
Effects of Mind-Body Training as a Mental Health Therapy in Adults with Diabetes Mellitus Type II: A Systematic Review


 , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Studies Selection Process
2.6. Data Extraction
2.7. Methodological Quality Assessment
3. Results
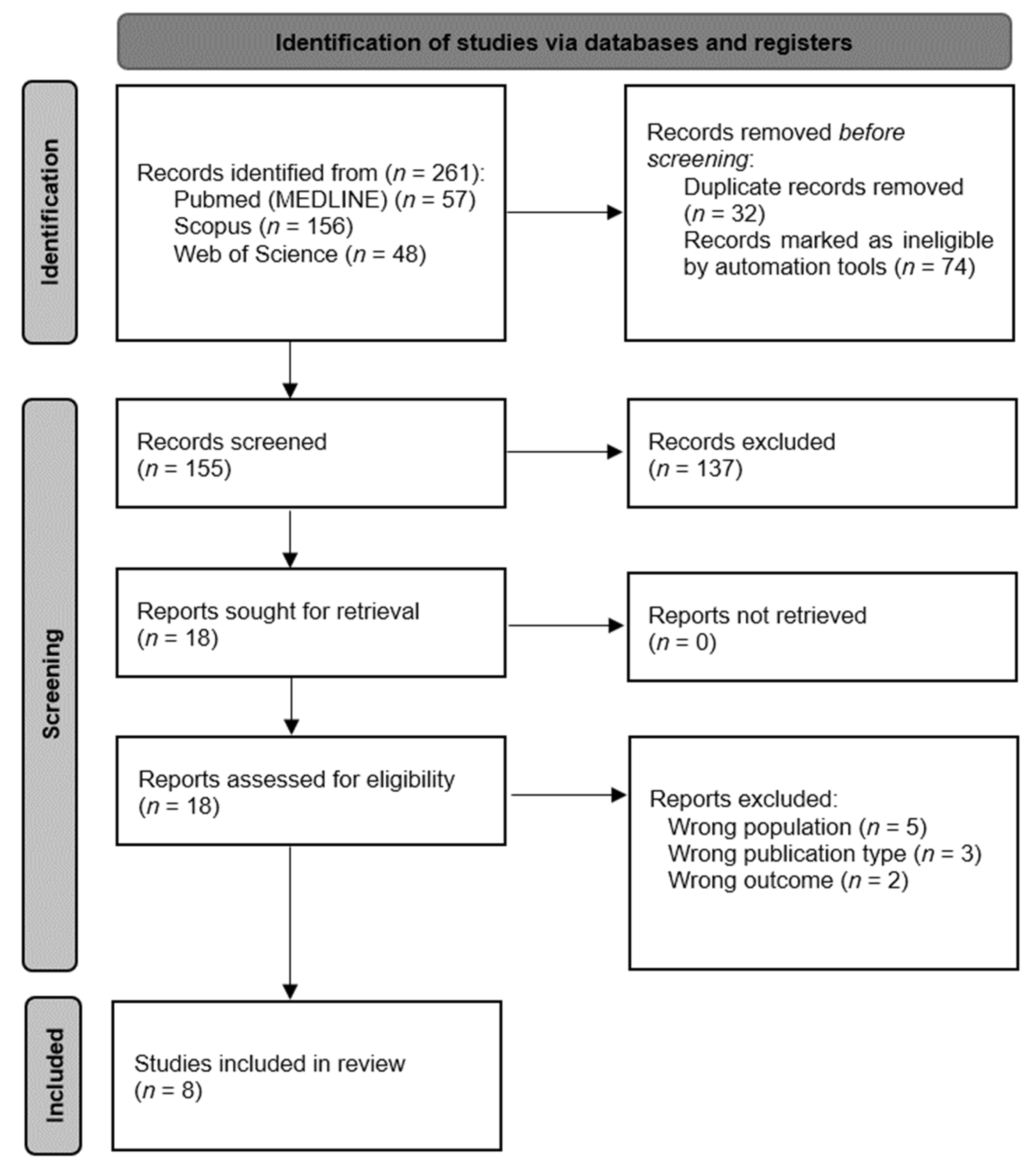
3.1. Selection of the Studies
3.2. Methodological Quality
3.3. Characteristics of the Studies
3.4. Characteristics of Study Interventions
3.5. Anxiety
3.6. Depression
3.7. Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Informe Mundial sobre la Diabetes, 2016; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Pouwer, F.; Kupper, N.; Adriaanse, M.C. Does emotional stress cause type 2 diabetes mellitus? A review from the European Depression in Diabetes (EDID) Research Consortium. Discov. Med. 2010, 9, 112–118. [Google Scholar] [PubMed]
- Roy, T.; Lloyd, C.E. Epidemiology of depression and diabetes: A systematic review. J. Affect. Disord. 2012, 142, S8–S21. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.J.; Freedland, K.E.; Clouse, R.E.; Lustman, P.J. The prevalence of comorbid depression in adults with diabetes: A meta-analysis. Diabetes Care 2001, 24, 1069–1078. [Google Scholar] [CrossRef] [PubMed]
- Vamos, E.P.; Mucsi, I.; Keszei, A.; Kopp, M.S.; Novak, M. Comorbid depression is associated with increased healthcare utilization and lost productivity in persons with diabetes: A large nationally representative Hungarian population survey. Psychosom. Med. 2009, 71, 501–507. [Google Scholar] [CrossRef]
- Kulzer, B. Depression—An important obstruction to the treatment of diabetes. MMW Fortschr. Med. 2005, 147, 37–40. [Google Scholar] [PubMed]
- Thent, Z.C.; Das, S.; Henry, L.J. Role of exercise in the management of diabetes mellitus: The global scenario. PLoS ONE 2013, 8, e80436. [Google Scholar] [CrossRef]
- León-Latre, M.; Moreno-Franco, B.; Andrés-Esteban, E.M.; Ledesma, M.; Laclaustra, M.; Alcalde, V.; Peñalvo, J.L.; Ordovás, J.M.; Casasnovas, J.A. Sedentary lifestyle and its relation to cardiovascular risk factors, insulin resistance and inflammatory profile. Rev. Esp. Cardiol. Engl. Ed. 2014, 67, 449–455. [Google Scholar] [CrossRef]
- Parra-Sánchez, J.; Moreno-Jiménez, M.; Nicola, C.M.; Nocua, R., II; Amegló-Parejo, M.R.; Del Carmen-Peña, M.; Cordero-Prieto, C.; Gajardo-Barrena, M.J. Evaluation of a supervised physical exercise program in sedentary patients over 65 years with type 2 diabetes mellitus. Aten. Primaria 2015, 47, 555–562. [Google Scholar] [CrossRef]
- Guerra Santiesteban, J.R.; Gutiérrez Cruz, M.; Zavala Plaza, M.; Singre Álvarez, J.; Goosdenovich Campoverde, D.; Romero Frómeta, E. Relación entre ansiedad y ejercicio físico. Rev. Cuba. Investig. Bioméd. 2017, 36, 169–177. [Google Scholar]
- Iglesias Martínez, B.; Olaya Velázquez, I.; Gómez Castro, M.J. Prevalence of performing and prescribing physical exercise in patients diagnosed with anxiety and depression. Aten. Primaria 2015, 47, 428–437. [Google Scholar] [CrossRef]
- Hernández Rodríguez, J.; Licea Puig, M.E. Papel del ejercicio físico en las personas con diabetes mellitus. Rev. Cuba. Endocrinol. 2010, 21, 182–201. [Google Scholar]
- Tang, Y.Y. Mechanism of integrative body-mind training. Neurosci. Bull. 2011, 27, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Lee, W.J.; Choi, S.H.; Jang, J.H.; Kang, D.H. Long-term beneficial effects of an online mind-body training program on stress and psychological outcomes in female healthcare providers: A non-randomized controlled study. Medicine 2020, 99, e21027. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Jagannathan, A.; Philip, M.; Thulasi, A.; Angadi, P.; Raghuram, N. Role of yoga for patients with type II diabetes mellitus: A systematic review and meta-analysis. Complement. Ther. Med. 2016, 25, 104–112. [Google Scholar] [CrossRef]
- Chen, Z.; Ye, X.; Xia, Y.; Song, H.; Wang, Y.; Guan, Y.; Shen, Z.; Chen, W.; Jiang, T.; Wu, H.; et al. Effect of Pilates on Glucose and Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Physiol. 2021, 12, 641968. [Google Scholar] [CrossRef]
- Wang, J.H. Effects of Tai Chi exercise on patients with type 2 diabetes. Med. Sport Sci. 2008, 52, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ Clin. Res. Ed. 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Albanese, E.; Bütikofer, L.; Armijo-Olivo, S.; Ha, C.; Egger, M. Construct validity of the Physiotherapy Evidence Database (PEDro) quality scale for randomized trials: Item response theory and factor analyses. Res. Synth. Methods 2020, 11, 227–236. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, M.; Kopf, S.; Kircher, C.; Faude-Lang, V.; Djuric, Z.; Augstein, F.; Friederich, H.C.; Kieser, M.; Bierhaus, A.; Humpert, P.M.; et al. Sustained effects of a mindfulness-based stress-reduction intervention in type 2 diabetic patients: Design and first results of a randomized controlled trial (the Heidelberger Diabetes and Stress-study). Diabetes Care 2012, 35, 945–947. [Google Scholar] [CrossRef] [PubMed]
- Koloverou, E.; Tentolouris, N.; Bakoula, C.; Darviri, C.; Chrousos, G. Implementation of a stress management program in outpatients with type 2 diabetes mellitus: A randomized controlled trial. Hormones 2014, 13, 509–518. [Google Scholar] [CrossRef]
- Chen, S.M.; Lin, H.S.; Atherton, J.J.; MacIsaac, R.J.; Wu, C.J. Effect of a mindfulness programme for long-term care residents with type 2 diabetes: A cluster randomised controlled trial measuring outcomes of glycaemic control, relocation stress and depression. Int. J. Older People Nurs. 2020, 15, e12312. [Google Scholar] [CrossRef] [PubMed]
- Sarika, K.S.; Kumar, H.; Balakrishnan, V.; Sundaram, K.R. Impact of Integrated Amrita Meditation® technique on stress in type 2 diabetic patients. Indian J. Med. Res. 2020, 152, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.P.; Khandelwal, B. Effect of Yoga and Exercise on Glycemic Control and Psychosocial Parameters in Type 2 Diabetes Mellitus: A Randomized Controlled Study. Int. J. Yoga 2020, 13, 144–151. [Google Scholar] [CrossRef]
- Nikkhah Ravari, O.; Mousavi, S.Z.; Babak, A. Evaluation of the Effects of 12 Weeks Mindfulness-Based Stress Reduction on Glycemic Control and Mental Health Indices in Women with Diabetes Mellitus Type 2. Adv. Biomed. Res. 2020, 9, 61. [Google Scholar] [CrossRef]
- Chen, Q.; Yang, G.; Lin, S.; Li, M.; Liu, Z.; Fu, Y.; Chen, Y. The effects of mindfulness-based stress reduction therapy combined with intensive education on the effectiveness of the care and the awareness rate in patients with arthritis and diabetes. Am. J. Transl. Res. 2021, 13, 3190–3197. [Google Scholar]
- Yadav, A.; Kaushik, R.M.; Kaushik, R. Effects of Diaphragmatic Breathing and Systematic Relaxation on Depression, Anxiety, Stress, and Glycemic Control in Type 2 Diabetes Mellitus. Int. J. Yoga Ther. 2021, 31, 13. [Google Scholar] [CrossRef]
- Li, Z.; Liu, S.; Wang, L.; Smith, L. Mind-Body Exercise for Anxiety and Depression in COPD Patients: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 17, 22. [Google Scholar] [CrossRef]
- Wang, X.; Li, P.; Pan, C.; Dai, L.; Wu, Y.; Deng, Y. The Effect of Mind-Body Therapies on Insomnia: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. Ecam 2019, 2019, 9359807. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Crawford, C.; Hickey, A. Mind-body therapies for the self-management of chronic pain symptoms. Pain Med. Malden Mass. 2014, 15 (Suppl. S1), S21–S39. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Liu, J.; Chen, X.; Xia, R.; Li, M.; Huang, M.; Li, S.; Park, J.; Wilson, G.; Lang, C.; et al. Mind-body exercise improves cognitive function and modulates the function and structure of the hippocampus and anterior cingulate cortex in patients with mild cognitive impairment. NeuroImage Clin. 2019, 23, 101834. [Google Scholar] [CrossRef]
- Toussaint, L.L.; Whipple, M.O.; Abboud, L.L.; Vincent, A.; Wahner-Roedler, D.L. A mind-body technique for symptoms related to fibromyalgia and chronic fatigue. Explore 2012, 8, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Thind, H.; Lantini, R.; Balletto, B.L.; Donahue, M.L.; Salmoirago-Blotcher, E.; Bock, B.C.; Scott-Sheldon, L.A.J. The effects of yoga among adults with type 2 diabetes: A systematic review and meta-analysis. Prev. Med. 2017, 105, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.X.; Ma, L.; Li, J.P. Effects of mindfulness-based intervention on glycemic control and psychological outcomes in people with diabetes: A systematic review and meta-analysis. J. Diabetes Investig. 2021, 12, 1092–1103. [Google Scholar] [CrossRef]
- Savović, J.; Jones, H.E.; Altman, D.G.; Harris, R.J.; Jüni, P.; Pildal, J.; Als-Nielsen, B.; Balk, E.M.; Gluud, C.; Gluud, L.L.; et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann. Intern. Med. 2012, 157, 429–438. [Google Scholar] [CrossRef]
- Streeter, C.C.; Whitfield, T.H.; Owen, L.; Rein, T.; Karri, S.K.; Yakhkind, A.; Perlmutter, R.; Prescot, A.; Renshaw, P.F.; Ciraulo, D.A.; et al. Effects of yoga versus walking on mood, anxiety, and brain GABA levels: A randomized controlled MRS study. J. Altern. Complement. Med. 2010, 16, 1145–1152. [Google Scholar] [CrossRef]
- Lozano Montes, L.; Balakrishnan, V.; Gopalakrishnan, S. Effects of Integrated Amrita Meditation Technique on Anxiety, Depression, and Plasma Neurotransmitters on a Healthy Population: A Randomized Controlled Trial Followed by a Case-Control Study. J. Altern. Complement. Med. 2021, 27, 641–648. [Google Scholar] [CrossRef]
- Savage, K.; Firth, J.; Stough, C.; Sarris, J. GABA-modulating phytomedicines for anxiety: A systematic review of preclinical and clinical evidence. Phytother. Res. PTR 2018, 32, 3–18. [Google Scholar] [CrossRef]
- Bagchi, B.; Wenger, M. Electrophysiological correlates of some yogi exercises. Electroencephalogr. Clin. Neurophysiol. 1957, 7, 132–149. [Google Scholar]
- Fell, J.; Axmacher, N.; Haupt, S. From alpha to gamma: Electrophysiological correlates of meditation-related states of consciousness. Med. Hypotheses 2010, 75, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Das, S.; Mondal, S.; Goswami, U.; Gandhi, A. Effect of Sahaj Yoga on neuro-cognitive functions in patients suffering from major depression. Indian J. Physiol. Pharmacol. 2006, 50, 375. [Google Scholar]
- Pascoe, M.C.; Thompson, D.R.; Ski, C.F. Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology 2017, 86, 152–168. [Google Scholar] [CrossRef]
- Carter, S.; Greenberg, J.; Funes, C.J.; Macklin, E.A.; Vranceanu, A.M. Effects of a mind-body program on symptoms of depression and perceived stress among adults with neurofibromatosis type 2 who are deaf: A live-video randomized controlled trial. Complement. Ther. Med. 2021, 56, 102581. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, R.; Šumec, R.; Vyhnálek, M.; Bendíčková, K.; Lázničková, P.; Forte, G.; Jeleník, A.; Římalová, V.; Frič, J.; Hort, J.; et al. The Effect of Mindfulness-Based Stress Reduction (MBSR) on Depression, Cognition, and Immunity in Mild Cognitive Impairment: A Pilot Feasibility Study. Clin. Interv. Aging 2020, 15, 1365–1381. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Zhang, X.; Liu, N.; Wang, J.; Chen, D.; Sun, W.; Li, P.; Zhang, W. Mind-body interventions on stress management in pregnant women: A systematic review and meta-analysis of randomized controlled trials. J. Adv. Nurs. 2021, 77, 125–146. [Google Scholar] [CrossRef]
- Graubard, R.; Perez-Sanchez, A.; Katta, R. Stress and Skin: An Overview of Mind Body Therapies as a Treatment Strategy in Dermatology. Dermatol. Pract. Concept. 2021, 11, e2021091. [Google Scholar] [CrossRef]
- McEwen, B.S. Protective and damaging effects of stress mediators: Central role of the brain. Dialogues Clin. Neurosci. 2006, 8, 367–381. [Google Scholar] [CrossRef]
- Weck, F.; Richtberg, S.; Esch, S.; Höfling, V.; Stangier, U. The relationship between therapist competence and homework compliance in maintenance cognitive therapy for recurrent depression: Secondary analysis of a randomized trial. Behav. Ther. 2013, 44, 162–172. [Google Scholar] [CrossRef]
- Helbig, S.; Fehm, L. Problems with homework in CBT: Rare exception or rather frequent? Behav. Cogn. Psychother. 2004, 32, 291–301. [Google Scholar] [CrossRef]
- Parsons, C.E.; Crane, C.; Parsons, L.J.; Fjorback, L.O.; Kuyken, W. Home practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behav. Res. Ther. 2017, 95, 29–41. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hartmann et al. 2012 [25] | Y | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| Koloverou et al. 2014 [26] | Y | Y | N | Y | N | N | Y | Y | N | Y | Y | 6 |
| Chen et al. 2020 [27] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 7 |
| Sarika et al. 2020 [28] | N | Y | N | N | N | N | N | Y | N | Y | Y | 4 |
| Singh & Khandelwal 2020 [29] | N | Y | Y | Y | N | N | N | Y | N | Y | Y | 6 |
| Ravari et al. 2020 [30] | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | 6 |
| Chen et al. 2021 [31] | Y | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| Yadav 2021 [32] | Y | Y | Y | Y | N | N | N | Y | N | Y | Y | 6 |
| Author and Year | Country | Sample CG/IG | Control Group | Intervention Group | |||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Intervention Type | Intervention Characteristics | Instruments and Variables Baseline Measures | Modifications over Time | |||||
| Hartmann et al. 2012 [25] | Germany | 57/53 | Usual care | CG: 59.30 ± 7.80 IG: 58.70 ± 7.40 | Mindfulness-Based Stress-Reduction | Frequency: 1 session/week. Volume: 2 h. Duration: 8 weeks. Measurement points: Baseline, 8 weeks and 1 year. | PHQ Depression 6.40 ± 4.90 Stress 6.40 ± 3.60 | 8 weeks Depression 5.70 ± 0.53 Stress 4.90 ± 0.47 | 1 Year Depression 5.30 ± 0.48 * Stress 5.00 ± 0.42 |
| Koloverou et al. 2014 [26] | Greece | 28/25 | Usual care | CG: 63.00 ± 8.00 IG: 60.52 ± 6.73 | Relaxation breathing + progressive muscle relaxation Yoga-Based | Frequency: 2 sessions/day. Volume: 25 min. Duration: 8 weeks. Measurement points: Baseline and 8 weeks. | PSS 27.21 ± 8.02 | 8 weeks −2.6 ±1.10 * | - |
| Chen et al. 2020 [27] | Taiwan | 60/60 | Usual care | CG: 78.95 ± 7.12 IG: 78.85 ± 7.62 | Mindfulness program | Frequency: 1 session/week. Volume: 1.5 h. Duration: 9 weeks. Measurement points: Baseline, 6 weeks and 9 weeks. | DASS-21 Depression 44.20 ± 16.57 RSS Relocated Stress 80.17 ± 12.77 | 6 weeks Depression 30.20 ± 11.89 Relocated Stress 67.91 ± 12.82 | 9 weeks Depression 23.17 ± 5.35 * Relocated Stress 54.85 ± 11.91 * |
| Sarika et al. 2020 [28] | India | 15/15 | Instructions on dietary modifications, exercises, and psychological counselling | CG: 48.53 ± 8.95 IG: 54.87 ± 10.27 | Combination of yoga, pranayama, and meditation. | Frequency: 1 session/day, minimum 4 times per week. Volume: 28 min. Duration: 3 months. Measurement points: Baseline and 3 months. | PSS 21.13 ± 3.71 | 3 months 16.80 ± 3.34 * | - |
| Singh & Khandelwal 2020 [29] | India | 115/112 | General instruction booklet: diet prescription and general information of standard care. | CG:49.40 ± 8.70 IG: 50.30 ± 9.10 | Yoga | Frequency: 1 session/day. Volume: Progressive increase in the duration of the different prescribed exercises, the full duration of the session is not specified. Duration: 3 months. Measurement points: Baseline and 3 months. | SSAI 37.5 ± 6.7 STAI 32.4 ± 6.5 total anxiety 69.9 ± 8.2 BDI 23.2 ± 4.3 | 3 months: SSAI 28.9 ± 10.2 * STAI 23.7 ± 6.0 * total anxiety 52.7 ± 12.1 * BDI 20.8 ± 3.2 * | - |
| Ravari et al. 2020 [30] | Iran | 51/50 | Routine care | CG:57.70 ± 5.65 IG: 56.40 ± 4.57 | Mindfulness-based stress reduction | Frequency: 1 session/week. Volume: 2 h. Duration: 12 weeks. Measurement points: Baseline and 12 weeks. | DASS-21 Depression 17.15 ± 6.94 Anxiety 17.15 ± 7.33 Stress score 21.11 ± 8.23 | 12 weeks Depression 13.69 ± 8.07 * Anxiety 13.09 ± 7.67 * Stress score 17.36 ± 8.51 * | - |
| Chen et al. 2021 [31] | China | 47/47 | 8-week-long intensive education program | CG:64.11 ± 4.36 IG: 63.98 ± 4.34 | Mindfulness-based stress reduction + yoga | Frequency: 1 session/week Volume: not specified. Duration: 8 weeks. Measurement points: Baseline and 8 weeks. | SCL-90 Anxiety 1.94 ± 0.26 Depression 1.91 ± 0.25 | 8 weeks Anxiety 0.72 ± 0.17 * Depression 0.90 ± 0.21 * | - |
| Yadav 2021 [32] | India | 50/50 | Conventional treatment: Dietary and physical exercise counseling, oral hypoglycemic agents, and/or insulin as per their symptomatology | CG: 56.40 ± 11.72 IG: 52.24 ± 10.36 | Deep breathing and Systematic Relaxation Yoga-Based + conventional treatment | Frequency: 1 session/week. Volume: 1 h. Duration: 6 months. Measurement points: Baseline and 6 months. | DASS-21 Depression 4.22 ± 2.49 Anxiety 6.90 ± 3.00 Stress 7.32 ± 2.59 | 6 Months Depression 3.24 ± 2.09 * Anxiety 5.79 ± 2.42 * Stress 6.01 ± 1.94 * | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Ariza, B.; Hita-Contreras, F.; Rodríguez-López, C.; Rivas-Campo, Y.; Aibar-Almazán, A.; Carcelén-Fraile, M.d.C.; Castellote-Caballero, Y.; Afanador-Restrepo, D.F. Effects of Mind-Body Training as a Mental Health Therapy in Adults with Diabetes Mellitus Type II: A Systematic Review. J. Clin. Med. 2023, 12, 853. https://doi.org/10.3390/jcm12030853
Ruiz-Ariza B, Hita-Contreras F, Rodríguez-López C, Rivas-Campo Y, Aibar-Almazán A, Carcelén-Fraile MdC, Castellote-Caballero Y, Afanador-Restrepo DF. Effects of Mind-Body Training as a Mental Health Therapy in Adults with Diabetes Mellitus Type II: A Systematic Review. Journal of Clinical Medicine. 2023; 12(3):853. https://doi.org/10.3390/jcm12030853
Chicago/Turabian StyleRuiz-Ariza, Beatriz, Fidel Hita-Contreras, Carlos Rodríguez-López, Yulieth Rivas-Campo, Agustín Aibar-Almazán, María del Carmen Carcelén-Fraile, Yolanda Castellote-Caballero, and Diego Fernando Afanador-Restrepo. 2023. "Effects of Mind-Body Training as a Mental Health Therapy in Adults with Diabetes Mellitus Type II: A Systematic Review" Journal of Clinical Medicine 12, no. 3: 853. https://doi.org/10.3390/jcm12030853
APA StyleRuiz-Ariza, B., Hita-Contreras, F., Rodríguez-López, C., Rivas-Campo, Y., Aibar-Almazán, A., Carcelén-Fraile, M. d. C., Castellote-Caballero, Y., & Afanador-Restrepo, D. F. (2023). Effects of Mind-Body Training as a Mental Health Therapy in Adults with Diabetes Mellitus Type II: A Systematic Review. Journal of Clinical Medicine, 12(3), 853. https://doi.org/10.3390/jcm12030853