
Effect of Digitalis on ICD or CRT-D Recipients: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Outcomes and Subgroups
2.5. Statistical Analysis
3. Results
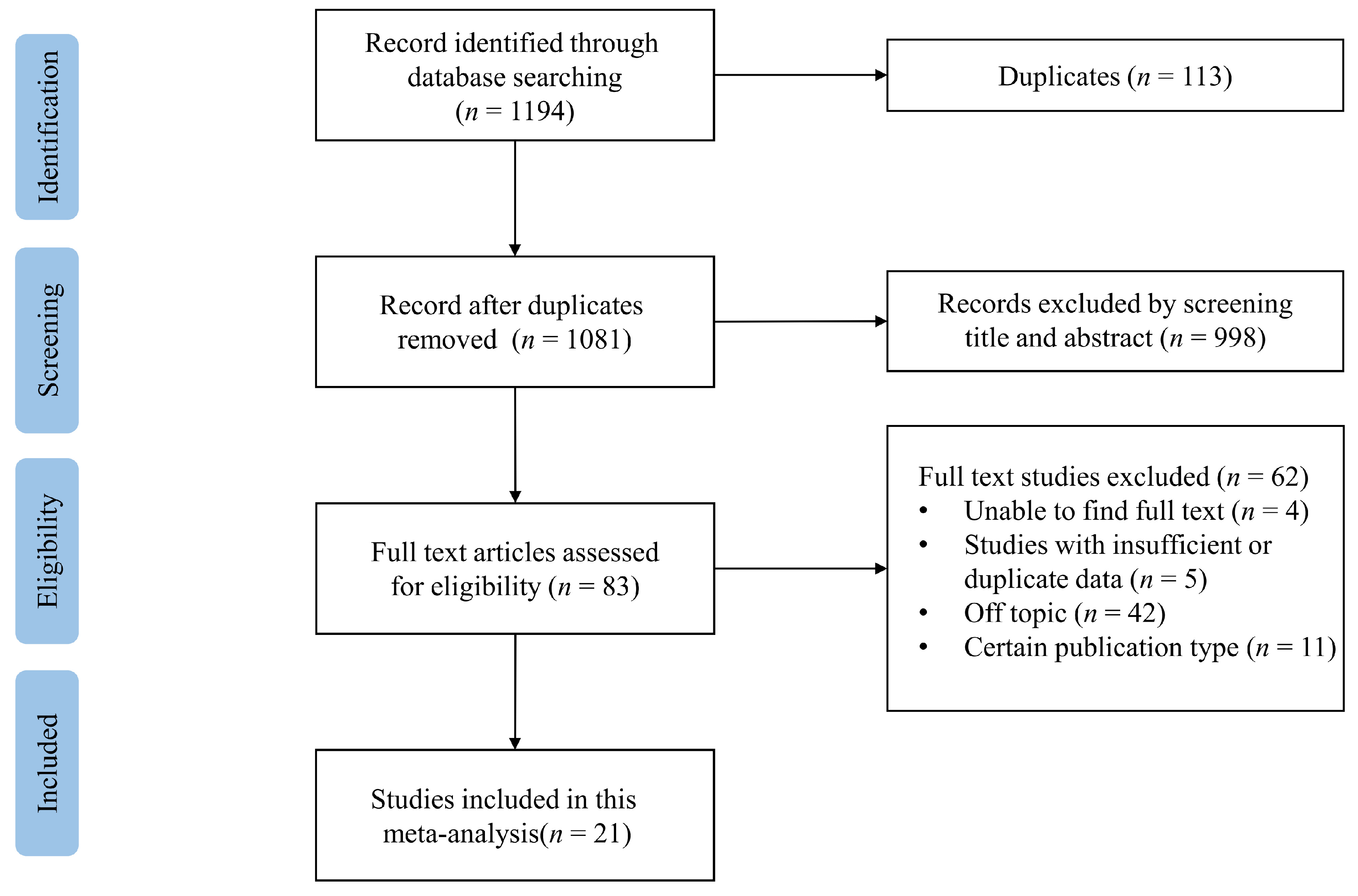
3.1. Study Selection and Study Characteristics
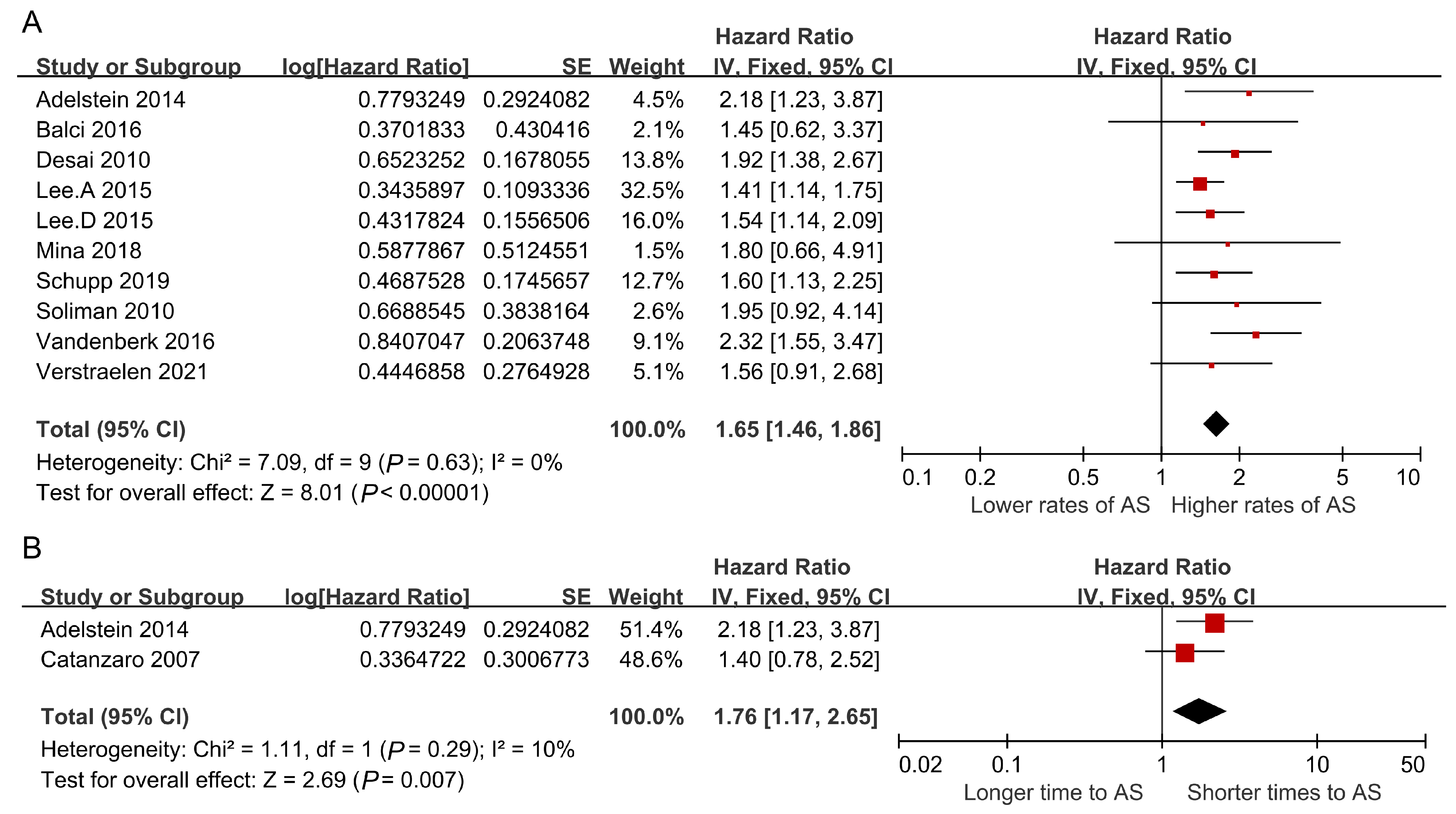
3.2. Digitalis and Appropriate Shocks
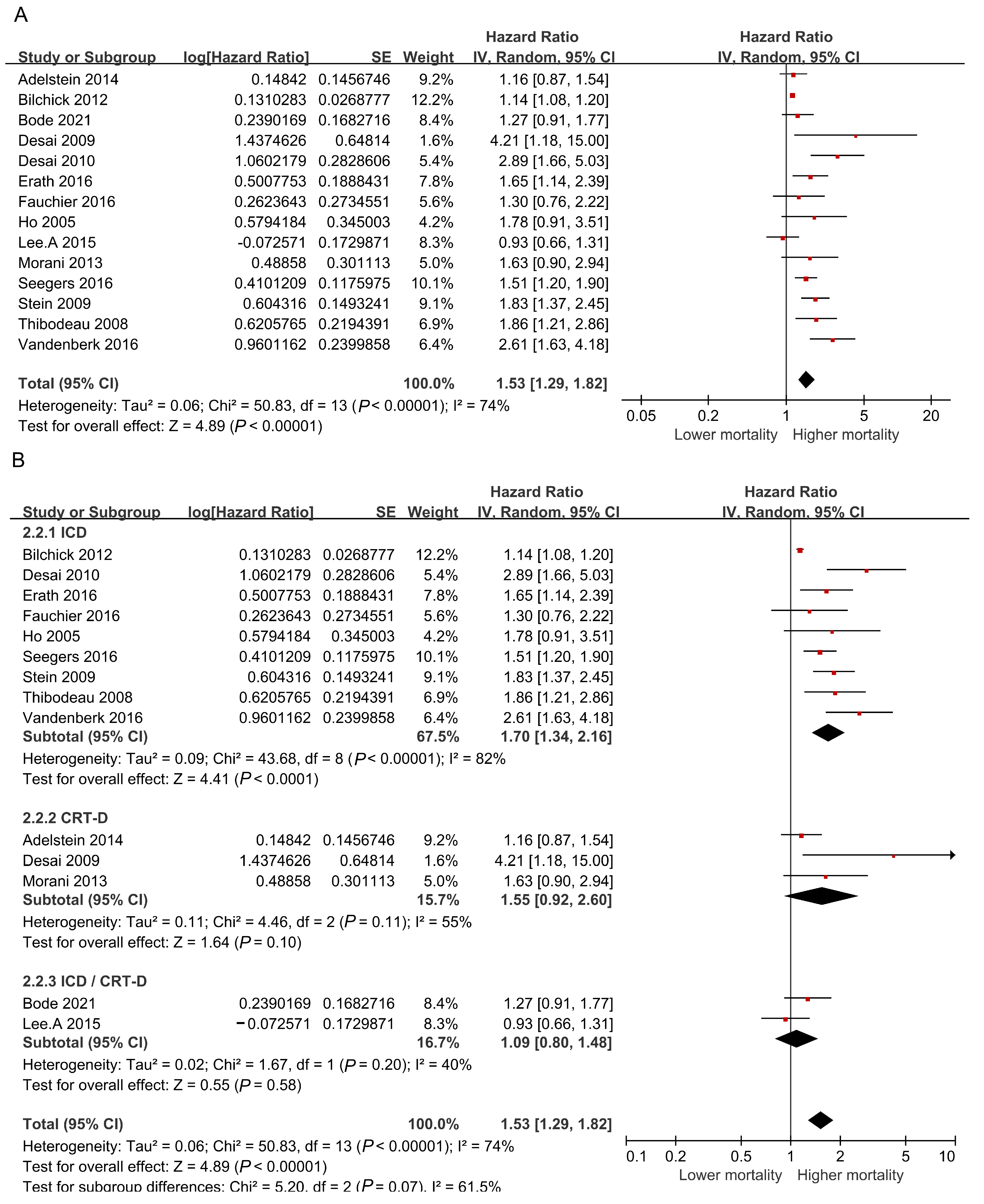
3.3. Digitalis and All-Cause Mortality
4. Discussion
4.1. Possible Mechanisms of Digitalis in Appropriate Device Shocks
4.2. Possible Mechanisms of Digitalis in Mortality
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations and Acronyms
| ICD | Implantable Cardioverter Defibrillator |
| CRT-D | Cardiac Resynchronization Therapy Defibrillator |
| HRs | Hazard Ratios |
| CIs | Confidence Intervals |
| HF | Heart Failure |
| AF | Atrial Fibrillation |
| SCD | Sudden Cardiac Death |
| LVEF | Left Ventricular Ejection Fractions |
| VT/VF | Ventricular Tachycardia/Fibrillation |
| NOS | Newcastle–Ottawa Scale |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| MeSH | Medical Subject Headings |
| NYHA | New York Heart Association |
| RevMan | Review Manager |
References
- Gumprecht, J.; Domek, M.; Proietti, M.; Li, Y.G.; Asaad, N.; Rashed, W.; Alsheikh-Ali, A.; Zubaid, M.; Lip, G.Y.H. Compliance of Atrial Fibrillation Treatment with the Atrial Fibrillation Better Care (ABC) Pathway Improves the Clinical Outcomes in the Middle East Population: A Report from the Gulf Survey of Atrial Fibrillation Events (SAFE) Registry. J. Clin. Med. 2020, 9, 1286. [Google Scholar] [CrossRef] [PubMed]
- Ziff, O.J.; Kotecha, D. Digoxin: The good and the bad. Trends Cardiovasc. Med. 2016, 26, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef]
- Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N. Engl. J. Med. 1997, 336, 525–533. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Zareba, W.; Hall, W.J.; Klein, H.; Wilber, D.J.; Cannom, D.S.; Daubert, J.P.; Higgins, S.L.; Brown, M.W.; Andrews, M.L.; et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N. Engl. J. Med. 2002, 346, 877–883. [Google Scholar] [CrossRef]
- Chen, Z.; Kotecha, T.; Crichton, S.; Shetty, A.; Sohal, M.; Arujuna, A.; Kirubakaran, S.; Bostock, J.; Cooklin, M.; O’Neill, M.; et al. Lower incidence of inappropriate shock therapy in patients with combined cardiac resynchronisation therapy defibrillators (CRT-D) compared with patients with non-CRT defibrillators (ICDs). Int. J. Clin. Pr. 2013, 67, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Steffen, M.M.; Osborn, J.S.; Cutler, M.J. Cardiac Implantable Electronic Device Therapy: Permanent Pacemakers, Implantable Cardioverter Defibrillators, and Cardiac Resynchronization Devices. Med. Clin. N. Am. 2019, 103, 931–943. [Google Scholar] [CrossRef]
- Lee, A.Y.; Kutyifa, V.; Ruwald, M.H.; McNitt, S.; Polonsky, B.; Zareba, W.; Moss, A.J.; Ruwald, A.C. Digoxin therapy and associated clinical outcomes in the MADIT-CRT trial. Heart Rhythm. 2015, 12, 2010–2017. [Google Scholar] [CrossRef]
- Vamos, M.; Erath, J.W.; Hohnloser, S.H. Digoxin-associated mortality: A systematic review and meta-analysis of the literature. Eur. Heart J. 2015, 36, 1831–1838. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Adelstein, E.; Schwartzman, D.; Jain, S.; Bazaz, R.; Saba, S. Effect of digoxin on shocks in cardiac resynchronization therapy-defibrillator patients with coronary artery disease. Am. J. Cardiol. 2014, 113, 970–975. [Google Scholar] [CrossRef]
- Balci, K.G.; Balci, M.M.; Şen, F.; Akboǧa, M.K.; Maden, O.; Selçuk, H.; Selçuk, T.; Balbay, Y.; Temizhan, A.; Aydoǧdu, S. The relation between digoxin and appropriate shocks in patients with ischemic heart failure and implantable cardioverter defibrillator. Anatol. J. Cardiol. 2016, 16, 52. [Google Scholar]
- Bilchick, K.C.; Stukenborg, G.J.; Kamath, S.; Cheng, A. Prediction of mortality in clinical practice for medicare patients undergoing defibrillator implantation for primary prevention of sudden cardiac death. J. Am. Coll. Cardiol. 2012, 60, 1647–1655. [Google Scholar] [CrossRef]
- Catanzaro, J.N.; Makaryus, A.N.; Sison, C.; Vavasis, C.; Donaldson, D.; Beldner, S.; Boal, B.; Jadonath, R. Clinical predictors of appropriate implantable-cardioverter defibrillator discharge. Pacing Clin. Electrophysiol. 2007, 30 (Suppl. 1), S120–S124. [Google Scholar] [CrossRef]
- Desai, H.; Aronow, W.S.; Tsai, F.S.; Ahn, C.; Lai, H.M.; Amin, H.; Gandhi, K.; Frishman, W.H.; Cohen, M.; Sorbera, C. Statins reduce appropriate cardioverter-defibrillator shocks and mortality in patients with heart failure and combined cardiac resynchronization and implantable cardioverter-defibrillator therapy. J. Cardiovasc. Pharm. 2009, 14, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Desai, H.; Aronow, W.S.; Ahn, C.; Gandhi, K.; Hussain, S.; Lai, H.M.; Sharma, M.; Frishman, W.H.; Cohen, M.; Sorbera, C. Risk factors for appropriate cardioverter-defibrillator shocks, inappropriate cardioverter-defibrillator shocks, and time to mortality in 549 patients with heart failure. Am. J. Cardiol. 2010, 105, 1336–1338. [Google Scholar] [CrossRef]
- Erath, J.W.; Vamos, M.; Hohnloser, S.H. Effects of digitalis on mortality in a large cohort of implantable cardioverter defibrillator recipients: Results of a long-Term follow-up study in 1020 patients. Eur. Heart J.—Cardiovasc. Pharmacother. 2016, 2, 168–174. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ho, A.T.; Pai, S.M.; Timothy, P.; Pai, R.G. Effect of concomitant antiarrhythmic therapy on survival in patients with implantable cardioverter defibrillators. Pacing Clin. Electrophysiol. 2005, 28, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Hardy, J.; Yee, R.; Healey, J.S.; Birnie, D.; Simpson, C.S.; Crystal, E.; Mangat, I.; Nanthakumar, K.; Wang, X.; et al. Clinical Risk Stratification for Primary Prevention Implantable Cardioverter Defibrillators. Circ. Heart Fail. 2015, 8, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Mina, G.S.; Acharya, M.; Shepherd, T.; Gobrial, G.; Tekeste, M.; Watti, H.; Bhandari, R.; Saini, A.; Reddy, P.; Dominic, P. Digoxin Is Associated With Increased Shock Events and Electrical Storms in Patients With Implantable Cardioverter Defibrillators. J. Cardiovasc. Pharmacol. Ther. 2018, 23, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Morani, G.; Gasparini, M.; Zanon, F.; Casali, E.; Spotti, A.; Reggiani, A.; Bertaglia, E.; Solimene, F.; Molon, G.; Accogli, M.; et al. Cardiac resynchronization therapy-defibrillator improves long-term survival compared with cardiac resynchronization therapy-pacemaker in patients with a class IA indication for cardiac resynchronization therapy: Data from the Contak Italian Registry. Europace 2013, 15, 1273–1279. [Google Scholar] [CrossRef]
- Schupp, T.; Behnes, M.; Weiss, C.; Nienaber, C.; Reiser, L.; Bollow, A.; Taton, G.; Reichelt, T.; Ellguth, D.; Engelke, N.; et al. Digitalis therapy and risk of recurrent ventricular tachyarrhythmias and ICD therapies in atrial fibrillation and heart failure. Cardiology 2019, 142, 129–140. [Google Scholar] [CrossRef]
- Fauchier, L.; Clementy, N.; Marijon, E.; Defaye, P.; Piot, O.; Sadoul, N.; Gras, D.; Klug, D.; Algalarrondo, V.; Bordachar, P.; et al. Effect of digoxin on mortality in patients after primary prevention implantable cardioverter-defibrillator. A multicenter population-based cohort study. Heart Rhythm. 2016, 13, S257. [Google Scholar]
- Soliman, O.I.; Theuns, D.A.; van Dalen, B.M.; Vletter, W.B.; Nemes, A.; Jordaens, L.J.; Balk, A.H.; Ten Cate, F.J.; Geleijnse, M.L. Prediction of appropriate defibrillator therapy in heart failure patients treated with cardiac resynchronization therapy. Am. J. Cardiol. 2010, 105, 105–111. [Google Scholar] [CrossRef]
- Seegers, J.; Conen, D.; Jung, K.; Bergau, L.; Dorenkamp, M.; Lüthje, L.; Sohns, C.; Sossalla, S.T.; Fischer, T.H.; Hasenfuss, G.; et al. Sex difference in appropriate shocks but not mortality during long-term follow-up in patients with implantable cardioverter-defibrillators. Europace 2016, 18, 1194–1202. [Google Scholar] [CrossRef] [PubMed]
- Stein, K.M.; Mittal, S.; Gilliam, F.R.; Gilligan, D.M.; Zhong, Q.; Kraus, S.M.; Meyer, T.E. Predictors of early mortality in implantable cardioverter-defibrillator recipients. Europace 2009, 11, 734–740. [Google Scholar] [CrossRef]
- Thibodeau, J.B.; Pillarisetti, J.; Khumri, T.M.; Jones, P.G.; Main, M.L. Mortality Rates and Clinical Predictors of Reduced Survival After Cardioverter Defibrillator Implantation. Am. J. Cardiol. 2008, 101, 861–864. [Google Scholar] [CrossRef]
- Verstraelen, T.E.; van Barreveld, M.; van Dessel, P.; Boersma, L.V.A.; Delnoy, P.; Tuinenburg, A.E.; Theuns, D.; van der Voort, P.H.; Kimman, G.P.; Buskens, E.; et al. Development and external validation of prediction models to predict implantable cardioverter-defibrillator efficacy in primary prevention of sudden cardiac death. Europace 2021, 23, 887–897. [Google Scholar] [CrossRef]
- Bode, N.; Hochadel, M.; Andresen, D.; Zahn, R.; Spitzer, S.G.; Brachmann, J.; Stellbrink, C.; Jung, W.; Gonska, B.D.; Reinke, F.; et al. Cardiac glycosides are not associated with increased mortality or hospitalization rates in ICD and CRT-ICD patients after adjustment for baseline-characteristics at one-year follow-up: Results from the German DEVICE registry. Int. J. Cardiol. 2021, 338, 109–114. [Google Scholar] [CrossRef]
- Vandenberk, B.; Garweg, C.; Voros, G.; Flore, V.; Marynissen, T.; Sticherling, C.; Zabel, M.; Ector, J.; Willems, R. Changes in Implantation Patterns and Therapy Rates of Implantable Cardioverter Defibrillators over Time in Ischemic and Dilated Cardiomyopathy Patients. Pacing Clin. Electrophysiol. 2016, 39, 848–857. [Google Scholar] [CrossRef]
- Biton, Y.; Daimee, U.A.; Baman, J.R.; Kutyifa, V.; McNitt, S.; Polonsky, B.; Zareba, W.; Goldenberg, I. Prognostic Importance of Defibrillator-Appropriate Shocks and Antitachycardia Pacing in Patients With Mild Heart Failure. J. Am. Heart Assoc. 2019, 8, e010346. [Google Scholar] [CrossRef]
- Smith, T.W. Digitalis. Mechanisms of action and clinical use. N. Engl. J. Med. 1988, 318, 358–365. [Google Scholar] [PubMed]
- Gonano, L.A.; Sepulveda, M.; Rico, Y.; Kaetzel, M.; Valverde, C.A.; Dedman, J.; Mattiazzi, A.; Vila Petroff, M. Calcium-calmodulin kinase II mediates digitalis-induced arrhythmias. Circ. Arrhythm. Electrophysiol. 2011, 4, 947–957. [Google Scholar] [CrossRef]
- Ferrier, G.R. Digitalis arrhythmias: Role of oscillatory afterpotentials. Prog. Cardiovasc. Dis. 1977, 19, 459–474. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, A.; Russo, V.; Bianchi, V.; Cavallaro, C.; Leonardi, S.; De Vivo, S.; Vecchione, F.; Rago, A.; Ammendola, E.; Tavoletta, V.; et al. Effects of defibrillation shock in patients implanted with a subcutaneous defibrillator: A biomarker study. Europace 2018, 20, f233–f239. [Google Scholar] [CrossRef]
- Francis, C.K.; Kuo, Y.H.; Azzam, I.; Selim, S.; Patel, N.; Beri, R.; Goldman, D.; Girgis, I.; Daniels, S. Brain natriuretic peptide and biomarkers of myocardial ischemia increase after defibrillation threshold testing. Pacing Clin. Electrophysiol. 2012, 35, 314–319. [Google Scholar] [CrossRef]
- Tsuji, Y.; Hojo, M.; Voigt, N.; El-Armouche, A.; Inden, Y.; Murohara, T.; Dobrev, D.; Nattel, S.; Kodama, I.; Kamiya, K. Ca(2+)-related signaling and protein phosphorylation abnormalities play central roles in a new experimental model of electrical storm. Circulation 2011, 123, 2192–2203. [Google Scholar] [CrossRef] [PubMed]
- Pakhomov, A.G.; Shevin, R.; White, J.A.; Kolb, J.F.; Pakhomova, O.N.; Joshi, R.P.; Schoenbach, K.H. Membrane permeabilization and cell damage by ultrashort electric field shocks. Arch. Biochem. Biophys. 2007, 465, 109–118. [Google Scholar] [CrossRef]
- Lee, R.C.; Zhang D and Hannig, J. Biophysical injury mechanisms in electrical shock trauma. Annu. Rev. Biomed. Eng. 2000, 2, 477–509. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [PubMed]
- Barsheshet, A.; Wang, P.J.; Moss, A.J.; Solomon, S.D.; Al-Ahmad, A.; McNitt, S.; Foster, E.; Huang, D.T.; Klein, H.U.; Zareba, W.; et al. Reverse remodeling and the risk of ventricular tachyarrhythmias in the MADIT-CRT (Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy). J. Am. Coll. Cardiol. 2011, 57, 2416–2423. [Google Scholar] [CrossRef] [PubMed]
- Hasdemir, C.; Shah, N.; Rao, A.P.; Acosta, H.; Matsudaira, K.; Neas, B.R.; Reynolds, D.W.; Po, S.; Lazzara, R.; Beckman, K.J. Analysis of troponin I levels after spontaneous implantable cardioverter defibrillator shocks. J. Cardiovasc. Electrophysiol. 2002, 13, 144–150. [Google Scholar] [CrossRef]
- Pedersen, S.S.; den Broek, K.C.; Theuns, D.A.; Erdman, R.A.; Alings, M.; Meijer, A.; Jordaens, L.; Denollet, J. Risk of chronic anxiety in implantable defibrillator patients: A multi-center study. Int. J. Cardiol. 2011, 147, 420–423. [Google Scholar] [CrossRef]
- Passman, R.; Subacius, H.; Ruo, B.; Schaechter, A.; Howard, A.; Sears, S.F.; Kadish, A. Implantable cardioverter defibrillators and quality of life: Results from the defibrillators in nonischemic cardiomyopathy treatment evaluation study. Arch. Intern Med. 2007, 167, 2226–2232. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study (First Author, Year) | Study Design | Region | Number of Participants (N) | Follow-Up Duration (m) | Age (year) | Male (%) | AF (%) | LVEF | QRS (ms) | Prevention Types | Disease | Medicine | Therapy | Outcome Events |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adelstein, 2014 [13] | Prospective study | USA | Digitalis: 162; non-digitalis: 188 | 48 ± 32 | Digitalis: 69 ± 10; non-digitalis: 71 ± 10 | Digitalis:77; non-digitalis: 84 | Digitalis: 32; non-digitalis: 26 | Digitalis: 21 ± 6; non-digitalis: 23 ± 6 | Digitalis: 165 ± 26; non-digitalis: 160 ± 24 | Primary | HF | Digoxin | CRT-D | Death/AS/time to first AS |
| Balci, 2016 [14] | Retrospective study | Turkey | 139 | NA | NA | NA | NA | NA | NA | NA | HF | Digoxin | ICD | AS |
| Bilchick, 2012 [15] | Prospective study | USA | 17,991 | 52.8 (median) | 72.5 (median) | 38.9 | NA | NA | NA | Primary | HF | Digoxin | ICD | Death |
| Bode, 2021 [31] | Prospective study | Germany | ICD: digitalis: 525; non-digitalis: 3257 | 1 y | ICD: digitalis: 65.7 ± 12.1; non-digitalis: 64 ± 13.7 | ICD: digitalis: 85.3; non-digitalis: 81.4 | NA | LVEF < 35%: digitalis: 85.7%; non-digitalis: 66.3% | QRS ≥ 130 ms: digitalis: 25.2%; non-digitalis: 18.4% | Primary | AF/ HF | Cardiac glycosides | ICD/CRT-D | Death |
| Catanzaro, 2007 [16] | Retrospective study | USA | 591 | 10.9 ± 13.8 | 67.9 ± 13.0 | 80.2 | Male: 5.9; female: 8.6 | LVEF < 35%: male: 61.7%; female: 52.4% | NA | NA | NA | Digitalis | ICD | Time to first AS |
| Desai, 2009 [17] | Retrospective study | USA | 209 | 41.4 ± 21.8 | 74 (median) | 79.9 | NA | NA | NA | NA | HF | Digoxin | ICD | Death |
| Desai, 2010 [18] | Retrospective study | USA | 549 | 34 (mean) | Inappropriate shock: 75 ± 6; non-inappropriate shocks: 73 ± 10 | Inappropriate shock: 77; non-inappropriate shocks: 79 | Inappropriate shock:41; non-inappropriate shocks: 9 | Inappropriate shock: 28 ± 8; non-inappropriate shocks: 29 ± 7 | Inappropriate shock: 117 ± 21; non-inappropriate shocks: 118 ± 19 | NA | HF | Digoxin | ICD | AS/death |
| Erath, 2016 [19] | Retrospective study | Germany | Digitalis: 438; non-digitalis: 582 | 37 (median) | Digitalis: 63; non-digitalis: 62 | Digitalis: 79; non-digitalis: 80 | Digitalis: 21; non-digitalis: 10 | Digitalis: 26; non-digitalis: 38 | QRS ≥ 120 ms: digitalis: 47%; non-digitalis: 33% | Primary: digoxin: 57%; non-digoxin: 57% secondary: digoxin: 43%; non-digoxin: 43% | NA | Digitalis | ICD | Death |
| Fauchier, 2016 [25] | Retrospective study | France | Digoxin: 225; non-digoxin: 3759 | 3.1 ± 2 y | Digoxin: 63 ± 11; non-digoxin: 63 ± 11 | NA | Digoxin: 51; non-digoxin: 20 | Digoxin: 24; non-digoxin: 27 | NA | Primary | AF/ HF | Digoxin | ICD | Death |
| Ho, 2005 [20] | Retrospective study | USA | 360 | 52.8 ± 44.4 | 62 ± 13 | 80 | NA | 33 ± 17 | NA | NA | NA | Digoxin | ICD | Death |
| Lee.A, 2015 [10] | Retrospective study | USA | Digoxin: 468; non-digoxin: 1352 | NA | Digoxin: 62.8 ± 11.9; non-digoxin: 65 ± 10.3 | Digoxin: 65; non-digoxin: 79 | Digoxin: 12; non-digoxin: 12 | Digoxin: 23.2 ± 5.5; non-digoxin: 24 ± 5.2 | Digoxin: 160 ± 21.3; non-digoxin: 157.2 ± 19.1 | NA | HF | Digoxin | ICD/CRT-D | AS/death |
| Lee.D, 2015 [21] | Prospective study | Canada | 3445 | 5918 person-years | 66 (58,30) | 80 | NA | NA | NA | Primary | HF | Digoxin | ICD | AS |
| Mina, 2018 [22] | Retrospective study | USA | Digoxin: 55; non-digoxin: 147 | NA | Digoxin: 60.18 ± 12.23; non-digoxin: 61.44 ± 9.44 | Digoxin: 61.8; non-digoxin: 64.6 | Digoxin: 10.9; non-digoxin: 6.1 | Digoxin: 27.86 ± 13.03; non-digoxin: 27.38 ± 11.18 | QRS > 120 ms: digoxin: 31.6%; non-digoxin: 28.8% | Primary: digoxin: 90.9%; non-Digoxin: 91.2% Secondary: digoxin: 9.1%; non-digoxin: 8.8% | AF/ HF | Digoxin | ICD | Shocks |
| Morani, 2013 [23] | Retrospective study | Italy | 374 | 55 (median) | 69 ± 10 | 80 | NA | 27 ± 5 | 168 ± 31 | Primary: 84%; Secondary: 16% | HF | Digoxin | CRT-D | Death |
| Schupp, 2019 [24] | Retrospective study | Germany | Digitalis: 104; non-digitalis: 290 | 60 (median) | Digitalis: 68; non-digitalis: 66 | Digitalis: 80; non-digitalis: 82 | Digitalis: 57; non-digitalis: 39 | LVEF < 35%: digitalis: 73%; non-digitalis: 62% | Digitalis: 109 ± 8; non-digitalis: 117 ± 5 | Primary: digoxin: 45%; non-digoxin: 46% Secondary: digoxin: 55%; non-digoxin: 54% | AF/ HF | Digitalis | ICD | Appropriate device therapy |
| Seegers, 2016 [27] | Retrospective study | Germany | 1151 | 58.8 ± 32.4 | Male: 65 ± 12; female: 62 ± 15 | 81.2 | NA | Male: 29 ± 11; female: 34 ± 13 | Male: 123 ± 32; female: 112 ± 30 | Primary: female: 53%; male: 55%; Secondary: female: 47%; male: 45% | NA | Digitalis | ICD | Death |
| Soliman, 2010 [26] | Retrospective study | Netherlands | 169 | 654 ± 394 days | 60 ± 12 | 74 | NA | 22 ± 4 | 166 ± 30 | Primary | HF | Digitalis | CRT-D | AS |
| Stein, 2009 [28] | Prospective study | USA | 1703 | 12.5 (median) | 67 ± 12 | 82 | 26 | LVEF < 20:10% 20 ≤ LVEF < 30:30% 30 ≤ LVEF < 40:33% 40 ≤ LVEF: 24% | NA | Primary: 48%; secondary: 52% | NA | Digitalis | ICD | Death |
| Thibodeau, 2008 [29] | Retrospective study | USA | 286 | 40 ± 21.7 | 64.7 ± 13.4 | 82.9 | NA | 10 ≤ LVEF < 25:37.1% 25 ≤ LVEF < 35:28.8% 35 ≤ LVEF < 45:18.7% 45 ≤ LVEF < 70:15.5% | NA | Primary: 39.5%; secondary: 60.1%; unknown: 0.3% | NA | Digoxin | ICD | Death |
| Vandenberk, 2016 [32] | Retrospective study | USA | 727 | 5.2 ± 4.1 y | 62.5 ± 11.7 | 84.9 | 8.1 | 32.4 ± 12.4 | 131 ± 34 | Primary: 56%; secondary: 44% | ICM or NICM | Digitalis | ICD | AS/Death |
| Verstraelen, 2021 [30] | Prospective study | England | DO-IT:1443; EU-CERT-ICD:1450 | 2.4 y | DO-IT: 65.9; EU-CERT-ICD: 61.9 | DO-IT: 72; EU-CERT-ICD: 83 | DO-IT: 31; EU-CERT-ICD: 25 | DO-IT: 26.1; EU-CERT-ICD: 27.5 | QRS > 150 ms DO-IT: 23%; EU-CERT-ICD: 2% | Primary | HF | Digoxin | ICD/CRT-D | AS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhuo, W.; Liu, H.; Fu, L.; Fan, W.; Hong, K. Effect of Digitalis on ICD or CRT-D Recipients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1686. https://doi.org/10.3390/jcm12041686
Zhuo W, Liu H, Fu L, Fan W, Hong K. Effect of Digitalis on ICD or CRT-D Recipients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(4):1686. https://doi.org/10.3390/jcm12041686
Chicago/Turabian StyleZhuo, Wen, Hualong Liu, Linghua Fu, Weiguo Fan, and Kui Hong. 2023. "Effect of Digitalis on ICD or CRT-D Recipients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 4: 1686. https://doi.org/10.3390/jcm12041686
APA StyleZhuo, W., Liu, H., Fu, L., Fan, W., & Hong, K. (2023). Effect of Digitalis on ICD or CRT-D Recipients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(4), 1686. https://doi.org/10.3390/jcm12041686