
Femoral Tunnel Position Affects Postoperative Femoral Tunnel Widening after Anterior Cruciate Ligament Reconstruction with Tibialis Anterior Allograft


Abstract
1. Introduction
2. Materials and Methods
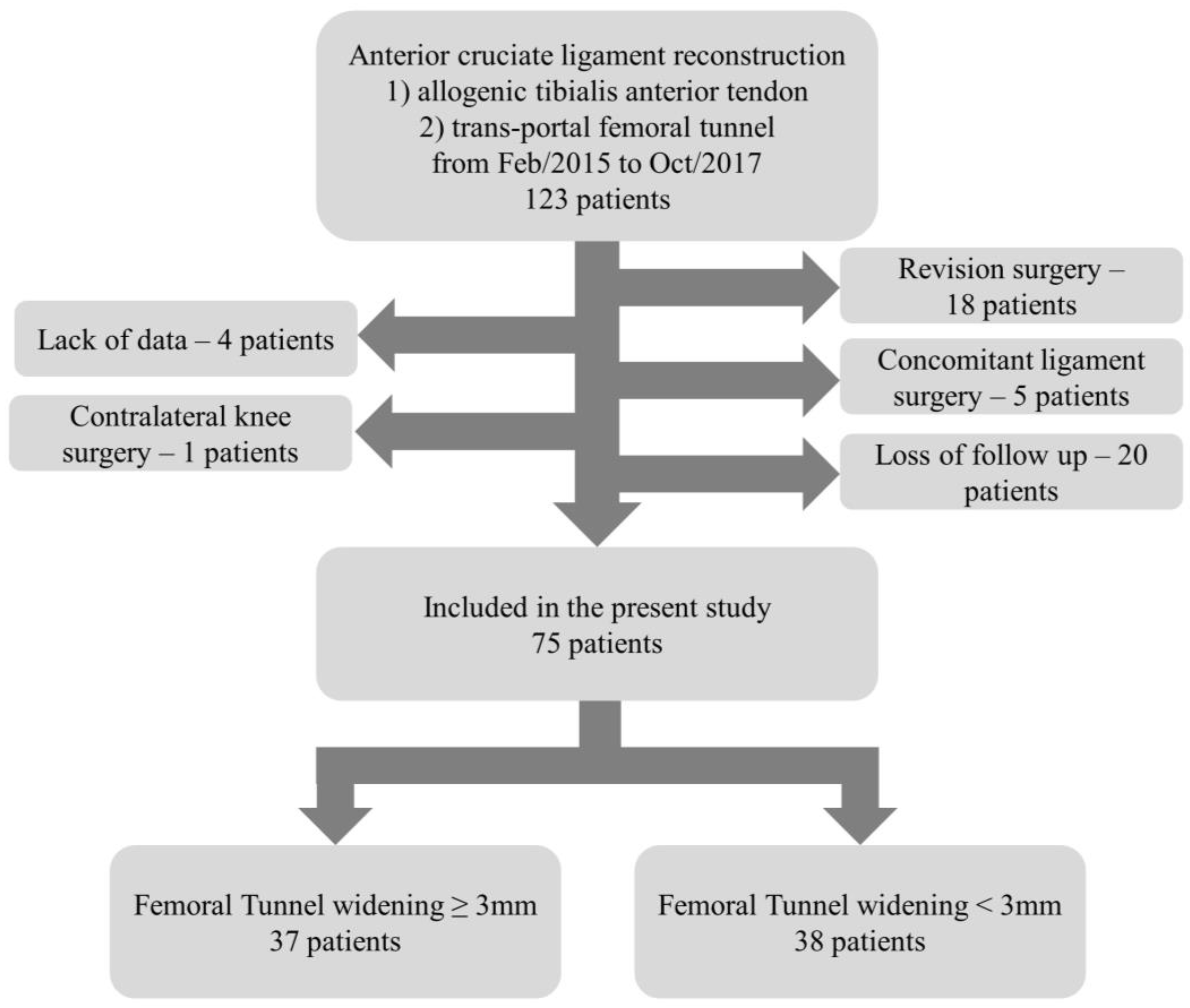
2.1. Study Design and Patients
2.2. Surgical Technique
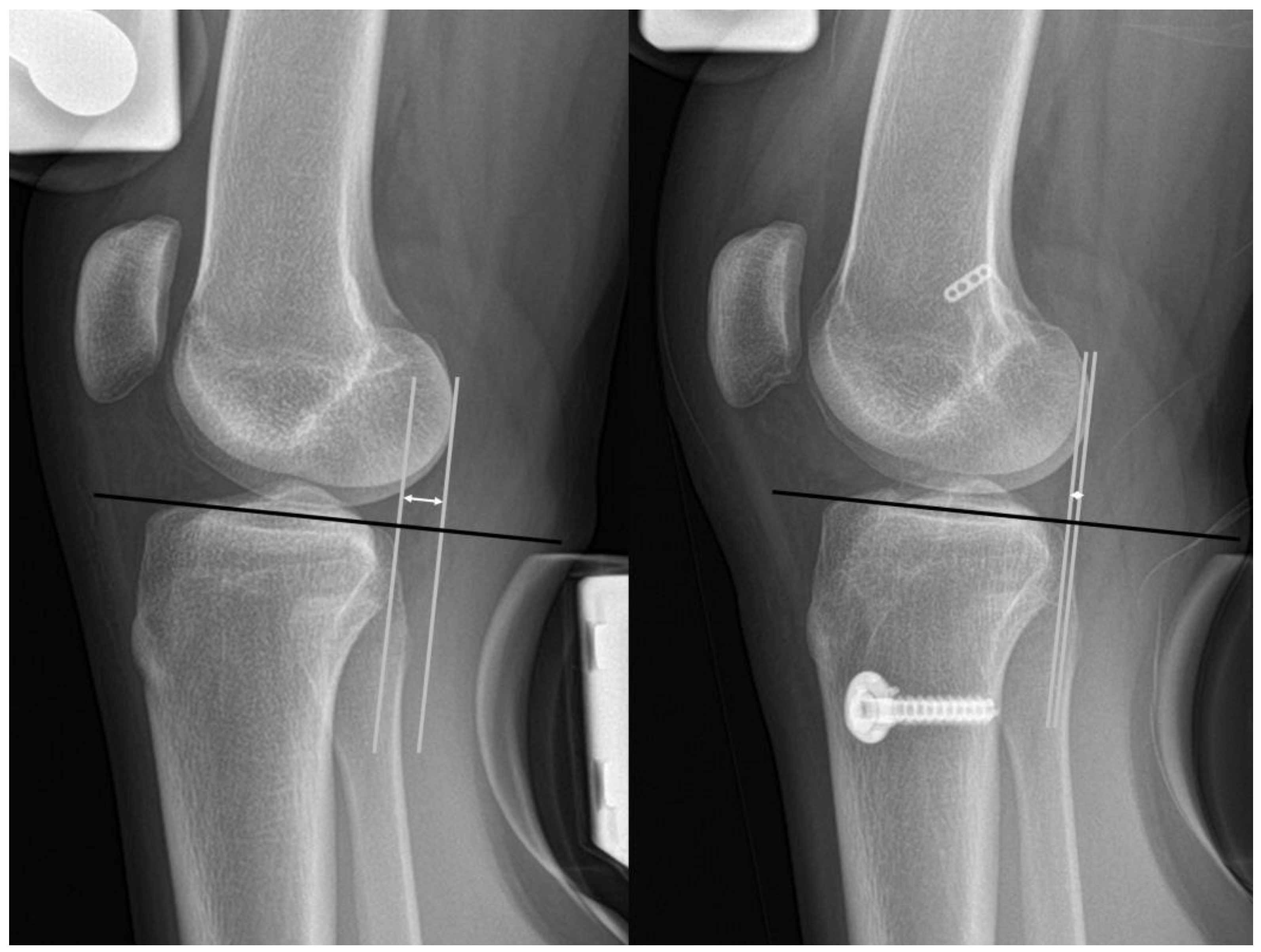
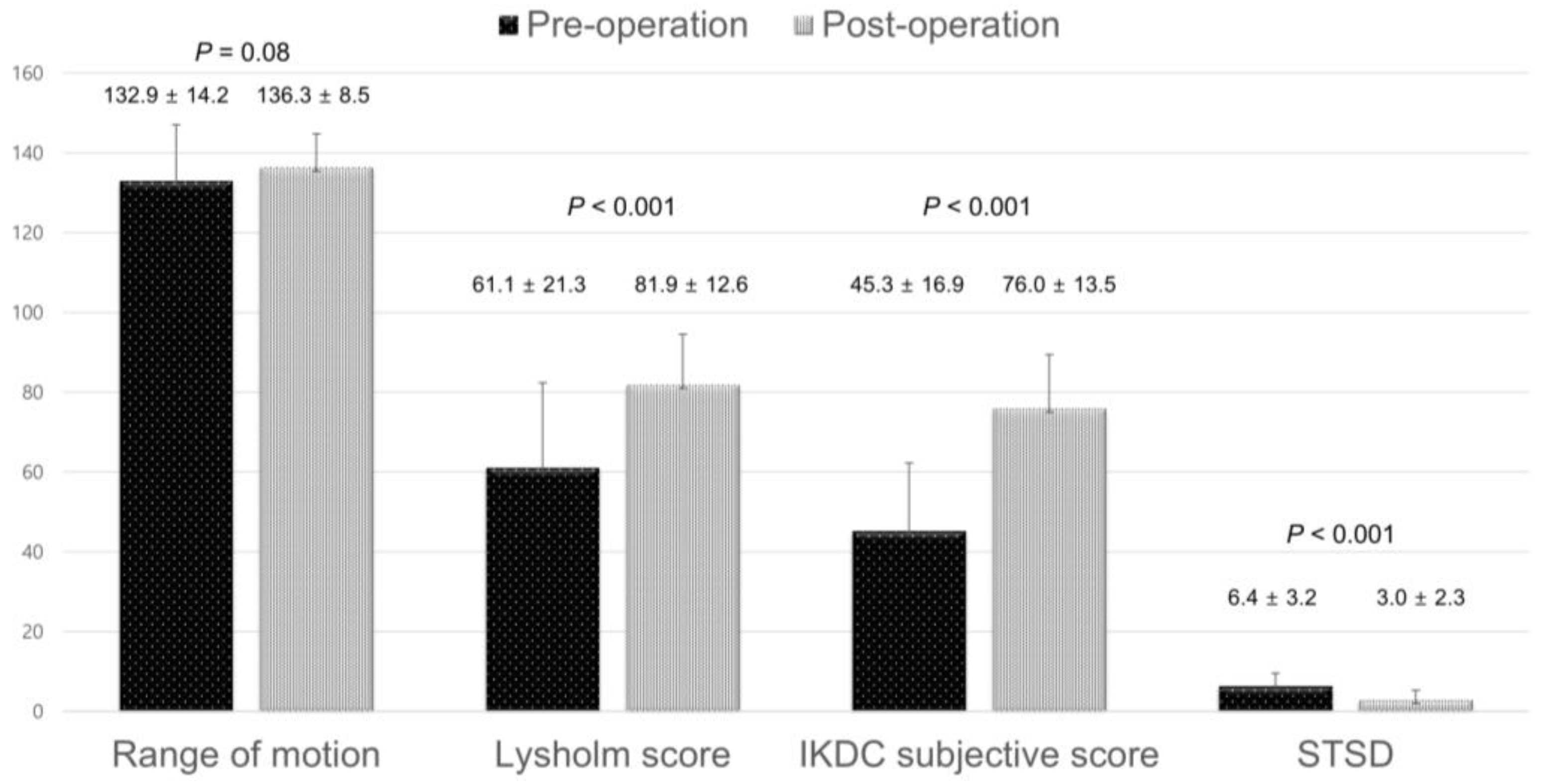
2.3. Clinical and Radiographic Assessments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baumfeld, J.A.; Diduch, D.R.; Rubino, L.J.; Hart, J.A.; Miller, M.D.; Barr, M.S.; Hart, J.M. Tunnel widening following anterior cruciate ligament reconstruction using hamstring autograft: A comparison between double cross-pin and suspensory graft fixation. Knee Surg. Sport. Traumatol. Arthrosc. 2008, 16, 1108–1113. [Google Scholar] [CrossRef]
- Clatworthy, M.G.; Annear, P.; Bulow, J.-U.; Bartlett, R.J. Tunnel widening in anterior cruciate ligament reconstruction: A prospective evaluation of hamstring and patella tendon grafts. Knee Surg. Sport. Traumatol. Arthrosc. 1999, 7, 138–145. [Google Scholar] [CrossRef]
- Sabzevari, S.; Shaikh, H.S.; Arner, J.W.; Irrgang, J.J.; Fu, F.H.; Rahnemai-Azar, A.A. Increased lateral tibial posterior slope is related to tibial tunnel widening after primary ACL reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 31, 2004–3913. [Google Scholar] [CrossRef]
- Schnetzke, M.; Vetter, S.; von der Linden, P.; Grützner, P.-A.; von Recum, J. Two-Stage Revision Anterior Cruciate Ligament Reconstruction Using Silicate-Substituted Calcium Phosphate. Arthrosc. Tech. 2019, 8, e1239–e1246. [Google Scholar] [CrossRef]
- Wolfson, T.S.; Mannino, B.; Owens, B.D.; Waterman, B.R.; Alaia, M.J. Tunnel Management in Revision Anterior Cruciate Ligament Reconstruction: Current Concepts. Am. J. Sport. Med. 2021, 51, 545–556. [Google Scholar] [CrossRef]
- Järvelä, T.; Moisala, A.-S.; Paakkala, T.; Paakkala, A. Tunnel Enlargement After Double-Bundle Anterior Cruciate Ligament Reconstruction: A Prospective, Randomized Study. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.K.; Kim, J.H.; Lee, S.-S.; Lee, B.H.; Kim, H.; Kim, J.; Wang, J.H. Femoral Tunnel Widening After Double-Bundle Anterior Cruciate Ligament Reconstruction with Hamstring Autograft Produces a Small Shift of the Tunnel Position in the Anterior and Distal Direction: Computed Tomography–Based Retrospective Cohort Analysis. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 2554–2563.e1. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Lee, J.W.; Kim, S.B.; Park, J.H.; Chung, K.S.; Ha, J.K.; Kim, J.G.; Kim, W.J. Comparison of Poly-L-Lactic Acid and Poly-L-Lactic Acid/Hydroxyapatite Bioabsorbable Screws for Tibial Fixation in ACL Reconstruction: Clinical and Magnetic Resonance Imaging Results. Clin. Orthop. Surg. 2017, 9, 270–279. [Google Scholar] [CrossRef]
- Weber, A.E.; Delos, D.; Oltean, H.N.; Vadasdi, K.; Cavanaugh, J.; Potter, H.G.; Rodeo, S.A. Tibial and Femoral Tunnel Changes After ACL Reconstruction: A Prospective 2-Year Longitudinal MRI Study. Am. J. Sport. Med. 2015, 43, 1147–1156. [Google Scholar] [CrossRef]
- Lee, M.C.; Seong, S.C.; Lee, S.; Chang, C.B.; Park, Y.K.; Jo, H.; Kim, C.H. Vertical Femoral Tunnel Placement Results in Rotational Knee Laxity After Anterior Cruciate Ligament Reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2007, 23, 771–778. [Google Scholar] [CrossRef]
- Moon, H.-S.; Choi, C.-H.; Yoo, J.-H.; Jung, M.; Lee, T.-H.; Choi, K.-H.; Kim, S.-H. The Graft Insertion Length in the Femoral Tunnel During Anterior Cruciate Ligament Reconstruction with Suspensory Fixation and Tibialis Anterior Allograft Does Not Affect Surgical Outcomes but Is Negatively Correlated with Tunnel Widening. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 2903–2914.e1. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, S.; Kimura, M.; Hagiwara, K.; Ogoshi, A.; Nakagawa, T.; Shiozawa, H.; Ohsawa, T. Patient age as a preoperative factor associated with tunnel enlargement following double-bundle anterior cruciate ligament reconstruction using hamstring tendon autografts. Knee Surg Sport. Traumatol. Arthrosc. 2018, 26, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Clancy, W.G.; Narechania, R.G.; Rosenberg, T.D.; Gmeiner, J.G.; Wisnefske, D.D.; A Lange, T. Anterior and posterior cruciate ligament reconstruction in rhesus monkeys. J. Bone Jt. Surg. 1981, 63, 1270–1284. [Google Scholar] [CrossRef]
- Fahey, M.; Indelicato, P.A. Bone tunnel enlargement after anterior cruciate ligament replacement. Am. J. Sport. Med. 1994, 22, 410–414. [Google Scholar] [CrossRef]
- Kim, S.-J.; Bae, J.-H.; Song, S.-H.; Lim, H.-C. Bone Tunnel Widening with Autogenous Bone Plugs Versus Bioabsorbable Interference Screws for Secondary Fixation in ACL Reconstruction. J. Bone Jt. Surg. 2013, 95, 103–108. [Google Scholar] [CrossRef]
- Silva, A.; Sampaio, R.; Pinto, E. Femoral tunnel enlargement after anatomic ACL reconstruction: A biological problem? Knee Surg Sport. Traumatol. Arthrosc. 2010, 18, 1189–1194. [Google Scholar] [CrossRef]
- Fauno, P.; Kaalund, S. Tunnel Widening After Hamstring Anterior Cruciate Ligament Reconstruction Is Influenced by the Type of Graft Fixation Used: A Prospective Randomized Study. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 1337–1341. [Google Scholar] [CrossRef]
- Sabat, D.; Kundu, K.; Arora, S.; Kumar, V. Tunnel Widening After Anterior Cruciate Ligament Reconstruction: A Prospective Randomized Computed Tomography–Based Study Comparing 2 Different Femoral Fixation Methods for Hamstring Graft. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, 776–783. [Google Scholar] [CrossRef]
- Vadalà, A.; Iorio, R.; De Carli, A.; Argento, G.; Di Sanzo, V.; Conteduca, F.; Ferretti, A. The effect of accelerated, brace free, rehabilitation on bone tunnel enlargement after ACL reconstruction using hamstring tendons: A CT study. Knee Surg. Sport. Traumatol. Arthrosc. 2006, 15, 365–371. [Google Scholar] [CrossRef]
- Choi, N.-H.; Lee, S.-J.; Park, S.-C.; Victoroff, B.N. Comparison of Postoperative Tunnel Widening After Hamstring Anterior Cruciate Ligament Reconstructions Between Anatomic and Nonanatomic Femoral Tunnels. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 36, 1105–1111. [Google Scholar] [CrossRef]
- Ko, Y.W.; Rhee, S.J.; Kim, I.W.; Yoo, J.-D. The Correlation of Tunnel Position, Orientation and Tunnel Enlargement in Outside-in Single-Bundle Anterior Cruciate Ligament Reconstruction. Knee Surg. Relat. Res. 2015, 27, 247–254. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Lajara, F.; Samitier, G.; Cugat, R. The transtibial versus the anteromedial portal technique in the arthroscopic bone-patellar tendon-bone anterior cruciate ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2009, 18, 1013–1037. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosi, R.; Giorgino, R.; Corona, K.; Jaykumar, T.; Mariani, I.; Ursino, N.; Mangiavini, L.; Vaishya, R. Hamstring tendon autografts and allografts show comparable clinical outcomes and knee stability after anterior cruciate ligament reconstruction in patients over fifty years old with no signs of osteoarthritis progression. Int. Orthop. 2022, 46, 2029–2039. [Google Scholar] [CrossRef] [PubMed]
- Soneru, A.; Sarwark, J.F. Survivorship of allograft ACL reconstruction in adolescent patients. J. Orthop. 2019, 16, 11–13. [Google Scholar] [CrossRef]
- Bistolfi, A.; Capella, M.; Guidotti, C.; Sabatini, L.; Artiaco, S.; Massè, A.; Ferracini, R. Functional results of allograft vs. autograft tendons in anterior cruciate ligament (ACL) reconstruction at 10-year follow-up. Eur. J. Orthop. Surg. Traumatol. 2020, 31, 729–735. [Google Scholar] [CrossRef]
- Hu, J.; Qu, J.; Xu, D.; Zhou, J.; Lu, H. Allograft versus autograft for anterior cruciate ligament reconstruction: An up-to-date meta-analysis of prospective studies. Int. Orthop. 2013, 37, 311–320. [Google Scholar] [CrossRef]
- Biswal, U.K.; Balaji, G.; Nema, S.; Poduval, M.; Menon, J.; Patro, D.K. Correlation of tunnel widening and tunnel positioning with short-term functional outcomes in single-bundle anterior cruciate ligament reconstruction using patellar tendon versus hamstring graft: A prospective study. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 647–655. [Google Scholar] [CrossRef]
- Zijl, J.A.C.; Kleipool, A.E.B.; Willems, W.J. Comparison of Tibial Tunnel Enlargement after Anterior Cruciate Ligament Reconstruction Using Patellar Tendon Autograft or Allograft. Am. J. Sport. Med. 2000, 28, 547–551. [Google Scholar] [CrossRef]
- Balazs, G.C.; Brelin, A.M.; Grimm, P.D.; Dickens, J.F.; Keblish, D.J.; Rue, J.H. Hybrid Tibia Fixation of Soft Tissue Grafts in Anterior Cruciate Ligament Reconstruction: A Systematic Review. Am. J. Sport. Med. 2016, 44, 2724–2732. [Google Scholar] [CrossRef]
- Song, I.-S.; Kwon, J. Analysis of changes in tibial torsion angle on open-wedge high tibial osteotomy depending on the osteotomy level. Knee Surg. Relat. Res. 2022, 34, 17. [Google Scholar] [CrossRef]
- Repo, J.P.; Uimonen, M.M.; Nevalainen, M.T.; Nurmi, H.; Ponkilainen, V.T.; Tuominen, A.; Paloneva, J. Outcomes following the operative treatment of intra-articular fracture combined with medial patellofemoral ligament reconstruction after patellar dislocation. Knee Surg. Relat. Res. 2022, 34, 21. [Google Scholar] [CrossRef] [PubMed]
- Helito, C.P.; da Silva, A.G.M.; Guimarães, T.M.; Sobrado, M.F.; Pécora, J.R.; Camanho, G.L. Functional results of multiple revision anterior cruciate ligament with anterolateral tibial tunnel associated with anterolateral ligament reconstruction. Knee Surg. Relat. Res. 2022, 34, 24. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.Y.; Lee, D.K.; Kim, H.S.; Wang, J.H. How to achieve an optimal alignment in medial opening wedge high tibial osteotomy? Knee Surg Relat Res. 2022, 34, 3. [Google Scholar] [CrossRef]
- Lee, H.W.; Park, C.H.; Bae, D.K.; Song, S.J. How much preoperative flexion contracture is a predictor for residual flexion contracture after total knee arthroplasty in hemophilic arthropathy and rheumatoid arthritis? Knee Surg Relat Res. 2022, 34, 20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-M.; Ha, C.; Jung, K.; Choi, W. Clinical Results after Design Modification of Lospa Total Knee Arthroplasty System: Comparison between Posterior-Stabilized (PS) and PS Plus Types. Clin. Orthop. Surg. 2022, 14, 236–243. [Google Scholar] [CrossRef]
- Kim, S.H.; Park, Y.B.; Ham, D.W.; Lim, J.W.; Lee, H.J. Stress radiography at 30 degrees of knee flexion is a reliable evaluation tool for high-grade rotatory laxity in complete ACL-injured knees. Knee Surg Sport. Traumatol. Arthrosc. 2020, 28, 2233–2244. [Google Scholar] [CrossRef]
- L’Insalata, J.C.; Klatt, B.; Fu, F.H.; Harner, C.D. Tunnel expansion following anterior cruciate ligament reconstruction: A comparison of hamstring and patellar tendon autografts. Knee Surg. Sport. Traumatol. Arthrosc. 1997, 5, 234–238. [Google Scholar] [CrossRef]
- Linn, R.M.; Fischer, D.A.; Smith, J.P.; Burstein, D.B.; Quick, D.C. Achilles tendon allograft reconstruction of the anterior cruciate ligament-deficient knee. Am. J. Sport. Med. 1993, 21, 825–831. [Google Scholar] [CrossRef]
- Höher, J.; Livesay, G.A.; Ma, C.B.; Withrow, J.D.; Fu, F.H.; Woo, S.L.-Y. Hamstring graft motion in the femoral bone tunnel when using titanium button/ polyester tape fixation. Knee Surg. Sport. Traumatol. Arthrosc. 1999, 7, 215–219. [Google Scholar] [CrossRef]
- Nakazato, K.; Taketomi, S.; Inui, H.; Yamagami, R.; Kawaguchi, K.; Tanaka, S. Lateral posterior tibial slope and length of the tendon within the tibial tunnel are independent factors to predict tibial tunnel widening following anatomic anterior cruciate ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 3818–3824. [Google Scholar] [CrossRef]
- Zhang, Q.; Hao, G.; Gu, M.; Cao, X. Tibial tunnel enlargement and joint instability after anterior cruciate ligament reconstruction. A prospective comparison between autograft and allograft. Acta Cir. Bras. 2017, 32, 1064–1074. [Google Scholar] [CrossRef]
- Amano, H.; Tanaka, Y.; Kita, K.; Uchida, R.; Tachibana, Y.; Yonetani, Y.; Mae, T.; Shiozaki, Y.; Horibe, S. Significant anterior enlargement of femoral tunnel aperture after hamstring ACL reconstruction, compared to bone–patellar tendon–bone graft. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 27, 461–470. [Google Scholar] [CrossRef]
- Kim, S.-J.; Bae, J.-H.; Lim, H.-C. Comparison of Achilles and tibialis anterior tendon allografts after anterior cruciate ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 22, 135–141. [Google Scholar] [CrossRef]
- Parkinson, B.; Robb, C.; Thomas, M.; Thompson, P.; Spalding, T. Factors That Predict Failure in Anatomic Single-Bundle Anterior Cruciate Ligament Reconstruction. Am. J. Sport. Med. 2017, 45, 1529–1536. [Google Scholar] [CrossRef]
- Musahl, V.; Plakseychuk, A.; VanScyoc, A.; Sasaki, T.; Debski, R.E.; McMahon, P.J.; Fu, F.H. Varying femoral tunnels between the anatomical footprint and isometric positions: Effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am. J. Sport. Med. 2005, 33, 712–718. [Google Scholar] [CrossRef] [PubMed]
- Rayan, F.; Nanjayan, S.K.; Quah, C.; Ramoutar, D.; Konan, S.; Haddad, F.S. Review of evolution of tunnel position in anterior cruciate ligament reconstruction. World J. Orthop. 2015, 6, 252–262. [Google Scholar] [CrossRef]
- Hussein, M.; van Eck, C.F.; Cretnik, A.; Dinevski, D.; Fu, F.H. Prospective randomized clinical evaluation of conventional single-bundle, anatomic single-bundle, and anatomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to 5-year follow-up. Am. J. Sport. Med. 2012, 40, 512–520. [Google Scholar] [CrossRef]
- Byrne, K.J.; Hughes, J.D.; Gibbs, C.; Vaswani, R.; Meredith, S.J.; Popchak, A.; Lesniak, B.P.; Karlsson, J.; Irrgang, J.J.; Musahl, V. Non-anatomic tunnel position increases the risk of revision anterior cruciate ligament reconstruction. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 30, 1388–1395. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lee, E.S.; Ko, T.W.; Lee, Y.S. Femoral tunnel placement in single-bundle, remnant-preserving anterior cruciate ligament reconstruction using a posterior trans-septal portal. Knee 2019, 26, 628–635. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria |
| (1) total ACL rupture diagnosed during magnetic resonance imaging or arthroscopic examination |
| (2) ACL reconstruction using a tibialis anterior allograft |
| (3) follow-up for more than 24 months |
| Exclusion criteria |
| (1) revision ACL reconstruction |
| (2) concomitant ligament surgery |
| (3) history of contralateral knee surgery |
| (4) lack of clinical or radiographic data |
| Number of Patients | 75 |
| Age, year | 31.5 ± 12.0 (18–60) |
| Sex, M:F | 61:14:00 |
| Body mass index, kg/m2 | 24.9 ± 3.7 (18.5–34.7) |
| Side of injury, Right:Left | 42:33:00 |
| Combined meniscus injury, n (%) | |
| Medial | 33 (44%) |
| Lateral | 10 (13.3%) |
| Both | 7 (9.3%) |
| HKA angle, degree | 0.5 ± 2.56 (−5.8–9.2) |
| Tibial slope, degree | 10.8 ± 3.3 (3.1–17.8) |
| Femoral tunnel length, mm | 29.5 ± 4.8 (20–40) |
| Tibial tunnel length, mm | 35.0 ± 5.2 (24–48) |
| Femoral tunnel position, % | |
| Depth | 29.6 ± 7.0 (17–53) |
| Height | 33.3 ± 8.7 (5–48) |
| Tibia tunnel position, % | |
| Anteroposterior | 44.0 ± 2.6 (36–51) |
| Mediolateral | 42.8 ± 6.6 (29–54) |
| Immediately after Operation | 2-Year after Operation | p Value | |
|---|---|---|---|
| Femoral tunnel width on AP radiograph, mm | 10.1 ± 1.0 | 13.1 ± 1.8 | <0.001 |
| Femoral tunnel width on lateral radiograph, mm | 9.9 ± 1.2 | 12.4 ± 1.8 | <0.001 |
| Tibial tunnel width on AP radiograph, mm | 10.3 ± 0.9 | 13.2 ± 1.4 | <0.001 |
| Tibial tunnel width on lateral radiograph, mm | 10.7 ± 1.1 | 13.6 ± 1.5 | <0.001 |
| Femoral TW ≥ 3 mm | Femoral TW < 3 mm | p-Value | |
|---|---|---|---|
| Number of patients | 37 | 38 | |
| Age, year | 33.1 ± 13.5 | 29.9 ± 10.3 | 0.257 |
| Sex, male:female | 30:07:00 | 31:07:00 | 0.956 |
| Body mass index, kg/m2 | 24.9 ± 3.9 | 24.9 ± 3.5 | 0.975 |
| Direction, right:left | 21:16 | 21:17 | 0.896 |
| Combined meniscal injury, n | |||
| Medial meniscus | 17 | 16 | 0.902 |
| Lateral meniscus | 5 | 5 | 0.831 |
| Both medial and lateral | 3 | 4 | 0.978 |
| Hip-knee-ankle angle, ° | 0.8 ± 2.6 | 0.1 ± 2.5 | 0.218 |
| Tibial slope, ° | 11.2 ± 3.6 | 10.4 ± 3.0 | 0.272 |
| Femoral tunnel length, mm | 29.5 ± 5.0 | 29.5 ± 4.7 | 0.98 |
| Tibial tunnel length, mm | 35.8 ± 5.5 | 33.9 ± 4.7 | 0.105 |
| Femoral tunnel position—Depth, % | 31.7 ± 7.3 | 27.6 ± 6.3 | 0.014 |
| Femoral tunnel position—Height, % | 32.8 ± 8.8 | 33.6 ± 8.8 | 0.638 |
| Tibia tunnel position—AP, % | 43.6 ± 6.9 | 42.0 ± 6.3 | 0.288 |
| Tibia tunnel position—ML, % | 44.1 ± 2.6 | 44.0 ± 2.6 | 0.751 |
| Preoperative ROM, ° | 130.7 ± 15.5 | 128.2 ± 15.2 | 0.546 |
| Preoperative Lysholm score | 62.0 ± 24.0 | 55.7 ± 17.8 | 0.33 |
| Preoperative IKDC subjective score | 44.9 ± 20.1 | 42.6 ± 14.3 | 0.671 |
| Preoperative STSD, mm | 6.4 ± 2.7 | 6.5 ± 3.6 | 0.949 |
| Postoperative 2-year ROM, ° | 138.4 ± 9.3 | 136.5 ± 8.5 | 0.44 |
| Postoperative 2-year Lysholm score | 84.1 ± 12.1 | 87.0 ± 11.8 | 0.318 |
| Postoperative 2-year IKDC subjective score | 78.4 ± 12.3 | 76.6 ± 14.6 | 0.583 |
| Postoperative 2-year STSD, mm | 3.7 ± 2.0 | 2.4 ± 2.3 | 0.013 |
| Tibial TW ≥ 3 mm | Tibial TW < 3 mm | p-Value | |
|---|---|---|---|
| Number of patients | 34 | 41 | |
| Age, year | 21.2 ± 12.0 | 30.9 ± 12.1 | 0.651 |
| Sex, male:female | 26:08:00 | 35:06:00 | 0.381 |
| Body mass index, kg/m2 | 24.8 ± 4.2 | 25.0 ± 3.2 | 0.849 |
| Direction, right:left | 19:15 | 23:18 | 0.985 |
| Combined meniscal injury, n | |||
| Medial meniscus | 15 | 18 | 0.598 |
| Lateral meniscus | 5 | 5 | 0.786 |
| Both medial and lateral | 2 | 5 | 0.813 |
| Hip-knee-ankle angle, ° | 0.7 ± 2.3 | 0.3 ± 2.7 | 0.494 |
| Tibial slope, ° | 11.4 ± 3.8 | 10.3 ± 2.9 | 0.153 |
| Femoral tunnel length, mm | 29.5 ± 3.3 | 29.5 ± 5.8 | 0.96 |
| Tibial tunnel length, mm | 34.8 ± 5.5 | 34.9 ± 4.9 | 0.971 |
| Femoral tunnel position—Depth, % | 29.0 ± 6.9 | 30.1 ± 7.3 | 0.544 |
| Femoral tunnel position—Height, % | 34.1 ± 8.7 | 32.6 ± 8.7 | 0.465 |
| Tibia tunnel position—AP, % | 44.0 ± 6.6 | 41.8 ± 6.5 | 0.15 |
| Tibia tunnel position—ML, % | 44.1 ± 2.6 | 44.0 ± 2.7 | 0.88 |
| Preoperative ROM, ° | 131.7 ± 12.6 | 127.5 ± 15.5 | 0.324 |
| Preoperative Lysholm score | 62.5 ± 24.4 | 55.2 ± 17.0 | 0.258 |
| Preoperative IKDC subjective | 44.0 ± 19.5 | 43.5 ± 15.3 | 0.932 |
| Preoperative STSD, mm | 6.7 ± 4.0 | 6.2 ± 2.3 | 0.426 |
| Postoperative 2-year ROM, ° | 136.6 ± 8.9 | 138.3 ± 8.9 | 0.489 |
| Postoperative 2-year Lysholm score | 83.5 ± 13.9 | 87.4 ± 9.9 | 0.184 |
| Postoperative 2-year IKDC subjective score | 76.3 ± 13.5 | 78.4 ± 13.5 | 0.535 |
| Postoperative 2-year STSD, mm | 3.6 ± 2.1 | 2.6 ± 2.3 | 0.055 |
| Dependent Variable | Independent Variables | Non-Standardized Coefficients | Standardized Coefficients | p-Value | |
|---|---|---|---|---|---|
| B | SE | B | |||
| Femoral tunnel widening on AP radiograph (Initial→2 years) | Age | 0.014 | 0.018 | 0.238 | |
| Sex | −0.146 | 0.649 | 0.567 | ||
| Body mass index | 0.001 | 0.061 | 0.696 | ||
| Medial meniscus injury | −0.085 | 0.434 | 0.751 | ||
| Lateral meniscus injury | −0.225 | 0.597 | 0.635 | ||
| Hip-knee-ankle angle | 0.081 | 0.085 | 0.173 | ||
| Tibial slope | −0.012 | 0.073 | 0.724 | ||
| Femoral tunnel length | −0.007 | 0.051 | 0.981 | ||
| Tibial tunnel length | 0.007 | 0.059 | 0.536 | ||
| Femoral tunnel position—Depth | 8.813 | 3.798 | 0.387 | 0.003 | |
| Femoral tunnel position—Height | 1.355 | 2.597 | 0.485 | ||
| Tibia tunnel position—AP | 0.54 | 9.384 | 0.613 | ||
| Tibia tunnel position—ML | 3.527 | 4.272 | 0.39 | ||
| Dependent Variable | Independent Variables | Non-Standardized Coefficients | Standardized Coefficients | p-Value | |
|---|---|---|---|---|---|
| B | SE | B | |||
| Femoral tunnel widening on the lateral radiograph (Initial→2 years) | Age | −0.009 | 0.015 | 0.524 | |
| Sex | −0.456 | 0.538 | 0.401 | ||
| Body mass index | 0.002 | 0.051 | 0.972 | ||
| Medial meniscus injury | −0.097 | 0.36 | 0.789 | ||
| Lateral meniscus injury | −0.204 | 0.495 | 0.681 | ||
| Hip-knee-ankle angle | 0.129 | 0.071 | 0.077 | ||
| Tibial slope | −0.044 | 0.061 | 0.478 | ||
| Femoral tunnel length | −0.054 | 0.042 | 0.21 | ||
| Tibial tunnel length | −0.039 | 0.049 | 0.435 | ||
| Femoral tunnel position—Depth | 8.462 | 2.348 | 0.437 | 0.001 | |
| Femoral tunnel position—Height | 0.221 | 2.153 | 0.919 | ||
| Tibia tunnel position—AP | −5.223 | 7.779 | 0.506 | ||
| Tibia tunnel position—ML | 2.672 | 3.541 | 0.455 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-S.; Kim, I.S.; Shin, T.S.; Lee, J.; Lee, D.-H. Femoral Tunnel Position Affects Postoperative Femoral Tunnel Widening after Anterior Cruciate Ligament Reconstruction with Tibialis Anterior Allograft. J. Clin. Med. 2023, 12, 1966. https://doi.org/10.3390/jcm12051966
Lee S-S, Kim IS, Shin TS, Lee J, Lee D-H. Femoral Tunnel Position Affects Postoperative Femoral Tunnel Widening after Anterior Cruciate Ligament Reconstruction with Tibialis Anterior Allograft. Journal of Clinical Medicine. 2023; 12(5):1966. https://doi.org/10.3390/jcm12051966
Chicago/Turabian StyleLee, Sung-Sahn, Il Su Kim, Tae Soo Shin, Jeounghun Lee, and Dae-Hee Lee. 2023. "Femoral Tunnel Position Affects Postoperative Femoral Tunnel Widening after Anterior Cruciate Ligament Reconstruction with Tibialis Anterior Allograft" Journal of Clinical Medicine 12, no. 5: 1966. https://doi.org/10.3390/jcm12051966
APA StyleLee, S.-S., Kim, I. S., Shin, T. S., Lee, J., & Lee, D.-H. (2023). Femoral Tunnel Position Affects Postoperative Femoral Tunnel Widening after Anterior Cruciate Ligament Reconstruction with Tibialis Anterior Allograft. Journal of Clinical Medicine, 12(5), 1966. https://doi.org/10.3390/jcm12051966