
Comparative Cardiac Magnetic Resonance-Based Feature Tracking and Deep-Learning Strain Assessment in Patients Hospitalized for Acute Myocarditis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Acquisition and Post-Processing of CMR Imaging
2.3. Statistical Analysis
3. Results
3.1. Study Population
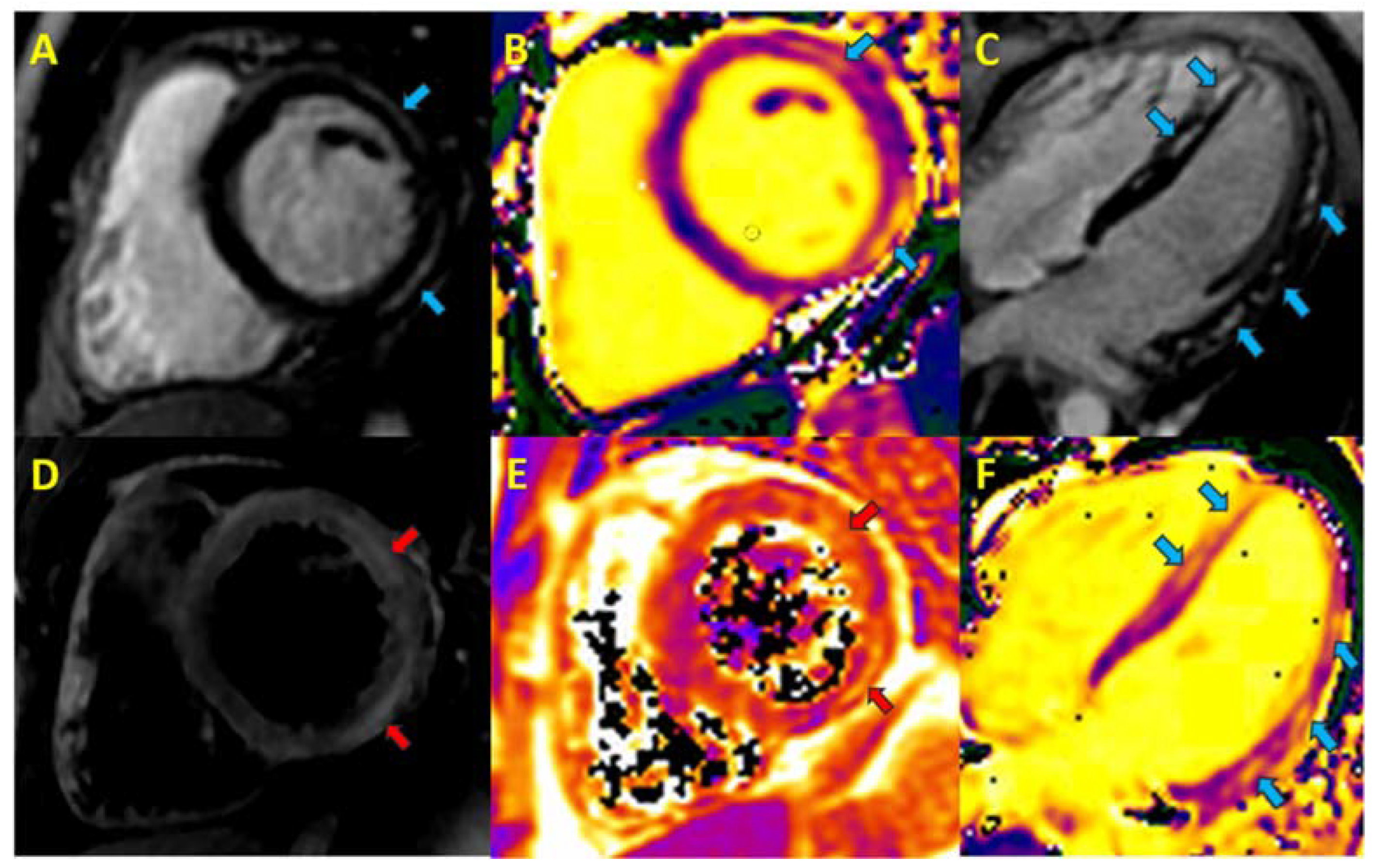
3.2. Cardiac Magnetic Resonance Imaging
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACE | Angiotensin-converting enzyme |
| AUC | Area under the curve |
| CMRc | Cardiac magnetic resonance, control |
| CMRf | Cardiac magnetic resonance, follow-up |
| CT | Computed tomography |
| DLSc | Circumferential deep learning-based strain |
| ECV | Extracellular volume |
| FTc | Circumferential feature tracking |
| ICC | Intraclass correlation coefficient |
| IR | Inversion recovery |
| LGE | Late gadolinium enhancement |
| LVEF | Left ventricular ejection fraction |
| RVEF | Right ventricular ejection fraction |
| ROI | Region of interest |
| STIR | Short tau inversion recovery |
References
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kuhl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the european society of cardiology working group on myocardial and pericardial diseases. Eur. Heart J. 2007, 29, 270–276. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Pinto, Y.M.; Elliott, P.M.; Arbustini, E.; Adler, Y.; Anastasakis, A.; Böhm, M.; Duboc, D.; Gimeno, J.; De Groote, P.; Imazio, M.; et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: A position statement of the ESC working group on myocardial and pericardial diseases. Eur. Heart J. 2016, 37, 1850–1858. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yang, W.; Zhao, S.; Lu, M. State-of-the-art myocardial strain by CMR feature tracking: Clinical applications and future perspectives. Eur. Radiol. 2022, 32, 5424–5435. [Google Scholar] [CrossRef] [PubMed]
- Claus, P.; Omar, A.M.S.; Pedrizzetti, G.; Sengupta, P.P.; Nagel, E. Tissue Tracking Technology for Assessing Cardiac Mechanics: Principles, Normal Values, and Clinical Applications. JACC Cardiovasc. Imaging 2015, 8, 1444–1460. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Petry, P.; Kuetting, D.; Dabir, D.; Schmeel, F.C.; Homsi, R.; Schild, H.H.; Thomas, D. Left and right ventricular strain in the course of acute myocarditis: A cardiovascular magnetic resonance study. Rofo 2018, 190, 722–732. [Google Scholar] [CrossRef]
- Secchi, F.M.; Monti, C.B.; Alì, M.; Carbone, F.S.; Cannaò, P.M.; Sardanelli, F. Diagnostic Value of Global Cardiac Strain in Patients With Myocarditis. J. Comput. Assist. Tomogr. 2020, 44, 591–598. [Google Scholar] [CrossRef]
- Gatti, M.; Palmisano, A.; Faletti, R.; Benedetti, G.; Bergamasco, L.; Bioletto, F.; Peretto, G.; Sala, S.; De Cobelli, F.; Fonio, P.; et al. Two-dimensional and three-dimensional cardiac magnetic resonance feature-tracking myocardial strain analysis in acute myocarditis patients with preserved ejection fraction. Int. J. Cardiovasc. Imaging 2019, 35, 1101–1109. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Homsi, R.; Dabir, D.; Kuetting, D.L.; Marx, C.; Doerner, J.; Schlesinger-Irsch, U.; Andrié, R.; Sprinkart, A.M.; Schmeel, F.C.; et al. Comprehensive Cardiac Magnetic Resonance for Short-Term Follow-Up in Acute Myocarditis. J. Am. Heart Assoc. 2016, 5, e003603. [Google Scholar] [CrossRef]
- Porcari, A.; Merlo, M.; Crosera, L.; Stolfo, D.; Barbati, G.; Biondi, F.; De Angelis, G.; Paldino, A.; Pagnan, L.; Belgrano, M.; et al. Strain analysis reveals subtle systolic dysfunction in confirmed and suspected myocarditis with normal LVEF. A cardiac magnetic resonance study. Clin. Res. Cardiol. 2020, 109, 869–880. [Google Scholar] [CrossRef]
- Ravesh, M.S.; Eden, M.; Langguth, P.; Piesch, T.-C.; Lehmann, J.K.; Lebenatus, A.; Hauttemann, D.; Graessner, J.; Frey, N.; Jansen, O.; et al. Non-contrast enhanced diagnosis of acute myocarditis based on the 17-segment heart model using 2D-feature tracking magnetic resonance imaging. Magn. Reson. Imaging 2020, 65, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhu, H.; Yang, Z.; Tang, D.; Huang, L.; Xia, L. Tissue Characterization by Mapping and Strain Cardiac MRI to Evaluate Myocardial Inflammation in Fulminant Myocarditis. J. Magn. Reson. Imaging 2020, 52, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hu, H.; Pan, J.; Shu, J.; Hu, Y.; Yu, R. Performance of cardiovascular magnetic resonance strain in patients with acute myocarditis. Cardiovasc. Diagn. Ther. 2020, 10, 725–737. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, J.U.; Osinalde, E.P.; Rodríguez-Hernández, J.L.; Fernández, H.M.; Islas, F.; de Agustín, A.; Marcos-Alberca, P.; Mahía, P.; Cobos, M.; Mateo, P.H.; et al. Myocardial strain in nonischemic dilated cardiomyopathy with feature tracking. Feasibility and prognostic implications. Rev. Española Cardiol. (Engl. Ed. ) 2021, 74, 159–166. [Google Scholar] [CrossRef]
- Ulloa, J.U.; de Vega, V.M.; Montañés, O.S.; Vázquez, A.; Sánchez-Enrique, C.; Jiménez, S.H.; García, F.D.S.; Ruiz, L.L.; Rodríguez, M.R.; Pizarro, G.; et al. Cardiac magnetic resonance in recovering COVID-19 patients. Feature tracking and mapping analysis to detect persistent myocardial involvement. IJC Heart Vasc. 2021, 36, 100854. [Google Scholar] [CrossRef]
- Chen, Y.; Sun, Z.; Xu, L.; Liu, J.; Li, Y.; Zhang, N.; Liu, D.; Wen, Z. Diagnostic and Prognostic Value of Cardiac Magnetic Resonance Strain in Suspected Myocarditis With Preserved LV-EF: A Comparison Between Patients With Negative and Positive Late Gadolinium Enhancement Findings. J. Magn. Reson. Imaging 2022, 55, 1109–1119. [Google Scholar] [CrossRef]
- Fischer, K.; Obrist, S.J.; Erne, S.A.; Stark, A.W.; Marggraf, M.; Kaneko, K.; Guensch, D.P.; Huber, A.T.; Greulich, S.; Aghayev, A.; et al. Feature Tracking Myocardial Strain Incrementally Improves Prognostication in Myocarditis Beyond Traditional CMR Imaging Features. JACC Cardiovasc. Imaging 2020, 13, 1891–1901. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Schlesinger-Irsch, U.; Kuetting, D.L.; Dabir, D.; Homsi, R.; Doerner, J.; Schmeel, F.C.; Fimmers, R.; Sprinkart, A.M.; Naehle, C.P.; et al. Feature-tracking myocardial strain analysis in acute myocarditis: Diagnostic value and association with myocardial oedema. Eur. Radiol. 2017, 27, 4661–4671. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Kokkinidis, D.G.; Kampaktsis, P.N.; Amir, E.A.; Marwick, T.H.; Gupta, D.; Thavendiranathan, P. Assessment of prognostic value of left ventricular global longitudinal strain for early prediction of chemotherapy-induced cardiotoxicity: A systematic review and meta-analysis. JAMA Cardiol. 2019, 4, 1007–1018. [Google Scholar] [CrossRef]
- Baeßler, B.; Schaarschmidt, F.; Dick, A.; Michels, G.; Maintz, D.; Bunck, A.C. Diagnostic implications of magnetic resonance feature tracking derived myocardial strain parameters in acute myocarditis. Eur. J. Radiol. 2016, 85, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Augustine, D.; Lewandowski, A.J.; Lazdam, M.; Rai, A.; Francis, J.; Myerson, S.; Noble, A.; Becher, H.; Neubauer, S.; Petersen, S.E.; et al. Global and regional left ventricular myocardial deformation measures by magnetic resonance feature tracking in healthy volunteers: Comparison with tagging and relevance of gender. J. Cardiovasc. Magn. Reson. 2013, 15, 8. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Myocarditis Patients | Healthy Group |
|---|---|---|
| Age (mean ± SD), years | 37 ± 17 | 44 ± 10 |
| Body mass index (Kg/m2) | 25 ± 4 | 25 ± 3 |
| Male | 15/17 (88.2%) | 7/20 (35%) |
| Hypertension | 2/17 (11.8%) | 2/20 (10%) |
| Diabetes | 0/17 (0%) | 0/20 (0%) |
| Dyslipidemia | 2/17 (11.8%) | 6/20 (30%) |
| Clinical presentation: | ||
| - Asymptomatic | 0/17 (0%) | 0/20 (0%) |
| - Fever and chest pain | 9/17 (52.9%) | 0/20 (0%) |
| - Chest pain | 8/17 (47.1%) | |
| ECG: | ||
| - Normal | 1/17 (5.9%) | 20/20 (100%) |
| - ST segment alterations | 11/17 (64.7%) | |
| - Q pathological | 1/17 (5.9%) | |
| - T negative | 2/17 (11.8%) | |
| - Right bundle branch block | 2/17 (11.8%) | |
| Analytical parameters: | ||
| - Fibrinogen (mg/dL) | 626.3 ± 145.9 | N/A |
| - Ferritin (ng/mL) | 160.4 ± 123.5 | |
| - Leukocytes (109/L cells per liter) | 8.7 ± 2.4 | |
| - CRP (mg/dL) | 0.98 [0.62–4.08] | |
| - Troponin T (ng/mL) | 972 ± 690 | |
| Coronary study: | ||
| - Not performed | 7/17 (41.2%) | N/A |
| - Normal CT angiography | 4/17 (23.5%) | |
| - Normal cardiac catheterization | 6/17 (35.3%) | |
| Treatment: | ||
| - Beta-blockers | 7/17 (41.2%) | N/A |
| - ACE inhibitors | 8/17 (47%) |
| CMR Findings | CMRd | CRMf | p |
|---|---|---|---|
| LGE pattern: | |||
| - Lateral subepicardial | 7/17 (41.2%) | ||
| - Septal subepicardial | 2/17 (11.8%) | N/A | |
| - Lateral/septal subepicardial | 4/17 (23.5%) | ||
| - Ring-like pattern | 3/17 (17.7%) | ||
| LVEF (%) | 55 ± 6 | 59 ± 4 | 0.008 |
| RVEF (%) | 55 ± 6 | 57 ± 4 | 0.113 |
| LGE quantification (%) | 8 [5–12] | 3 [2–5] | 0.001 |
| Mapping: | |||
| - T1-native myocardial (msec) | 1083 ± 72 | 976 ± 20 | 0.008 |
| - Extracellular volume (%) | 30 ± 2% | 25 ± 2% | <0.001 |
| - T2-mapping (msec) | 61 [57–68] | 49 [47–51] | 0.003 |
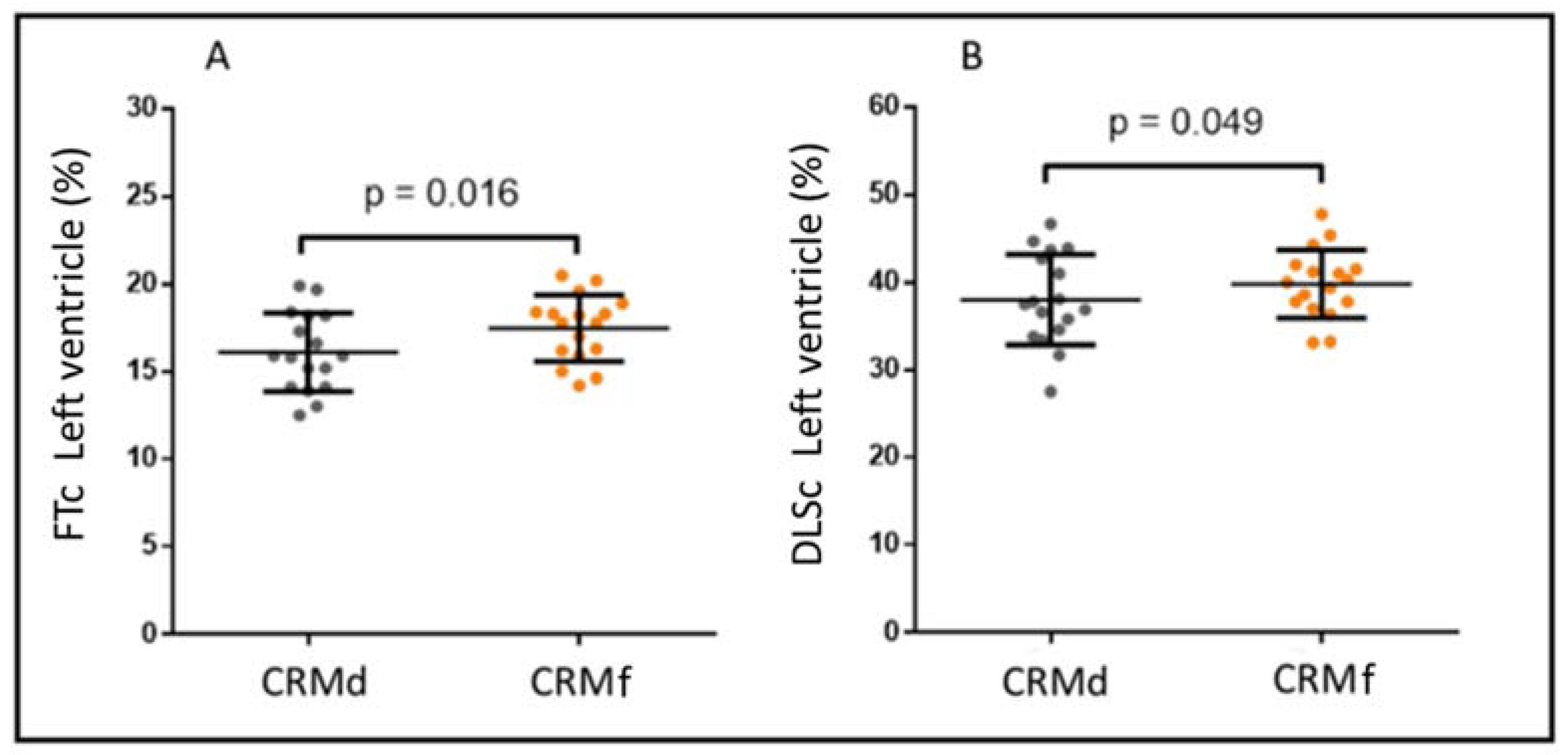
| FTc (%) | −16.1 ± 2.2 | −17.5 ± 1.9 | 0.016 |
| DLSc (%) | −38.1 ± 5.2 | −39.8 ± 3.9 | 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urmeneta Ulloa, J.; Martínez de Vega, V.; Álvarez Vázquez, A.; Andreu-Vázquez, C.; Thuissard-Vasallo, I.J.; Recio Rodríguez, M.; Pizarro, G.; Cabrera, J.Á. Comparative Cardiac Magnetic Resonance-Based Feature Tracking and Deep-Learning Strain Assessment in Patients Hospitalized for Acute Myocarditis. J. Clin. Med. 2023, 12, 1113. https://doi.org/10.3390/jcm12031113
Urmeneta Ulloa J, Martínez de Vega V, Álvarez Vázquez A, Andreu-Vázquez C, Thuissard-Vasallo IJ, Recio Rodríguez M, Pizarro G, Cabrera JÁ. Comparative Cardiac Magnetic Resonance-Based Feature Tracking and Deep-Learning Strain Assessment in Patients Hospitalized for Acute Myocarditis. Journal of Clinical Medicine. 2023; 12(3):1113. https://doi.org/10.3390/jcm12031113
Chicago/Turabian StyleUrmeneta Ulloa, Javier, Vicente Martínez de Vega, Ana Álvarez Vázquez, Cristina Andreu-Vázquez, Israel John Thuissard-Vasallo, Manuel Recio Rodríguez, Gonzalo Pizarro, and José Ángel Cabrera. 2023. "Comparative Cardiac Magnetic Resonance-Based Feature Tracking and Deep-Learning Strain Assessment in Patients Hospitalized for Acute Myocarditis" Journal of Clinical Medicine 12, no. 3: 1113. https://doi.org/10.3390/jcm12031113
APA StyleUrmeneta Ulloa, J., Martínez de Vega, V., Álvarez Vázquez, A., Andreu-Vázquez, C., Thuissard-Vasallo, I. J., Recio Rodríguez, M., Pizarro, G., & Cabrera, J. Á. (2023). Comparative Cardiac Magnetic Resonance-Based Feature Tracking and Deep-Learning Strain Assessment in Patients Hospitalized for Acute Myocarditis. Journal of Clinical Medicine, 12(3), 1113. https://doi.org/10.3390/jcm12031113