

Initial In-Hospital Visit-to-Visit Heart Rate Variability Is Associated with Higher Risk of Atrial Fibrillation in Patients with Acute Ischemic Stroke
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
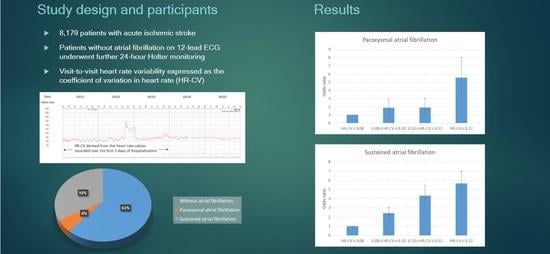
2.1. Study Population
2.2. Ascertainment of AF Types
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Association of HR-CV Level with AF
3.3. Subgroup Analysis
3.4. Interaction of Mean HR and HR-CV
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations and Acronyms
References
- Marini, C.; De Santis, F.; Sacco, S.; Russo, T.; Olivieri, L.; Totaro, R.; Carolei, A. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: Results from a population-based study. Stroke 2005, 36, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Hohnloser, S.H.; Pajitnev, D.; Pogue, J.; Healey, J.S.; Pfeffer, M.A.; Yusuf, S.; Connolly, S.J.; Investigators, A.W. Incidence of stroke in paroxysmal versus sustained atrial fibrillation in patients taking oral anticoagulation or combined antiplatelet therapy: An ACTIVE W Substudy. J. Am. Coll. Cardiol. 2007, 50, 2156–2161. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.G.; Pearce, L.A.; Rothbart, R.M.; McAnulty, J.H.; Asinger, R.W.; Halperin, J.L. Stroke with intermittent atrial fibrillation: Incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators. J. Am. Coll. Cardiol. 2000, 35, 183–187. [Google Scholar] [CrossRef]
- Sposato, L.A.; Cipriano, L.E.; Saposnik, G.; Ruiz Vargas, E.; Riccio, P.M.; Hachinski, V. Diagnosis of atrial fibrillation after stroke and transient ischaemic attack: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Schaer, B.A.; Zellweger, M.J.; Cron, T.A.; Kaiser, C.A.; Osswald, S. Value of routine holter monitoring for the detection of paroxysmal atrial fibrillation in patients with cerebral ischemic events. Stroke 2004, 35, e68–e70. [Google Scholar] [CrossRef]
- Suissa, L.; Lachaud, S.; Mahagne, M.H. Optimal timing and duration of continuous electrocardiographic monitoring for detecting atrial fibrillation in stroke patients. J. Stroke Cerebrovasc. Dis. 2013, 22, 991–995. [Google Scholar] [CrossRef] [PubMed]
- Zeng, R.; Wang, Z.; Cheng, W.; Yang, K. Visit-to-Visit Heart Rate Variability Is Positively Associated with the Risk of Adverse Cardiovascular Outcomes. Front. Cardiovasc. Med. 2022, 9, 850223. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhao, M.; Sun, Y.; Hou, Z.; Wang, C.; Yun, C.; Li, Y.; Li, Z.; Wang, M.; Wu, S.; et al. Frequency of Visit-to-Visit Variability of Resting Heart Rate and the Risk of New-Onset Atrial Fibrillation in the General Population. Am. J. Cardiol. 2021, 155, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Shiroto, H.; Tomita, H.; Hagii, J.; Metoki, N.; Fujita, A.; Kamada, T.; Takahashi, K.; Saito, S.; Sasaki, S.; Hitomi, H.; et al. Impact of Atrial Natriuretic Peptide Value for Predicting Paroxysmal Atrial Fibrillation in Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2017, 26, 772–778. [Google Scholar] [CrossRef]
- Baturova, M.A.; Sheldon, S.H.; Carlson, J.; Brady, P.A.; Lin, G.; Rabinstein, A.A.; Friedman, P.A.; Platonov, P.G. Electrocardiographic and Echocardiographic predictors of paroxysmal atrial fibrillation detected after ischemic stroke. BMC Cardiovasc. Disord. 2016, 16, 209. [Google Scholar] [CrossRef]
- Seo, W.K.; Kang, S.H.; Jung, J.M.; Choi, J.Y.; Oh, K. Novel composite score to predict atrial Fibrillation in acute stroke patients: AF predicting score in acute stroke. Int. J. Cardiol. 2016, 209, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014, 64, e1–e76. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: Executive summary. Heart Rhythm. 2017, 14, e445–e494. [Google Scholar] [CrossRef] [PubMed]
- Sung, S.F.; Hsieh, C.Y.; Lin, H.J.; Chen, Y.W.; Chen, C.H.; Kao Yang, Y.H.; Hu, Y.H. Validity of a stroke severity index for administrative claims data research: A retrospective cohort study. BMC Health Serv. Res. 2016, 16, 509. [Google Scholar] [CrossRef] [PubMed]
- Uphaus, T.; Weber-Kruger, M.; Grond, M.; Toenges, G.; Jahn-Eimermacher, A.; Jauss, M.; Kirchhof, P.; Wachter, R.; Groschel, K. Development and validation of a score to detect paroxysmal atrial fibrillation after stroke. Neurology 2019, 92, e115–e124. [Google Scholar] [CrossRef]
- Bohm, M.; Schumacher, H.; Linz, D.; Reil, J.C.; Ukena, C.; Lonn, E.; Teo, K.; Sliwa, K.; Schmieder, R.E.; Sleight, P.; et al. Low resting heart rates are associated with new-onset atrial fibrillation in patients with vascular disease: Results of the ONTARGET/TRANSCEND studies. J. Intern. Med. 2015, 278, 303–312. [Google Scholar] [CrossRef]
- Bohm, M.; Robertson, M.; Borer, J.; Ford, I.; Komajda, M.; Mahfoud, F.; Ewen, S.; Swedberg, K.; Tavazzi, L. Effect of Visit-to-Visit Variation of Heart Rate and Systolic Blood Pressure on Outcomes in Chronic Systolic Heart Failure: Results from the Systolic Heart Failure Treatment with the If Inhibitor Ivabradine Trial (SHIFT) Trial. J. Am. Heart Assoc. 2016, 5, e002160. [Google Scholar] [CrossRef]
- Zhao, M.; Yao, S.; Li, Y.; Wang, M.; Wang, C.; Yun, C.; Zhang, S.; Sun, Y.; Hou, Z.; Wu, S.; et al. Combined effect of visit-to-visit variations in heart rate and systolic blood pressure on all-cause mortality in hypertensive patients. Hypertens. Res. 2021, 44, 1291–1299. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Norby, F.L.; Whitsel, E.A.; Soliman, E.Z.; Chen, L.Y.; Loehr, L.R.; Fuster, V.; Heiss, G.; Coresh, J.; Alonso, A. Cardiac Autonomic Dysfunction and Incidence of Atrial Fibrillation: Results From 20 Years Follow-Up. J. Am. Coll. Cardiol. 2017, 69, 291–299. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Dulli, D.A.; Stanko, H.; Levine, R.L. Atrial fibrillation is associated with severe acute ischemic stroke. Neuroepidemiology 2003, 22, 118–123. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Tanabe, N.; Yagihara, N.; Watanabe, T.; Aizawa, Y.; Kodama, M. Association between lipid profile and risk of atrial fibrillation. Circ. J. 2011, 75, 2767–2774. [Google Scholar] [CrossRef]
- Ruigomez, A.; Johansson, S.; Wallander, M.A.; Garcia Rodriguez, L.A. Predictors and prognosis of paroxysmal atrial fibrillation in general practice in the UK. BMC Cardiovasc. Disord. 2005, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Staerk, L.; Wang, B.; Preis, S.R.; Larson, M.G.; Lubitz, S.A.; Ellinor, P.T.; McManus, D.D.; Ko, D.; Weng, L.C.; Lunetta, K.L.; et al. Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: Cohort study based on longitudinal data from the Framingham Heart Study. BMJ 2018, 361, k1453. [Google Scholar] [CrossRef]
- Camm, A.J.; Accetta, G.; Al Mahmeed, W.; Ambrosio, G.; Goldhaber, S.Z.; Haas, S.; Jansky, P.; Kayani, G.; Misselwitz, F.; Oh, S.; et al. Impact of gender on event rates at 1 year in patients with newly diagnosed non-valvular atrial fibrillation: Contemporary perspective from the GARFIELD-AF registry. BMJ Open 2017, 7, e014579. [Google Scholar] [CrossRef]
- Holroyd-Leduc, J.M.; Kapral, M.K.; Austin, P.C.; Tu, J.V. Sex differences and similarities in the management and outcome of stroke patients. Stroke 2000, 31, 1833–1837. [Google Scholar] [CrossRef]
- Lopez, F.L.; Agarwal, S.K.; Maclehose, R.F.; Soliman, E.Z.; Sharrett, A.R.; Huxley, R.R.; Konety, S.; Ballantyne, C.M.; Alonso, A. Blood lipid levels, lipid-lowering medications, and the incidence of atrial fibrillation: The atherosclerosis risk in communities study. Circ. Arrhythm. Electrophysiol. 2012, 5, 155–162. [Google Scholar] [CrossRef]
- Mora, S.; Akinkuolie, A.O.; Sandhu, R.K.; Conen, D.; Albert, C.M. Paradoxical association of lipoprotein measures with incident atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2014, 7, 612–619. [Google Scholar] [CrossRef]
- Li, X.; Gao, L.; Wang, Z.; Guan, B.; Guan, X.; Wang, B.; Han, X.; Xiao, X.; Waleed, K.B.; Chandran, C.; et al. Lipid profile and incidence of atrial fibrillation: A prospective cohort study in China. Clin. Cardiol. 2018, 41, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Fauchier, L.; Clementy, N.; Pelade, C.; Collignon, C.; Nicolle, E.; Lip, G.Y. Patients with Ischemic Stroke and Incident Atrial Fibrillation: A Nationwide Cohort Study. Stroke 2015, 46, 2432–2437. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, M.; Munoz-Venturelli, P.; Billot, L.; Wang, X.; Song, L.; Arima, H.; Lavados, P.M.; Hackett, M.L.; Olavarria, V.V.; Brunser, A.; et al. Low blood pressure and adverse outcomes in acute stroke: HeadPoST study explanations. J. Hypertens. 2021, 39, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Steger, C.; Pratter, A.; Martinek-Bregel, M.; Avanzini, M.; Valentin, A.; Slany, J.; Stollberger, C. Stroke patients with atrial fibrillation have a worse prognosis than patients without: Data from the Austrian Stroke registry. Eur. Heart J. 2004, 25, 1734–1740. [Google Scholar] [CrossRef]
- Temu, T.M.; Lane, K.A.; Shen, C.; Ng’ang’a, L.; Akwanalo, C.O.; Chen, P.S.; Emonyi, W.; Heckbert, S.R.; Koech, M.M.; Manji, I.; et al. Clinical characteristics and 12-month outcomes of patients with valvular and non-valvular atrial fibrillation in Kenya. PLoS One 2017, 12, e0185204. [Google Scholar] [CrossRef]
- Ruperti Repilado, F.J.; Doerig, L.; Blum, S.; Aeschbacher, S.; Krisai, P.; Ammann, P.; Erne, P.; Moschovitis, G.; di Valentino, M.; Shah, D.; et al. Prevalence and predictors of atrial fibrillation type among individuals with recent onset of atrial fibrillation. Swiss. Med. Wkly. 2018, 148, w14652. [Google Scholar] [CrossRef]
- Meinertz, T.; Kirch, W.; Rosin, L.; Pittrow, D.; Willich, S.N.; Kirchhof, P.; investigators, A. Management of atrial fibrillation by primary care physicians in Germany: Baseline results of the ATRIUM registry. Clin. Res. Cardiol. 2011, 100, 897–905. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acute Ischemic Stroke | p Value | ||||
|---|---|---|---|---|---|
| Total (N = 8179) | Without AF (N = 5013) | With Paroxysmal AF (N = 441) | With Persistent AF (N = 2725) | ||
| Age, years | <0.001 | ||||
| Mean (SD) | 68.05 (13.56) | 64.30 (13.67) | 74.73 (10.38) | 73.86 (11.15) | |
| Median (Q1, Q3) | 69.00 (59.00, 78.00) | 65.00 (55.00, 75.00) | 76.00 (68.00, 82.00) | 75.00 (66.00, 82.00) | |
| Male | 4997 (61.1) | 3340 (66.6) | 240 (54.4) | 1417 (52.0) | <0.001 |
| eNIHSS | <0.001 | ||||
| Mean (SD) | 8.34 (6.64) | 6.58 (4.96) | 9.78 (7.26) | 11.34 (7.98) | |
| Median (Q1, Q3) | 4.06 (4.06, 10.90) | 4.06 (4.06, 6.00) | 5.66 (4.06, 16.27) | 8.95 (4.06, 20.04) | |
| Hypertension | 5931 (72.5) | 3662 (73.1) | 336 (76.2) | 1933 (70.9) | 0.028 |
| Diabetes mellitus | 2837 (34.7) | 1874 (37.4) | 129 (29.3) | 834 (30.6) | <0.001 |
| Dyslipidemia | 3600 (44.0) | 2592 (51.7) | 139 (31.5) | 869 (31.9) | <0.001 |
| Congestive heart failure | 687 (8.4) | 212 (4.2) | 55 (12.5) | 420 (15.4) | <0.001 |
| Coronary artery disease | 871 (10.6) | 445 (8.9) | 79 (17.9) | 347 (12.7) | <0.001 |
| Current smoker | 2180 (26.7) | 1630 (32.5) | 97 (22.0) | 453 (16.6) | <0.001 |
| History of cancer | 478 (5.8) | 279 (5.6) | 29 (6.6) | 170 (6.2) | 0.385 |
| Body mass index, kg/m2 | <0.001 | ||||
| Mean (SD) | 24.76 (4.26) | 25.05 (4.32) | 24.01 (3.96) | 24.35 (4.17) | |
| Median (Q1, Q3) | 24.40 (21.91, 27.12) | 24.66 (22.20, 27.34) | 23.92 (21.23, 26.67) | 24.07 (21.45, 26.69) | |
| Total cholesterol, mmol/L | <0.001 | ||||
| Mean (SD) | 4.55 (1.09) | 4.69 (1.13) | 4.36 (1.06) | 4.32 (0.99) | |
| Median (Q1, Q3) | 4.45 (3.83, 5.15) | 4.58 (3.96, 5.31) | 4.27 (3.66, 4.91) | 4.25 (3.68, 4.90) | |
| Triglycerides, mmol/L | <0.001 | ||||
| Mean (SD) | 1.41 (1.05) | 1.56 (1.08) | 1.26 (0.85) | 1.15 (0.97) | |
| Median (Q1, Q3) | 1.18 (0.84, 1.67) | 1.31 (0.94, 1.86) | 1.05 (0.79, 1.46) | 0.97 (0.72, 1.33) | |
| Creatinine, μmol/L | <0.001 | ||||
| Mean (SD) | 112.09 (115.82) | 111.25 (120.01) | 126.77 (138.48) | 111.26 (103.13) | |
| Median (Q1, Q3) | 85.75 (69.84, 109.62) | 83.98 (68.95, 106.96) | 91.94 (73.37, 118.90) | 88.40 (70.72, 114.04) | |
| Alanine aminotransferase, U/L | <0.001 | ||||
| Mean (SD) | 26.42 (38.14) | 26.86 (25.90) | 23.78 (19.01) | 26.05 (55.33) | |
| Median (Q1, Q3) | 21.00 (16.00, 29.00) | 21.00 (16.00, 29.00) | 20.00 (14.00, 27.00) | 20.00 (15.00, 28.00) | |
| Mean SBP, mmHg | <0.001 | ||||
| Mean (SD) | 148.36 (19.35) | 150.51 (19.73) | 145.29 (18.78) | 144.90 (18.15) | |
| Median (Q1, Q3) | 147.20 (134.50, 161.60) | 149.43 (136.39, 164.06) | 144.50 (132.63, 156.78) | 144.01 (132.12, 157.24) | |
| Mean DBP, mmHg | <0.001 | ||||
| Mean (SD) | 83.85 (11.26) | 84.76 (11.17) | 79.49 (11.46) | 82.90 (11.15) | |
| Median (Q1, Q3) | 83.14 (76.37, 90.91) | 84.00 (77.14, 91.76) | 79.00 (72.61, 86.06) | 82.30 (75.44, 90.19) | |
| Mean heart rate, bpm | <0.001 | ||||
| Mean (SD) | 75.84 (12.01) | 73.19 (10.71) | 77.68 (13.41) | 80.42 (12.59) | |
| Median (Q1, Q3) | 74.86 (67.62, 82.83) | 72.74 (65.92, 79.36) | 75.89 (68.76, 85.46) | 79.88 (12.59, 89.19) | |
| CV in heart rate | <0.001 | ||||
| Mean (SD) | 0.109 (0.048) | 0.097 (0.039) | 0.148 (0.078) | 0.126 (0.047) | |
| Median (Q1, Q3) | 0.101 (0.077, 0.133) | 0.090 (0.069, 0.118) | 0.132 (0.095, 0.181) | 0.118 (0.093, 0.149) | |
| Paroxysmal Atrial Fibrillation | Persistent Atrial Fibrillation | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| HR-CV (per 1 SD) | 2.082 (1.867–2.322) | <0.001 | 1.887 (1.748–2.036) | <0.001 |
| Male | 0.652 (0.484–0.879) | 0.005 | 0.612 (0.519–0.721) | <0.001 |
| Age | 1.057 (1.044–1.071) | <0.001 | 1.067 (1.060–1.075) | <0.001 |
| Hypertension | 1.048 (0.759–1.446) | 0.776 | 0.965 (0.811–1.149) | 0.693 |
| Diabetes mellitus | 0.838 (0.628–1.117) | 0.228 | 0.997 (0.852–1.167) | 0.972 |
| Current smoker | 1.039 (0.736–1.467) | 0.829 | 0.835 (0.694–1.004) | 0.055 |
| Coronary artery disease | 1.823 (1.260–2.635) | 0.001 | 1.128 (0.895–1.421) | 0.308 |
| Dyslipidemia | 0.559 (0.420–0.744) | <0.001 | 0.630 (0.540–0.735) | <0.001 |
| Congestive heart failure | 1.543 (0.975–2.443) | 0.064 | 2.515 (1.938–3.265) | <0.001 |
| History of cancer | 0.717 (0.408–1.261) | 0.248 | 0.928 (0.688–1.253) | 0.627 |
| eNIHSS | 1.015 (0.994–1.037) | 0.168 | 1.074 (1.061–1.086) | <0.001 |
| Body mass index | 1.017 (0.983–1.052) | 0.326 | 1.042 (1.024–1.061) | <0.001 |
| Total Cholesterol | 0.985 (0.864–1.123) | 0.822 | 0.899 (0.832–0.970) | 0.006 |
| Triglycerides | 0.974 (0.823–1.152) | 0.757 | 0.756 (0.678–0.844) | <0.001 |
| Alanine aminotransferase | 0.998 (0.993–1.004) | 0.600 | 1.000 (0.999–1.002) | 0.719 |
| Creatinine | 1.001 (1.000–1.002) | 0.216 | 1.000 (0.999–1.001) | 0.816 |
| Mean heart rate | 1.020 (1.008–1.033) | 0.002 | 1.027 (1.020–1.035) | <0.001 |
| Mean systolic blood pressure | 0.986 (0.977–0.996) | 0.006 | 0.961 (0.955–0.966) | <0.001 |
| Mean diastolic blood pressure | 0.995 (0.977–1.013) | 0.587 | 1.065 (1.054–1.076) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-D.; Kuo, Y.-W.; Lee, C.-P.; Huang, Y.-C.; Lee, M.; Lee, T.-H. Initial In-Hospital Visit-to-Visit Heart Rate Variability Is Associated with Higher Risk of Atrial Fibrillation in Patients with Acute Ischemic Stroke. J. Clin. Med. 2023, 12, 1050. https://doi.org/10.3390/jcm12031050
Lee J-D, Kuo Y-W, Lee C-P, Huang Y-C, Lee M, Lee T-H. Initial In-Hospital Visit-to-Visit Heart Rate Variability Is Associated with Higher Risk of Atrial Fibrillation in Patients with Acute Ischemic Stroke. Journal of Clinical Medicine. 2023; 12(3):1050. https://doi.org/10.3390/jcm12031050
Chicago/Turabian StyleLee, Jiann-Der, Ya-Wen Kuo, Chuan-Pin Lee, Yen-Chu Huang, Meng Lee, and Tsong-Hai Lee. 2023. "Initial In-Hospital Visit-to-Visit Heart Rate Variability Is Associated with Higher Risk of Atrial Fibrillation in Patients with Acute Ischemic Stroke" Journal of Clinical Medicine 12, no. 3: 1050. https://doi.org/10.3390/jcm12031050
APA StyleLee, J.-D., Kuo, Y.-W., Lee, C.-P., Huang, Y.-C., Lee, M., & Lee, T.-H. (2023). Initial In-Hospital Visit-to-Visit Heart Rate Variability Is Associated with Higher Risk of Atrial Fibrillation in Patients with Acute Ischemic Stroke. Journal of Clinical Medicine, 12(3), 1050. https://doi.org/10.3390/jcm12031050