
The Clinical Significance of Anaerobic Coverage in the Antibiotic Treatment of Aspiration Pneumonia: A Systematic Review and Meta-Analysis
 ,
,
Abstract
1. Introduction
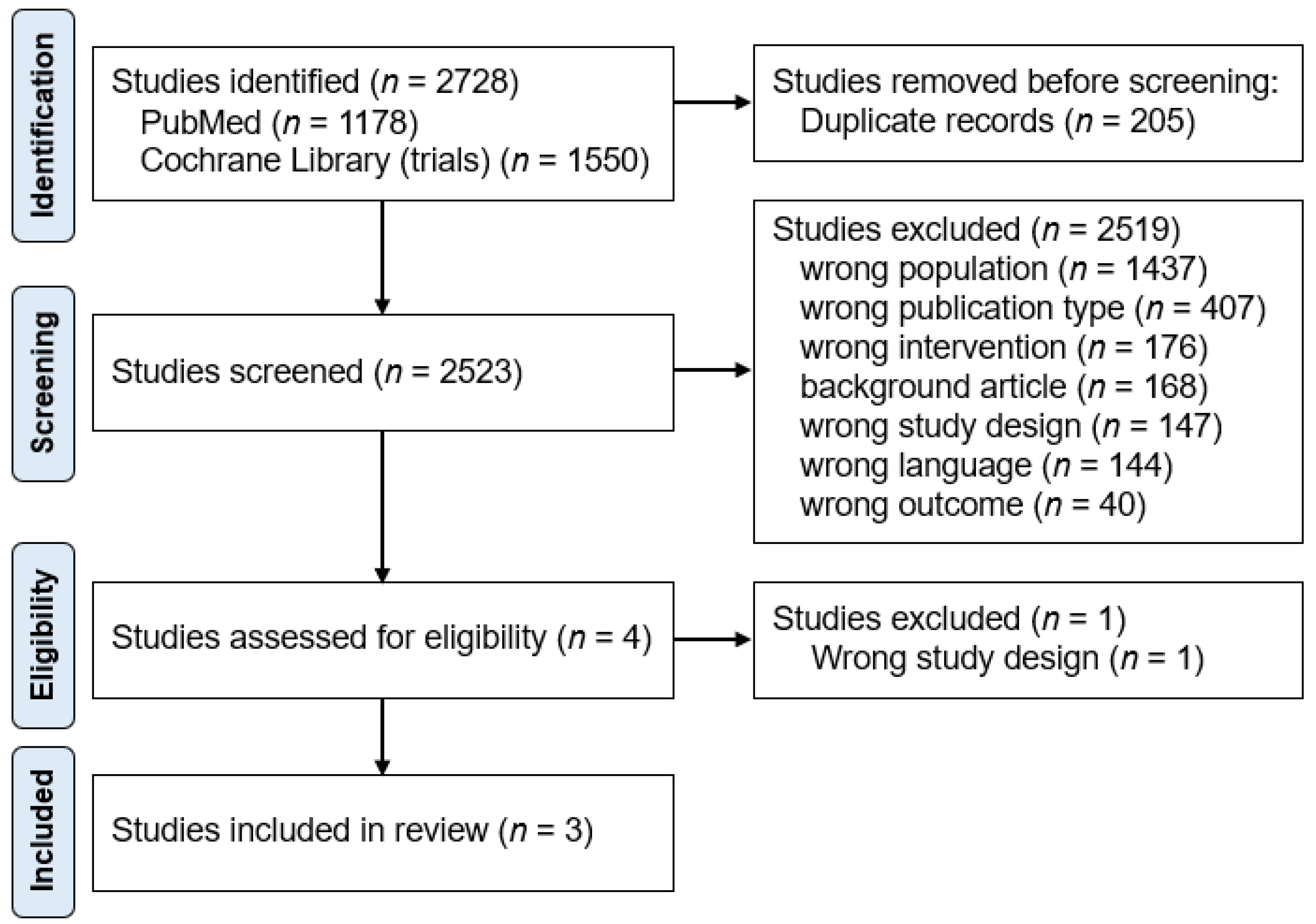
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Search Strategy for PubMED
Appendix A.2. Search Strategy for Cochrane
Appendix A.3. Funnel Plots for Publication Bias Evaluation

References
- Teramoto, S.; Fukuchi, Y.; Sasaki, H.; Sato, K.; Sekizawa, K.; Matsuse, T. High incidence of aspiration pneumonia in community- and hospital-acquired pneumonia in hospitalized patients: A multicenter, prospective study in Japan. J. Am. Geriatr. Soc. 2008, 56, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Komiya, K.; Ishii, H.; Umeki, K.; Mizunoe, S.; Okada, F.; Johkoh, T.; Kadota, J. Impact of aspiration pneumonia in patients with com-munity-acquired pneumonia and healthcare-associated pneumonia: A multicenter retrospective cohort study. Respirology 2013, 18, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G. How Important Are Anaerobic Bacteria in Aspiration Pneumonia: When Should They Be Treated and What Is Optimal Therapy. Infect. Dis. Clin. N. Am. 2013, 27, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G.; Gorbach, S.L.; Finegold, S.M. The bacteriology of aspiration pneumonia. Am. J. Med. 1974, 56, 202–207. [Google Scholar] [CrossRef]
- Cesar, L.; Gonzalez, C.; Calia, F.M. Bacteriologic flora of aspiration-induced pulmonary infections. Arch Intern Med. 1975, 135, 711–714. [Google Scholar] [CrossRef]
- Lorber, B.; Swenson, R.M. Bacteriology of aspiration pneumonia. A prospective study of community- and hospital-acquired cases. Ann. Intern. Med. 1974, 81, 329–331. [Google Scholar] [CrossRef]
- Finegold, S.M. Anaerobic bacteria. Their role in infection and their management. Postgrad. Med. 1987, 81, 141–147. [Google Scholar] [CrossRef]
- Marin-Corral, J.; Pascual-Guardia, S.; Amati, F.; Aliberti, S.; Masclans, J.R.; Soni, N.; Rodriguez, A.; Sibila, O.; Sanz, F.; Sotgiu, G.; et al. Aspiration Risk Factors, Microbiology, and Empiric Antibiotics for Patients Hospitalized with Community-Acquired Pneumonia. Chest 2021, 159, 58–72. [Google Scholar] [CrossRef]
- Mandell, L.A.; Niederman, M.S. Aspiration Pneumonia. N. Engl. J. Med. 2019, 380, 651–663. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the american thoracic society and infectious diseases society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64, iii1–iii55. [Google Scholar] [CrossRef] [PubMed]
- Chanderraj, R.; Baker, J.M.; Kay, S.G.; Brown, C.A.; Hinkle, K.J.; Fergle, D.J.; McDonald, R.A.; Falkowski, N.R.; Metcalf, J.D.; Kaye, K.S.; et al. In critically ill patients, anti-anaerobic antibiotics increase risk of adverse clinical outcomes. Eur. Respir. J. 2023, 61, 2200910. [Google Scholar] [CrossRef] [PubMed]
- Simeonova, M.; Daneman, N.; Lam, P.W.; Elligsen, M. Addition of anaerobic coverage for treatment of biliary tract infections: A propensity score-matched cohort study. JAC Antimicrob. Resist. 2023, 5, dlac141. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.E.; Restrepo, M.I. New perspectives in aspiration community acquired Pneumonia. Expert Rev. Clin. Pharmacol. 2019, 12, 991–1002. [Google Scholar] [CrossRef] [PubMed]
- DiBardino, D.M.; Wunderink, R.G. Aspiration pneumonia: A review of modern trends. J. Crit. Care 2015, 30, 40–48. [Google Scholar] [CrossRef]
- Page, M.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- The Japanese Respiratory Society. The JRS Guidelines for the Management of Pneumonia in Adults; Medical Review Co.: Tokyo, Japan, 2017. [Google Scholar]
- Klompas, M. Aspiration Pneumonia in Adults. UpToDate. 2022. Available online: https://www.uptodate.com/contents/aspiration-pneumonia-in-adults (accessed on 15 September 2022).
- Bowerman, T.J.; Zhang, J.; Waite, L.M. Antibacterial treatment of aspiration pneumonia in older people: A systematic review. Clin. Interv. Aging 2018, 13, 2201–2213. [Google Scholar] [CrossRef]
- Marumo, S.; Teranishi, T.; Higami, Y.; Koshimo, Y.; Kiyokawa, H.; Kato, M. Effectiveness of azithromycin in aspiration pneumonia: A prospective observational study. BMC Infect. Dis. 2014, 14, 685. [Google Scholar] [CrossRef]
- Hasegawa, S.; Shiraishi, A.; Yaegashi, M.; Hosokawa, N.; Morimoto, K.; Mori, T. Ceftriaxone versus ampicillin/sulbactam for the treatment of aspiration-associated pneumonia in adults. J. Comp. Eff. Res. 2019, 8, 1275–1284. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 December 2019).
- Oi, I.; Ito, I.; Tanabe, N.; Konishi, S.; Hamao, N.; Yasutomo, Y.; Kadowaki, S.; Hirai, T. Cefepime vs. meropenem for moderate-to-severe pneumonia in patients at risk for aspiration: An open-label, randomized study. J. Infect. Chemother. 2020, 26, 181–187. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, J.G.; Gorbach, S.L. Treatment of aspiration pneumonia and primary lung abscess. Penicillin G vs clindamycin. JAMA 1975, 234, 935–937. [Google Scholar] [CrossRef] [PubMed]
- Lode, H. Microbiological and clinical aspects of aspiration pneumonia. J. Antimicrob. Chemother. 1988, 21, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E. Aspiration Pneumonitis and Aspiration Pneumonia. N. Engl. J. Med. 2001, 344, 665–671. [Google Scholar] [CrossRef] [PubMed]
- El-Solh, A.A.; Pietrantoni, C.; Bhat, A.; Aquilina, A.T.; Okada, M.; Grover, V.; Gifford, N. Microbiology of Severe Aspiration Pneumonia in Institutionalized Elderly. Am. J. Respir. Crit. Care Med. 2003, 167, 1650–1654. [Google Scholar] [CrossRef]
- Marik, P.E.; Careau, P. The role of anaerobes in patients with ventilator-associated pneumonia and aspiration pneumonia: A prospective study. Chest 1999, 115, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Mier, L.; Dreyfuss, D.; Darchy, B.; Lanore, J.J.; Djedaini, K.; Weber, P.; Brun, P.; Coste, F. Is penicillin G an adequate initial treatment for aspiration pneumonia? A prospective evaluation using a protected specimen brush and quantitative cultures. Intensive Care Med. 1993, 19, 279–284. [Google Scholar] [CrossRef]
- Yoneyama, T.; Yoshida, M.; Matsui, T.; Sasaki, H. Oral care and pneumonia. Oral Care Working Group. Lancet 1999, 354, 515. [Google Scholar] [CrossRef]
- Kocher, T.; Holtfreter, B.; Pitchika, V.; Kuhr, K.; Jordan, R.A. Trends in dental and oral health status in Germany between 1997 and 2014. Bundesgesundheitsblatt Gesundh. Gesundheitsschutz 2021, 64, 782–792. [Google Scholar] [CrossRef]
- Furuta, M.; Takeuchi, K.; Takeshita, T.; Shibata, Y.; Suma, S.; Kageyama, S.; Asakawa, M.; Hata, J.; Yoshida, D.; Shimazaki, Y.; et al. 10-year trend of tooth loss and associated factors in a Japanese population-based longitudinal study. BMJ Open 2021, 11, e048114. [Google Scholar] [CrossRef]
- Raittio, E.; Helakorpi, S.; Suominen, A.L. Age-Period-Cohort Analysis of Toothbrushing Frequency in Finnish Adults: Results from Annual National Cross-Sectional Surveys From 1978 to 2014. Int. Dent. J. 2021, 71, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Yoshimatsu, Y.; Melgaard, D.; Westergren, A.; Skrubbeltrang, C.; Smithard, D.G. The diagnosis of aspiration pneumonia in older persons: A systematic review. Eur. Geriatr. Med. 2022, 13, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Marrie, T.J.; Durant, H.; Yates, L. Community-Acquired Pneumonia Requiring Hospitalization: 5-Year Prospective Study. Rev. Infect. Dis. 1989, 11, 586–599. [Google Scholar] [CrossRef] [PubMed]
- Komiya, K.; Ishii, H.; Kadota, J.-I. Healthcare-associated Pneumonia and Aspiration Pneumonia. Aging Dis. 2015, 6, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Komiya, K.; Yamamoto, T.; Yoshikawa, H.; Goto, A.; Umeki, K.; Johkoh, T.; Hiramatsu, K.; Kadota, J.-I. Factors associated with gravity-dependent dis-tribution on chest CT in elderly patients with community-acquired pneumonia: A retrospective observational study. Sci. Rep. 2022, 12, 8023. [Google Scholar] [CrossRef] [PubMed]
- Yoshimatsu, Y.; Smithard, D.G. A Paradigm Shift in the Diagnosis of Aspiration Pneumonia in Older Adults. J. Clin. Med. 2022, 11, 5214. [Google Scholar] [CrossRef]
- Smithard, D.G.; Yoshimatsu, Y. Pneumonia, Aspiration Pneumonia, or Frailty-Associated Pneumonia? Geriatrics 2022, 7, 115. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Tobino, K.; Ko, Y.; Yasuda, M.; Ide, H.; Oku, Y. Careful history taking detects initially unknown underlying causes of aspiration pneumonia. Geriatr. Gerontol. Int. 2020, 20, 785–790. [Google Scholar] [CrossRef]
- Yoshimatsu, Y.; Tobino, K.; Ortega, O.; Oda, H.; Ota, H.; Kawabata, T.; Hiramatsu, Y.; Murakami, Y.; Clavé, P. Development and implementation of an aspiration pneumonia cause investigation algorithm. Clin. Respir. J. 2022, 17, 20–28. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Design | Setting | Subjects | Age (Years) | Antibiotics (Number of Subjects) | |
|---|---|---|---|---|---|---|---|
| Anaerobic Coverage Group | Control Group | ||||||
| Oi, 2022 [23] | Japan | Open-labeled Randomized comparative trial | Single centre, inpatient | Moderate to severe CAP/NHCAP patients at risk of aspiration | mean 85 | MEPM (86) | CFPM (101) |
| Hasegawa, 2019 [21] | Japan | Prospective observational | Multicentre, inpatient/outpatient | Pneumonia patients with aspiration-related risk factor | median 77 | SBT/ABPC (400) | CTRX (237) |
| Marumo, 2014 [20] | Japan | Prospective observational | Single centre, inpatient/outpatient | Aspiration pneumonia within the NHCAP group B (no risk of MDR pathogen) | mean 78 | SBT/ABPC (81) | AZM (36) |
| Author, Year | Mortality (30 Day * or in Hospital) | Clinical Cure Rate (n, %) | ||||
|---|---|---|---|---|---|---|
| Anaerobic Coverage | Control | OR, 95%CI | Anaerobic Coverage | Control | OR, 95%CI | |
| Oi, 2020 [23] | 7/86 * (8.1%) | 12/101 * (11.9%) | 0.66 [0.25, 1.75] | 73/86 (84.9%) | 83/101 (82.2%) | 1.22 [0.56, 2.66] |
| Hasegawa, 2019 [21] | 40/400 (10.0%) | 15/237 (6.3%) | 1.64 [0.89, 3.05] | NR | NR | NR |
| Marumo, 2014 [20] | 9/81 (11.1%) | 3/36 (8.3%) | 1.38 [0.35, 5.41] | 60/81 (74.1%) | 24/36 (66.7%) | 1.43 [0.61, 3.35] |
| Author, Year | Selection | Comparability | Outcome | Total Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of Exposed Cohort | Selection of Controls | Ascertainment of Exposure | Demonstration that Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Adequate Length of Follow-up | Adequacy of Follow up of Cohorts | ||
| Oi, 2020 [23] | b | a | a | a | a | c | a | a | 7 |
| Hasegawa, 2019 [21] | b | a | a | a | a | c | a | a | 7 |
| Marumo, 2014 [20] | c | a | a | a | a | c | a | a | 6 |
| Outcomes | No of Participants (Studies) | Odds Ratio [95% CI] | Certainty of Evidence (GRADE) | Reason for GRADing | Comments |
|---|---|---|---|---|---|
| Mortality | 941 (3) | 1.24 [0.70, 2.18] | Very low | Risk of bias, imprecision | There may be little or no difference in the mortality. |
| Clinical cure rate | 304 (2) | 1.31 [0.74, 2.33] | Very low | Risk of bias, imprecision | There may be little or no difference in the clinical cure rate. |
| Development of resistant bacteria | 0 (0) | - | - | - | No data available |
| Length of hospital stay | 117 (1) | - | Very low | Risk of bias, imprecision, indirectness | There may be little or no difference in the length of stay. |
| Recurrence rate | 187 (1) | - | Low | Imprecision, indirectness | There may be little or no difference in the rate of recurrence. |
| Adverse effect rate | 176 (1) | - | Low | Imprecision, indirectness | There may be little or no difference in the rate of adverse effects. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimatsu, Y.; Aga, M.; Komiya, K.; Haranaga, S.; Numata, Y.; Miki, M.; Higa, F.; Senda, K.; Teramoto, S. The Clinical Significance of Anaerobic Coverage in the Antibiotic Treatment of Aspiration Pneumonia: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1992. https://doi.org/10.3390/jcm12051992
Yoshimatsu Y, Aga M, Komiya K, Haranaga S, Numata Y, Miki M, Higa F, Senda K, Teramoto S. The Clinical Significance of Anaerobic Coverage in the Antibiotic Treatment of Aspiration Pneumonia: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(5):1992. https://doi.org/10.3390/jcm12051992
Chicago/Turabian StyleYoshimatsu, Yuki, Masaharu Aga, Kosaku Komiya, Shusaku Haranaga, Yuka Numata, Makoto Miki, Futoshi Higa, Kazuyoshi Senda, and Shinji Teramoto. 2023. "The Clinical Significance of Anaerobic Coverage in the Antibiotic Treatment of Aspiration Pneumonia: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 5: 1992. https://doi.org/10.3390/jcm12051992
APA StyleYoshimatsu, Y., Aga, M., Komiya, K., Haranaga, S., Numata, Y., Miki, M., Higa, F., Senda, K., & Teramoto, S. (2023). The Clinical Significance of Anaerobic Coverage in the Antibiotic Treatment of Aspiration Pneumonia: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(5), 1992. https://doi.org/10.3390/jcm12051992