
Stereotactic MR-Guided Radiotherapy for Liver Metastases: First Results of the Montpellier Prospective Registry Study

 , , ,
, , ,  , ,
, ,  , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Methods and Materials
2.1. Patient Selection
2.2. Radiotherapy Planning and Delivery
2.3. Clinical Assessment, Dosimetric Evaluation and Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
3.2. Toxicities
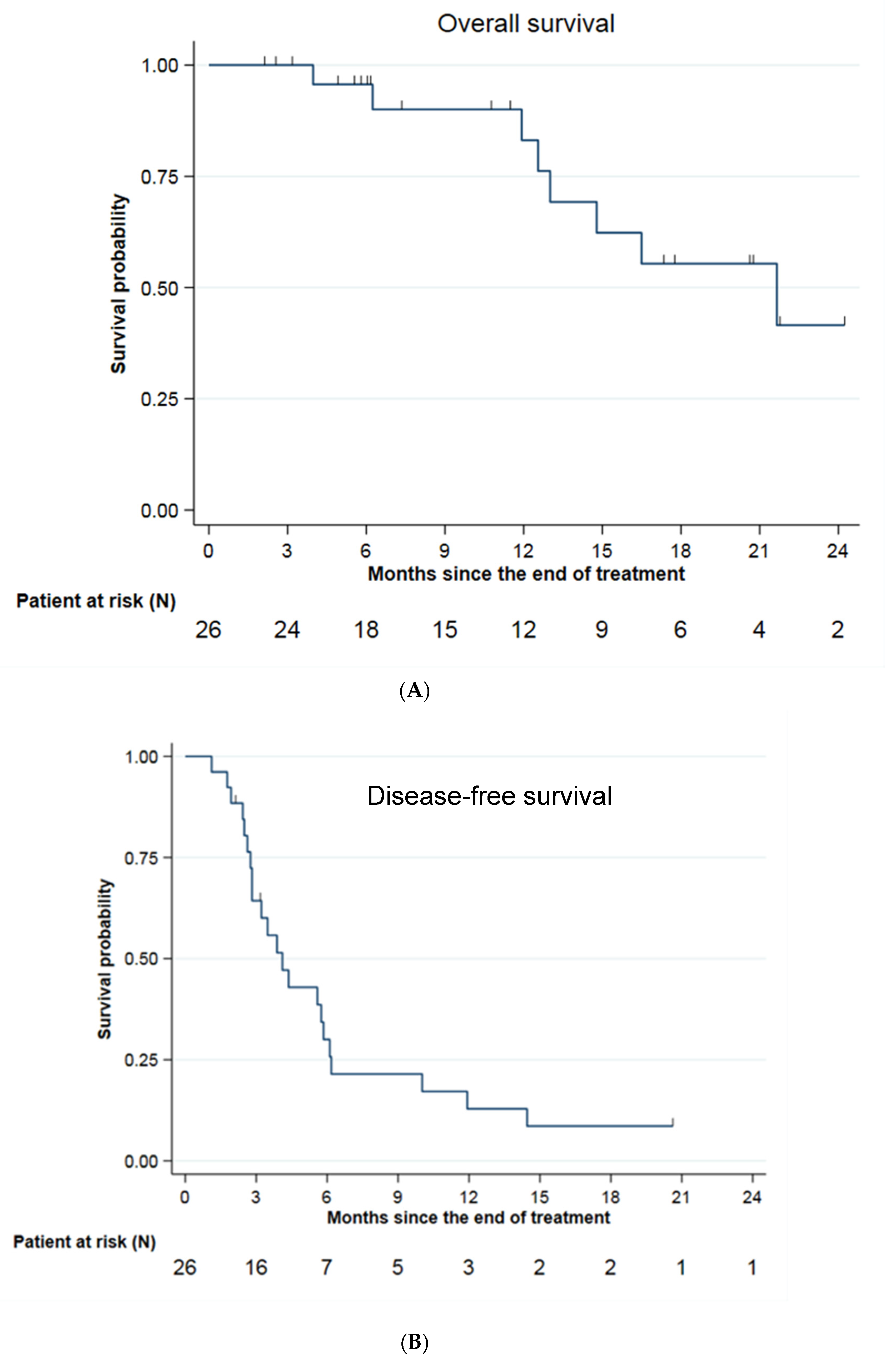
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katipally, R.R.; Pitroda, S.P.; Juloori, A.; Chmura, S.J.; Weichselbaum, R.R. The oligometastatic spectrum in the era of improved detection and modern systemic therapy. Nat. Rev. Clin. Oncol. 2022, 19, 585–599. [Google Scholar] [CrossRef]
- Kopetz, S.; Chang, G.J.; Overman, M.J.; Eng, C.; Sargent, D.; Larson, D.W.; Grothey, A.; Vauthey, J.-N.; Nagorney, D.M.; McWilliams, R.R. Improved Survival in Metastatic Colorectal Cancer Is Associated with Adoption of Hepatic Resection and Improved Chemotherapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. 2009, 27, 3677–3683. [Google Scholar] [CrossRef] [PubMed]
- Sutton, T.L.; Wong, L.H.; Walker, B.S.; Dewey, E.N.; Eil, R.; Lopez, C.D.; Kardosh, A.; Chen, E.Y.; Rocha, F.G.; Billingsley, K.G.; et al. Hepatectomy is associated with improved oncologic outcomes in recurrent colorectal liver metastases: A propensity-matched analysis. Surgery 2022, 173, S0039–S6060. [Google Scholar] [CrossRef] [PubMed]
- Vico, T.D.; Castro, P.G.; Navarro, L.A.; Sánchez, A.S.; Góngora, L.M.; Orón, E.M.M.; Ibáñez, J.M.; Alonso, N.T.; Arrillaga, I.G.P.; Trancón, J.E.G. Two stage hepatectomy (TSH) versus ALPPS for initially unresectable colorectal liver metastases: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2022, 49, S0748–S7983. [Google Scholar]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]
- Cervantes, A.; Adam, R.; Roselló, S.; Arnold, D.; Normanno, N.; Taïeb, J.; Seligmann, J.; De Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 34, 10–32. [Google Scholar] [CrossRef]
- MR Linac Radiotherapy—A New Personalized Treatment Approach. In Advances in Magnetic Resonance Technology and Applications; Elsevier: Amsterdam, The Netherlands, 2022; Volume 8, Available online: https://linkinghub.elsevier.com/retrieve/pii/C20210005770 (accessed on 4 January 2023).
- Brandner, E.D.; Wu, A.; Chen, H.; Heron, D.; Kalnicki, S.; Komanduri, K.; Gerszten, K.; Burton, S.; Ahmed, I.; Shou, Z. Abdominal organ motion measured using 4D CT. Int. J. Radiat. Oncol. 2006, 65, 554–560. [Google Scholar] [CrossRef]
- Bordeau, K.; Michalet, M.; Keskes, A.; Valdenaire, S.; Debuire, P.; Cantaloube, M.; Cabaillé, M.; Portales, F.; Draghici, R.; Ychou, M.; et al. Stereotactic MR-Guided Adaptive Radiotherapy for Pancreatic Tumors: Updated Results of the Montpellier Prospective Registry Study. Cancers 2023, 15, 7. [Google Scholar] [CrossRef]
- Michalet, M.; Bettaïeb, O.; Khalfi, S.; Ghorbel, A.; Valdenaire, S.; Debuire, P.; Aillères, N.; Draghici, R.; Bellefon, M.D.M.D.; Charissoux, M.; et al. Stereotactic MR-Guided Radiotherapy for Adrenal Gland Metastases: First Clinical Results. J. Clin. Med. 2022, 12, 291. [Google Scholar] [CrossRef]
- Bordeau, K.; Michalet, M.; Keskes, A.; Debrigode, C.; Azria, D.; Riou, O. Stereotactic body radiotherapy of primary liver tumours: Indications and new techniques. Cancer Radiother. J. Soc. Francaise Radiother. Oncol. 2022, 26, 851–857. [Google Scholar]
- Rogowski, P.; von Bestenbostel, R.; Walter, F.; Straub, K.; Nierer, L.; Kurz, C.; Landry, G.; Reiner, M.; Auernhammer, C.; Belka, C.; et al. Feasibility and Early Clinical Experience of Online Adaptive MR-Guided Radiotherapy of Liver Tumors. Cancers 2021, 13, 1523. [Google Scholar] [CrossRef] [PubMed]
- Ugurluer, G.; Mustafayev, T.Z.; Gungor, G.; Atalar, B.; Abacioglu, U.; Sengoz, M.; Agaoglu, F.; Demir, G.; Ozyar, E. Stereotactic MR-guided online adaptive radiation therapy (SMART) for the treatment of liver metastases in oligometastatic patients: Initial clinical experience. Radiat. Oncol. J. 2021, 39, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Michalet, M.; Bordeau, K.; Cantaloube, M.; Valdenaire, S.; Debuire, P.; Simeon, S.; Portales, F.; Draghici, R.; Ychou, M.; Assenat, E.; et al. Stereotactic MR-Guided Radiotherapy for Pancreatic Tumors: Dosimetric Benefit of Adaptation and First Clinical Results in a Prospective Registry Study. Front. Oncol. 2022, 12, 842402. [Google Scholar] [CrossRef] [PubMed]
- Mittauer, K.E.; Hill, P.M.; Bassetti, M.F.; Bayouth, J.E. Validation of an MR-guided online adaptive radiotherapy (MRgoART) program: Deformation accuracy in a heterogeneous, deformable, anthropomorphic phantom. Radiother. Oncol. 2020, 146, 97–109. [Google Scholar] [CrossRef]
- Rosenberg, S.A.; Henke, L.E.; Shaverdian, N.; Mittauer, K.; Wojcieszynski, A.P.; Hullett, C.R.; Kamrava, M.; Lamb, J.; Cao, M.; Green, O.L.; et al. A Multi-Institutional Experience of MR-Guided Liver Stereotactic Body Radiation Therapy. Adv. Radiat. Oncol. 2019, 4, 142–149. [Google Scholar] [CrossRef]
- Hoegen, P.; Zhang, K.S.; Tonndorf-Martini, E.; Weykamp, F.; Regnery, S.; Naumann, P.; Lang, K.; Ristau, J.; Körber, S.A.; Dreher, C.; et al. MR-guided adaptive versus ITV-based stereotactic body radiotherapy for hepatic metastases (MAESTRO): A randomized controlled phase II trial. Radiat. Oncol. 2022, 17, 59. [Google Scholar] [CrossRef]
- Weykamp, F.; Hoegen, P.; Klüter, S.; Spindeldreier, C.K.; König, L.; Seidensaal, K.; Regnery, S.; Liermann, J.; Rippke, C.; Koerber, S.A.; et al. Magnetic Resonance-Guided Stereotactic Body Radiotherapy of Liver Tumors: Initial Clinical Experience and Patient-Reported Outcomes. Front. Oncol. 2021, 11, 610637. [Google Scholar] [CrossRef]
- Petrelli, F.; Comito, T.; Barni, S.; Pancera, G.; Scorsetti, M.; Ghidini, A. Stereotactic body radiotherapy for colorectal cancer liver metastases: A systematic review. Radiother. Oncol. 2018, 129, 427–434. [Google Scholar] [CrossRef]
- Ohri, N.; Tomé, W.A.; Romero, A.M.; Miften, M.; Haken, R.K.T.; Dawson, L.A.; Grimm, J.; Yorke, E.; Jackson, A. Local Control After Stereotactic Body Radiation Therapy for Liver Tumors. Int. J. Radiat. Oncol. 2021, 110, 188–195. [Google Scholar] [CrossRef]
- Klement, R.J.; Abbasi-Senger, N.; Adebahr, S.; Alheid, H.; Allgaeuer, M.; Becker, G.; Blanck, O.; Boda-Heggemann, J.; Brunner, T.; Duma, M.; et al. The impact of local control on overall survival after stereotactic body radiotherapy for liver and lung metastases from colorectal cancer: A combined analysis of 388 patients with 500 metastases. BMC Cancer 2019, 1, 173. [Google Scholar] [CrossRef]
- Ahmed, K.A.; Fulp, W.J.; Berglund, A.E.; Hoffe, S.E.; Dilling, T.J.; Eschrich, S.A.; Shridhar, R.; Torres-Roca, J.F. Differences Between Colon Cancer Primaries and Metastases Using a Molecular Assay for Tumor Radiation Sensitivity Suggest Implications for Potential Oligometastatic SBRT Patient Selection. Int. J. Radiat. Oncol. 2015, 92, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.A.; Caudell, J.J.; El-Haddad, G.; Berglund, A.E.; Welsh, E.A.; Yue, B.; Hoffe, S.E.; Naghavi, A.O.; Abuodeh, Y.A.; Frakes, J.M.; et al. Radiosensitivity Differences Between Liver Metastases Based on Primary Histology Suggest Implications for Clinical Outcomes After Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. 2016, 95, 1399–1404. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | |
|---|---|
| Women | 13 (50.0%) |
| Men | 13 (50.0%) |
| Median age (range) | 68.5 (45.0; 89.0) |
| Number of lesions | |
| 1 2 | 21 (80.8%) 5 (19.2%) |
| Primary cancer | |
| NSCLC Colorectal Pancreas Ovary Sarcoma Breast Esophagus Kidney | 2 (7.7%) 11 (42.3%) 6 (23.1%) 1 (3.8%) 1 (3.8%) 3 (11.5%) 1 (3.8%) 1 (3.8%) |
| Number of previous liver local treatments | |
| 0 1 2 | 3 (11.5%) 9 (34.6%) 14 (53.8%) |
| ECOG score | |
| 0 1 2 | 12 (46.2%) 10 (38.5%) 4 (15.4%) |
| Previous treatment | |
| RFA Liver surgery Electroporation Chemotherapy Radiotherapy TACE ICI Targeted therapy | 4 (17.4%) 9 (39.1%) 2 (8.7%) 20 (87.0%) 3 (13.0%) 1 (4.3%) 1 (4.3%) 6 (26.1%) |
| Localization | |
| Left liver Segment 4 Segment 1 Right liver | 5 (16.1%) 9 (29.0%) 2 (6.5%) 15 (48.4%) |
| Characteristics | Number of Lesions (%) or Median Value (Min–Max) |
|---|---|
| Total Dose (Gy) | |
| 60 50 40 35 30 | 2 (6.5%) 3 (9.7%) 1 (3.2%) 17 (54.8%) 8 (25.8%) |
| Total treatment duration (days) | 5.0 (5.0–29.0) |
| Fraction dose (Gy) | 10 (8–12) |
| Median PTV (cm3) | 35.6 (9.9–343.2) |
| Median liver volume (cm3) | 1372.3 (676.9–2158.5) |
| Fraction duration (minutes) | 82.6 (52–133) |
| PTV | |
| V95% (%) V100% (%) D95% (Gy) D1cc (Gy) | 95.9 (71.6–98.9) 50.0 (49.2–90.8) 47.5 (26.9–58.0) 52.0 (41.2–63.1)) |
| Kidney | |
| V18 Gy (cm3) | 0.0 (0.0–0.4) |
| Spinal Cord | |
| Dmax (Gy) | 6.9 (0.7–20.3) |
| Stomach | |
| Dmax (Gy) | 17.1 (0.4–31.5) |
| Duodenum | |
| Dmax (Gy) | 11.4 (0.0–27.4) |
| Small intestine | |
| Dmax (Gy) | 3.5 (0.0–29.0) |
| Large intestine | |
| Dmax (Gy) | 12.5 (0.3–31.8) |
| Esophagus | |
| Dmax (Gy) | 6.5 (0.0–23.9) |
| Heart | |
| Dmax (Gy) | 23.0 (0.7–38.0) |
| Liver | |
| Mean dose V15 Gy (cm3) | 8.5 (3.7–19.1) 342.2 (63.5–774.2) |
| CTCAE v5.0 | Acute Toxicity (0–90 Days) (26 Patients) | Late Toxicity (90 Days–1 Year) (22 Patients) |
|---|---|---|
| Abdominal pain | ||
| g0 g1 g2 | 22 (84.8%) 2 (7.6%) 2 (7.6%) | 14 (63.6%) 3 (13.6%) 5 (22.8%) |
| Nausea/Vomiting | ||
| g0 g1 g2 | 17 (69.3%) 7 (26.9%) 1 (3.8%) | 19 (86.3%) 2 (9.1%) 1 (4.6%) |
| Gastro-Duodenal ulcer | ||
| g0 g1 | 26 (100%) 0 (0%) | 21 (95.4%) 1 (4.6%) |
| Parietal pain | ||
| g0 g1 g2 | 22 (84.8%) 3 (11.4%) 1 (3.8%) | 22 (100%) 0 (0%) 0 (0%) |
| Diarrhea | ||
| g0 g1 g2 | 24 (92.3%) 2 (7.7%) 0 (0%) | 18 (81.8%) 2 (9.1%) 2 (9.1%) |
| Ascites | ||
| g0 | 26 (100%) | 22 (100%) |
| Biological hepatic cytolysis | ||
| g0 g1 g2 | 25 (96.2%) 1 (3.2%) 0 (0%) | 16 (72.7%) 6 (27.3%) 0 (0%) |
| Other gastrointestinal and hepatobiliary events | ||
| Angiocholitis (g3) Angiocholitis (g4) Bile duct stenosis (g4) | 1 (3.8%) 1 (3.8%) 0 (0%) | 2 (9.1%) 0 (0%) 1 (4.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bordeau, K.; Michalet, M.; Keskes, A.; Valdenaire, S.; Debuire, P.; Cantaloube, M.; Cabaillé, M.; Jacot, W.; Draghici, R.; Demontoy, S.; et al. Stereotactic MR-Guided Radiotherapy for Liver Metastases: First Results of the Montpellier Prospective Registry Study. J. Clin. Med. 2023, 12, 1183. https://doi.org/10.3390/jcm12031183
Bordeau K, Michalet M, Keskes A, Valdenaire S, Debuire P, Cantaloube M, Cabaillé M, Jacot W, Draghici R, Demontoy S, et al. Stereotactic MR-Guided Radiotherapy for Liver Metastases: First Results of the Montpellier Prospective Registry Study. Journal of Clinical Medicine. 2023; 12(3):1183. https://doi.org/10.3390/jcm12031183
Chicago/Turabian StyleBordeau, Karl, Morgan Michalet, Aïcha Keskes, Simon Valdenaire, Pierre Debuire, Marie Cantaloube, Morgane Cabaillé, William Jacot, Roxana Draghici, Sylvain Demontoy, and et al. 2023. "Stereotactic MR-Guided Radiotherapy for Liver Metastases: First Results of the Montpellier Prospective Registry Study" Journal of Clinical Medicine 12, no. 3: 1183. https://doi.org/10.3390/jcm12031183
APA StyleBordeau, K., Michalet, M., Keskes, A., Valdenaire, S., Debuire, P., Cantaloube, M., Cabaillé, M., Jacot, W., Draghici, R., Demontoy, S., Quantin, X., Ychou, M., Assenat, E., Mazard, T., Gauthier, L., Dupuy, M., Guiu, B., Bourgier, C., Aillères, N., ... Riou, O. (2023). Stereotactic MR-Guided Radiotherapy for Liver Metastases: First Results of the Montpellier Prospective Registry Study. Journal of Clinical Medicine, 12(3), 1183. https://doi.org/10.3390/jcm12031183