
Acute Modification of Hemodynamic Forces in Patients with Severe Aortic Stenosis after Transcatheter Aortic Valve Implantation
 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Amplitude Parameters
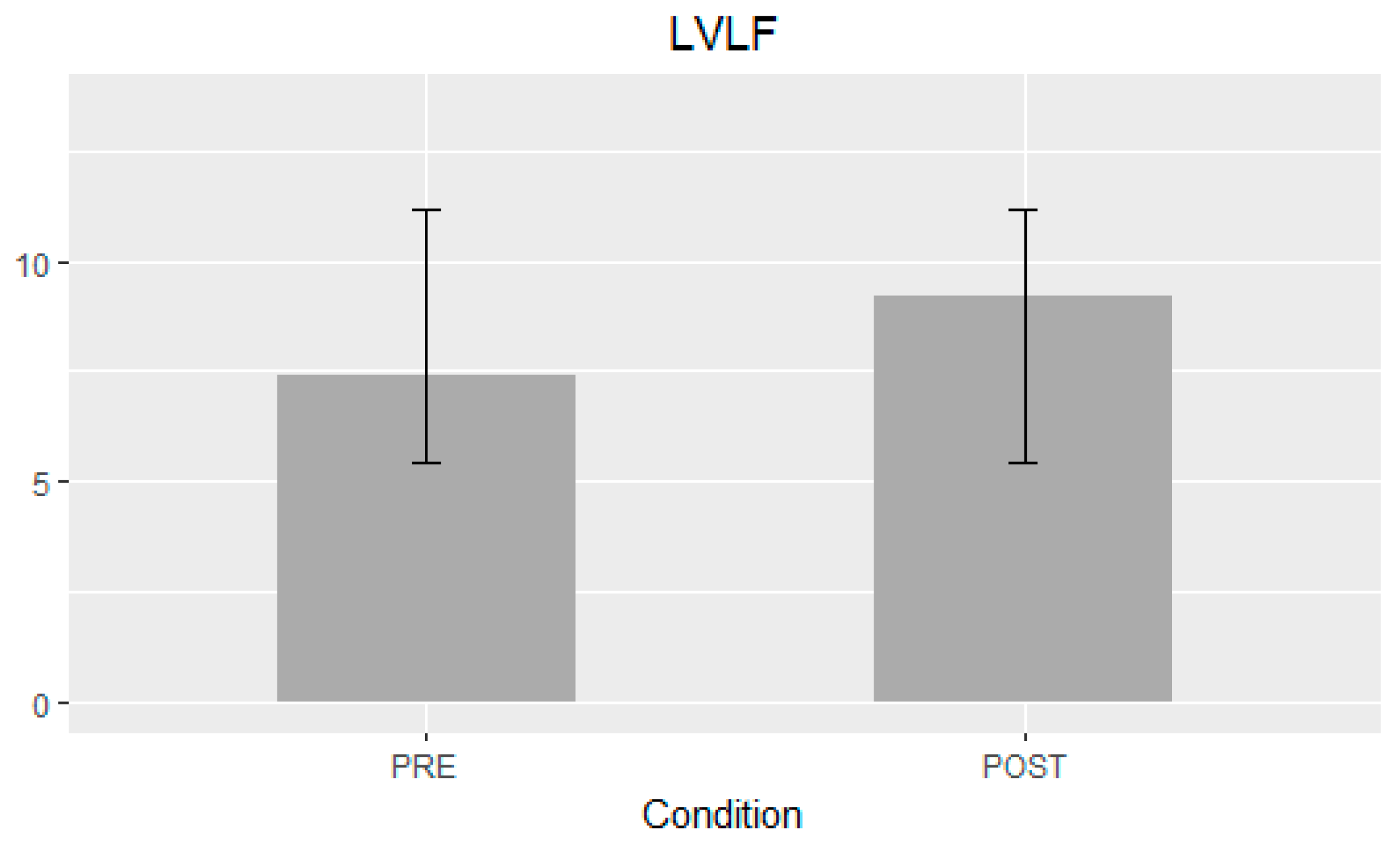
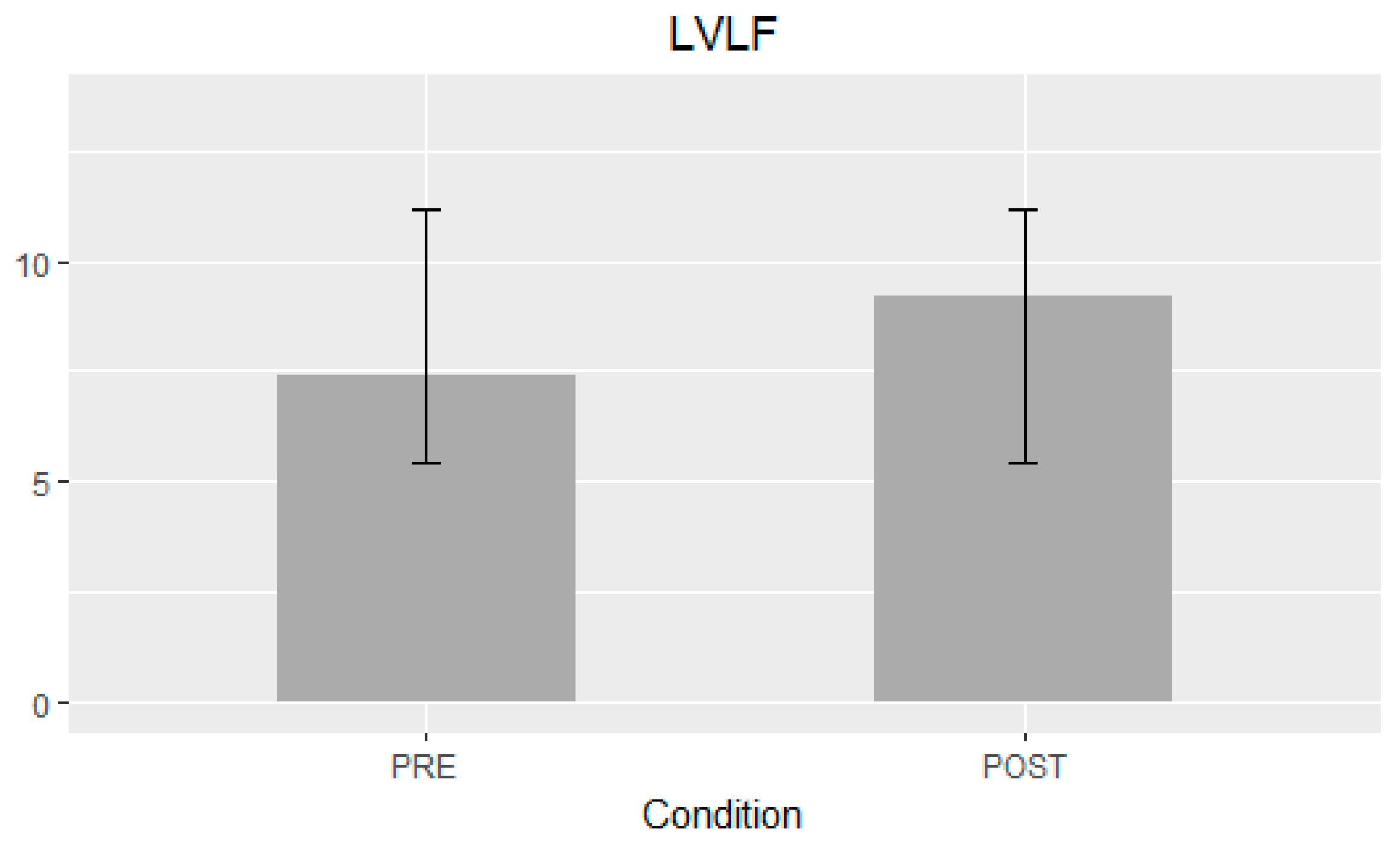
- LV longitudinal force (LVLF) as the mean amplitude of the longitudinal force throughout the cardiac cycle; since it includes both positive and negative values, the amplitude was computed as the root mean square of all values.
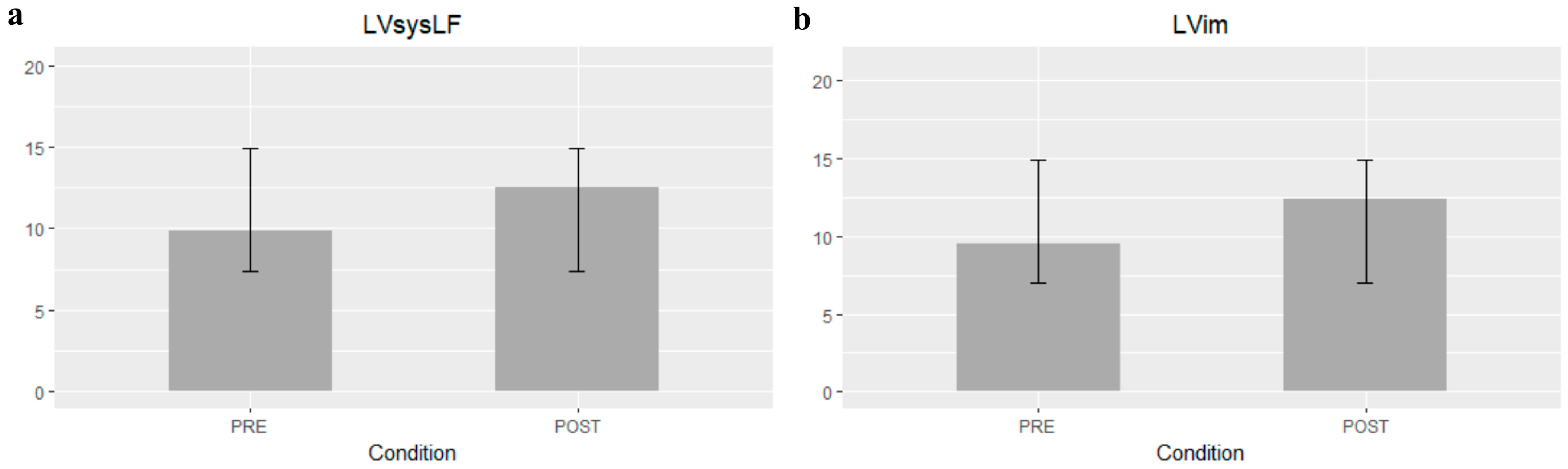
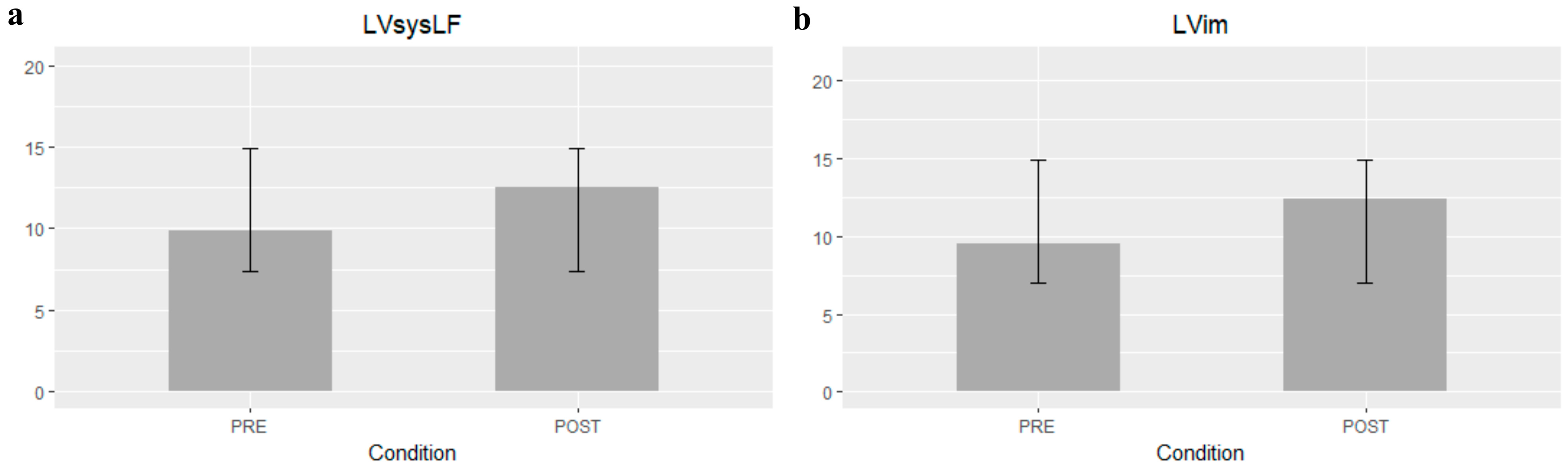
- LV systolic longitudinal force (LVsysLF), calculated as for the LVLF above, but limited to the systolic phase only.
- LV impulse (LVim) as the mean longitudinal force during the systolic propulsive phase, when the force is positive (directed from the LV cavity toward the aorta); it is the area under the curve of the positive force profile during systole, normalized by the corresponding time interval [19].
- LV suction (LVs) as the mean longitudinal force during the period following propulsion while the force is negative, which is computed as the LVim but in the period comprising the end of the systole (when the force decelerates the exiting flow, with the aorta open and the mitral valve closed) and the initial part of the diastole (the effective suction when the mitral inflow accelerates, with the aorta closed and the mitral valve open).
2.2. Timing Parameters
- Time from R-wave to positive peak of systolic LV longitudinal force, including the rates of force generation and force decay (RtoPeak).
- Duration of LV negative longitudinal force in the transition from systole to diastole.
- Time from the start of relaxation to positive peak of diastolic LV longitudinal force.
2.3. Orientation Parameters
- Ratio between the transverse force and the longitudinal force (TF/TL).
- Dominant angle of the force vector, ranging from 90° (when the force is perfectly parallel to the base-apex axis) to 0°.
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circ. Circ. 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; Lefevre, M.; Miller, F.; Otto, C.M. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef] [PubMed]
- Pawade, T.; Clavel, M.-A.; Tribouilloy, C.; Dreyfus, J.; Mathieu, T.; Tastet, L.; Renard, C.; Gun, M.; Jenkins, W.S.A.; Macron, L.; et al. Computed Tomography Aortic Valve Calcium Scoring in Patients with Aortic Stenosis. Circ. Cardiovasc. Imaging 2018, 11, e007146. [Google Scholar] [CrossRef] [PubMed]
- Clavel, M.A.; Pibarot, P.; Messika-Zeitoun, D.; Capoulade, R.; Malouf, J.; Aggarval, S.; Araoz, P.A.; Michelena, H.I.; Cueff, C.; Larose, E.; et al. Impact of aortic valve calcification, as measured by MDCT, on survival in patients with aortic stenosis: Results of an international registry study. J. Am. Coll. Cardiol. 2014, 64, 1202–1213. [Google Scholar] [CrossRef]
- Cueff, C.; Serfaty, J.-M.; Cimadevilla, C.; Laissy, J.-P.; Himbert, D.; Tubach, F.; Duval, X.; Iung, B.; Enriquez-Sarano, M.; Vahanian, A.; et al. Measurement of aortic valve calcification using multislice computed tomography: Correlation with haemodynamic severity of aortic stenosis and clinical implication for patients with low ejection fraction. Heart 2011, 97, 721–726. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart disease Developed by the Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. Oxf. Acad. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef]
- Deeb, G.M.; Reardon, M.J.; Chetcuti, S.; Patel, H.J.; Grossman, P.M.; Yakubov, S.J.; Kleiman, N.S.; Coselli, J.S.; Gleason, T.G.; Lee, J.S.; et al. 3-Year Outcomes in High-Risk Patients Who Underwent Surgical or Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 67, 2565–2574. [Google Scholar] [CrossRef]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Smith, C.R.; Miller, D.C.; Moses, J.W.; Tuzcu, E.M.; Webb, J.G.; Douglas, P.S.; Anderson, W.N.; Blackstone, E.H.; et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2477–2484. [Google Scholar] [CrossRef]
- Adams, D.H.; Popma, J.J.; Reardon, M.J.; Yakubov, S.J.; Coselli, J.S.; Deeb, G.M.; Gleason, T.G.; Buchbinder, M.; Hermiller, J., Jr.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis. N. Engl. J. Med. 2014, 370, 1790–1798. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Siontis, G.C.M.; Overtchouk, P.; Cahill, T.J.; Modine, T.; Prendergast, B.; Praz, F.; Pilgrim, T.; Petrinic, T.; Nikolakopoulou, A.; Salanti, G.; et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: An updated meta-analysis. Eur. Heart J. 2019, 40, 3143–3153. [Google Scholar] [CrossRef] [PubMed]
- Vallelonga, F.; Airale, L.; Tonti, G.; Argulian, E.; Milan, A.; Narula, J.; Pedrizzetti, G. Introduction to Hemodynamic Forces Analysis: Moving Into the New Frontier of Cardiac Deformation Analysis. J. Am. Heart Assoc. 2021, 10, e023417. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Pedrizzetti, G. On the computation of hemodynamic forces in the heart chambers. J. Biomech. 2019, 95, 109323. [Google Scholar] [CrossRef]
- Rushmer, R.F. Initial Ventricular Impulse. A Potential Key to Cardiac Evaluation. Circ. Circ. 1964, 29, 268–283. [Google Scholar] [CrossRef]
- Faganello, G.; Collia, D.; Furlotti, S.; Pagura, L.; Zaccari, M.; Pedrizzetti, G.; Di Lenarda, A. A new integrated approach to cardiac mechanics: Reference values for normal left ventricle. Int. J. Cardiovasc. Imaging 2020, 36, 2173–2185. [Google Scholar] [CrossRef]
- Monosilio, S.; Filomena, D.; Luongo, F.; Sannino, M.; Cimino, S.; Neccia, M.; Mariani, M.V.; Birtolo, L.I.; Benedetti, G.; Tonti, G.; et al. Cardiac and Vascular Remodeling after 6 Months of Therapy with Sacubitril/Valsartan: Mechanistic Insights from Advanced Echocardiographic Analysis. Front. Cardiovasc. Med. 2022, 9, 883769. [Google Scholar] [CrossRef] [PubMed]
- Faganello, G.; Pagura, L.; Collia, D.; Barbati, G.; Paldino, A.; Ferro, M.D.; Croatto, E.; Sinagra, G.; Pedrizzetti, G.; Di Lenarda, A. Prognostic value of echocardiographic evaluation of cardiac mechanics in patients with aortic stenosis and preserved left ventricular ejection fraction. Int. J. Cardiovasc. Imaging 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, F.; Capuano, F.; Cocchia, R.; Ranieri, B.; Contaldi, C.; Lacava, G.; Capone, V.; Chianese, S.; Rega, S.; Annunziata, R.; et al. Reference Ranges of Left Ventricular Hemodynamic Forces in Healthy Adults: A Speckle-Tracking Echocardiographic Study. J. Clin. Med. 2021, 10, 5937. [Google Scholar] [CrossRef]
- Maes, F.; Lerakis, S.; Barbosa Ribeiro, H.; Gilard, M.; Cavalcante, J.L.; Makkar, R.; Herrmann, H.C.; Windecker, S.; Enriquez-Sarano, M.; Cheema, A.N.; et al. Outcomes from Transcatheter Aortic Valve Replacement in Patients with Low-Flow, Low-Gradient Aortic Stenosis and Left Ventricular Ejection Fraction Less Than 30%: A Substudy from the TOPAS-TAVI Registry. JAMA Cardiol. Am. Med. Assoc. 2019, 4, 64–70. [Google Scholar] [CrossRef]
- Fernández-Santos, S.; Théron, A.; Pibarot, P.; Collart, F.; Gilard, M.; Urena, M.; Hovorka, T.; Kahlert, P.; Gomez, J.L.Z. Valve hemodynamic performance and myocardial strain after implantation of a third-generation, balloon-expandable, transcatheter aortic valve. Cardiol. J. 2020, 27, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Airale, L.; Vallelonga, F.; Forni, T.; Leone, D.; Magnino, C.; Avenatti, E.; Iannaccone, A.; Astarita, A.; Mingrone, G.; Cesareo, M.; et al. A Novel Approach to Left Ventricular Filling Pressure Assessment: The Role of Hemodynamic Forces Analysis. Front. Cardiovasc. Med. 2021, 8, 704909. [Google Scholar] [CrossRef]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart BMJ Publ. Group Ltd Br. Cardiovasc. Soc. 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Pedrizzetti, G.; Arvidsson, P.M.; Töger, J.; Borgquist, R.; Domenichini, F.; Arheden, H.; Heiberg, E. On estimating intraventricular hemodynamic forces from endocardial dynamics: A comparative study with 4D flow MRI. J. Biomech. 2017, 60, 203–210. [Google Scholar] [CrossRef]
- Ravaux, J.M.; Van Kuijk, S.M.J.; Di Mauro, M.; Vernooy, K.; Bidar, E.; Hof, A.W.V.; Veenstra, L.; Kats, S.; Houterman, S.; Maessen, J.G.; et al. Incidence and Predictors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Procedures: Data of the Netherlands Heart Registration (NHR). J. Clin. Med. 2022, 11, 560. [Google Scholar] [CrossRef]
- Töger, J.; Arvidsson, P.M.; Bock, J.; Kanski, M.; Pedrizzetti, G.; Carlsson, M.; Arheden, H.; Heiberg, E. Hemodynamic forces in the left and right ventricles of the human heart using 4D flow magnetic resonance imaging: Phantom validation, reproducibility, sensitivity to respiratory gating and free analysis software. PLoS ONE 2018, 13, e0195597. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (±SD) or N (%) |
|---|---|
| Age—years | 83 ± 5 |
| Female sex—no. (%) | 9 (36%) |
| Body surface area—m2 | 1.79 ± 0.22 |
| CAD—no. (%) | 9 (36%) |
| Other cardiopathy—no. (%) | 5 (20%) |
| Conduction disturbances—no. (%) | 9 (36%) |
| HG AS—no. (%) | 21 (84%) |
| LF-LG AS with reduced EF—no. (%) | 3 (12%) |
| LF-LG AS with preserved EF—no. (%) | 1 (4%) |
| Moderate or severe MR—no. (%) | 8 (32%) |
| Moderate or severe AR—no. (%) | 9 (36%) |
| Moderate or severe TR—no. (%) | 8 (32%) |
| Left ventricular ejection fraction (LVEF)—% | 57 ± 8 |
| LV global longitudinal strain (GLS)—% | −19 ± 4.5 |
| Endo strain rate (SR) LV—no. | −0.87 ± 0.28 |
| Stroke volume index (SVi)—mL/m2 | 43 ± 8 |
| Flow rate (FR)—mL/s | 234 ± 50 |
| Hemodynamic work—(mJ) | 0.89 ± 0.97 |
| E/e’ average—no. | 15 ± 5 |
| Left ventricular longitudinal force (LVLF) apex-base—% | 7.41 ± 2.65 |
| Left ventricular systolic longitudinal force (LVsysLF) apex-base—% | 9.85 ± 3.15 |
| Left ventricular impulse (LVim) apex-base—% | 9.52 ± 2.95 |
| Left ventricular suction (LVs) apex-base—% | −4.92 ± 2.3 |
| Variable | Mean Δ | C.I. 95% | p-Value | |
|---|---|---|---|---|
| Lower Limit | Upper Limit | |||
| LVLF apex-base (%) | 1.80 | 1.07 | 2.52 | <0.001 |
| LVsysLF apex-base (%) | 2.64 | 1.57 | 3.70 | <0.001 |
| LVim apex-base (%) | 2.89 | 1.48 | 4.29 | <0.001 |
| LVLF angle (°) | 1.52 | 0.07 | 2.97 | 0.04 |
| LVim angle (°) | 2.16 | 0.76 | 3.56 | 0.004 |
| FR (ml/s) | 31.40 | 12.19 | 50.61 | <0.001 |
| E/e’ avg. | −1.42 | −2.64 | −0.19 | 0.03 |
| LVs apex-base (%) | −0.54 | −1.31 | 0.22 | 0.16 |
| LVs angle (°) | 0.16 | −3.31 | 3.63 | 0.93 |
| SVi (mL/m2) | 0.36 | −3.43 | 4.16 | 0.84 |
| LVEF (%) | 1.44 | −0.15 | 3.03 | 0.07 |
| Variable | % of Patients within Normality Pre-TAVI | % of Patients within Normality Post-TAVI |
|---|---|---|
| LVLF apex-base (%) | 4 | 56 |
| LVsysLF apex-base (%) | 4 | 52 |
| LVim apex-base (%) | 4 | 60 |
| LVEF (%) | 72 | 72 |
| LV GLS (%) | 56 | 60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vairo, A.; Zaccaro, L.; Ballatore, A.; Airale, L.; D’Ascenzo, F.; Alunni, G.; Conrotto, F.; Scudeler, L.; Mascaretti, D.; Miccoli, D.; et al. Acute Modification of Hemodynamic Forces in Patients with Severe Aortic Stenosis after Transcatheter Aortic Valve Implantation. J. Clin. Med. 2023, 12, 1218. https://doi.org/10.3390/jcm12031218
Vairo A, Zaccaro L, Ballatore A, Airale L, D’Ascenzo F, Alunni G, Conrotto F, Scudeler L, Mascaretti D, Miccoli D, et al. Acute Modification of Hemodynamic Forces in Patients with Severe Aortic Stenosis after Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine. 2023; 12(3):1218. https://doi.org/10.3390/jcm12031218
Chicago/Turabian StyleVairo, Alessandro, Lorenzo Zaccaro, Andrea Ballatore, Lorenzo Airale, Fabrizio D’Ascenzo, Gianluca Alunni, Federico Conrotto, Luca Scudeler, Daniela Mascaretti, Davide Miccoli, and et al. 2023. "Acute Modification of Hemodynamic Forces in Patients with Severe Aortic Stenosis after Transcatheter Aortic Valve Implantation" Journal of Clinical Medicine 12, no. 3: 1218. https://doi.org/10.3390/jcm12031218
APA StyleVairo, A., Zaccaro, L., Ballatore, A., Airale, L., D’Ascenzo, F., Alunni, G., Conrotto, F., Scudeler, L., Mascaretti, D., Miccoli, D., Torre, M. L., Rinaldi, M., Pedrizzetti, G., Salizzoni, S., & De Ferrari, G. M. (2023). Acute Modification of Hemodynamic Forces in Patients with Severe Aortic Stenosis after Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine, 12(3), 1218. https://doi.org/10.3390/jcm12031218