
The Efficacy of Platelet-Rich Plasma Injection Therapy in the Treatment of Patients with Achilles Tendinopathy: A Systematic Review and Meta-Analysis

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Search Methods
2.4. Literature Selection
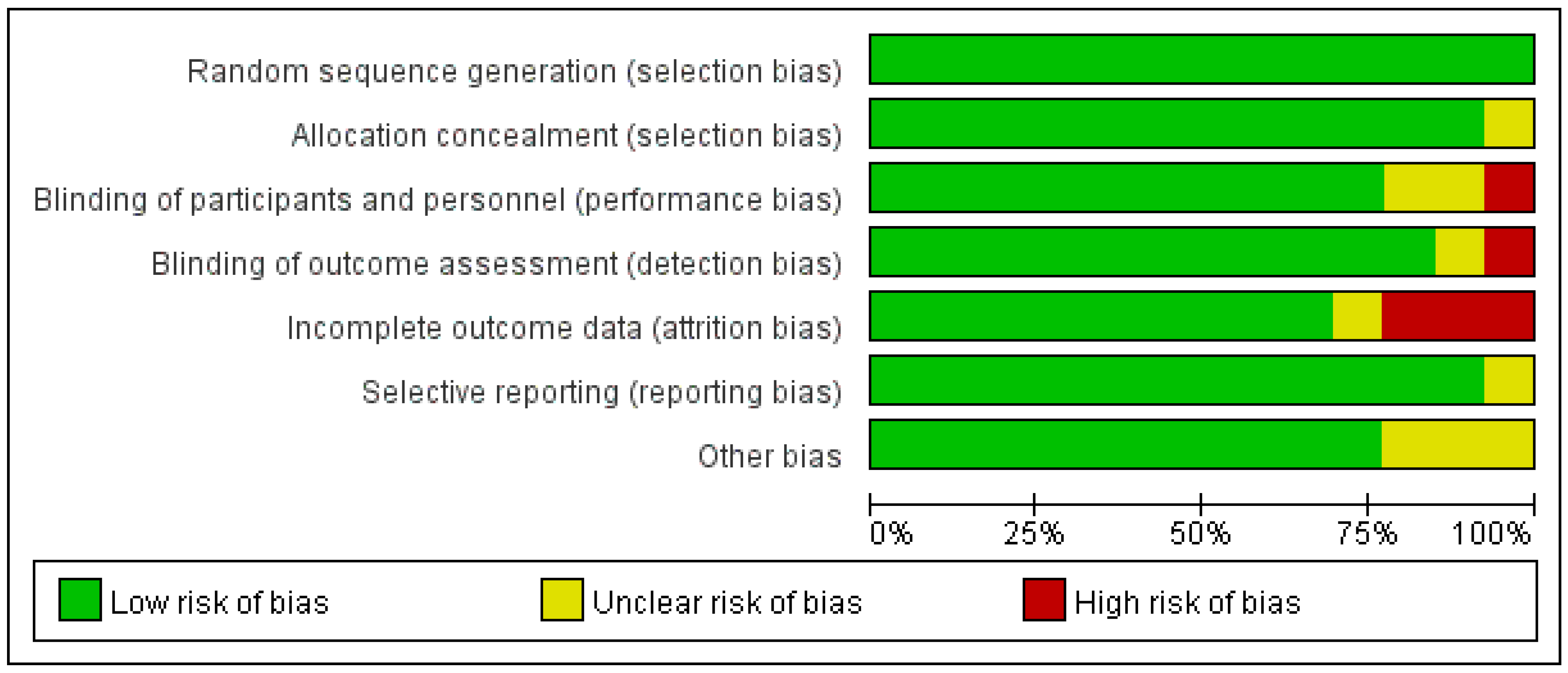
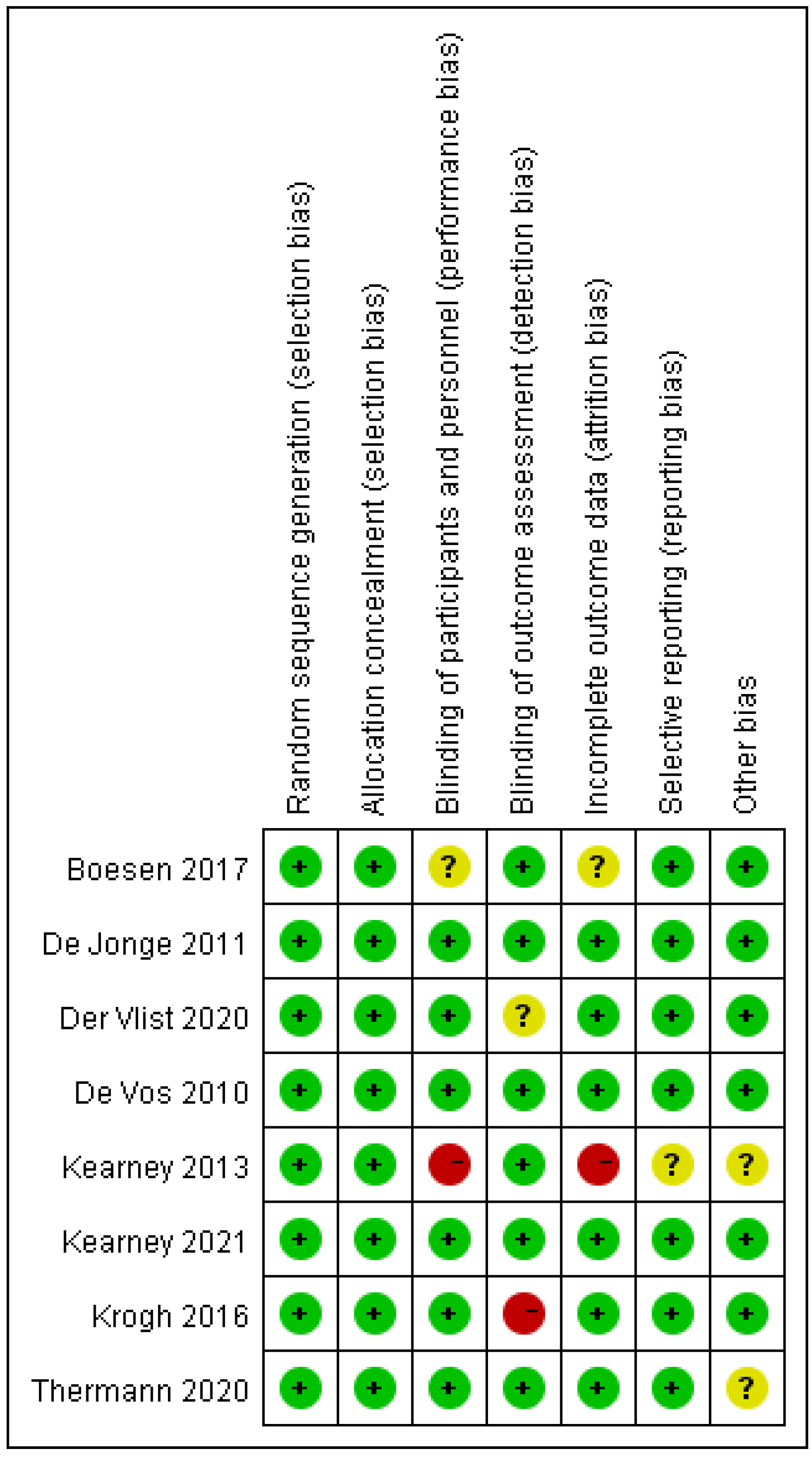
2.5. Quality Evaluation of the Included Studies
2.6. Statistical Analysis
2.7. Sensitivity Analysis
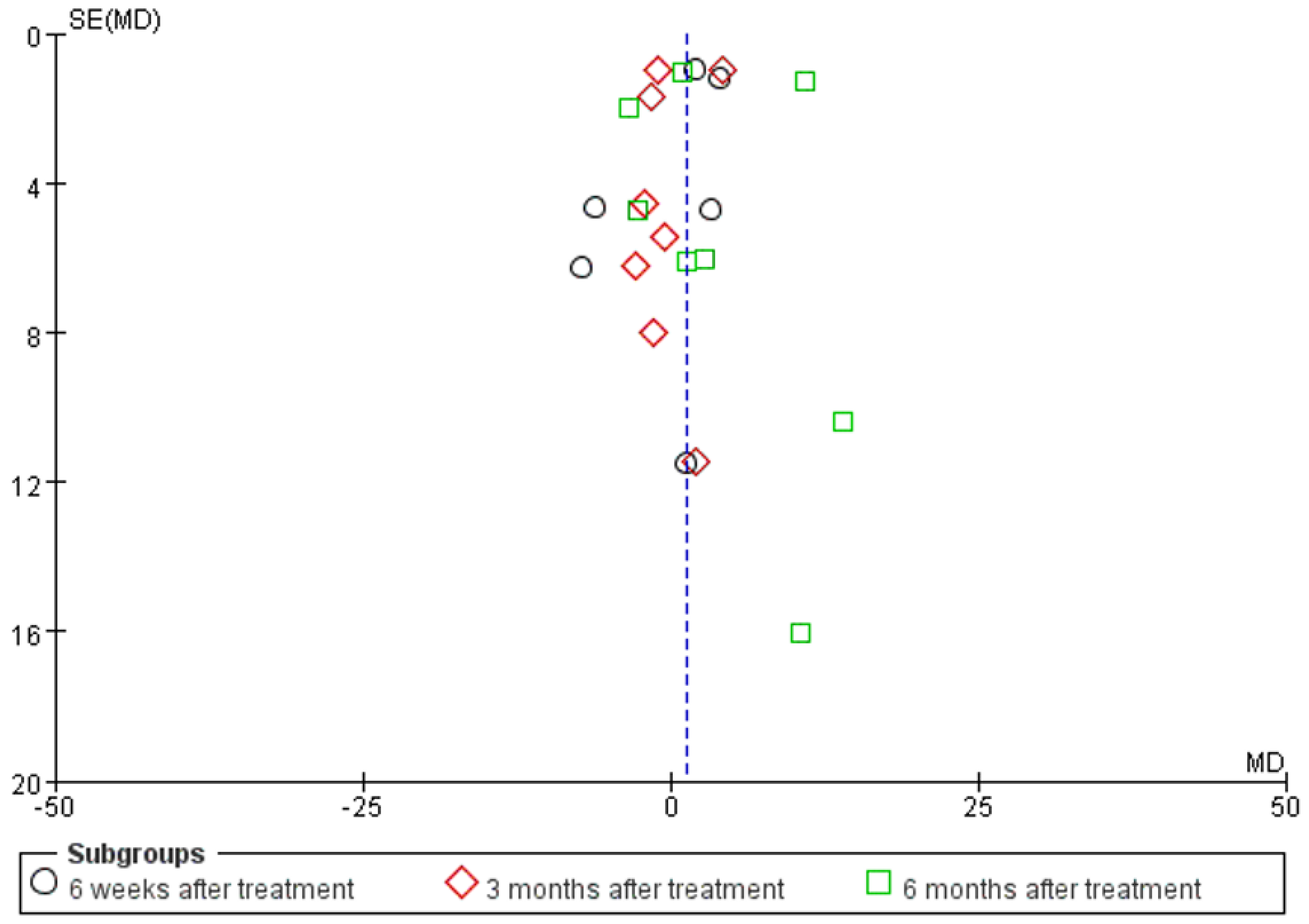
2.8. Publication Bias
3. Result
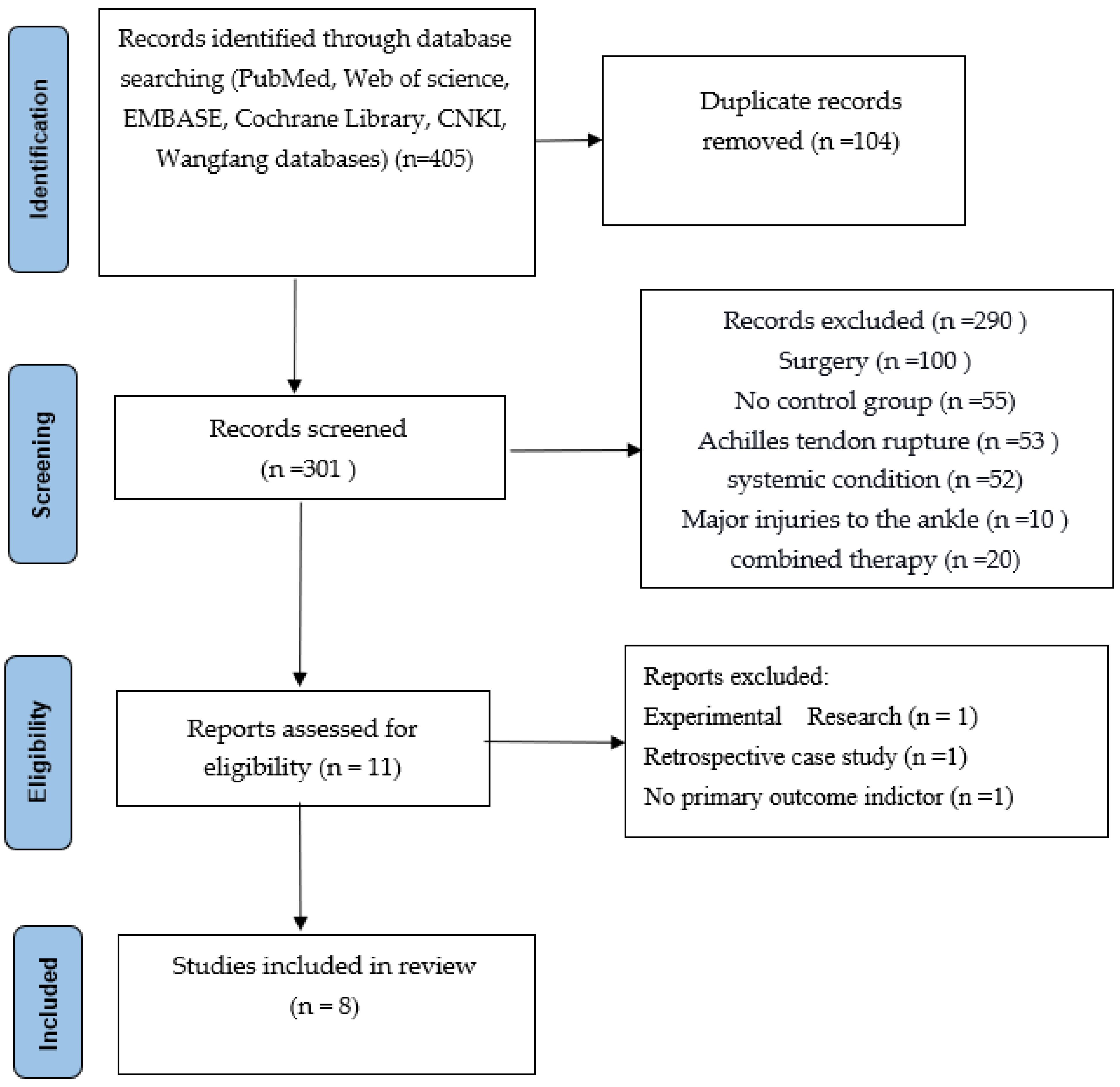
3.1. Literature Screening Results
3.2. General Information on the Included Literature
3.3. Meta-Analysis Results
3.3.1. Results of the Analysis of AT
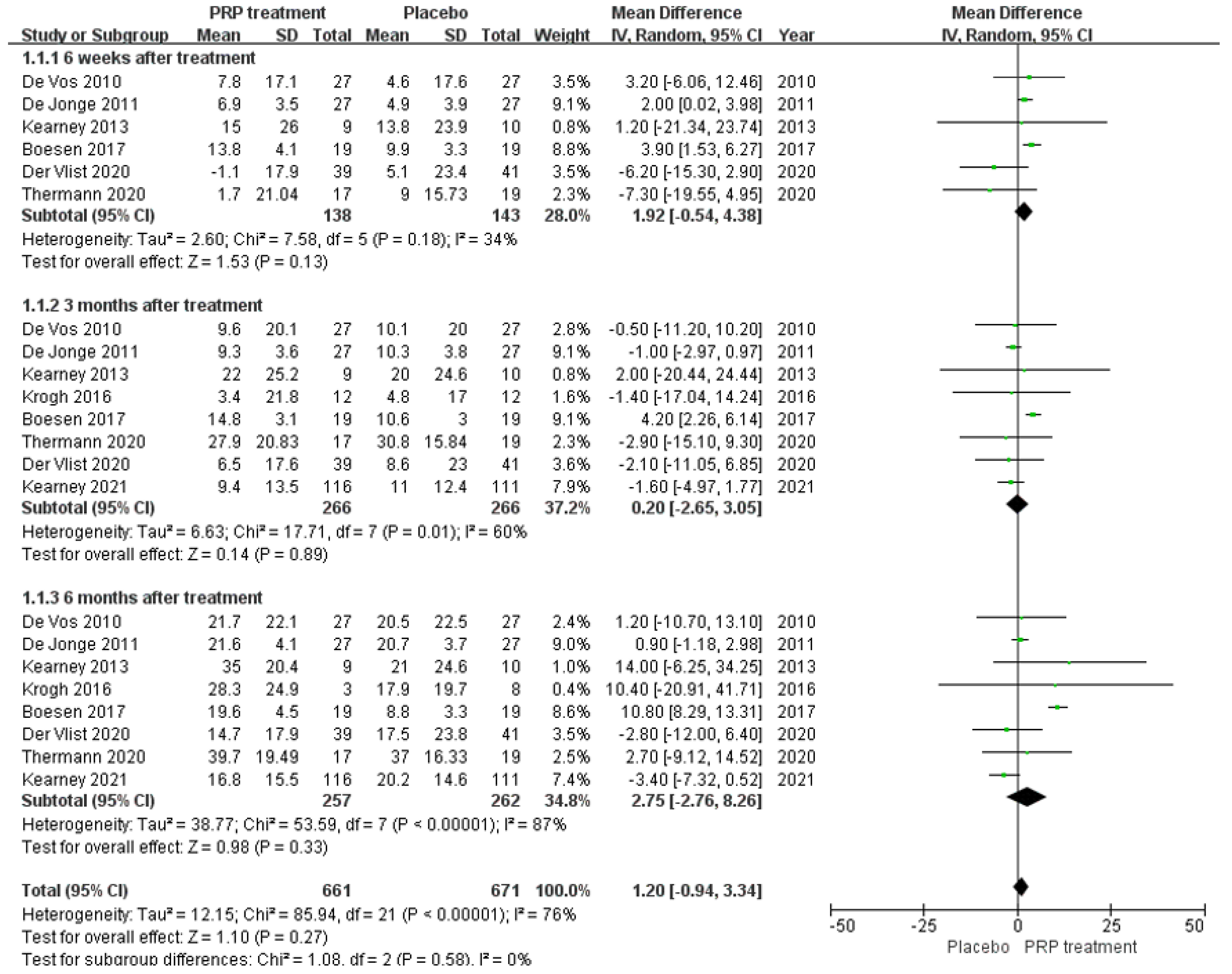
VISA–A Score Description
VISA–A Score Result
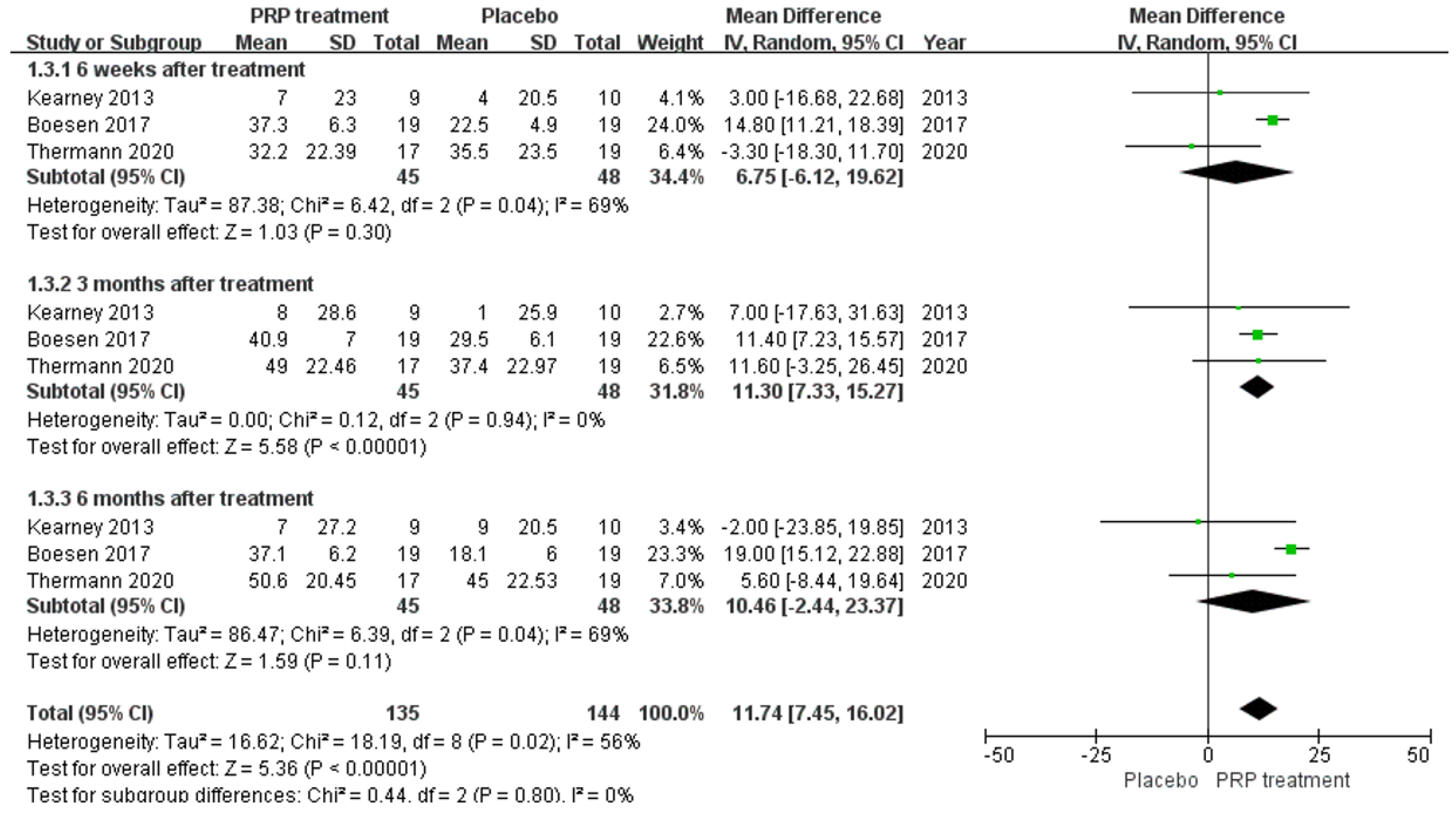
Changes in Achilles Tendon Thickness
VAS Scoring
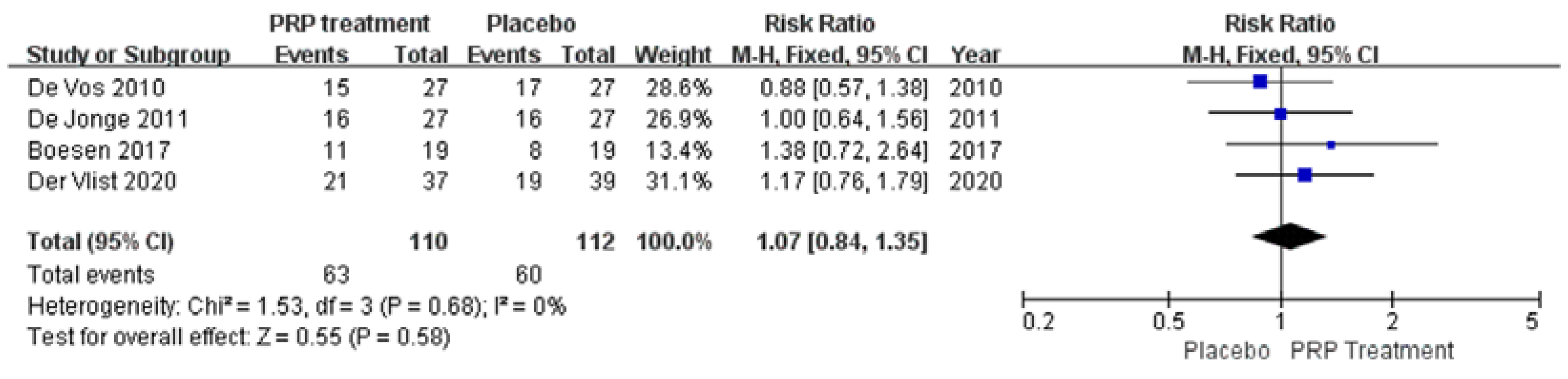
Patient Satisfaction
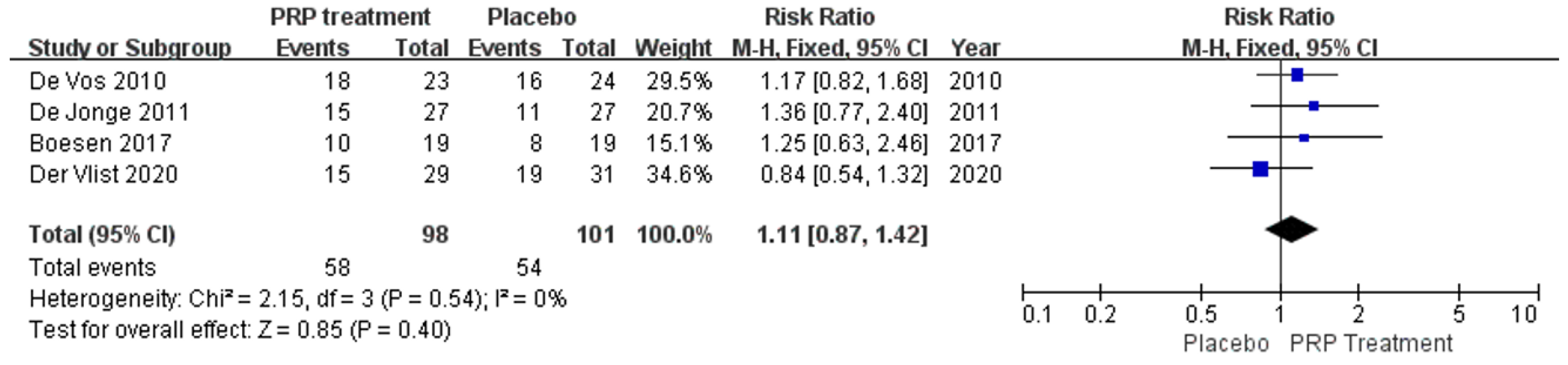
Return to Sport
4. Discussion
5. Unanswered Questions and Prospects
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Schneider, M.; Angele, P.; Järvinen, T.A.; Docheva, D. Rescue plan for Achilles: Therapeutics steering the fate and functions of stem cells in tendon wound healing. Adv. Drug Deliv. Rev. 2018, 129, 352375. [Google Scholar] [CrossRef] [PubMed]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Prim. 2017, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Mattila, V.M.; Huttunen, T.T.; Haapasalo, H.; Sillanpää, P.; Malmivaara, A.; Pihlajamäki, H. Declining incidence of surgery for Achilles tendon rupture follows publication of major RCTs: Evidence-influenced change evident using the Finnish registry study. Br. J. Sport. Med. 2015, 49, 1084–1086. [Google Scholar] [CrossRef] [PubMed]
- Van der Vlist, A.C.; Winters, M.; Weir, A.; Ardern, C.L.; Welton, N.J.; Caldwell, D.M.; Verhaar, J.A.N.; de Vos, R.J. Which treatment is most effective for patients with Achilles tendinopathy? A living systematic review with network meta-analysis of 29 randomised controlled trials. Br. J. Sport. Med. 2021, 55, 249–256. [Google Scholar] [CrossRef]
- Wetke, E.; Johannsen, F.; Langberg, H. Achilles tendinopathy: A prospective study on the effect of active rehabilitation and steroid injections in a clinical setting. Scand. J. Med. Sci. Sport. 2015, 25, e392-9. [Google Scholar] [CrossRef]
- Speed, C.A. Corticosteroid injections in tendon lesions. BMJ 2001, 323, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, P.; Aggarwal, A. Ultrasound-guided retro-calcaneal bursa corticosteroid injection for refractory Achilles tendinitis in patients with seronegative spondyloarthropathy: Effificacy and follow-up study. Rheumatol. Int. 2016, 36, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Caudell, G.M. Insertional Achilles tendinopathy. Clin. Podiatr. Med. Surg. 2017, 34, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Zellers, J.A.; Carmont, M.R.; Grävare Silbernagel, K. Return to play post-Achilles tendon rupture: A systematic review and meta-analysis of rate and measuRes. of return to play. Br. J. Sport. Med. 2016, 50, 1325–1332. [Google Scholar] [CrossRef]
- Smith, O.J.; Leigh, R.; Kanapathy, M.; Macneal, P.; Jell, G.; Hachach-Haram, N.; Mann, H.; Mosahebi, A. Fat grafting and platelet-rich plasma for the treatment of diabetic foot ulcers: A feasibility-randomised controlled trial. Int. Wound J. 2020, 17, 1578–1594. [Google Scholar] [CrossRef]
- Chen, J.; Wan, Y.; Lin, Y.; Jiang, H. Platelet-rich fibrin and concentrated growth factors as novel platelet concentrates for chronic hard-to-heal skin ulcers: A systematic review and Meta-analysis of randomized controlled trials. J. Dermatolog. Treat. 2020, 33, 613–621. [Google Scholar] [CrossRef]
- Weller, C.D.; Gardiner, E.E.; Arthur, J.F.; Southey, M.; Andrews, R.K. Autologous platelet-rich plasma for healing chronic venous leg ulcers: Clinical efficacy and potential mechanisms. Int. Wound J. 2019, 16, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.; Onishi, K.; JayarAm, P.; Lana, J.F.; Mautner, K. Platelet-rich plasma: New performance understandings and therapeutic considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.A.; van Erp, A.; DeSimone, A.; Cohen, D.S.; Gardner, R.D. Platelet rich plasma in orthopedic surgical medicine. Platelets 2021, 32, 163–174. [Google Scholar] [CrossRef]
- Harmon, K.G.; Rao, A.L. The use of platelet-rich plasma in the nonsurgical management of sports injuries: Hype or hope? Hematol. Am. Soc. Hematol. Educ. Program 2013, 2013, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P.; Calabrese, C.; De Angelis, B.; Dionisi, L.; Pizzicannella, J.; Kothari, A.; De Fazio, D.; Garcovich, S. Impact of the different preparation methods to obtain Autologous non-activated platelet-rich plasma (A-PRP) and activated platelet-rich plasma (AA-PRP) in plastic surgery: Wound healing and hair regrowth evaluation. Int. J. Mol. Sci. 2021, 21, 431. [Google Scholar] [CrossRef]
- Chamata, E.S.; Bartlett, E.L.; Weir, D.; Rohrich, R.J. Platelet-rich plasma: Evolving role in plastic surgery. Plast. Reconstr. Surg. 2021, 147, 219–230. [Google Scholar] [CrossRef]
- Ozer, K.; Colak, O. Micro-autologous fat transplantation combined with platelet-rich plasma for facial filling and regeneration: A clinical perspective in the shadow of evidence-based medicine. J. Craniofac. Surg. 2020, 30, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Fernández-de-Retana, S.; Alkhraisat, M.H. Platelet rich plasma in oral and maxillofacial surgery from the perspective of composition. Platelets 2021, 32, 174–182. [Google Scholar] [CrossRef]
- Gokçe Kutuk, S.; Gökçe, G.; Arslan, M.; Özkan, Y.; Kütük, M.; Kursat Arikan, O. Clinical and radiological comparison of effects of platelet-rich plasma, hyaluronic acid, and corticosteroid injections on temporomandibular joInt. osteoarthritis. J. Craniofac. Surg. 2019, 30, 1144–1148. [Google Scholar] [CrossRef]
- Görgü, M.; Gökkaya, A.; Karanfil, E. What should be adequate PRP dose for an effective treatment? An in-vitro experimental study on the skin. Aesthet. Surg. J. 2021, 41, NP887–NP901. [Google Scholar] [CrossRef]
- Chen, J.; Wan, Y.; Lin, Y.; Jiang, H. Current art of combination therapy with autologous platelet-rich plasma for stable vitiligo: A meta-analysis. Int. Wound J. 2020, 18, 251–260. [Google Scholar] [CrossRef]
- Lansdown, D.A.; Fortier, L.A. Platelet-rich plasma: Formulations, preparations, constituents, and their effects. Oper. Tech. Sport. Med. 2017, 25, 7–12. [Google Scholar] [CrossRef]
- Le, A.D.K.; Enweze, L.; DeBaun, M.R.; Dragoo, J.L. Current clinical recommendations for use of platelet-rich plasma. Curr. Rev. Musculoskelet. Med. 2018, 11, 624–634. [Google Scholar] [CrossRef]
- O’Connell, B.; Wragg, N.M.; Wilson, S.L. The use of PRP injections in the management of knee osteoarthritis. Cell Tissue Res. 2019, 376, 143–152. [Google Scholar] [CrossRef]
- De Vos, R.J.; Weir, A.; van Schie, H.T.; Bierma-Zeinstra, S.M.A.; Verhaar, J.A.N.; Weinans, H.; Tol, J.L. Platelet-rich plasma injection for chronic Achilles tendinopathy: A randomized controlled trial. JAMA 2010, 303, 144–149. [Google Scholar] [CrossRef]
- De Jonge, S.; de Vos, R.J.; Weir, A.; van Schie, H.T.M.; Bierma-Zeinstra, S.M.A.; Verhaar, J.A.N.; Weinans, H.; Tol, J.L. One-year follow-up of platelet-rich plasma treatment in chronic Achilles tendinopathy: A double-blind randomized placebo-controlled trial. Am. J. Sport. Med. 2011, 39, 1623–1629. [Google Scholar] [CrossRef]
- Kearney, R.S.; Parsons, N.; Costa, M.L. Achilles tendinopathy management: A pilot randomised controlled trial comparing platelet-richplasma injection with an eccentric loading programme. Bone Jt. Res. 2013, 2, 227–232. [Google Scholar] [CrossRef]
- Krogh, T.P.; Ellingsen, T.; Christensen, R.; Jensen, P.; Fredberg, U. Ultrasound-guided Injection therapy of Achilles tendinopathy with platelet-rich plasma or saline: A randomized, blinded, placebo-controlled trial. Am. J. Sport. Med. 2016, 44, 1990–1997. [Google Scholar] [CrossRef]
- Boesen, A.P.; Hansen, R.; Boesen, M.I.; Malliaras, P.; Langberg, H. Effect of high-volume injection, platelet-rich plasma, and shAm. treatment in chronic midportion Achilles tendinopathy: A randomized double-blinded prospective study. Am. J. Sport. Med. 2017, 45, 2034–2043. [Google Scholar] [CrossRef]
- Van der Vlist Arco, C.; Van Oosterom, R.F.; Van Veldhoven, P.L.J.; A Bierma-Zeinstra, S.M.; Waarsing, J.H.; Verhaar, J.A.N.; De Vos, R.-J. Effectiveness of a high volume injection as treatment for chronic Achilles tendinopathy: Randomised controlled trial. BMJ 2020, 370, m3027. [Google Scholar] [CrossRef] [PubMed]
- Thermann, H.; Fischer, R.; Gougoulias, N.; Cipollaro, L.; Maffulli, N. Endoscopic debridement for non-insertional Achilles tendinopathy with and without platelet-rich plasma. J. Sport Health Sci. 2020; in press. [Google Scholar] [CrossRef] [PubMed]
- Kearney Rebecca, S.; Costa, M.L. Effect of platelet-rich plasma injection vs shAm. injection on tendon dysfunction in patients with chronic Midportion Achilles tendinopathy: A randomized clinical trial. JAMA 2021, 326, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Yang, H.; Shen, H.; Ye, G.; Lin, X.-J. The clinical effect of tendon repair for tendon spontaneous rupture after corticosteroid injection in hands. Medicine 2016, 95, e5145. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.L.; Tsai, C.C.; Wu, S.L.; Ko, S.-Y.; Chiang, W.-F.; Yang, J.W. Effect of arthrocentesis plus plateletrich plasma and platelet-rich plasma alone in the treatment of temporomandibular joint. osteoarthritis. Medicine 2018, 97, e0477. [Google Scholar] [CrossRef]
- Murawski, C.D.; Smyth, N.A.; Newman, H.; Kennedy, J.G. A single plateletrich plasma injection for chronic midsubst. Foot Ankle Spec. 2014, 7, 372–376. [Google Scholar] [CrossRef]
- Jiang, G.; Wu, Y.; Meng, J.; Wu, F.; Li, S.; Lin, M.; Gao, X.; Hong, J.; Chen, W.; Yan, S.; et al. Comparison of leukocyte-rich platelet-rich plasma and leukocyte-poor platelet-rich plasma on Achilles tendinopathy at an early stage in a rabbit model. Am. J. Sport. Med. 2020, 48, 1189–1199. [Google Scholar] [CrossRef]
- Li, S.; Wu, Y.; Jiang, G.; Tian, X.; Hong, J.; Chen, S.; Yan, R.; Feng, G.; Cheng, Z. Intratendon delivery of leukocyte-rich platelet-rich plasma at early stage promotes tendon repair in a rabbit Achilles tendinopathy model. J. Tissue Eng. Regen. Med. 2020, 14, 452–463. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, J.; Zhang, J.; Hua, Y. Simvastatin with PRP promotes chondrogenesis of bone marrow stem cells in vitro and wounded rat Achilles tendon-bone interface healing in vivo. Am. J. Sport. Med. 2019, 47, 729–739. [Google Scholar] [CrossRef]
- Yuksel, S.; Guleç, M.A.; Gultekin, M.Z.; Adanır, O.; Caglar, A.; Beytemur, O.; Onur Küçükyıldırım, B.; Avcı, A.; Subaşı, C.; İnci, Ç.; et al. Comparison of the early period effects of bone marrow-derived mesenchymal stem cells and platelet-rich plasma on the Achilles tendon ruptures in rats. Connect. Tissue Res. 2016, 57, 360–373. [Google Scholar] [CrossRef] [PubMed]
- González, J.C.; López, C.; Álvarez, M.E.; Pérez, J.E.; Carmona, J.U. Autologous leukocyte-reduced platelet-rich plasma therapy for Achilles tendinopathy induced by collagenase in a rabbit model. Sci. Rep. 2016, 19, 19623. [Google Scholar] [CrossRef] [PubMed]
- Alsousou, J.; Thompson, M.; Harrison, P.; Willett, K.; Franklin, S. Effect of platelet-rich plasma on healing tissues in acute ruptured Achilles tendon: A human immunohistochemistry study. Lancet 2015, 385 (Suppl. S1), S19. [Google Scholar] [CrossRef]
- Boesen, A.P.; Boesen, M.I.; Hansen, R.; Barfod, K.W.; Lenskjold, A.; Malliaras, P.; Langberg, H. Effect of platelet-rich plasma on nonsurgically treated acute Achilles tendon ruptures: A randomized, double-blinded prospective study. Am. J. Sport. Med. 2020, 48, 2268–2276. [Google Scholar] [CrossRef] [PubMed]
- De Carli, A.; Lanzetti, R.M.; Ciompi, A.; Lupariello, D.; Vadalà, A.; Argento, G.; Ferretti, A.; Vulpiani, M.C.; Vetrano, M. Can platelet-rich plasma have a role in Achilles tendon surgical repair? Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2231–2237. [Google Scholar] [CrossRef] [PubMed]
- Keene, D.J.; Alsousou, J.; Harrison, P.; Hulley, P.; Wagland, S.; Parsons, S.R.; Thompson, J.Y.; O’Connor, H.M.; Schlüssel, M.M.; Dutton, S.J.; et al. Platelet rich plasma injection for acute Achilles tendon rupture: PATH-2 randomised, placebo controlled, superiority trial. BMJ 2019, 367, l6132. [Google Scholar] [CrossRef] [PubMed]
- Schepull, T.; Kvist, J.; Norrman, H.; Trinks, M.; Berlin, G.; Aspenberg, P. Autologous platelets have no effect on the healing of human achilles tendon ruptures: A randomized single-blind study. Am. J. Sport. Med. 2011, 39, 38–47. [Google Scholar] [CrossRef]
- Zou, J.; Mo, X.; Shi, Z.; Li, T.; Xue, J.; Mei, G.; Li, X. A prospective study of platelet-rich plasma as biological augmentation for acute Achilles tendon rupture repair. Biomed. Res. Int. 2016, 2016, 9364170. [Google Scholar] [CrossRef]
- Verrall, G.M.; Dolman, B.K.; Best, T.M. Applying physical science principles to mid-substance Achilles tendinopathy and the relationship to eccentric lengthening exercises. Scand. J. Med. Sci. Sport. 2018, 28, 1159–1165. [Google Scholar] [CrossRef]
- Van der Plas, A.; De Jonge, S.; De Vos, R.J.; van der Heide, H.J.; Verhaar, J.; Weir, A.; Tol, J. A 5-year follow-up study of Alfredson’s heel-drop exercise programme in chronic midportion Achilles tendinopathy. Br. J. Sport. Med. 2012, 46, 214–218. [Google Scholar] [CrossRef]
- O’Neill, S.; Watson, P.J.; Barry, S. Why are eccentric exercises effective for Achilles tendinopathy. Int. J. Sport. Phys. Ther. 2015, 10, 552–562. [Google Scholar]
- Nikolopoulos, K.I.; Pergialiotis, V.; Perrea, D.; Doumouchtsis, S. Restoration of the pubourethral ligament with platelet rich plasma for the treatment of stress urinary incontinence. Med. Hypotheses 2016, 90, 29–31. [Google Scholar] [CrossRef]
- Harrison, P.; Didembourg, M.; Wood, A.; Devi, A.; Dinsdale, R.; Hazeldine, J.; Alsousou, J.; Keene, D.J.; Hulley, P.; Wagland, S.; et al. Characteristics of L-PRP preparations for treating Achilles tendon rupture within the PATH-2 study. Platelets 2020, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.A.; Murray, I.R.; Chu, C.R.; Muschler, G.F.; Rodeo, S.A.; Piuzzi, N.S. Classification systems for platelet-rich plasma. Bone Jt. J. 2019, 101-B, 891–896. [Google Scholar] [CrossRef] [PubMed]
- DeLong, J.M.; Russell, R.P.; Mazzocca, A.D. Platelet-rich plasma: The PAW classification system. Arthroscopy 2012, 28, 9981009. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Harmon, K.; Woodall, J.; Vieira, A. Sports medicine applications of platelet-rich plasma. Curr. Pharm. Biotechnol. 2012, 13, 11851195. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009, 27, 158–167. [Google Scholar] [CrossRef]
- Magalon, J.; Chateau, A.L.; Bertrand, B.; Louis, M.L.; Silvestre, A.; Giraudo, L.; Veran, J.; Sabatier, F. DEPA classification: A proposal for standardising PRP use and a retrospective application of available devices. BMJ Open Sport Exerc. Med. 2016, 2, e000060. [Google Scholar] [CrossRef]
- Lana, J.F.S.D.; Purita, J.; Paulus, C.; Huber, S.C.; Rodrigues, B.L.; Rodrigues, A.A.; Santana, M.H.; Madureira, J.L., Jr.; Malheiros Luzo, Â.C.; Belangero, W.D.; et al. Contributions for classification of platelet-rich plasma-proposal of a new classification: MARSPILL. Regen. Med. 2017, 12, 565–574. [Google Scholar] [CrossRef]
- Mautner, K.; Malanga, G.A.; Smith, J.; Shiple, B.; Ibrahim, V.; Sampson, S.; Bowen, J.E. A call for a standard classification system, for future biologic research: The rationale for new PRP nomenclature. PM R. 2015, 74, S53–S59. [Google Scholar] [CrossRef]
- Harrison, P. Subcommittee on Platelet Physiology. The use of platelets in regenerative medicine and proposal for a new classification system: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1895–1900. [Google Scholar] [CrossRef]
- Abate, M.; Di Carlo, L.; Verna, S.; Di Gregorio, P.; Schiavone, C.; Salini, V. Synergistic activity of platelet-rich plasma and high volume image guided injection for patellar tendinopathy. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 3645–3651. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Control | SD | Sample Size (I/C) | Achilles Tendon Lesion | Location | PRP Injection Frequency/Interval/Dose (mL) | Follow-Up (wks/mos) |
|---|---|---|---|---|---|---|---|---|
| De Vos [26] | 2010 | Saline | RCT | 27/27 | C-AT (>2 mos) | Netherlands | Once/-/4 | 6. 12. 24 weeks |
| DeJonge [27] | 2011 | Saline | RCT | 27/27 | C-AT (>2 mos) | Netherlands | Once/-/4 | 6. 12. 24. 48 weeks |
| Kearney [28] | 2013 | Blank | RCT | 9/10 | C-AT (>8 mos) | UK | Once/-/3 to 5 | 6 wks. 3 mos, 6 mos |
| Krogh [29] | 2016 | Saline | RCT | 12/12 | C-AT (mean 33 mos) | Denmark | Once/-/6 | 3. 6. 12 mos |
| Boesen [30] | 2017 | Saline | RCT | 19/19 | C-AT (>3 mos) | Denmark | 4 times/2-wks/4 | 6. 12. 24 weeks |
| Van der Vlist et al. [31] | 2020 | Saline | RCT | 39/41 | C-AT (>6 mos) | Netherlands | Once/-/NR | 2. 6. 12. 24 weeks |
| Thermann [32] | 2020 | Blank | RCT | 17/19 | C-AT (>6 mos) | Italy | Once/-/NR | 6 wks. 3. 6. 12 mos |
| Kearney [33] | 2021 | Blank | RCT | 121/119 | C-AT (>3 mos) | UK | Once/-/3 | 2 wks. 3. 6 mos |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arthur Vithran, D.T.; Xie, W.; Opoku, M.; Essien, A.E.; He, M.; Li, Y. The Efficacy of Platelet-Rich Plasma Injection Therapy in the Treatment of Patients with Achilles Tendinopathy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 995. https://doi.org/10.3390/jcm12030995
Arthur Vithran DT, Xie W, Opoku M, Essien AE, He M, Li Y. The Efficacy of Platelet-Rich Plasma Injection Therapy in the Treatment of Patients with Achilles Tendinopathy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(3):995. https://doi.org/10.3390/jcm12030995
Chicago/Turabian StyleArthur Vithran, Djandan Tadum, Wenqing Xie, Michael Opoku, Anko Elijah Essien, Miao He, and Yusheng Li. 2023. "The Efficacy of Platelet-Rich Plasma Injection Therapy in the Treatment of Patients with Achilles Tendinopathy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 3: 995. https://doi.org/10.3390/jcm12030995
APA StyleArthur Vithran, D. T., Xie, W., Opoku, M., Essien, A. E., He, M., & Li, Y. (2023). The Efficacy of Platelet-Rich Plasma Injection Therapy in the Treatment of Patients with Achilles Tendinopathy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(3), 995. https://doi.org/10.3390/jcm12030995