; Saft, C.; Barker, R.A.; Blair, N.F.; Craufurd, D.; Priller, J.; Rickards, H.; et al. Targeting Huntingtin Expression in Patients with Huntington’s Disease. N. Engl. J. Med. 2019, 380, 2307–2316. [Google Scholar] [CrossRef]
- Bonelli, R.M.; Hofmann, P. A systematic review of the treatment studies in Huntington’s disease since 1990. Expert Opin. Pharmacother. 2007, 8, 141–153. [Google Scholar] [CrossRef]
- Podvin, S.; Reardon, H.T.; Yin, K.; Mosier, C.; Hook, V. Multiple clinical features of Huntington’s disease correlate with mutant HTT gene CAG repeat lengths and neurodegeneration. J. Neurol. 2019, 266, 551–564. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.A.; Tabrizi, S.J. Huntington’s disease: From molecular pathogenesis to clinical treatment. Lancet Neurol. 2011, 10, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Bashir, H.; Jankovic, J. Deutetrabenazine for the treatment of Huntington’s chorea. Expert Rev. Neurother. 2018, 18, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Dean, M.; Sung, V.W. Review of deutetrabenazine: A novel treatment for chorea associated with Huntington’s disease. Drug Des. Devel. Ther. 2018, 12, 313–319. [Google Scholar] [CrossRef]
- Schweitzer, I.; Maguire, K.; Ng, C. Sexual Side-Effects of Contemporary Antidepressants: Review. Aust. N. Z. J. Psychiatry 2009, 43, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, J.; Murgai, A.; Sharma, S.; Aur, D.; Jog, M. Non-invasive Transcranial Electrical Stimulation in Movement Disorders. Front. Neurosci. 2020, 14, 522. [Google Scholar] [CrossRef]
- Sanches, C.; Stengel, C.; Godard, J.; Mertz, J.; Teichmann, M.; Migliaccio, R.; Valero-Cabré, A. Past, Present, and Future of Non-invasive Brain Stimulation Approaches to Treat Cognitive Impairment in Neurodegenerative Diseases: Time for a Comprehensive Critical Review. Front. Aging Neurosci. 2020, 12, 578339. [Google Scholar] [CrossRef]
- Vonsattel, J.P.; Myers, R.H.; Stevens, T.J.; Ferrante, R.J.; Bird, E.D.; Richardson, E.P., Jr. Neuropathological classification of Huntington’s disease. J. Neuropathol. Exp. Neurol. 1985, 44, 559–577. [Google Scholar] [CrossRef]
- Ross, C.A.; Aylward, E.H.; Wild, E.J.; Langbehn, D.R.; Long, J.D.; Warner, J.H.; Scahill, R.I.; Leavitt, B.R.; Stout, J.C.; Paulsen, J.S.; et al. Huntington disease: Natural history, biomarkers and prospects for therapeutics. Nat. Rev. Neurol. 2014, 10, 204–216. [Google Scholar] [CrossRef] [PubMed]
- Pini, L.; Jacquemot, C.; Cagnin, A.; Meneghello, F.; Semenza, C.; Mantini, D.; Vallesi, A. Aberrant brain network connectivity in presymptomatic and manifest Huntington’s disease: A systematic review. Hum. Brain Mapp. 2020, 41, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Leaver, A.M.; Espinoza, R.; Wade, B.; Narr, K.L. Parsing the Network Mechanisms of Electroconvulsive Therapy. Biol. Psychiatry 2022, 92, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Chase, H.W.; Boudewyn, M.A.; Carter, C.S.; Phillips, M.L. Transcranial direct current stimulation: A roadmap for research, from mechanism of action to clinical implementation. Mol. Psychiatry 2020, 25, 397–407. [Google Scholar] [CrossRef]
- Guerra, A.; Rocchi, L.; Grego, A.; Berardi, F.; Luisi, C.; Ferreri, F. Contribution of TMS and TMS-EEG to the Understanding of Mechanisms Underlying Physiological Brain Aging. Brain Sci. 2021, 11, 405. [Google Scholar] [CrossRef]
- Institute, J.B. Critical appraisal checklist for analytical cross sectional studies. Crit. Apprais. Tools 2021, 11, 405. [Google Scholar]
- Evans, D.L.; Pedersen, C.A.; Tancer, M.E. ECT in the Treatment of Organic Psychosis in Huntington’s Disease. Convuls. Ther. 1987, 3, 145–150. [Google Scholar]
- Ranen, N.G.; Peyser, C.E.; Folstein, S.E. ECT as a treatment for depression in Huntington’s disease. J. Neuropsychiatry Clin. Neurosci. 1994, 6, 154–159. [Google Scholar] [CrossRef]
- Lewis, C.F.; DeQuardo, J.R.; Tandon, R. ECT in genetically confirmed Huntington’s disease. J. Neuropsychiatry Clin. Neurosci. 1996, 8, 209–210. [Google Scholar] [CrossRef]
- Beale, M.D.; Kellner, C.H.; Gurecki, P.; Pritchett, J.T. ECT for the treatment of Huntington’s disease: A case study. Convuls. Ther. 1997, 13, 108–112. [Google Scholar]
- Merida-Puga, J.; Ramirez-Bermudez, J.; Aguilar-Venegas, L.C.; Fricchione, G.L.; Espinola-Nadurille, M. Westphal variant Huntington disease and refractory catatonia: A case report. Cogn. Behav. Neurol. 2011, 24, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Ono, S.; Yamaguchi, J.; Sugimoto, R.; Yamaguchi, N.; Morimoto, Y.; Kubo, T.; Ozawa, H.; Kurotaki, N. Modified electroconvulsive therapy for the treatment of refractory schizophrenia-like psychosis associated with Huntington’s disease. J. Neurol. 2013, 260, 312–314. [Google Scholar] [CrossRef] [PubMed]
- Cusin, C.; Franco, F.B.; Fernandez-Robles, C.; DuBois, C.M.; Welch, C.A. Rapid improvement of depression and psychotic symptoms in Huntington’s disease: A retrospective chart review of seven patients treated with electroconvulsive therapy. Gen. Hosp. Psychiatry 2013, 35, e673–e675. [Google Scholar] [CrossRef] [PubMed]
- Magid, M.; Trevino, K.; Reid, W.H.; Jalalat, S.; Husain, M.M.; Kahn, D.A. Emergency ECT in an incapacitated, medically compromised patient with Huntington’s disease. J. Psychiatr. Pract. 2014, 20, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Petit, A.C.; Hozer, F.; Youssov, K.; Lavaud, P.; Hardy, P.; Mouaffak, F. Differential Response to ECT of Psychotic and Affective Symptoms in Huntington’s Disease: A Case Report. J. Neuropsychiatry Clin. Neurosci. 2016, 28, e3–e5. [Google Scholar] [CrossRef]
- Shah, R.P.; Alluri, V.; Sharma, S. Treatment of Agitation in Huntington’s Disease with Electroconvulsive Therapy. J. Neuropsychiatry Clin. Neurosci. 2017, 29, 293–294. [Google Scholar] [CrossRef]
- Adrissi, J.; Nadkarni, N.A.; Gausche, E.; Bega, D. Electroconvulsive Therapy (ECT) for Refractory Psychiatric Symptoms in Huntington’s Disease: A Case Series and Review of the Literature. J. Huntingt. Dis. 2019, 8, 291–300. [Google Scholar] [CrossRef]
- Abeysundera, H.; Campbell, A.; Sarma, S. Worsening of movement disorder following treatment with electroconvulsive therapy in a patient with Huntington’s disease. BMJ Case Rep. 2019, 12, e230389. [Google Scholar] [CrossRef]
- Mowafi, W.; Millard, J. Electroconvulsive therapy for severe depression, psychosis and chorea in a patient with Huntington’s disease: Case report and review of the literature. BJPsych Bull. 2021, 45, 97–104. [Google Scholar] [CrossRef]
- Brusa, L.; Versace, V.; Koch, G.; Bernardi, G.; Iani, C.; Stanzione, P.; Centonze, D. Improvement of choreic movements by 1 Hz repetitive transcranial magnetic stimulation in Huntington’s disease patients. Ann. Neurol. 2005, 58, 655–656. [Google Scholar] [CrossRef]
- Groiss, S.; Netz, J.; Lange, H.; Buetefisch, C. Frequency dependent effects of rTMS on motor and cognitive functions in Huntington’s disease. Basal Ganglia 2012, 2, 41–48. [Google Scholar] [CrossRef]
- Shukla, A.; Jayarajan, R.N.; Muralidharan, K.; Jain, S. Repetitive transcranial magnetic stimulation not beneficial in severe choreiform movements of Huntington disease. J. ECT 2013, 29, e16–e17. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.; Phillips, A.; Tendler, A.; Oberdeck, A. Deep rTMS for Neuropsychiatric Symptoms of Huntington’s Disease: Case Report. Brain Stimul. 2016, 9, 960–961. [Google Scholar] [CrossRef] [PubMed]
- Eddy, C.M.; Shapiro, K.; Clouter, A.; Hansen, P.C.; Rickards, H.E. Transcranial direct current stimulation can enhance working memory in Huntington’s disease. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2017, 77, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Bocci, T.; Baloscio, D.; Ferrucci, R.; Sartucci, F.; Priori, A. Cerebellar Direct Current Stimulation (ctDCS) in the Treatment of Huntington’s Disease: A Pilot Study and a Short Review of the Literature. Front. Neurol. 2020, 11, 614717. [Google Scholar] [CrossRef] [PubMed]
- Gazdag, G.; Ungvari, G.S. Electroconvulsive therapy: 80 years old and still going strong. World J. Psychiatry 2019, 9, 1–6. [Google Scholar] [CrossRef]
- Rojas, M.; Ariza, D.; Ortega, A.; Riano-Garzon, M.E.; Chavez-Castillo, M.; Perez, J.L.; Cudris-Torres, L.; Bautista, M.J.; Medina-Ortiz, O.; Rojas-Quintero, J.; et al. Electroconvulsive Therapy in Psychiatric Disorders: A Narrative Review Exploring Neuroendocrine-Immune Therapeutic Mechanisms and Clinical Implications. Int. J. Mol. Sci. 2022, 23, 6918. [Google Scholar] [CrossRef]
- Bioque, M.; Mac-Dowell, K.S.; Meseguer, A.; Macau, E.; Valero, R.; Vieta, E.; Leza, J.C.; Bernardo, M. Effects of electroconvulsive therapy in the systemic inflammatory balance of patients with severe mental disorder. Psychiatry Clin. Neurosci. 2019, 73, 628–635. [Google Scholar] [CrossRef]
- Trevino, K.; McClintock, S.M.; Husain, M.M. A review of continuation electroconvulsive therapy: Application, safety, and efficacy. J. ECT 2010, 26, 186–195. [Google Scholar] [CrossRef]
- Reti, I. Brain Stimulation: Methodologies and Interventions; John Wiley & Sons, Incorporated: Somerset, MD, USA, 2015. [Google Scholar]
- Kim, A.; Lalonde, K.; Truesdell, A.; Welter, P.G.; Brocardo, P.S.; Rosenstock, T.R.; Gil-Mohapel, J. New Avenues for the Treatment of Huntington’s Disease. Int. J. Mol. Sci. 2021, 22, 8363. [Google Scholar] [CrossRef]
- Wolf, R.C.; Sambataro, F.; Vasic, N.; Depping, M.S.; Thomann, P.A.; Landwehrmeyer, G.B.; Sussmuth, S.D.; Orth, M. Abnormal resting-state connectivity of motor and cognitive networks in early manifest Huntington’s disease. Psychol. Med. 2014, 44, 3341–3356. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.J.; Dogan, I.; Sass, C.; Mirzazade, S.; Schiefer, J.; Shah, N.J.; Schulz, J.B.; Reetz, K. Altered resting-state connectivity in Huntington’s disease. Hum. Brain Mapp. 2014, 35, 2582–2593. [Google Scholar] [CrossRef] [PubMed]
- Yoldi-Negrete, M.; Gill, L.N.; Olivares, S.; Lauziere, A.; Desilets, M.; Tourjman, S.V. The effect of continuation and maintenance electroconvulsive therapy on cognition: A systematic review of the literature and meta-analysis. J. Affect. Disord. 2022, 316, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Dybedal, G.S.; Tanum, L.; Sundet, K.; Gaarden, T.L.; Bjolseth, T.M. Cognitive side-effects of electroconvulsive therapy in elderly depressed patients. Clin. Neuropsychol. 2014, 28, 1071–1090. [Google Scholar] [CrossRef]
- Verwijk, E.; Comijs, H.C.; Kok, R.M.; Spaans, H.P.; Tielkes, C.E.; Scherder, E.J.; Stek, M.L. Short- and long-term neurocognitive functioning after electroconvulsive therapy in depressed elderly: A prospective naturalistic study. Int. Psychogeriatr. 2014, 26, 315–324. [Google Scholar] [CrossRef]
- Hausner, L.; Damian, M.; Sartorius, A.; Frolich, L. Efficacy and cognitive side effects of electroconvulsive therapy (ECT) in depressed elderly inpatients with coexisting mild cognitive impairment or dementia. J. Clin. Psychiatry 2011, 72, 91–97. [Google Scholar] [CrossRef]
- Ustohal, L. Introductory Chapter: Introduction to Transcranial Magnetic Stimulation in Neuropsychiatry, 12th ed.; IntechOpen Limited: London, UK, 2018. [Google Scholar]
- George, M.S.; Post, R.M. Daily Left Prefrontal Repetitive Transcranial Magnetic Stimulation for Acute Treatment of Medication-Resistant Depression. Am. J. Psychiatry 2011, 168, 356–364. [Google Scholar] [CrossRef]
- Schwedt, T.J.; Vargas, B. Neurostimulation for Treatment of Migraine and Cluster Headache. Pain Med. 2015, 16, 1827–1834. [Google Scholar] [CrossRef]
- Antonelli, P.J.; Martinez, S.A.; Kleinjung, T.; Eichhammer, P.; Landgrebe, M.; Sand, P.; Hajak, G.; Strutz, J.; Langguth, B. 08:18: Combined Temporal and Prefrontal TMS for Tinnitus Treatment. Otolaryngol. Head Neck Surg. 2007, 137, P119–P120. [Google Scholar] [CrossRef]
- Carmi, L.; Al Yagon, U.; Dar, R.; Zohar, J.; Zangen, A. Deep Transcranial Magnetic Stimulation (Tms) in Obsessive Compulsive Disorder (Ocd) Patients. Eur. Psychiatry 2015, 30, 794. [Google Scholar] [CrossRef]
- Zangen, A. Resting-state and stimulation train induced EEG activity predict alleviation of ADHD symptoms following deep TMS treatment. Brain Stimul. 2019, 12, 553. [Google Scholar] [CrossRef]
- Pripfl, J.; Tomova, L.; Riecansky, I.; Lamm, C. Transcranial Magnetic Stimulation of the Left Dorsolateral Prefrontal Cortex Decreases Cue-induced Nicotine Craving and EEG Delta Power. Brain Stimul. 2014, 7, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Leone, A.; Bartres-Faz, D.; Keenan, J.P. Transcranial magnetic stimulation: Studying the brain-behaviour relationship by induction of ‘virtual lesions. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1999, 354, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Herwig, U.; Abler, B.; Schonfeldt-Lecuona, C.; Wunderlich, A.; Grothe, J.; Spitzer, M.; Walter, H. Verbal storage in a premotor-parietal network: Evidence from fMRI-guided magnetic stimulation. Neuroimage 2003, 20, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Herwig, U.; Satrapi, P.; Schonfeldt-Lecuona, C. Using the international 10-20 EEG system for positioning of transcranial magnetic stimulation. Brain Topogr. 2003, 16, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Herbsman, T.; Avery, D.; Ramsey, D.; Holtzheimer, P.; Wadjik, C.; Hardaway, F.; Haynor, D.; George, M.S.; Nahas, Z. More lateral and anterior prefrontal coil location is associated with better repetitive transcranial magnetic stimulation antidepressant response. Biol. Psychiatry 2009, 66, 509–515. [Google Scholar] [CrossRef]
- Bersani, F.S.; Minichino, A.; Enticott, P.G.; Mazzarini, L.; Khan, N.; Antonacci, G.; Raccah, R.N.; Salviati, M.; Chiaie, R.D.; Bersani, G.; et al. Deep transcranial magnetic stimulation as a treatment for psychiatric disorders: A comprehensive review. Eur. Psychiatry 2013, 28, 30–39. [Google Scholar] [CrossRef]
- Stultz, D.J.; Osburn, S.; Burns, T.; Pawlowska-Wajswol, S.; Walton, R. Transcranial Magnetic Stimulation (TMS) Safety with Respect to Seizures: A Literature Review. Neuropsychiatr. Dis. Treat. 2020, 16, 2989–3000. [Google Scholar] [CrossRef]
- Slotema, C.W.; Blom, J.D.; Hoek, H.W.; Sommer, I.E. Should we expand the toolbox of psychiatric treatment methods to include Repetitive Transcranial Magnetic Stimulation (rTMS)? A meta-analysis of the efficacy of rTMS in psychiatric disorders. J. Clin. Psychiatry 2010, 71, 873–884. [Google Scholar] [CrossRef]
- Jannati, A.; Oberman, L.M.; Rotenberg, A.; Pascual-Leone, A. Assessing the mechanisms of brain plasticity by transcranial magnetic stimulation. Neuropsychopharmacology 2023, 48, 191–208. [Google Scholar] [CrossRef]
- Voigt, J.; Carpenter, L.; Leuchter, A. Cost effectiveness analysis comparing repetitive transcranial magnetic stimulation to antidepressant medications after a first treatment failure for major depressive disorder in newly diagnosed patients—A lifetime analysis. PLoS ONE 2017, 12, e0186950. [Google Scholar] [CrossRef] [PubMed]
- Zaghi, S.; Heine, N.; Fregni, F. Brain stimulation for the treatment of pain: A review of costs, clinical effects, and mechanisms of treatment for three different central neuromodulatory approaches. J. Pain Manag. 2009, 2, 339–352. [Google Scholar] [PubMed]
- Woods, A.J.; Antal, A.; Bikson, M.; Boggio, P.S.; Brunoni, A.R.; Celnik, P.; Cohen, L.G.; Fregni, F.; Herrmann, C.S.; Kappenman, E.S.; et al. A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin. Neurophysiol. 2016, 127, 1031–1048. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.-F.; Polanía, R.; Nitsche, M. Physiology of Transcranial Direct and Alternating Current Stimulation. In Transcranial Direct Current Stimulation in Neuropsychiatric Disorders: Clinical Principles and Management; Brunoni, A., Nitsche, M., Loo, C., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 29–46. [Google Scholar]
- Wörsching, J.; Padberg, F.; Ertl-Wagner, B.; Kumpf, U.; Kirsch, B.; Keeser, D. Imaging transcranial direct current stimulation (tDCS) of the prefrontal cortex—Correlation or causality in stimulation-mediated effects? Neurosci. Biobehav. Rev. 2016, 69, 333–356. [Google Scholar] [CrossRef] [PubMed]
- Loo, C.K.; Alonzo, A.; Fong, J. Principles in Use of home-based tDCS in Depression. Brain Stimul. 2017, 10, 397. [Google Scholar] [CrossRef]
- Matsumoto, H.; Ugawa, Y. Adverse events of tDCS and tACS: A review. Clin. Neurophysiol. Pract. 2017, 2, 19–25. [Google Scholar] [CrossRef]
- De Souza, C.G.; Pegado, R.; Costa, J.; Morya, E.; Baptista, A.F.; Unal, G.; Bikson, M.; Okano, A.H. Alternate sessions of transcranial direct current stimulation (tDCS) reduce chronic pain in women affected by chikungunya. A randomized clinical trial. Brain Stimul. 2021, 14, 541–548. [Google Scholar] [CrossRef]
- Katz, B.; Au, J.; Buschkuehl, M.; Abagis, T.; Zabel, C.; Jaeggi, S.M.; Jonides, J. Individual Differences and Long-term Consequences of tDCS-augmented Cognitive Training. J. Cogn. Neurosci. 2017, 29, 1498–1508. [Google Scholar] [CrossRef]
- Garcia, S.; Hampstead, B.M. HD-tDCS as a neurorehabilitation technique for a case of post-anoxic leukoencephalopathy. Neuropsychol. Rehabil. 2020, 32, 946–966. [Google Scholar] [CrossRef]
- Franklin, G.L.; Camargo, C.H.F.; Meira, A.T.; Lima, N.S.C.; Teive, H.A.G. The Role of the Cerebellum in Huntington’s Disease: A Systematic Review. Cerebellum 2021, 20, 254–265. [Google Scholar] [CrossRef]
- Hordacre, B.; Moezzi, B.; Ridding, M.C. Neuroplasticity and network connectivity of the motor cortex following stroke: A transcranial direct current stimulation study. Hum. Brain Mapp. 2018, 39, 3326–3339. [Google Scholar] [CrossRef] [PubMed]
- Indahlastari, A.; Albizu, A.; Kraft, J.N.; O’Shea, A.; Nissim, N.R.; Dunn, A.L.; Carballo, D.; Gordon, M.P.; Taank, S.; Kahn, A.T.; et al. Individualized tDCS modeling predicts functional connectivity changes within the working memory network in older adults. Brain Stimul. 2021, 14, 1205–1215. [Google Scholar] [CrossRef] [PubMed]
- Begemann, M.J.; Brand, B.A.; Curcic-Blake, B.; Aleman, A.; Sommer, I.E. Efficacy of non-invasive brain stimulation on cognitive functioning in brain disorders: A meta-analysis. Psychol. Med. 2020, 50, 2465–2486. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Date | Study Type | Sample | Intervention | Tools | Outcome | Side Effects |
|---|---|---|---|---|---|---|
| Evans et al. (1987) [17] | Case—Report | 1 (F, 49 years old) CAG repeat: NA TFC: NA | Intervention: ECT, parameters not specified. Electrode position: RUL. Number of sessions: 6 sessions. Seizure length: 239 s by EEG recordings. | Physician examination and observations (symptoms: cognitive functional, and behavioral) |
| Mild increase in choreiform movements during the course of treatment. |
| Ranen et al. (1994) [18] | Case—Series | 6 (2F, 4M, aged between 41 and 62 years) CAG Repeat: NA TFC: NA | Intervention: ECT, initial parameters with 70 Hz, pulse width of 1.0 ms, and duration of 2.0 ms. Parameters were increased as necessary to achieve adequate seizure duration. Electrode position: Initial treatment with RUL for all patients. BL placement was used when necessary to achieve adequate seizure duration. Only RUL was used in Cases 1 and 2; Case 4 used RUL and BL in different sessions; Cases 3, 5 and 6 were not specified. Number of sessions: 7 (Case 1), 7 (Case 2), 8 (Case 3 and Case 6), 5 (Case 4), and 9 (Case 5). Seizure length: Raged from 5 to 120 s. | Physician observations (symptoms: alteration in movements, behavior, psychiatric, and cognitive functions) Mini-Mental State Exam (MMSE) |
| One patient developed psychosis and cognitive impairment (Case 3), and one patient had worsened catatonia with agitation (Case 4). |
| Lewis et al. (1996) [19] | Case—Report | 1 (M, 65 years old) CAG Repeat: 44 TFC stage: Il/V | Intervention: ECT, 90 Hz, brief pulse 1.0–1.6 ms, dynamic energy 33.3–55.7 joules. Electrode position: Frontotemporal (BL). Number of sessions: 8 sessions. Electrode position: frontotemporal (bilateral) Seizure length: Range between 24 and 140 s. | Hamilton Depression Rating Scale (Ham-D) and MMSE |
| NA |
| Beale et al. (1997) [20] | Case—Report | 1 (M, 56 years old) CAG Repeat: 46 TFC: NA | Intervention: First ECT session: stimulation dose started at 12.7 joules (72 mC), which did not cause seizure, and the dose was increased to 40.1 joules (229 mC). Second ECT session: stimulation dose was at 40.8 joules (233 mC). Stimulus dose was increased by 10–20 joules for each subsequent session. Electrode position: BL Number of sessions: 11 ECT, given 3 times per week. Maintenance ECT given once every 3 months. Seizure length (average): 34.3 s (motor) and 39.1 s (EEG). Range: 19–57 s. | Self-reported and clinical examination |
| NA |
| Merida-Puga et al. (2011) [21] | Case—Report | 1 (F, 26 years old) CAG Repeat: 45 TFC: NA | Intervention: ECT, stimulus was calculated using the half-life method and increased by up to 25%. Electrode position: NA Number of sessions: 42 sessions of ECT, (13 in the first, 15 in the second, and 14 in the third cycle of intervention). Seizure length: 42 to 80 s. | Self-reported Bush-Francis Catatonia Rating Scale (BFCRS) |
| NA |
| Nakano et al. (2013) [22] | Case—Report | 1 (M, 59 years old) CAG Repeat: 44 TFC: NA | Intervention: modified ECT, stimulation parameters not specified. Electrode position: NA Number of sessions: 21 sessions of modified ECT over a period of 6 months’ time. Seizure length: NA | MMSE scores, positive and negative symptom scale (PANSS), and brief psychiatric rating scale (BPRS) |
| Transient cardiovascular problem and anterograde/retrograde amnesia |
| Cusin et al. (2013) [23] | Case—Series | 7 (4F, 3M, age range from 20 to 56) CAG Repeat: NA TFC: NA | Intervention: ECT, pulse width of 1 msec, frequency of 90 Hz, and duration of 2–4 s. Electrode position: RUL. Number of sessions: 4 to 13 sessions to treat the acute series. One patient had further ECT to treat depressive recurrence several months later, and two patients required maintenance ECT at regular intervals to maintain the recovery. Seizure length: NA | Self-reported and clinical examination (symptoms: motor and behavioral symptoms) |
| Two patients developed short-term agitation upon recovery from anesthesia. |
| Magid et al. (2014) [24] | Case—Report | 1 (F, 57 years old) CAG Repeat: 43 TFC: NA | Intervention: ECT, brief-pulse stimulus with age-based stimulus dosing. Electrode position: BL (bi-temporal). Number of sessions: 4 sessions before hospital discharge. Maintenance ECT once every 1 to 4 weeks for 6 months. Seizure length: NA | Self-reported and clinician observation (symptoms: visual hallucinations, agitation, frequent verbal outbursts, weight loss, impaired judgement, disorientation, and the patient had become non-communicative). |
| NA |
| Petit et al. (2016) [25] | Case—Report | 1 (M, 60 years old) CAG Repeat: 41 TFC score: 2 | Intervention: ECT, stimulation parameters not specified. Electrode position: NA Number of sessions: 18 sessions. Seizure length: NA | Expanded version of the Brief Psychiatric Rating Scale (BPRS-E); Clinical Global Impression (CGI); Montgomery-Åsberg Depression Rating Scale (MADRS); Unified Huntington’s Disease Rating Scale (UHDRS); MMSE | After 12 ECT sessions:
| NA |
| Shah et al. (2017) [26] | Case—Report | 1 (F, 51 years old) CAG Repeat: NA TFC: NA | Intervention: ECT, stimulation parameters not specified. Electrode position: BL (bitemporal). Number of sessions: 5 sessions. Seizure length: NA | Self-reported and clinical examination |
| NA |
| Adrissi et al. (2019) [27] | Case—Series | 4 (1F, 3M age range from 38 to 52) CAG Repeat: 44 (case 1), 42 (case 2), 46 (case 3) and 39 (case 4) TFC: NA | Intervention: ECT, Case 1: 0.50 ms pulse width, 40% charge dose. Case 2: 0.25 ms pulse width, 10–70 Hz frequency, 5–25% charge. Case 3: 0.25–1.0 ms pulse width, 40–140 Hz frequency, 100% charge dose (except for two sessions with 50%). Case 4: 0.25 ms pulse width, 40 Hz frequency (except initial session 10 Hz), 25–50% charge dose (except for first session with 5%). Electrode position—BL (bitemporal) (Cases 1 and 3) and RUL (Cases 2 and 4). Number of sessions: 29 (Case 1), 27 (Case 2), 41 (Case 3), 7 (Case 4). Seizure length—ranged from 21 to 84 s. | Symptoms: Psychiatric—suicidal ideation, anxiety, depression, agitation evaluated using clinical examination, motor—evaluated using UHDRS—case 1 and 2 and cognition evaluated using Montreal Cognitive Assessment (MoCA)—case 2 |
| One patient developed irritability and delirium after ECT |
| Abeysundera et al. (2019) [28] | Case—Report | 1 (F, 56 years old) CAG Repeat: NA TFC: NA | Intervention: ECT, stimulation parameter not specified. Electrode position: RUL. Number of sessions: 10 sessions. Seizure length: NA | MADRS; MoCA; Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES Q-SF); UHDRS. |
| After fifth session of ECT, there was worsening of her involuntary movements along with increasing difficulty with walking. After 10 ECT sessions, the patient experienced worsening balance and involuntary movements. |
| Mowafi et al. (2021) [29] | Case—Report | 1 (F, 57 years old) CAG Repeat: 46 TFC: NA | Intervention: ECT, current intensity: First 12 sessions used between 75 and 150 mC; last 12 sessions used between 150 and 225 mC. Maintenance ECT used between 150 and 300 mC. Electrode position: BL. Number of sessions: 24 ECT sessions and later maintenance ECT once every week and later fortnightly (total number of sessions is not described). Seizure length: from 30 to 60 s. | Self-reported and clinical examination |
| NA |
| Author, Date | Study Type | Sample | Intervention | Tools | Outcome | Side Effects |
|---|---|---|---|---|---|---|
| Brusa et al. (2005) [30] | Clinical trial | 4 (sex and age NA) CAG Repeat: NA TFC stage: II to IV | Intervention (crossover design): Sham rTMS—consisted of 900 pulses delivered at 1 Hz, intensity was set at 90% of the resting motor threshold (RMT), and the coil was angled away so that no current was induced in the brain. 1 Hz rTMS—consisted of 900 pulses delivered at 1 Hz, intensity was set at 90% of the resting motor threshold. 5 Hz rTMS—consisted of 18 trains of 50 stimuli at 5 Hz frequency separated by 40 s of pause, delivered at 110% resting motor threshold for a total of 900 pulses. Frequency—one-time stimulation. Coil type/position—Figure-of-eight coil/supplementary motor area (SMA) of both hemispheres (3 cm anterior to Cz in the sagittal midline). Interval period—The patients received each of the stimulation in three consecutive days (one day for each stimulation i.e., sham, 1 Hz and 5 Hz) | Abnormal Involuntary movement scale (AIMs), UHDRS—chorea and bradykinesia items of the motor section. | 1 Hz rTMS
| One patient’s bradykinesia transiently worsened immediately after receiving 1 Hz rTMS stimulation. |
| Groiss et al. (2012) [31] | Clinical trial | 8 (4F and 4M, age range from 32 to 63) CAG Repeat: ranges from 39 to 51. TFC: NA | Intervention (crossover design): Sham rTMS—consisted of 10 trains of 5 Hz rTMS with duration of 4 s and intertrain interval of 60 s and a total number of 200 stimuli were applied during one session. 1 Hz rTMS—consisted of a train of 200 stimuli applied at 1 Hz, total number of 200 stimuli were applied during each session. 10 Hz rTMS—consisted of 10 trains of 10 Hz rTMS with duration of 2 s and intertrain interval of 60 s and 200 stimuli were applied during each session. Coil type/position: Figure-of-eight coil/The coil was positioned on the scalp over the left primary motor cortex (M1). Frequency: one-time stimulation Interval period—three sessions separated by at least two weeks. | UHDRS; Nine Hole Peg Test (NHPT); Reaction times (RT), including simple (sRT) and choice (cRT)); Digit span test (DST); Beck Depression Inventory (BDI); HD-activity of daily living (HD-ADL). | 1 Hz rTMS
| NA |
| Shukla et al. (2013) [32] | Case-Series | 2 (sex and age NA) CAG Repeat: NA TFC score: 1 (case 1), 2 (case 2). | Intervention: rTMS, 900 pulses at 1 Hz frequency and intensity was set at 90% of the motor threshold Coil type/position: Figure-of-eight coil/supplementary motor area of both cerebral hemispheres, which is approximately three cm anterior to the Cz in the sagittal midline. Frequency: Seven sessions on a once-daily basis Interval period: 1 day apart (7 consecutive sessions in total). | AIMs Total Functional Capacity (TFC) |
| NA |
| Davis et al. (2016) [33] | Case-Report | 1 (M, 77 years old with late onset HD, TRD and GAD) CAG Repeat: NA TFC: NA | Intervention: dTMS, 1600 pulses at 1 Hz frequency at 120% of the motor threshold. Coil type/position: H coil/right dorsolateral prefrontal cortex. Frequency: 49 days (once per day). | The Geriatric Depression Scale (GDS) |
| Lacrimation in the right eye, as well as scalp discomfort at the treatment site. |
| Author, Date | Study Design | Sample | Intervention | Outcome Measures | Outcome | Side Effects |
|---|---|---|---|---|---|---|
| Eddy et al. (2017) [34] | Clinical Trial | 20 (Sex: NA; age range between 50 and 72) CAG Repeat: NA TFC: NA | Intervention: Anodal tDCS—1.5 mA tDCS was sustained for 15 min, followed by a 60- second ramp down. Sham—after the 60 s ramp up, stimulation was programmed to ramp down again. Electrode position: The anode was placed over F3 to stimulate left DLPFC and the cathode was placed over the contralateral orbital area (FP2). Duration: 17 min/session. Frequency: 1 day for anodal tDCS and 1 day for sham. Washout period: One week. | Outcome measures (pre and post-tests): Digit ordering test-adapted (DOT-A), Stroop test, 1-back and 2-back tests (N-back tasks); | Primary: Working Memory (WM). DOT-A
Tolerability
| Tingling (anodal tDCS n = 6; sham n = 6), itching (anodal tDCS n = 5; sham n = 3), feelings of increased/decreased alertness and concentration (anodal tDCS n = 5; sham n = 5). |
| Bocci et al. (2020) [35] | Clinical Trial | 4 (2M, 2F, aged between 43 and 50 year) CAG Repeat: ≥40 UHDRS motor score: >5 TFC score: >7 | Interventions:Anodal tDCS—2.0 mA tDCS was sustained for 20 min, followed by a decrease in current in a ramp-like manner; current intensity: ∼0.08 mA/cm2. Sham—the current was turned on for 5 s and then turned off in a ramp-shaped fashion, thus inducing skin sensations similar to those produced by real tDCS. Electrode position—The anode was applied on the median line, 2 cm below the inion, with lateral borders about 1 cm medially to the mastoid apophysis, and the cathode over the right shoulder. Duration 20 min per session for 5 consecutive days (3 months interval between interventions). | Tools: UHDRS-part I. Time points: Baseline (T0), end of the stimulation week (T1), and 4 weeks later (T2). |
| NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jose, L.; Martins, L.B.; Cordeiro, T.M.; Lee, K.; Diaz, A.P.; Ahn, H.; Teixeira, A.L. Non-Invasive Neuromodulation Methods to Alleviate Symptoms of Huntington’s Disease: A Systematic Review of the Literature. J. Clin. Med. 2023, 12, 2002. https://doi.org/10.3390/jcm12052002
Jose L, Martins LB, Cordeiro TM, Lee K, Diaz AP, Ahn H, Teixeira AL. Non-Invasive Neuromodulation Methods to Alleviate Symptoms of Huntington’s Disease: A Systematic Review of the Literature. Journal of Clinical Medicine. 2023; 12(5):2002. https://doi.org/10.3390/jcm12052002
Chicago/Turabian StyleJose, Lijin, Lais Bhering Martins, Thiago M. Cordeiro, Keya Lee, Alexandre Paim Diaz, Hyochol Ahn, and Antonio L. Teixeira. 2023. "Non-Invasive Neuromodulation Methods to Alleviate Symptoms of Huntington’s Disease: A Systematic Review of the Literature" Journal of Clinical Medicine 12, no. 5: 2002. https://doi.org/10.3390/jcm12052002
APA StyleJose, L., Martins, L. B., Cordeiro, T. M., Lee, K., Diaz, A. P., Ahn, H., & Teixeira, A. L. (2023). Non-Invasive Neuromodulation Methods to Alleviate Symptoms of Huntington’s Disease: A Systematic Review of the Literature. Journal of Clinical Medicine, 12(5), 2002. https://doi.org/10.3390/jcm12052002