
A Standardized Operative Protocol for Fixation of Proximal Humeral Fractures Using a Locking Plate to Minimize Surgery-Related Complications

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
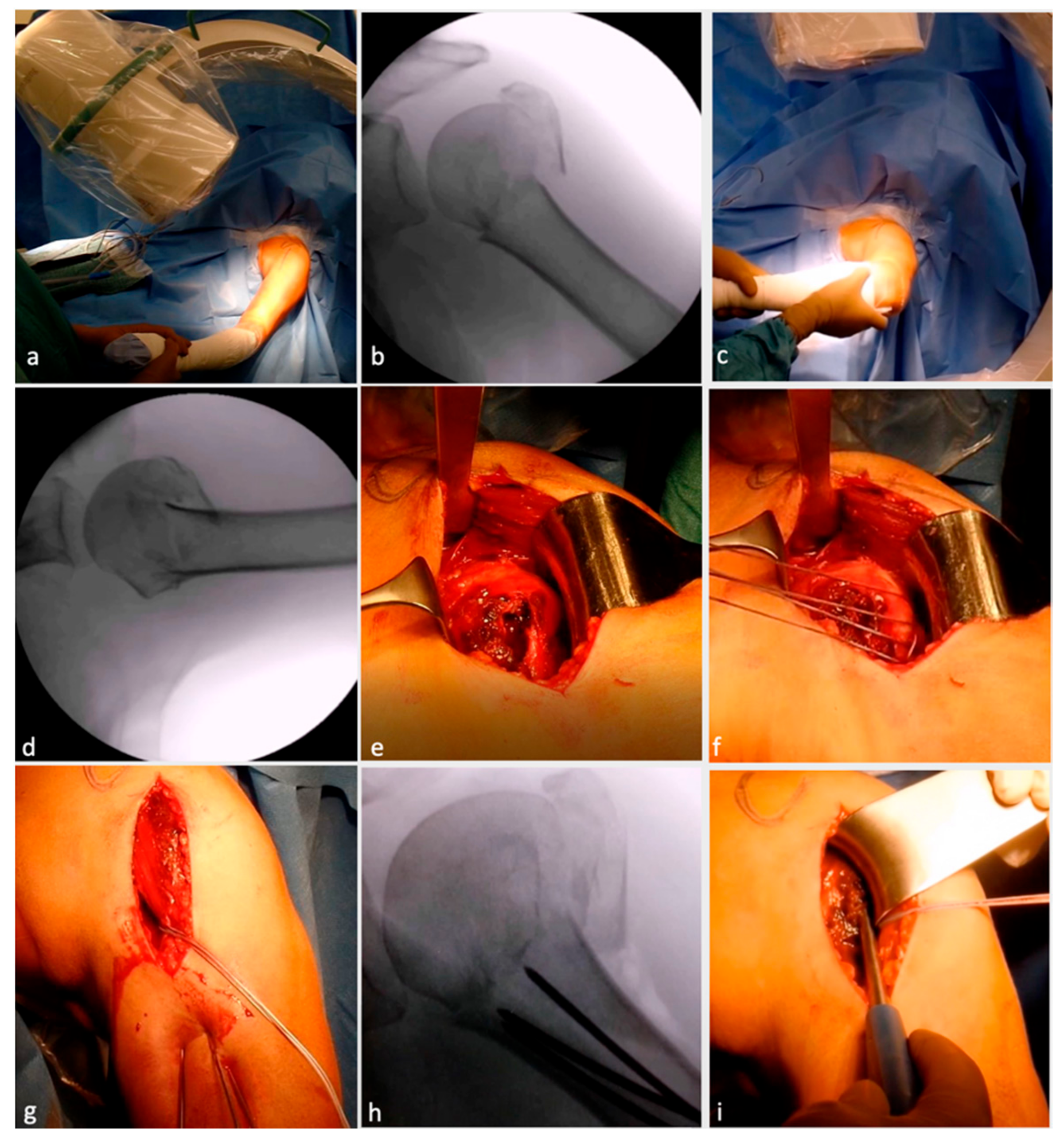
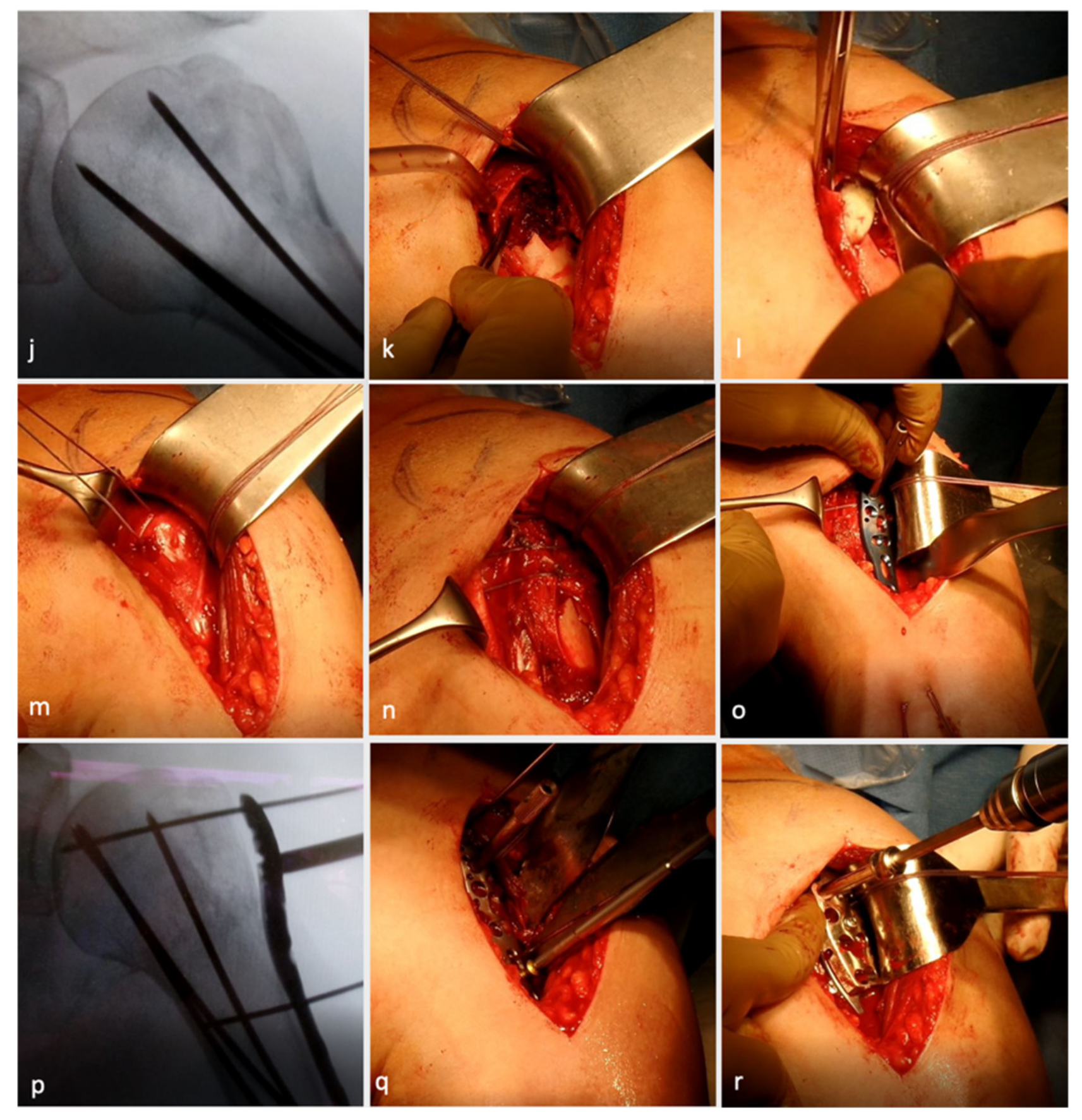
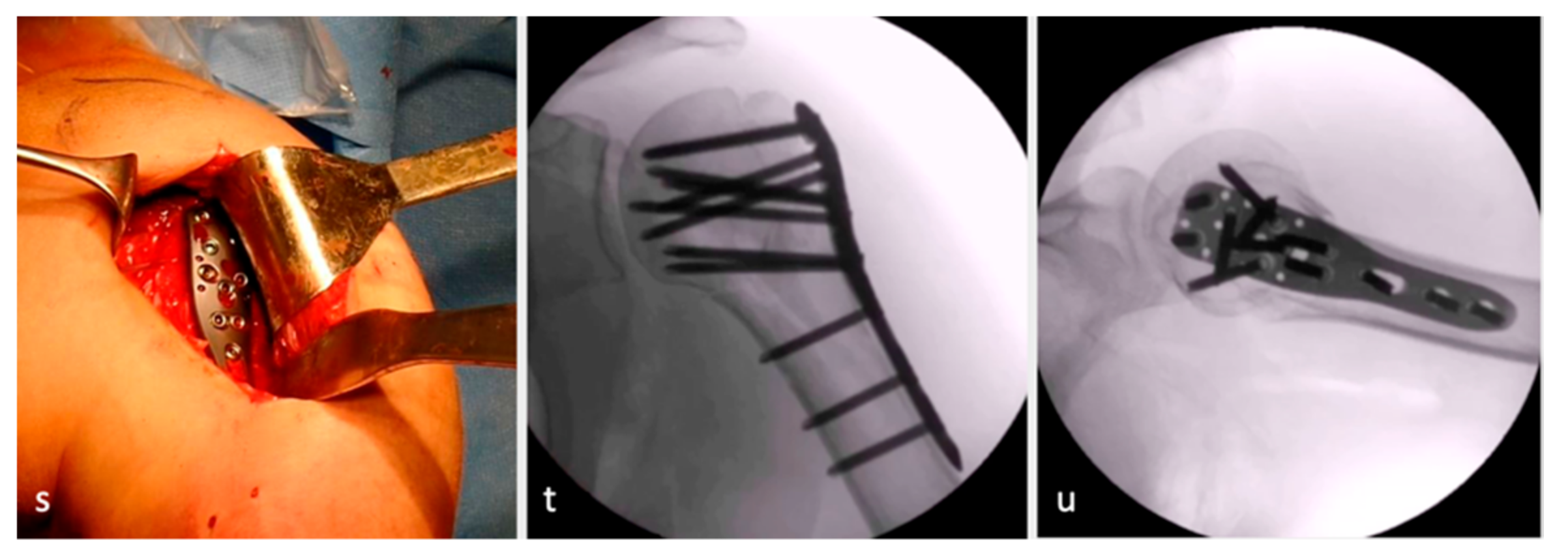
2.2. Surgical Procedure and Postoperative Protocol
2.3. Intraoperative Assessment
2.4. Clinical Examinations
2.5. Radiographic Evaluation
2.6. Adverse Events
2.7. Statistical Analysis
3. Results
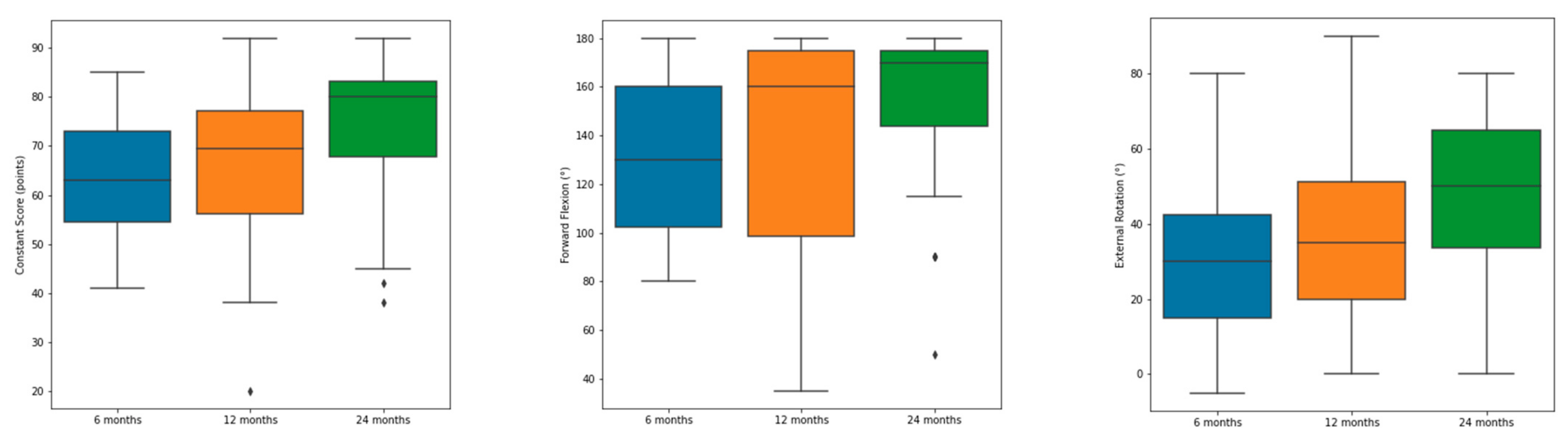
3.1. Clinical Results
3.2. LHB Tenodesis vs. Tenotomy
3.3. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baron, J.; Barrett, J.; Karagas, M. The epidemiology of peripheral fractures. Bone 1996, 18, S209–S213. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8777090 (accessed on 15 September 2021). [CrossRef]
- Court-Brown, C.M.; Caesar, B. Epidemiology of adult fractures: A review. Injury 2006, 37, 691–697. [Google Scholar] [CrossRef]
- Lanting, B.; MacDermid, J.; Drosdowech, D.; Faber, K.J. Proximal humeral fractures: A systematic review of treatment modalities. J. Shoulder Elb. Surg. 2008, 17, 42–54. [Google Scholar] [CrossRef]
- Lee, S.H.; Dargent-Molina, P.; Breart, G. Risk Factors for Fractures of the Proximal Humerus: Results from the EPIDOS Prospective Study. J. Bone Miner. Res. 2002, 17, 817–825. [Google Scholar] [CrossRef]
- Nguyen, T.V.; Center, J.R.; Sambrook, P.N.; Eisman, J.A. Risk factors for proximal humerus, forearm, and wrist fractures in elderly men and women: The Dubbo Osteoporosis Epidemiology Study. Am. J. Epidemiol. 2001, 153, 587–595. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11257067 (accessed on 15 September 2021). [CrossRef]
- Park, C.; Jang, S.; Lee, A.; Kim, H.Y.; Lee, Y.B.; Kim, T.Y.; Ha, Y.C. Incidence and Mortality after Proximal Humerus Fractures Over 50 Years of Age in South Korea: National Claim Data from 2008 to 2012. J. Bone Metab. 2015, 22, 17–21. [Google Scholar] [CrossRef]
- Palvanen, M.; Kannus, P.; Niemi, S.; Parkkari, J. Update in the Epidemiology of Proximal Humeral Fractures. Clin. Orthop. Relat. Res. 2006, 442, 87–92. [Google Scholar] [CrossRef]
- Kim, S.H.; Szabo, R.M.; Marder, R.A. Epidemiology of humerus fractures in the United States: Nationwide emergency department sample, 2008. Arthritis Care Res. 2011, 64, 407–414. [Google Scholar] [CrossRef]
- Dimai, H.P.; Svedbom, A.; Fahrleitner-Pammer, A.; Pieber, T.; Resch, H.; Zwettler, E.; Thaler, H.; Szivak, M.; Amrein, K.; Borgström, F. Epidemiology of proximal humeral fractures in Austria between 1989 and 2008. Osteoporos. Int. 2013, 24, 2413–2421. [Google Scholar] [CrossRef]
- Khatib, O.; Onyekwelu, I.; Zuckerman, J.D. The incidence of proximal humeral fractures in New York State from 1990 through 2010 with an emphasis on operative management in patients aged 65 years or older. J. Shoulder Elb. Surg. 2014, 23, 1356–1362. [Google Scholar] [CrossRef]
- Boileau, P.; Pennington, S.D.; Alami, G. Proximal humeral fractures in younger patients: Fixation techniques and arthroplasty. J. Shoulder Elb. Surg. 2011, 20, S47–S60. [Google Scholar] [CrossRef]
- Gavaskar, A.S.; Tummala, N.C. Locked plate osteosynthesis of humeral head–splitting fractures in young adults. J. Shoulder Elb. Surg. 2015, 24, 908–914. [Google Scholar] [CrossRef]
- Jones, C.B.; Sietsema, D.L.; Williams, D.K. Locked Plating of Proximal Humeral Fractures: Is Function Affected by Age, Time, and Fracture Patterns? Clin. Orthop. Relat. Res. 2011, 469, 3307–3316. [Google Scholar] [CrossRef]
- Hong, C.; Hey, H.; Murphy, D. Evolving trends in surgically managed patients with proximal humerus fracture: Are we different after ten years? Singap. Med. J. 2014, 55, 574–578. [Google Scholar] [CrossRef]
- Young, T.B.; Wallace, W.A. Conservative treatment of fractures and fracture-dislocations of the upper end of the humerus. J. Bone Joint Surg. Br. 1985, 67, 373–377. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3997943 (accessed on 15 September 2021). [CrossRef]
- Rasmussen, S.; Hvass, I.; Dalsgaard, J.; Christensen, B.; Holstad, E. Displaced proximal humeral fractures: Results of conservative treatment. Injury 1992, 23, 41–43. Available online: http://www.ncbi.nlm.nih.gov/pubmed/1541498 (accessed on 15 September 2021). [CrossRef]
- Neer, C.S., 2nd. Displaced proximal humeral fractures. I. Classification and evaluation. J. Bone Joint Surg. Am. 1970, 52, 1077–1089. Available online: http://www.ncbi.nlm.nih.gov/pubmed/5455339 (accessed on 15 September 2021). [CrossRef]
- Solberg, B.D.; Moon, C.N.; Franco, D.P.; Paiement, G.D. Surgical Treatment of Three and Four-Part Proximal Humeral Fractures. J. Bone Jt. Surg. 2009, 91, 1689–1697. [Google Scholar] [CrossRef]
- Olerud, P.; Ahrengart, L.; Ponzer, S.; Saving, J.; Tidermark, J. Hemiarthroplasty versus nonoperative treatment of displaced 4-part proximal humeral fractures in elderly patients: A randomized controlled trial. J. Shoulder Elb. Surg. 2011, 20, 1025–1033. [Google Scholar] [CrossRef]
- Olerud, P.; Ahrengart, L.; Ponzer, S.; Saving, J.; Tidermark, J. Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: A randomized controlled trial. J. Shoulder Elb. Surg. 2011, 20, 747–755. [Google Scholar] [CrossRef]
- Iyengar, J.J.; Devcic, Z.; Sproul, R.C.; Feeley, B.T. Nonoperative Treatment of Proximal Humerus Fractures: A Systematic Review. J. Orthop. Trauma 2011, 25, 612–617. [Google Scholar] [CrossRef]
- Ockert, B.; Siebenbürger, G.; Kettler, M.; Braunstein, V.; Mutschler, W. Long-term functional outcomes (median 10 years) after locked plating for displaced fractures of the proximal humerus. J. Shoulder Elb. Surg. 2014, 23, 1223–1231. [Google Scholar] [CrossRef]
- Schliemann, B.; Siemoneit, J.; Theisen, C.; Kösters, C.; Weimann, A.; Raschke, M.J. Complex fractures of the proximal humerus in the elderly—Outcome and complications after locking plate fixation. Musculoskelet. Surg. 2012, 96, 3–11. [Google Scholar] [CrossRef]
- Sproul, R.C.; Iyengar, J.J.; Devcic, Z.; Feeley, B.T. A systematic review of locking plate fixation of proximal humerus fractures. Injury 2011, 42, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Thanasas, C.; Kontakis, G.; Angoules, A.; Limb, D.; Giannoudis, P. Treatment of proximal humerus fractures with locking plates: A systematic review. J. Shoulder Elb. Surg. 2009, 18, 837–844. [Google Scholar] [CrossRef]
- Chudik, S.C.; Weinhold, P.; Dahners, L.E. Fixed-angle plate fixation in simulated fractures of the proximal humerus: A biomechanical study of a new device. J. Shoulder Elb. Surg. 2003, 12, 578–588. [Google Scholar] [CrossRef]
- Laflamme, G.Y.; Rouleau, D.M.; Berry, G.K.; Beaumont, P.H.; Reindl, R.; Harvey, E.J. Percutaneous Humeral Plating of Fractures of the Proximal Humerus: Results of a Prospective Multicenter Clinical Trial. J. Orthop. Trauma 2008, 22, 153–158. [Google Scholar] [CrossRef]
- Spross, C.; Platz, A.; Erschbamer, M.; Lattmann, T.; Dietrich, M. Surgical Treatment of Neer Group VI Proximal Humeral Fractures: Retrospective Comparison of PHILOS® and Hemiarthroplasty. Clin. Orthop. Relat. Res. 2012, 470, 2035–2042. [Google Scholar] [CrossRef]
- Hirschmann, M.T.; Quarz, V.; Audigé, L.; Ludin, D.; Messmer, P.; Regazzoni, P.; Gross, T. Internal Fixation of Unstable Proximal Humerus Fractures With an Anatomically Preshaped Interlocking Plate: A Clinical and Radiologic Evaluation. J. Trauma: Inj. Infect. Crit. Care 2007, 63, 1314–1323. [Google Scholar] [CrossRef]
- Kettler, M.; Biberthaler, P.; Braunstein, V.; Zeiler, C.; Kroetz, M.; Mutschler, W. Die winkelstabile Osteosynthese am proximalen Humerus mit der PHILOS-Platte. Der Unfallchirurg 2006, 109, 1032–1040. [Google Scholar] [CrossRef]
- Südkamp, N.; Bayer, J.; Hepp, P.; Voigt, C.; Oestern, H.; Kääb, M.; Luo, C.; Plecko, M.; Wendt, K.; Köstler, W.; et al. Open Reduction and Internal Fixation of Proximal Humeral Fractures with Use of the Locking Proximal Humerus Plate. J. Bone Jt. Surg. 2009, 91, 1320–1328. [Google Scholar] [CrossRef]
- Tepass, A.; Blumenstock, G.; Weise, K.; Rolauffs, B.; Bahrs, C. Current strategies for the treatment of proximal humeral fractures: An analysis of a survey carried out at 348 hospitals in Germany, Austria, and Switzerland. J. Shoulder Elb. Surg. 2013, 22, e8–e14. [Google Scholar] [CrossRef]
- Agudelo, J.; Schürmann, M.; Stahel, P.; Helwig, P.; Morgan, S.J.; Zechel, W.; Bahrs, C.; Parekh, A.; Ziran, B.; Williams, A.; et al. Analysis of Efficacy and Failure in Proximal Humerus Fractures Treated with Locking Plates. J. Orthop. Trauma 2007, 21, 676–681. [Google Scholar] [CrossRef]
- Han, R.J.; Sing, D.C.; Feeley, B.T.; Ma, C.B.; Zhang, A.L. Proximal humerus fragility fractures: Recent trends in nonoperative and operative treatment in the Medicare population. J. Shoulder Elb. Surg. 2016, 25, 256–261. [Google Scholar] [CrossRef]
- Jost, B.; Spross, C.; Grehn, H.; Gerber, C. Locking plate fixation of fractures of the proximal humerus: Analysis of complications, revision strategies and outcome. J. Shoulder Elb. Surg. 2013, 22, 542–549. [Google Scholar] [CrossRef]
- Owsley, K.C.; Gorczyca, J.T. Displacement/Screw Cutout After Open Reduction and Locked Plate Fixation of Humeral Fractures. J. Bone Jt. Surg. 2008, 90, 233–240. [Google Scholar] [CrossRef]
- Koeppe, J.; Katthagen, J.C.; Rischen, R.; Freistuehler, M.; Faldum, A.; Raschke, M.J.; Stolberg-Stolberg, J. Male Sex Is Associated with Higher Mortality and Increased Risk for Complications after Surgical Treatment of Proximal Humeral Fractures. J. Clin. Med. 2021, 10, 2500. [Google Scholar] [CrossRef]
- Sanders, R.J.; Thissen, L.G.; Teepen, J.C.; van Kampen, A.; Jaarsma, R.L. Locking plate versus nonsurgical treatment for proximal humeral fractures: Better midterm outcome with nonsurgical treatment. J. Shoulder Elb. Surg. 2011, 20, 1118–1124. [Google Scholar] [CrossRef]
- Bahrs, C.; Kühle, L.; Blumenstock, G.; Stöckle, U.; Rolauffs, B.; Freude, T. Which parameters affect medium- to long-term results after angular stable plate fixation for proximal humeral fractures? J. Shoulder Elb. Surg. 2015, 24, 727–732. [Google Scholar] [CrossRef]
- Minkus, M.; Scheibel, M. Open reduction, retention, and fixation of proximal humeral fractures using a locking plate osteosynthesis. Obere Extremität 2019, 14, 136–138. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop Relat. Res. 1987, 214, 160–164. Available online: https://www.ncbi.nlm.nih.gov/pubmed/3791738 (accessed on 15 September 2021). [CrossRef]
- Fuchs, B.; Jost, B.; Gerber, C. Posterior-inferior capsular shift for the treatment of recurrent, voluntary posterior subluxation of the shoulder. J. Bone Joint Surg. Am. 2000, 82, 16–25. Available online: https://www.ncbi.nlm.nih.gov/pubmed/10653080 (accessed on 15 September 2021). [CrossRef]
- Scheibel, M.; Schröder, R.-J.; Chen, J.; Bartsch, M. Arthroscopic Soft Tissue Tenodesis Versus Bony Fixation Anchor Tenodesis of the Long Head of the Biceps Tendon. Am. J. Sports Med. 2011, 39, 1046–1052. [Google Scholar] [CrossRef]
- Gilbart, M.K.; Gerber, C. Comparison of the subjective shoulder value and the Constant score. J. Shoulder Elb. Surg. 2007, 16, 717–721. [Google Scholar] [CrossRef]
- Silverstein, M.P.; Yirenkyi, K.; Haidukewych, G.; Koval, K.J. Analysis of Failure with the Use of Locked Plates for Stabilization of Proximal Humerus Fractures. Bull Hosp. Jt. Dis. 2015, 73, 185–189. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26535597 (accessed on 15 September 2021).
- Haupt, S.; Weber, S.; Frima, H.; Hutter, R.; Grehn, H.; Sommer, C. Proximal humeral fracture-dislocation: Outcome analysis in osteosynthesis and arthroplasties. Eur. J. Orthop. Surg. Traumatol. 2022. [Google Scholar] [CrossRef]
- Lorenz, G.; Schönthaler, W.; Huf, W.; Komjati, M.; Fialka, C.; Boesmueller, S. Complication rate after operative treatment of three- and four-part fractures of the proximal humerus: Locking plate osteosynthesis versus proximal humeral nail. Eur. J. Trauma Emerg. Surg. 2021, 47, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Ranson, R.; Roller, R.; Dedhia, N.; Littlefield, C.P.; Konda, S.; Zuckerman, J.D.; Egol, K. No change in outcome ten years following locking plate repair of displaced proximal humerus fractures. Eur. J. Orthop. Surg. Traumatol. 2022, 32, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Kerschbaum, M.; Werth, M.; Gerhardt, C.; Scheibel, M. Simultane Versorgung der langen Bizepssehne im Rahmen der operativen Therapie proximaler Humerusfrakturen. Der Unfallchirurg 2017, 120, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Hazra, R.-O.D.; Illner, J.; Szewczyk, K.; Warnhoff, M.; Ellwein, A.; Blach, R.M.; Lill, H.; Jensen, G. Age-Independent Clinical Outcome in Proximal Humeral Fractures: 2-Year Results Using the Example of a Precontoured Locking Plate. J. Clin. Med. 2022, 11, 408. [Google Scholar] [CrossRef]
- Peker, B.; Polat, A.E.; Carkci, E.; Senel, A.; Soydan, C.; Tuzuner, T. Functional Outcomes and Complication Analysis of Plate Osteosynthesis versus Hemiarthroplasty in Three-part and Four-part Proximal Humerus Fractures. J. Pak. Med. Assoc. 2022, 72, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Harris, J.; Erickson, B.J.; Abrams, G.D.; Bruce, B.; McCormick, F.; Nicholson, G.P.; Romeo, A. Surgical Management of Complex Proximal Humerus Fractures—A Systematic Review of 92 Studies Including 4500 Patients. J. Orthop. Trauma 2015, 29, 54–59. [Google Scholar] [CrossRef]
- Solberg, B.D.; Moon, C.N.; Franco, D.P.; Paiement, G.D. Locked Plating of 3- and 4-Part Proximal Humerus Fractures in Older Patients: The Effect of Initial Fracture Pattern on Outcome. J. Orthop. Trauma 2009, 23, 113–119. [Google Scholar] [CrossRef]
- Geiger, E.V. functional outcome and complications following PHILOS plate fixation proximal humeral fractures. Acta Orthop. et Traumatol. Turc. 2010, 44, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gomes, G.R.; Maciel, R.A.; Neto, J.I.D.A.; DE Toledo, D.C.; Machado, C.J.; Bomfim, L.d.S. Antegrade Nailing Versus Locking Plate of 2-and 3-Part Proximal Humerus Fractures. Acta Ortopédica Bras. 2022, 30, e256113. [Google Scholar] [CrossRef]
- Fraser, A.N.; Bjørdal, J.; Wagle, T.M.; Karlberg, A.C.; Lien, O.A.; Eilertsen, L.; Mader, K.; Apold, H.; Larsen, L.B.; Madsen, J.E.; et al. Reverse Shoulder Arthroplasty Is Superior to Plate Fixation at 2 Years for Displaced Proximal Humeral Fractures in the Elderly. J. Bone Jt. Surg. 2020, 102, 477–485. [Google Scholar] [CrossRef]
- Imiolczyk, J.-P.; Moroder, P.; Scheibel, M. Fracture-Specific and Conventional Stem Designs in Reverse Shoulder Arthroplasty for Acute Proximal Humerus Fractures—A Retrospective, Observational Study. J. Clin. Med. 2021, 10, 175. [Google Scholar] [CrossRef]
- Imiolczyk, J.-P.; Brunner, U.; Imiolczyk, T.; Freislederer, F.; Endell, D.; Scheibel, M. Reverse Shoulder Arthroplasty for Proximal Humerus Head-Split Fractures—A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 2835. [Google Scholar] [CrossRef]
- Porschke, F.; Bockmeyer, J.; Nolte, P.-C.; Studier-Fischer, S.; Guehring, T.; Schnetzke, M. More Adverse Events after Osteosyntheses Compared to Arthroplasty in Geriatric Proximal Humeral Fractures Involving Anatomical Neck. J. Clin. Med. 2021, 10, 979. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.C.; Kang, S.-W.; Son, S.M.; Seo, J.S.; Choi, M.H. High bone union rate using a locking plate for proximal humeral fractures in patients older than 70 years: Importance of the medial column. Eur. J. Trauma Emerg. Surg. 2022, 48, 2937–2942. [Google Scholar] [CrossRef] [PubMed]
- Samborski, S.A.; Haws, B.E.; Karnyski, S.; Soles, G.; Gorczyca, J.T.; Nicandri, G.; Voloshin, I.; Ketz, J.P. Outcomes for type C proximal humerus fractures in the adult population: Comparison of nonoperative treatment, locked plate fixation, and reverse shoulder arthroplasty. JSES Int. 2022, 6, 755–762. [Google Scholar] [CrossRef]
- Lanzetti, R.M.; Gaj, E.; Berlinberg, E.J.B.; Patel, H.H.B.; Spoliti, M. Reverse Total Shoulder Arthroplasty Demonstrates Better Outcomes Than Angular Stable Plate in the Treatment of Three-part and Four-part Proximal Humerus Fractures in Patients Older Than 70 Years. Clin. Orthop. Relat. Res. 2022. [CrossRef] [PubMed]
- Laflamme, G.-Y.; Moisan, P.; Chapleau, J.; Goulet, J.; Leduc, S.; Benoit, B.; Rouleau, D.M. Novel Technical Factors Affecting Proximal Humerus Fixation Stability. J. Orthop. Trauma 2021, 35, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Bhayana, H.; Chouhan, D.K.; Aggarwal, S.; Prakash, M.; Patel, S.; Arora, C.; Dhillon, M.S. Outcomes of plate osteosynthesis for displaced 3-part and 4-part proximal humerus fractures with deltopectoral vs. deltoid split approach. Eur. J. Trauma Emerg. Surg. 2022, 48, 4559–4567. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Wang, X.; Wang, C.; Jiao, Z.; Chen, W. Displaced proximal humerus fractures treated with ORIF via the deltoid interfascicular approach vs the deltopectoral approach. Medicine 2022, 101, e29075. [Google Scholar] [CrossRef]
- Launonen, A.P.; Sumrein, B.O.; Reito, A.; Lepola, V.; Paloneva, J.; Jonsson, K.B.; Wolf, O.; Ström, P.; Berg, H.E.; Felländer-Tsai, L.; et al. Operative versus non-operative treatment for 2-part proximal humerus fracture: A multicenter randomized controlled trial. PLoS Med. 2019, 16, e1002855. [Google Scholar] [CrossRef]
- Clavert, P.; Adam, P.; Bevort, A.; Bonnomet, F.; Kempf, J.-F. Pitfalls and complications with locking plate for proximal humerus fracture. J. Shoulder Elb. Surg. 2010, 19, 489–494. [Google Scholar] [CrossRef]
- Kuhlmann, T.; Hofmann, T.; Seibert, O.; Gundlach, G.; Schmidt-Horlohé, K.; Hoffmann, R. Vergleich Philos- vs. Königseeplattenosteosynthese bei der operativen Versorgung von 4-Fragment-Frakturen des proximalen Humerus bei über 65-jährigen Patienten. Zeitschrift für Orthopädie und Unfallchirurgie 2012, 150, 149–155. [Google Scholar] [CrossRef]
- Hettrich, C.M.; Neviaser, A.; Beamer, B.S.; Paul, O.; Helfet, D.L.; Lorich, D.G. Locked Plating of the Proximal Humerus Using an Endosteal Implant. J. Orthop. Trauma 2012, 26, 212–215. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operative Characteristics | n |
| AO/OTA Fracture and Dislocation Classification | |
| A2 | 4 |
| A3 | 13 |
| B1 | 7 |
| B2 | 6 |
| B3 | 2 |
| C1 | 12 |
| C2 | 5 |
| C3 | 1 |
| Additional treatment | |
| Fiber wire Cerclage GT | 24 |
| Fiber wire Cerclage LT | 2 |
| Fiber wire Cerclage GT + LT | 9 |
| Fiber wire cerclage around proximal humerus | 3 |
| No Fiber wire cerclage | 12 |
| Bone augmentation | 20 |
| Biceps tenodesis | 24 |
| Biceps tenotomy | 26 |
| Additional anterosuperior rotator cuff reconstruction | 6 |
| Rating of surgery (difficulty) (subjective) | |
| easy | 27 |
| moderate | 19 |
| difficult | 4 |
| Bone quality (1 = good; 5 = bad) (subjective) | |
| 1 | 3 |
| 2 | 21 |
| 3 | 19 |
| 4 | 7 |
| 5 | 0 |
| Follow-Up Examination | Forward Flexion (°) | Abduction | External Rotation (°) | Internal Rotation | Absolute CS (Points) | Relative CS * (%) | SSV (%) |
|---|---|---|---|---|---|---|---|
| 6 months (n = 35) | 132 (±32) (80–180) | 118 (±38) (40–180) | 31 (±20) (−5–80) | L2 (buttocks–T5) | 62 (±13) (41–85) | 82 (±10) (42–100) | - |
| 12 months (n = 40) | 138 (±42) (35–180) | 129 (±45) (30–180) | 38 (±26) (0–90) | T12 (buttocks-T3) | 66 (±16) (20–92) | 84 (±7) (52–100) | 77 (±20) (10–100) |
| 24 months (n = 34) | 153 (±35) (50–180) | 146 (±38) (55–180) | 48 (±23) (0–80) | T10 (buttocks-T3) | 74 (±14) (38–92) | 89 (±8) (43–100) | 83 (±17) (5–100) |
| Mean differences | |||||||
| between 6 and 12 months (95% CI) | 16 (3;30) | 20 (7;33) | 11 (2;19) | 3 vertebra (2;4) | 6 (1;11) | 6 (3;10) | - |
| between 12 and 24 months (95% CI) | 6 (1;12) | 9 (2;15) | 6 (0;11) | 1 vertebra (1;1) | 4 (2;6) | 4 (2;7) | 3 (−1–8) |
| No. | Fracture Type | Difficulty of Surgery | Bone Quality * | Complication | 1Y CMS (Points) | 1Y SSV (%) | 2Y CMS (Points) | 2Y SSV (%) | Revision |
|---|---|---|---|---|---|---|---|---|---|
| 1 | C2 | difficult | 3 | Secondary screw cut-out | 68 | 60 | - | - | Implant removal after 1Y, no 2 year FU |
| 2 | B2 | moderate | 2 | Secondary screw cut-out | 54 | 80 | 71 | 90 | Implant removal |
| 3 | A3 | moderate | 3 | Partial (distal) plate loosening | 57 | 70 | 56 | 70 | No revision surgery |
| 4 | A3 | easy | 2 | Total AVN with secondary screw cut-out | 41 | 60 | 37 | 60 | Revision to reverse shoulder arthroplasty after 12 months |
| 5 | B3 | difficult | 2 | Partial AVN with secondary screw cut-out | 20 | 10 | 18 | 5 | Revision to hemiarthroplasty after 12 months |
| 6 | C3 | difficult | 2 | Partial AVN with secondary screw cut-out | 78 | 75 | 83 | 65 | Implant removal and arthroscopic capsulotomy |
| 7 | C1 | easy | 3 | Secondary GT displacement and extraanatomical consolidation | 49 | 50 | - | - | No revision, no 2-year FU |
| 8 | B2 | difficult | 3 | Partial AVN with secondary screw cut-out | 68 | 90 | 68 | 80 | Implant removal |
| 9 | A3 | moderate | 3 | Partial AVN with secondary screw cut-out | 39 | 65 | 60 | 90 | Revision to hemiarthroplasty after 12 months |
| 10 | B2 | moderate | 2 | Pseudoarthrosis | 45 | 35 | 45 | 70 | Implant removal and Re-ORIF after 12 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwisda, S.; Imiolczyk, J.-P.; Imiolczyk, T.; Werth, M.; Scheibel, M. A Standardized Operative Protocol for Fixation of Proximal Humeral Fractures Using a Locking Plate to Minimize Surgery-Related Complications. J. Clin. Med. 2023, 12, 1216. https://doi.org/10.3390/jcm12031216
Kwisda S, Imiolczyk J-P, Imiolczyk T, Werth M, Scheibel M. A Standardized Operative Protocol for Fixation of Proximal Humeral Fractures Using a Locking Plate to Minimize Surgery-Related Complications. Journal of Clinical Medicine. 2023; 12(3):1216. https://doi.org/10.3390/jcm12031216
Chicago/Turabian StyleKwisda, Sebastian, Jan-Philipp Imiolczyk, Tankred Imiolczyk, Magdalena Werth, and Markus Scheibel. 2023. "A Standardized Operative Protocol for Fixation of Proximal Humeral Fractures Using a Locking Plate to Minimize Surgery-Related Complications" Journal of Clinical Medicine 12, no. 3: 1216. https://doi.org/10.3390/jcm12031216
APA StyleKwisda, S., Imiolczyk, J.-P., Imiolczyk, T., Werth, M., & Scheibel, M. (2023). A Standardized Operative Protocol for Fixation of Proximal Humeral Fractures Using a Locking Plate to Minimize Surgery-Related Complications. Journal of Clinical Medicine, 12(3), 1216. https://doi.org/10.3390/jcm12031216