
Female Sexual Dysfunction in Association with Sexual History, Sexual Abuse and Satisfaction: A Cross-Sectional Study in Hungary


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
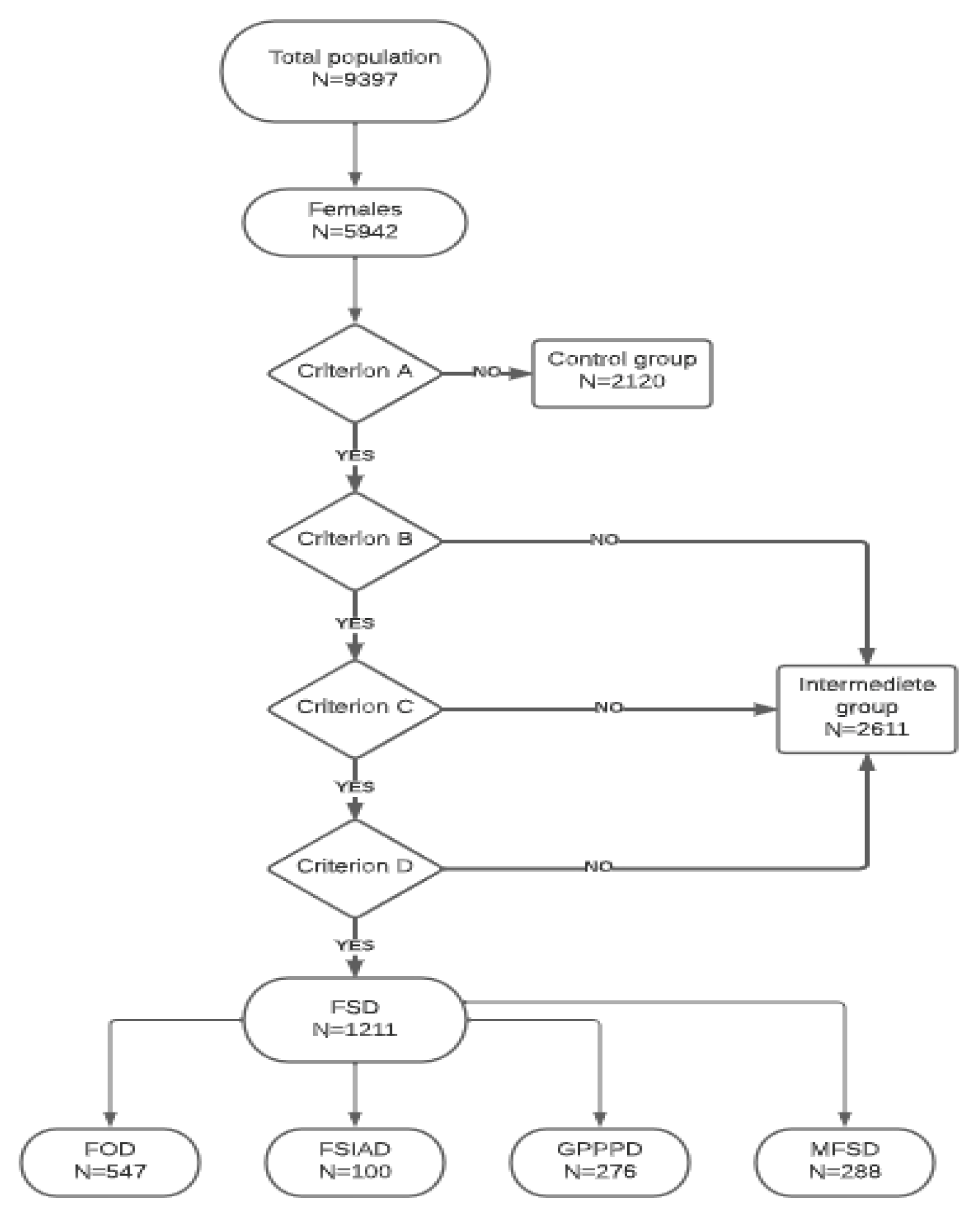
2.1.1. Transformation of the DSM-5 Criteria into Online Questions
2.1.2. Variables
- Sexual history was measured by four questions: (1) the satisfaction with the first sexual experience (evaluated by a 1 to 10 scale: 1 = very bad, 10 = very good); (2) previous sexual education (yes–no); (3) the age at the first encounter with pornographic content (age in years); (4) the lifetime prevalence of sexually transmitted diseases (STD) (yes–no).
- Sexual orientation was measured by four categories: heterosexual, homosexual, bisexual, and asexual.
- The sexual self-esteem of women was evaluated by three questions: (1) satisfaction with their own body image (e.g., body weight, height, abdominal circumference, shoulder or waist width, and face); (2) satisfaction with their own genitalia, (3) satisfaction with their own sexual attraction. All three questions were answered on a 1 to 10 scale:1 = not at all satisfied, 10 = completely satisfied.
2.2. Statistical Analysis
3. Results
3.1. Factors Associated with FOD
3.2. Factors Associated with FSIAD
3.3. Factors Associated with GPPPD
3.4. Factors Associated with MFSD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Khajehei, M.; Doherty, M.; Tilley, P.J. An update on sexual function and dysfunction in women. Arch. Womens Ment. Health 2015, 18, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, I.; Kim, N.N.; Clayton, A.H.; DeRogatis, L.R.; Giraldi AParish, S.J.; Pfaus, J.; Simon, J.A.; Kingsberg, S.A.; Meston, C.; Stahl, S.M.; et al. Hypoactive Sexual Desire Disorder: International Society for the Study of Women’s Sexual Health (ISSWSH) Expert Consensus Panel Review. Mayo Clin. Proc. 2017, 92, 114–128. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, K.R.; Hughan, C.P.; Meston, C.M. Childhood sexual abuse moderates the association between sexual functioning and sexual distress in women. Child. Abuse Negl. 2012, 36, 180–189. [Google Scholar] [CrossRef]
- Wallwiener, S.; Strohmaier, J.; Wallwiener, L.M.; Schönfisch, B.; Zipfel, S.; Brucker, S.Y.; Rietschel, M.; Wallwiener, C.W. Sexual Function Is Correlated With Body Image and Partnership Quality in Female University Students. J. Sex. Med. 2016, 13, 1530–1538. [Google Scholar] [CrossRef]
- Reissing, E.D.; Binik, Y.M.; Khalifé, S.; Cohen, D.; Amsel, R. Etiological correlates of vaginismus: Sexual and physical abuse, sexual knowledge, sexual self-schema, and relationship adjustment. J. Sex. Marital. Ther. 2003, 29, 47–59. [Google Scholar] [CrossRef]
- Pazmany, E.; Bergeron, S.; Van Oudenhove, L.; Verhaeghe, J.; Enzlin, P. Aspects of sexual self-schema in premenopausal women with dyspareunia: Associations with pain, sexual function, and sexual distress. J. Sex. Med. 2013, 10, 2255–2264. [Google Scholar] [CrossRef]
- Stephenson, K.R.; Meston, C.M. Why is impaired sexual function distressing to women? The primacy of pleasure in female sexual dysfunction. J. Sex. Med. 2015, 12, 728–737. [Google Scholar] [CrossRef]
- Safarinejad, M.R. Female sexual dysfunction in a population-based study in Iran: Prevalence and associated risk factors. Int. J. Impot. Res. 2006, 18, 382–395. [Google Scholar] [CrossRef]
- Brassil, D.F.; Keller, M. Female sexual dysfunction: Definitions, causes, and treatment. Urol. Nurs. 2002, 22, 237–244. [Google Scholar]
- McCabe, M.P.; Sharlip, I.D.; Lewis, R.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Lee, S.W.; Segraves, R.T. Incidence and Prevalence of Sexual Dysfunction in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015. J. Sex. Med. 2016, 13, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, A.; Laumann, E.O.; Glasser, D.B.; Moreira, E.D., Jr.; Paik, A.; Gingell, C. Global Study of Sexual Attitudes and Behaviors Investigators’ Group. Sexual behavior and sexual dysfunctions after age 40: The global study of sexual attitudes and behaviors. Urology 2004, 64, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Starc, A.; Jukić, T.; Poljšak, B.; Dahmane, R. Female Sexual Function and Dysfunction: A Cross-National Prevalence Study in Slovenia. Acta Clin. Croat. 2018, 57, 52–60. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; pp. 429–440. [Google Scholar]
- Clayton, A.H.; Valladares Juarez, E.M. Female Sexual Dysfunction. Med. Clin. N. Am. 2019, 103, 681–698. [Google Scholar] [CrossRef]
- Fugl-Meyer, K.S.; Oberg, K.; Lundberg, P.O.; Lewin, B.; Fugl-Meyer, A. On orgasm, sexual techniques, and erotic perceptions in 18- to 74-year-old Swedish women. J. Sex. Med. 2006, 3, 56–68. [Google Scholar] [CrossRef]
- Laumann, E.O.; Nicolosi, A.; Glasser, D.B.; Paik, A.; Gingell, C.; Moreira, E.; Wang, T.; GSSAB Investigators’ Group. Sexual problems among women and men aged 40-80 y: Prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int. J. Impot. Res. 2005, 17, 39–57. [Google Scholar] [CrossRef]
- Laumann, E.O.; Paik, A.; Rosen, R.C. Sexual dysfunction in the United States: Prevalence and predictors. JAMA 1999, 281, 537–544. [Google Scholar] [CrossRef]
- Lewis, R.W.; Fugl-Meyer, K.S.; Bosch, R.; Fugl-Meyer, A.R.; Laumann, E.O.; Lizza, E.; Martin-Morales, A. Epidemiology/risk factors of sexual dysfunction. J. Sex. Med. 2004, 1, 35–39. [Google Scholar] [CrossRef]
- Hayes, R.D.; Bennett, C.M.; Fairley, C.K.; Dennerstein, L. What can prevalence studies tell us about female sexual difficulty and dysfunction? J. Sex. Med. 2006, 3, 589–595. [Google Scholar] [CrossRef]
- Latthe, P.; Latthe, M.; Say, L.; Gülmezoglu, M.; Khan, K.S. WHO systematic review of prevalence of chronic pelvic pain: A neglected reproductive health morbidity. BMC Public Health 2006, 6, 177. [Google Scholar] [CrossRef]
- Peixoto, M.M.; Nobre, P. Prevalence and sociodemographic predictors of sexual problems in Portugal: A population-based study with women aged 18 to 79 years. J. Sex. Marital Ther. 2015, 41, 69–80. [Google Scholar] [CrossRef]
- Smith, A.M.; Lyons, A.; Ferris, J.A.; Richters, J.; Pitts, M.K.; Shelley, J.M.; Simpson, J.M.; Heywood, W.; Patrick, K. Incidence and persistence/recurrence of women’s sexual difficulties: Findings from the Australian Longitudinal Study of Health and Relationships. J. Sex. Marital Ther. 2012, 38, 378–393. [Google Scholar] [CrossRef] [PubMed]
- Barlow, D.H.; Cardozo, L.D.; Francis, R.M.; Griffin, M.; Hart, D.M.; Stephens, E.; Sturdee, D.W. Urogenital ageing and its effect on sexual health in older British women. Br. J. Obstet. Gynaecol. 1997, 104, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Villeda Sandoval, C.I.; Calao-Pérez, M.; Enríquez González, A.B.; Gonzalez-Cuenca, E.; Ibarra-Saavedra, R.; Sotomayor, M.; Castillejos Molina, R.A. Orgasmic dysfunction: Prevalence and risk factors from a cohort of young females in Mexico. J. Sex. Med. 2014, 11, 1505–1511. [Google Scholar] [CrossRef]
- Graham, C.A. The DSM diagnostic criteria for female orgasmic disorder. Arch. Sex. Behav. 2010, 39, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Bleck, R.T.; Loveless, J. Human sexual malfunction: A consideration of ‘inner- mind’ thought process. Int. J. Psychosom. 1987, 34, 18–21. [Google Scholar]
- Bradford, A. Female Orgasmic Disorder: Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis. UpToDate. Available online: https://www.uptodate.com/contents/female-orgasmic-disorder-epidemiology-pathogenesis-clinical-manifestations-course-assessment-and-diagnosis (accessed on 8 November 2022).
- Rellini, A. Review of the empirical evidence for a theoretical model to understand the sexual problems of women with a history of CSA. J. Sex. Med. 2008, 5, 31–46. [Google Scholar] [CrossRef]
- Leonard, L.M.; Follette, V.M. Sexual functioning in women reporting a history of child sexual abuse: Review of the empirical literature and clinical implications. Annu. Rev. Sex. Res. 2002, 13, 346–388. [Google Scholar] [PubMed]
- Alizadeh, A.; Farnam, F.; Raisi, F.; Parsaeian, M. Prevalence of and Risk Factors for Genito-Pelvic Pain/Penetration Disorder: A Population-Based Study of Iranian Women. J. Sex. Med. 2019, 16, 1068–1077. [Google Scholar] [CrossRef]
- Mitchell, K.R.; Geary, R.; Graham, C.A.; Datta, J.; Wellings, K.; Sonnenberg, P.; Field, N.; Nunns, D.; Bancroft, J.; Jones, K.G.; et al. Painful sex (dyspareunia) in women: Prevalence and associated factors in a British population probability survey. BJOG Int. J. Obstet. Gynaecol. 2017, 124, 1689–1697. [Google Scholar] [CrossRef]
- Ramezani Tehrani, F.; Farahmand, M.; Simbar, M.; Malek Afzali, H. Factors associated with sexual dysfunction; a population based study in Iranian reproductive age women. Arch. Iran Med. 2014, 17, 679–684. [Google Scholar] [PubMed]


{kind=link}
| Characteristics | Total n = 5942 | FOD n = 547 | FSIAD n = 100 | GPPPD n = 276 | Control n = 2120 |
|---|---|---|---|---|---|
| Marital status: | |||||
| Single n (%) | 1387 (23.3) | 142 (26.0) *** | 27 (27.0) * | 50 (18.1) | 351 (28.8) |
| Friend with benefits n (%) | 492 (8.3) | 45 (8.2) *** | 6 (6.0) * | 26 (9.4) | 178 (20.2) |
| Married/partnership n (%) | 4010 (67.6) | 356 (65.2) *** | 67 (67.0) * | 196 (71.0) | 1572 (74.2) |
| In more relationships (polyamory) n (%) | 47 (0.8) | 3 (0.5) *** | 0 (0.0) * | 4 (1.4) | 17 (0.8) |
| Place of living: | |||||
| Village n (%) | 1489 (25.1) | 147 (26.9) | 29 (29.0) | 63 (22.8) | 533 (21.1) |
| City/Town n (%) | 3895 (65.6) | 341 (62.3) | 60 (60.0) | 181 (65.6) | 1404 (66.2) |
| Capital city n (%) | 1557 (9.4) | 59 (10.8) | 11 (11.0) | 32 (11.6) | 183 (8.6) |
| Sexual history: | |||||
| Sexual education n (%) | 4130 (69.5) | 350 (64.0) *** | 59 (59.0) ** | 177 (64.1) *** | 1557 (73.4) |
| STD n (%) | 846 (14.2) | 103 (18.8) *** | 16 (16.0) | 51 (18.5) * | 269 (12.7) |
| Sexual abuse n (%) | 822 (13.8) | 90 (16.5) *** | 19 (19.0) * | 54 (19.6) *** | 229 (10.8) |
| Sexual orientation | |||||
| Heterosexual n (%) | 5477 (92.2) | 499 (91.2) | 87 (87.0) * | 251 (90.9) * | 1977 (93.3) |
| Homosexual n (%) | 68 (1.1) | 4 (0.7) | 2 (2.0) * | 6 (2.2) * | 24 (1.1) |
| Bisexual n (%) | 377 (6.3) | 44 (8.0) | 10 (10.0) * | 17 (6.2) * | 118 (5.6) |
| Asexual n (%) | 19 (0.3) | 0 (0.0) | 1 (1.0) * | 2 (0.7) * | 1 (0.0) |
| Variables | Group | Mean (SD) | Median | n | Mean Rank | Sum of Ranks | U | Effect Size (r) | p (2-Tailed) |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | FOD | 22.12 (3.41) | 22.0 | 547 | 1323.55 | 723,983.50 | 574,105.500 | 0.0069 | 0.720 |
| Control | 22.26 (3.64) | 21.0 | 2120 | 1336.70 | 2,833,794.50 | ||||
| Evaluation of first sexual experience | FOD | 5.20 (2.55) | 5.0 | 520 | 1137.35 | 622,132.50 | 472,254.500 | 0.1305 | <0.001 |
| Control | 6.03 (2.55) | 6.0 | 1929 | 1384.74 | 2,935,645.50 | ||||
| Age of first pornographic content | FOD | 14.01 (3.35) | 14.0 | 547 | 1127.14 | 586,111.50 | 450,651.500 | 0.0692 | <0.001 |
| Control | 14.64 (3.07) | 15.0 | 2120 | 1251.38 | 2,413,913.50 | ||||
| Satisfaction with | |||||||||
| own sexual attraction | FOD | 6.19 (2.07) | 7.0 | 547 | 1116.35 | 610,645.50 | 460,767.500 | 0.1458 | <0.001 |
| Control | 6.92 (1.93) | 7.0 | 2120 | 1390.16 | 2,947,132.50 | ||||
| own body image | FOD | 4.84 (2.63) | 5.0 | 547 | 1117.87 | 611,474.00 | 461,596.000 | 0.1436 | <0.001 |
| Control | 5.79 (2.50) | 6.0 | 2120 | 1389.77 | 2,946,304.00 | ||||
| own genitalia | FOD | 6.73 (2.58) | 7.0 | 547 | 1020.51 | 558,217.50 | 408,339.500 | 0.2106 | <0.001 |
| Control | 7.99 (2.13) | 9.0 | 2120 | 1414.89 | 2,999,560.50 |
| Variables | Group | Mean (SD) | Median | n | Mean Rank | Sum of | U | Effect Size (r) | p (2-Tailed) |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | FSIAD | 21.67 (3.19) | 21.0 | 100 | 1026.54 | 102,654.00 | 97,604.000 | 0.0261 | 0.178 |
| Control | 22.26 (3.64) | 21.0 | 2120 | 1114.46 | 2,362,656.00 | ||||
| Evaluation of first sexual experience | FSIAD | 5.53 (2.55) | 5.0 | 90 | 985.36 | 88,682.00 | 84,587.000 | 0.0390 | 0.066 |
| Control | 6.03 (2.55) | 6.0 | 2120 | 1110.60 | 2,354,473.00 | ||||
| Age of the first pornographic content | FSIAD | 14.15 (3.35) | 14.0 | 93 | 926.52 | 86,166.00 | 81,795.000 | 0.0321 | 0.148 |
| Control | 14.64 (3.07) | 15.0 | 1929 | 1015.60 | 1,959,087.00 | ||||
| Satisfaction with | |||||||||
| own sexual attraction | FSIAD | 6.23 (2.07) | 6.0 | 100 | 897.89 | 89,788.50 | 84,738.500 | 0.0668 | <0.001 |
| Control | 6.92 (1.93) | 7.0 | 2120 | 1120.53 | 2,375,521.50 | ||||
| own body image | FSIAD | 4.79 (2.66) | 4.5 | 100 | 876.89 | 87,688.50 | 82,638.500 | 0.0727 | <0.001 |
| Control | 5.79 (2.50) | 6.0 | 2120 | 1121.52 | 2,377,621.50 | ||||
| own genitalia | FSIAD | 6.75 (2.54) | 7.0 | 100 | 779.82 | 77,982.00 | 72,932.000 | 0.1044 | <0.001 |
| Control | 7.99 (2.13) | 9.0 | 2120 | 1126.10 | 2,387,328.00 |
| Variables | Group | Mean (SD) | Median | n | Mean Rank | Sum of Ranks | U | Effect Size (r) | p (2-Tailed) |
|---|---|---|---|---|---|---|---|---|---|
| Age (18-35) | GPPPD | 22.16 (3.47) | 22.0 | 276 | 1193.78 | 329,482.50 | 291,256.500 | 0.0024 | 0.452 |
| Control | 22.26 (3.64) | 21.0 | 2120 | 1199.11 | 2,542,123.50 | ||||
| Evaluation of first sexual experience | GPPPD | 4.92 (2.73) | 5.0 | 276 | 951.94 | 262,736.50 | 224,510.500 | 0.1294 | <0.001 |
| Control | 6.03 (2.55) | 6.0 | 2120 | 1230.60 | 2,608,869.50 | ||||
| Age of the first pornographic content | GPPPD | 14.18 (3.23) | 15.0 | 251 | 1026.93 | 262,736.50 | 226,132.500 | 0.0366 | 0.087 |
| Control | 14.64 (3.07) | 15.0 | 1929 | 1098.77 | 2,119,531.50 | ||||
| Satisfaction with | |||||||||
| own sexual attraction | GPPPD | 6.03 (2.01) | 6.00 | 276 | 911.82 | 251,661.00 | 213,435.000 | 0.1518 | <0.001 |
| Control | 6.92 (1.93) | 7.00 | 2120 | 1235.82 | 2,619,945.00 | ||||
| own body image | GPPPD | 4.93 (2.45) | 5.00 | 276 | 989.14 | 273,001.50 | 234,775.500 | 0.1099 | <0.001 |
| Control | 5.79 (2.50) | 6.00 | 2120 | 1225.76 | 2,598,604.50 | ||||
| own genitalia | GPPPD | 6.78 (2.45) | 7.00 | 276 | 869.90 | 240,093.50 | 201,867.500 | 0.1748 | <0.001 |
| Control | 7.99 (2.13) | 9.00 | 2120 | 1241.28 | 2,631,512.50 |
| Variables | Group | Mean (SD) | Median | n | Mean Rank | Sum of Ranks | U | Effect Size (r) | p (2-Tailed) |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | MFSD | 22.16 (3.47) | 22.00 | 288 | 1243.62 | 358,162.50 | 294,013.500 | 0.0208 | 0.306 |
| Control | 22.26 (3.64) | 21.00 | 2120 | 1199.19 | 2,542,273.50 | ||||
| Evaluation of first sexual experience | MFSD | 4.92 (2.73) | 5.00 | 288 | 921.51 | 265,393.50 | 223,777.500 | 0.1510 | <0.001 |
| Control | 6.03 (2.55) | 6.00 | 2120 | 1242.94 | 2,635,042.50 | ||||
| Age of the first pornographic content | MFSD | 14.18 (3.23) | 15.00 | 269 | 1010.21 | 271,746.00 | 235,431.000 | 0.0528 | 0.012 |
| Control | 14.64 (3.07) | 15.00 | 1929 | 1111.95 | 2,144,955.00 | ||||
| Satisfaction with | |||||||||
| own sexual attraction | MFSD | 5.36 (2.32) | 6.00 | 288 | 786.70 | 226,570.50 | 184,954.500 | 0.2247 | <0.001 |
| Control | 6.92 (1.93) | 7.00 | 2120 | 1261.26 | 2,673,865.50 | ||||
| own body image | MFSD | 4.32 (2.72) | 5.00 | 288 | 875.71 | 252,204.50 | 210,588.500 | 0.1755 | <0.001 |
| Control | 5.79 (2.57) | 6.00 | 2120 | 1249.17 | 2,648,231.50 | ||||
| own genitalia | MFSD | 5.83 (2.71) | 7.00 | 288 | 710.51 | 204,627.00 | 163,011.000 | 0.2668 | <0.001 |
| Control | 7.99 (2.13) | 9.00 | 2120 | 1271.61 | 2,695,809.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erdős, C.; Kelemen, O.; Pócs, D.; Horváth, E.; Dudás, N.; Papp, A.; Paulik, E. Female Sexual Dysfunction in Association with Sexual History, Sexual Abuse and Satisfaction: A Cross-Sectional Study in Hungary. J. Clin. Med. 2023, 12, 1112. https://doi.org/10.3390/jcm12031112
Erdős C, Kelemen O, Pócs D, Horváth E, Dudás N, Papp A, Paulik E. Female Sexual Dysfunction in Association with Sexual History, Sexual Abuse and Satisfaction: A Cross-Sectional Study in Hungary. Journal of Clinical Medicine. 2023; 12(3):1112. https://doi.org/10.3390/jcm12031112
Chicago/Turabian StyleErdős, Csaba, Oguz Kelemen, Dávid Pócs, Edina Horváth, Nóra Dudás, András Papp, and Edit Paulik. 2023. "Female Sexual Dysfunction in Association with Sexual History, Sexual Abuse and Satisfaction: A Cross-Sectional Study in Hungary" Journal of Clinical Medicine 12, no. 3: 1112. https://doi.org/10.3390/jcm12031112
APA StyleErdős, C., Kelemen, O., Pócs, D., Horváth, E., Dudás, N., Papp, A., & Paulik, E. (2023). Female Sexual Dysfunction in Association with Sexual History, Sexual Abuse and Satisfaction: A Cross-Sectional Study in Hungary. Journal of Clinical Medicine, 12(3), 1112. https://doi.org/10.3390/jcm12031112