
Validation of the Acoustic Breathiness Index in Speakers of Finnish Language

Abstract
:1. Introduction
1.1. What Is Breathiness
1.2. Perceptual Tools to Detect Breathiness
1.3. Acoustic Tools to Detect Breathiness
1.4. What Is ABI?
1.5. Aim and Research Questions of the Present Study
2. Materials and Methods
2.1. Participants
2.2. Dysphonic Participants
2.3. Non-Dysphonic Controls
2.4. Recordings
2.5. Voice Samples
2.6. Auditory–Perceptual Analysis
2.7. Statistical Analysis
3. Results
3.1. Reliability of the Perceptual Evaluation
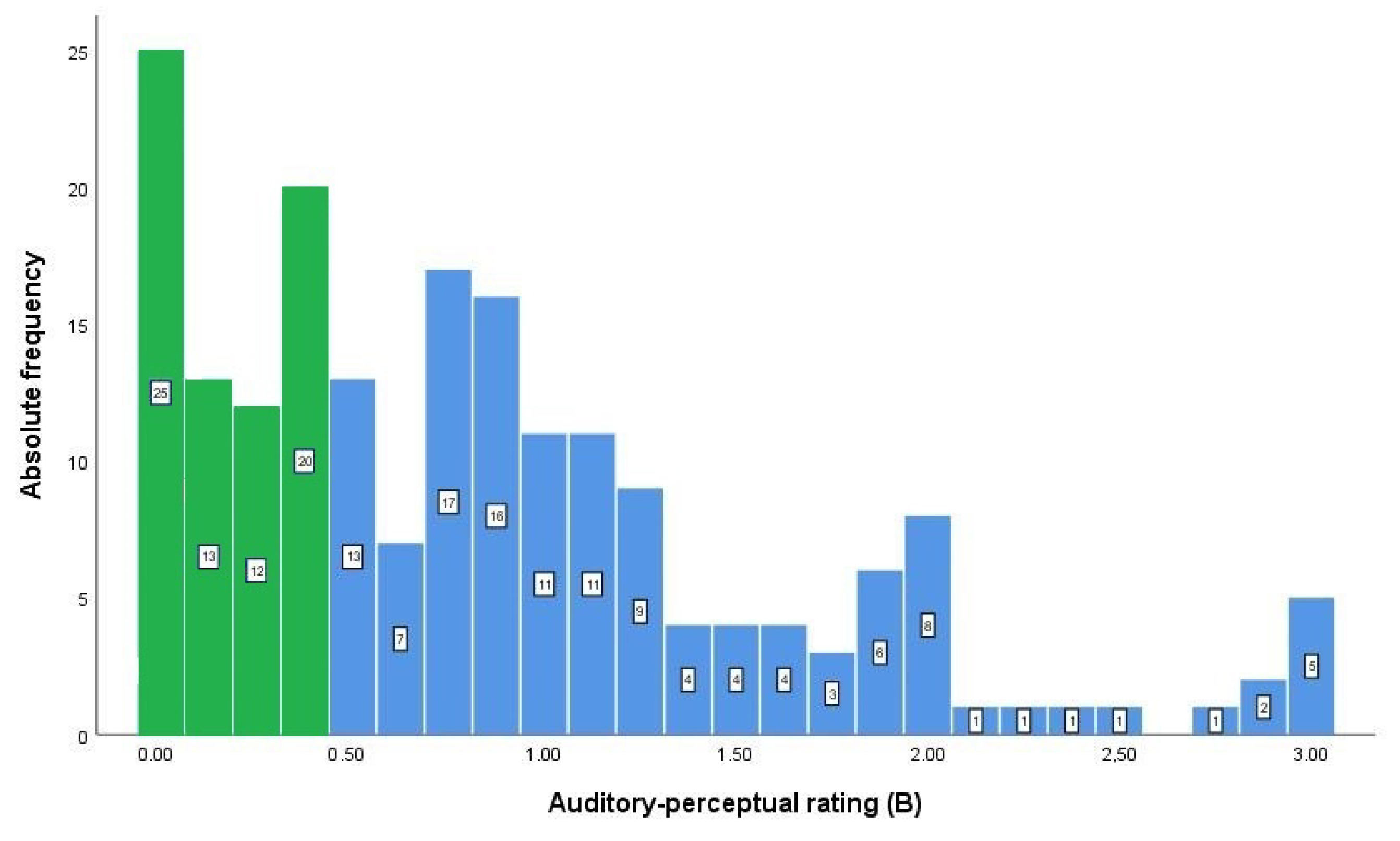
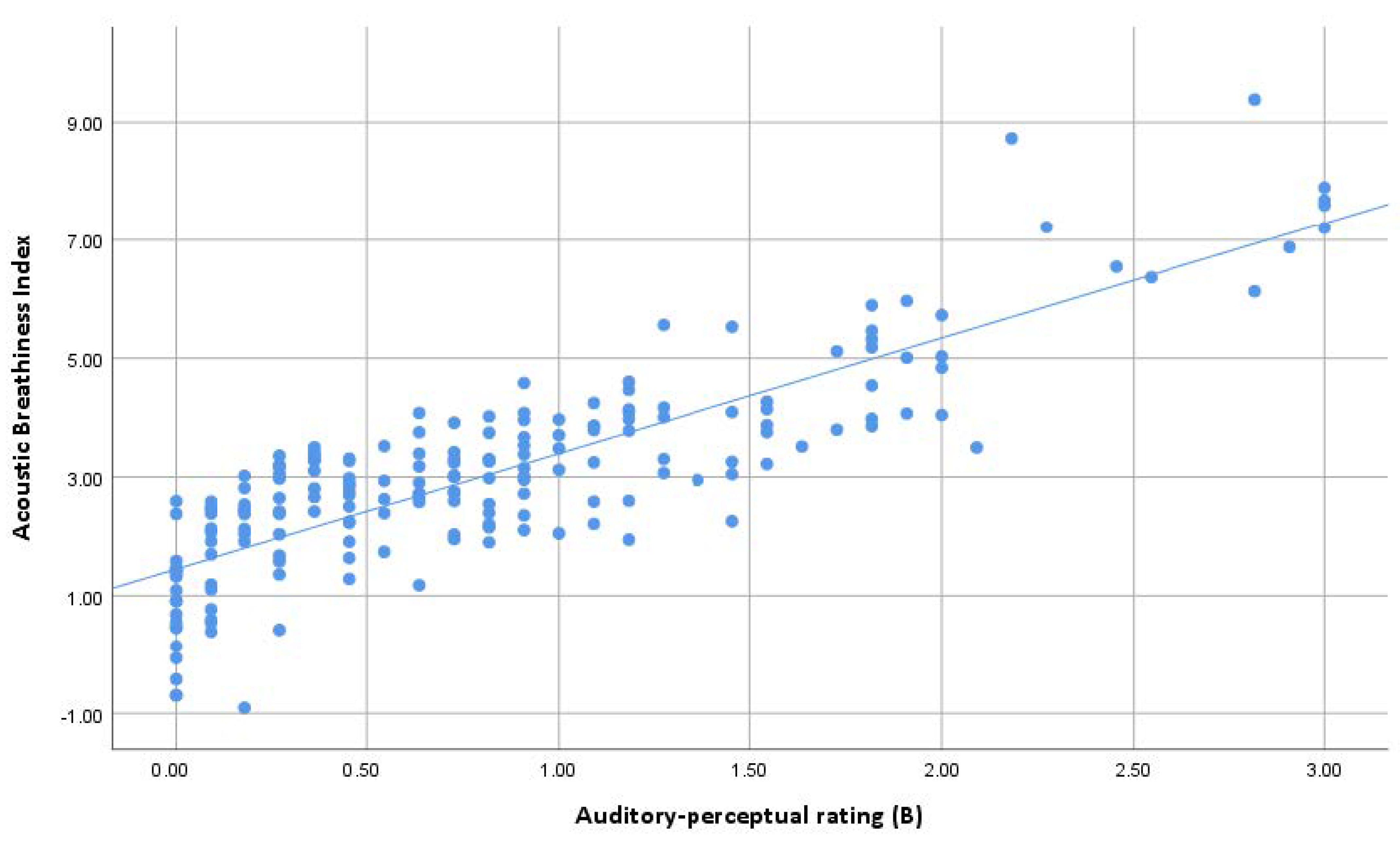
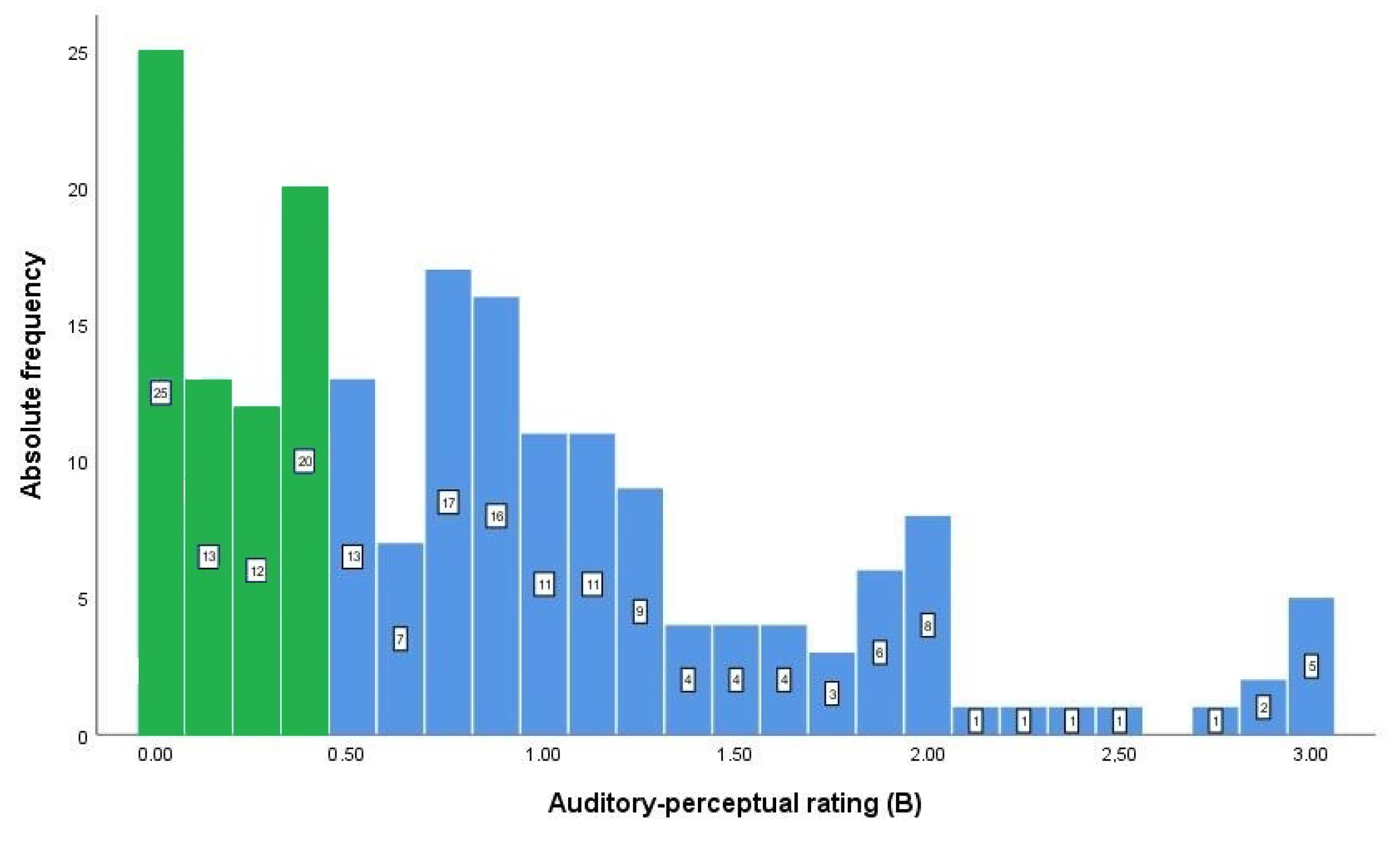
3.2. Results for the ABI and Perceptual Evaluation of Breathiness
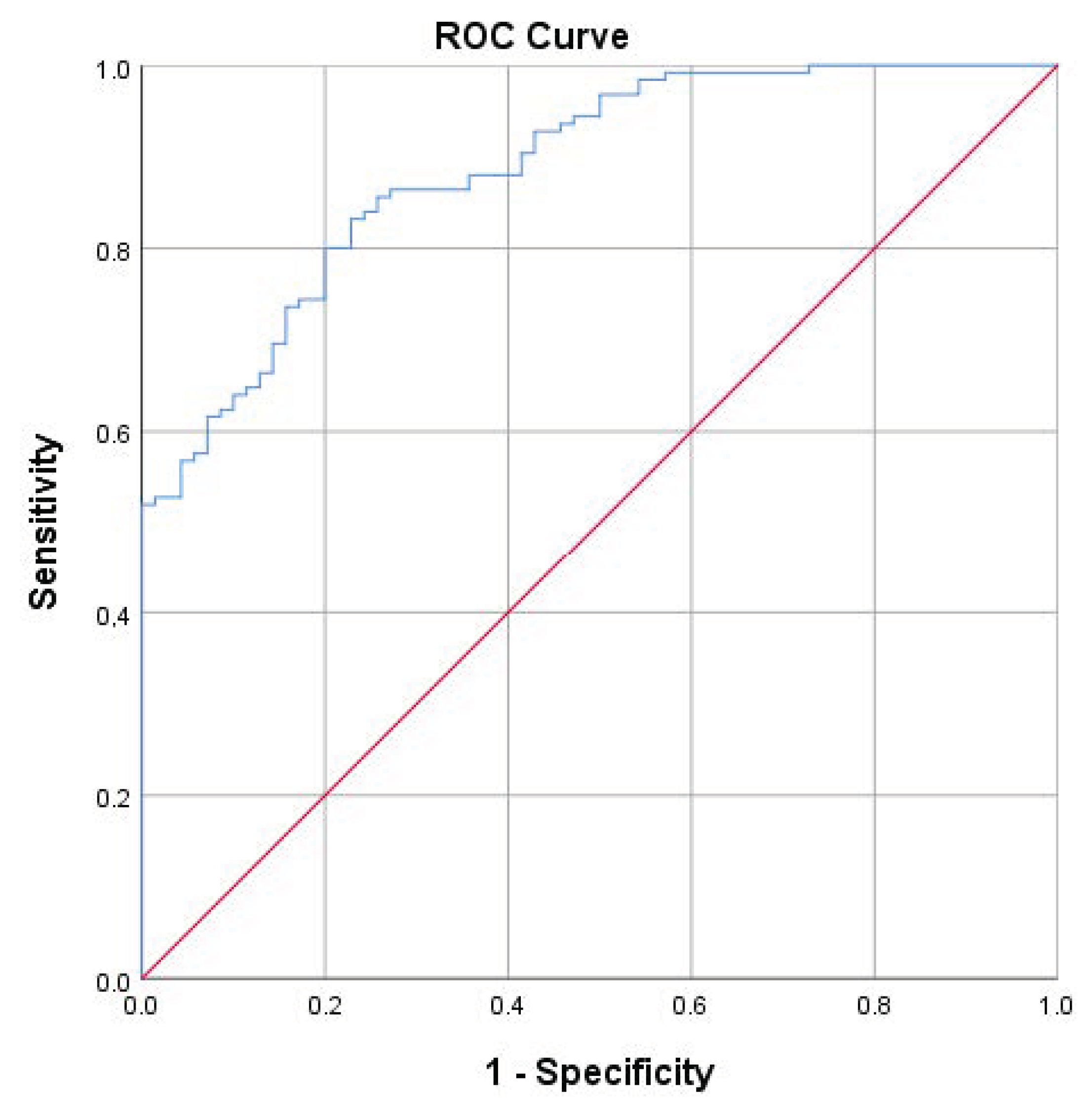
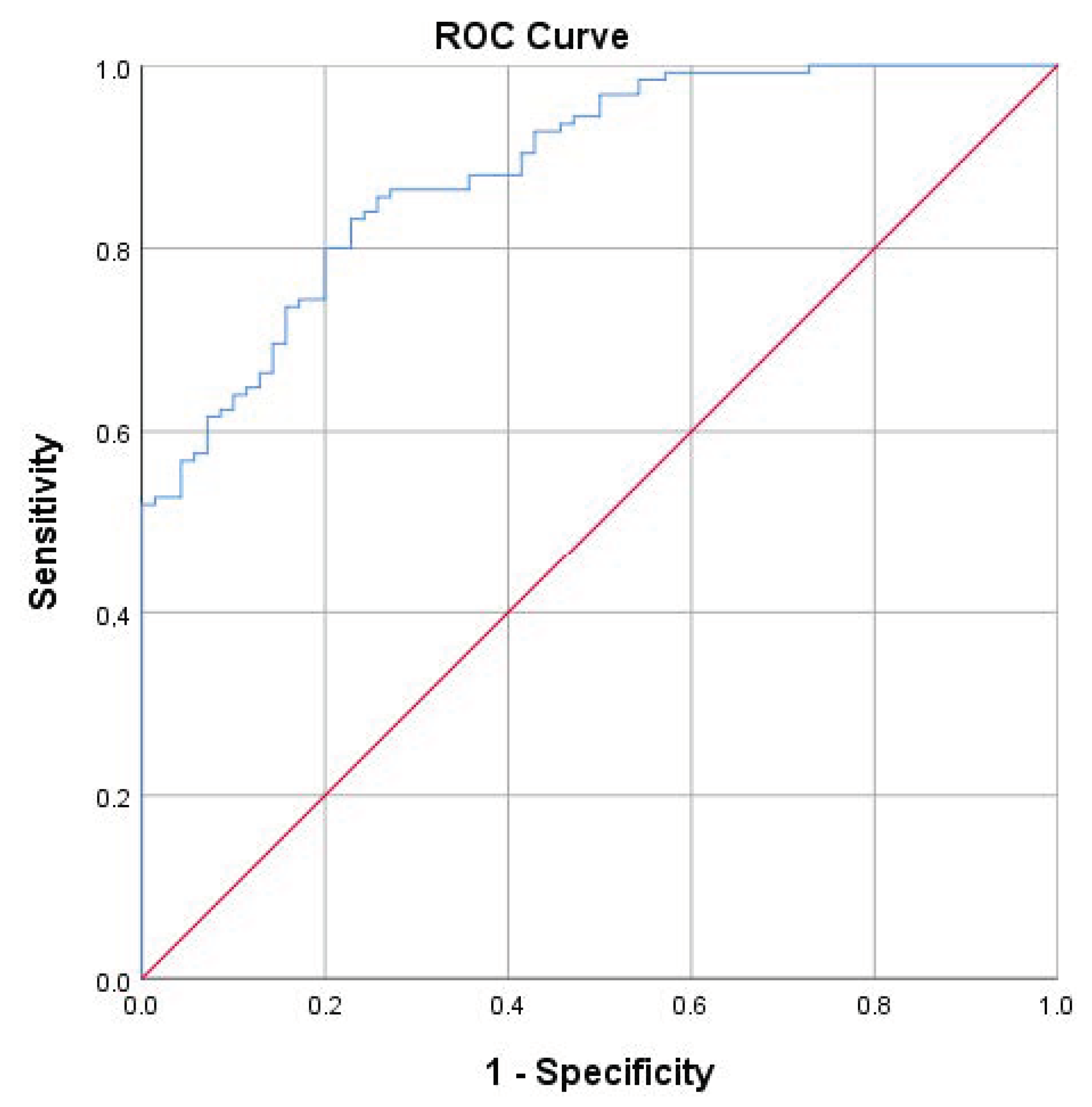
3.3. Sensitivity and Specificity of ABI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hillenbrand, J.M.; Houde, R.A. Acoustic Correlates of Breathy Vocal Quality: Dysphonic Voices and Continuous Speech. J. Speech Hear Res. 1996, 39, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Colton, R.H.; Casper, J.K.; Leonard, R. Understanding Voice Problems: A Physiological Perspective for Diagnosis and Treatment.; Lippincott Willams & Wilkins: Baltimore, MD, USA, 2006. [Google Scholar]
- Dejonckere, P.H.; Obbens, C.; De Moor, G.M.; Wieneke, G.H. Perceptual Evaluation of Dysphonia: Reliability and Relevance. Folia Phoniatr. Logop. 1993, 45, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, E.; Valencia, N.; Muñoz, J.; Trujillo, H. Differences in Voice Quality between Men and Women: Use of the Long-Term Average Spectrum (LTAS). J. Voice 1996, 10, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Van Borsel, J.; Janssens, J.; De Bodt, M. Breathiness as a Feminine Voice Characteristic: A Perceptual Approach. J. Voice 2009, 23, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Hirano, M. Psycho-Acoustic Evaluation of Voice. In Book Disorders of Human Communication 5. Clinical Examination of Voice; Hirano, M., Arnold, G.E., Winckel, F., Wyke, B.D., Eds.; Springer: Vienna, Austria, 1981. [Google Scholar]
- Dejonckere, P.H.; Wieneke, G.H. Cepstra of Normal and Pathological Voices: Correlation with Acoustic, Aerodynamic and Perceptual Data. Adv. Clin. Phon. 1996, 6, 217–226. [Google Scholar]
- Kempster, G.B.; Verdolini Abbott, K.; Barkmeier-Kraemer, J.; Hillman, R. Consensus Auditory-Perceptual Evaluation of Voice: Development of a Standardized Clinical Protocol. Am. J. Speech Lang. Pathol. 2009, 8, 124–132. [Google Scholar] [CrossRef]
- Oates, J.; Russell, A. Learning Voice Analysis Using an Interactive Multi-Media Package: Development and Preliminary Evaluation. J. Voice 1998, 12, 500–512. [Google Scholar] [CrossRef]
- Hammarberg, B. Voice Research and Clinical Needs. Folia Phoniatr. Logop. 2000, 52, 93–102. [Google Scholar] [CrossRef]
- Iwarsson, J.; Bingen-Jakobsen, A.; Johansen, D.S.; Kølle, I.E.; Pedersen, S.G.; Thorsen, S.L.; Petersen, N.R. Auditory-Perceptual Evaluation of Dysphonia: A Comparison Between Narrow and Broad Terminology Systems. J. Voice 2018, 32, 428–436. [Google Scholar] [CrossRef]
- Latoszek, B.B.v.; Maryn, Y.; Gerrits, E.; De Bodt, M. The Acoustic Breathiness Index (ABI): A Multivariate Acoustic Model for Breathiness. J. Voice 2017, 31, 511.e11–511.e27. [Google Scholar] [CrossRef]
- Penido, F.A.; Gama, A.C.C. Accuracy Analysis of the Multiparametric Acoustic Indices AVQI, ABI, and DSI for Speech-Language Pathologist Decision-Making. J. Voice, 2023; in press. [Google Scholar] [CrossRef]
- Kankare, E.; Latoszek, B.B.v.; Maryn, Y.; Asikainen, M.; Rorarius, E.; Vilpas, S.; Rantala, L.; Laukkanen, A.M. The Acoustic Voice Quality Index Version 02.02 in the Finnish-Speaking Population. Logoped. Phoniatr. Vocol. 2020, 45, 49–56. [Google Scholar] [CrossRef]
- De Krom, G. A Cepstrum-Based Technique for Determining a Harmonics-to-Noise Ratio in Speech Signals. J. Speech Lang. Hear Res. 1993, 36, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Deliyski, D. Acoustic Model and Evaluation of Pathological Voice Production. In Proceedings of the Third European Conference on Speech Communication and Technology Eurospeech, Berlin, Germany, 22–25 September 1993; pp. 1969–1972. [Google Scholar]
- Bhuta, T.; Patrick, L.; Garnett, J.D. Perceptual Evaluation of Voice Quality and Its Correlation with Acoustic Measurements. J. Voice 2004, 18, 299–304. [Google Scholar] [CrossRef]
- Hillenbrand, J.M.; Cleveland, R.A.; Erickson, R.L. Acoustic Correlates of Breathy Vocal Quality. J. Speech Hear Res. 1994, 37, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Glaze, L.E.; Bless, D.M.; Susser, R.D. Acoustic Analysis of Vowel and Loudness Differences in Children’s Voice. J. Voice 1990, 4, 37–44. [Google Scholar] [CrossRef]
- Orlikoff, R.F.; Kahane, J.C. Influence of Mean Sound Pressure Level on Jitter and Shimmer Measures. J. Voice 1991, 5, 113–119. [Google Scholar] [CrossRef]
- Brockmann-Bauser, M.; Bohlender, J.E.; Mehta, D.D. Acoustic Perturbation Measures Improve with Increasing Vocal Intensity in Individuals with and without Voice Disorders. J. Voice 2018, 32, 162–168. [Google Scholar] [CrossRef]
- Latoszek, B.B.v.; Maryn, Y.; Gerrits, E.; De Bodt, M. A Meta-Analysis: Acoustic Measurement of Roughness and Breathiness. J. Speech Lang. Hear Res. 2018, 61, 298–323. [Google Scholar] [CrossRef]
- Maryn, Y.; Roy, N.; De Bolt, M.; Van Cauwenberge, P.; Corthals, P. Acoustic Measurement of Overall Voice Quality: A Meta-Analysis. J. Acoust. Soc. Am. 2009, 126, 2619–2634. [Google Scholar] [CrossRef]
- Latoszek, B.B.v.; Lehnert, B.; Janotte, B. Validation of the Acoustic Voice Quality Index Version 03.01 and Acoustic Breathiness Index in German. J. Voice 2020, 34, 157.e17–157.e25. [Google Scholar] [CrossRef]
- Michaelis, D.; Gramss, T.; Strube, H.W. Glottal-to-Noise Excitation Ratio—A New Measure for Describing Pathological Voices. Acta Acust. United Acust. 1997, 83, 700–706. [Google Scholar]
- Dejonckere, P.H.; Lebacq, J. Harmonic Emergence in Formant Zone of a Sustained [a] as a Parameter for Evaluating Hoarseness. Acta Otorhinolaryngol. Belg. 1987, 41, 988–996. [Google Scholar] [PubMed]
- Hosokawa, K.; von Latoszek, B.B.; Ferrer-Riesgo, C.A.; Iwahashi, T.; Iwahashi, M.; Iwaki, S.; Kato, C.; Yoshida, M.; Umatani, M.; Miyauchi, A.; et al. Acoustic Breathiness Index for the Japanese-Speaking Population: Validation Study and Exploration of Affecting Factors. J. Speech Lang. Hear Res. 2019, 62, 2617–2631. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-H.; von Latoszek, B.B.; Lee, Y.-W. Validation of Acoustic Voice Quality Index Version 3.01 and Acoustic Breathiness Index in Korean Population. J. Voice 2021, 35, 660.e9–660.e18. [Google Scholar] [CrossRef] [PubMed]
- Englert, M.; Lima, L.; Behlau, M. Acoustic Voice Quality Index and Acoustic Breathiness Index: Analysis With Different Speech Material in the Brazilian Portuguese. J. Voice 2020, 34, 810.e11–810.e17. [Google Scholar] [CrossRef]
- Delgado Hernández, J.; León Gómez, N.M.; Jiménez, A.; Izquierdo, L.M.; Latoszek, B.B.v. Validation of the Acoustic Voice Quality Index Version 03.01 and the Acoustic Breathiness Index in the Spanish Language. Annal. Otol. Rhinol. Laryngol. 2018, 127, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, T.; Benoy, J. Validation of Acoustic Breathiness Index (ABI) in the South Indian Population. J. Voice, 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Aghajanzadeh, M.; Saeedi, S.; Jalaie, S.; Esarian, K.; Latoszek, B.B.v. Validation of the Acoustic Voice Quality Index and the Acoustic Breathiness Index in the Persian Language. J. Voice, 2023; in press. [Google Scholar] [CrossRef]
- Ma, E.P.-M.; Yiu, E.M.-L. Voice Activity and Participation Profile: Assessing the Impact of Voice Disorders on Daily Activities. J. Speech Lang. Hear Res. 2001, 44, 511–524. [Google Scholar] [CrossRef]
- Kleemola, L.; Helminen, M.; Rorarius, E.; Isotalo, E.; Sihvo, M. Voice Activity and Participation Profile in Assessing the Effects of Voice Disorders on Quality of Life: Estimation of the Validity, Reliability and Responsiveness of the Finnish Version. Folia Phoniatr. Logop. 2010, 63, 113–121. [Google Scholar] [CrossRef]
- Kankare, E.; Rantala, L.; Ikävalko, T.; Latoszek, B.B.v.; Laukkanen, A.-M. Akustisen Äänenlaatuindeksin (AVQI) Version 03.01 Validointi Suomenkielisille Puhujille. Puhe Kieli 2020, 40, 165–182. [Google Scholar] [CrossRef]
- Barsties, B.; Maryn, Y. The Improvement of Internal Consistency of the Acoustic Voice Quality Index. Am. J. Otolaryngol. 2015, 36, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Gierlich, J.; Latoszek, B.B.v. Test-Retest Reliability of the Acoustic Voice Quality Index and the Acoustic Breathiness Index. J. Voice, 2023; in press. [Google Scholar] [CrossRef] [PubMed]
- Brinca, L.; Batista, A.P.; Tavares, A.I.; Pinto, P.N.; Araújo, L. The Effect of Anchors and Training on the Reliability of Voice Quality Ratings for Different Types of Speech Stimuli. J. Voice 2015, 29, 776.e7–776.e14. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, P.C.M.; Vieira, M.N.; Sansão, J.P.H.; Gama, A.C.C. Effect of Auditory-Perceptual Training With Natural Voice Anchors on Vocal Quality Evaluation. J. Voice 2019, 33, 220–225. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Dejonckere, P.H.; Lebacq, J. Acoustic, Perceptual, Aero-Dynamic and Anatomical Correlations Invoice Pathology. J. Oto-Rhino-Laryngol. Relat. Specialt. 1996, 58, 326–332. [Google Scholar] [CrossRef]
- Södersten, M.; Lindestad, P.-Å. Glottal Closure and Perceived Breathiness During Phonation in Normally Speaking Subjects. J. Speech Lang. Hear Res. 1990, 33, 601–611. [Google Scholar] [CrossRef]
- Liu, X.; Xu, Y. What Makes a Female Voice Attractive? In Proceedings of the Proceedings of ICPhS XVII, Hong Kong, China, 17–21 August 2011; pp. 1274–1277. [Google Scholar]
- Šebesta, P.; Kleisner, K.; Tureček, P.; Kočnar, T.; Akoko, R.M.; Třebický, V.; Havlíček, J. Voices of Africa: Acoustic Predictors of Human Male Vocal Attractiveness. Anim. Behav. 2017, 127, 205–211. [Google Scholar] [CrossRef]
- Giles, H. Ethnicity Markers in Speech. In Book Social Markers in Speech; Scherer, K.R., Giles, H., Eds.; Cambridge University Press: Cambridge, UK, 1979. [Google Scholar]
- Waaramaa, T.; Lukkarila, P.; Järvinen, K.; Geneid, A.; Laukkanen, A.-M. Impressions of Personality from Intentional Voice Quality in Arabic-Speaking and Native Finnish-Speaking Listeners. J. Voice 2021, 35, 326.e21–326.e28. [Google Scholar] [CrossRef]
- Ladefoged, P.; Maddieson, I. Vowels of the World’s Languages. J. Phon. 1990, 18, 93–122. [Google Scholar] [CrossRef]
- Lukkarila, P.; Laukkanen, A.M.; Palo, P. Influence of the Intentional Voice Quality on the Impression of Female Speaker. Logoped. Phoniatr. Vocol. 2012, 37, 158–166. [Google Scholar] [CrossRef]
- De Bodt, M.; Van den Steen, L.; Mertens, F.; Raes, J.; Van Bel, L.; Heylen, L.; Pattyn, J.; Gordts, F.; van de Heyning, P. Characteristics of a Dysphonic Population Referred for Voice Assessment and/or Voice Therapy. Folia Phoniatr. Logop. 2016, 67, 178–186. [Google Scholar] [CrossRef]
- Mozzanica, F.; Ginocchio, D.; Barillari, R.; Barozzi, S.; Maruzzi, P.; Ottaviani, F.; Schindler, A. Prevalence and Voice Characteristics of Laryngeal Pathology in an Italian Voice Therapy-Seeking Population. J. Voice 2016, 30, 774.e13–774.e21. [Google Scholar] [CrossRef] [PubMed]
- Remacle, A.; Petitfils, C.; Flinck, C.; Morsomme, D. Description of Patients Consulting the Voice Clinic Regarding Gender, Age, Occupational Status, and Diagnosis. Eur. Arch. Otorhinolaryngol. 2017, 274, 1567–1576. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Number |
|---|---|
| Functional dysphonia | 30 |
| Paralysis/paresis of vocal fold | 23 |
| Laryngeal dystonia | 23 |
| Other diseases of vocal fold or larynx/other undefined dysphonia | 10 |
| Chronic laryngitis | 9 |
| Nodules | 5 |
| Larynx irritable with voice symptoms | 2 |
| Cough with voice symptoms | 1 |
| Polyp of vocal cord | 1 |
| Laryngeal spasm | 1 |
| Dysphagia with voice symptoms | 1 |
| Ehlers–Danlos syndrome | 1 |
| Larynx trauma | 1 |
| Total | 108 |
| N | Mean | SD | Min | Max | p-Value | |
|---|---|---|---|---|---|---|
| ABI Non-dysphonic Dysphonic | ||||||
| 87 | 2.26 | 1.15 | −0.70 | 4.58 | <0.001 | |
| 108 | 3.07 | 1.75 | −0.91 | 9.38 | ||
| Perceptually assessed BNon-dysphonic Dysphonic | 87 | 0.37 | 0.35 | 0 | 1.25 | <0.001 |
| 108 | 1.26 | 0.74 | 0 | 3 |
| Language | ABI Cut-Off Value | Sensitivity % | Specificity % | LR+ | LR− | Correlation rs between ABI and B |
|---|---|---|---|---|---|---|
| Dutch | 3.44 | 82 | 93 | 11.63 | 0.19 | 0.84 |
| German | 3.42 | 72 | 90 | 7.40 | 0.31 | 0.86 |
| Japanese | 3.44 | 76 | 94 | 8.09 | 0.13 | 0.89 |
| Korean | 3.69 | 88 | 86 | 6.47 | 0.14 | 0.87 |
| Brazilian Portuguese | 3.13 | 88 | 91 | −0.03 | 0.13 | 0.87 |
| Spanish | 3.40 | 74 | 95 | 16.02 | 0.27 | 0.83 |
| South Indian | 3.66 | 62 | 95 | 12.19 | 2.48 | 0.76 |
| Persian | 2.97 | 70 | 87 | 5.44 | 0.35 | 0.74 |
| Finnish | 2.68 | 80 | 80 | 4.00 | 0.25 | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kankare, E.; Laukkanen, A.-M. Validation of the Acoustic Breathiness Index in Speakers of Finnish Language. J. Clin. Med. 2023, 12, 7607. https://doi.org/10.3390/jcm12247607
Kankare E, Laukkanen A-M. Validation of the Acoustic Breathiness Index in Speakers of Finnish Language. Journal of Clinical Medicine. 2023; 12(24):7607. https://doi.org/10.3390/jcm12247607
Chicago/Turabian StyleKankare, Elina, and Anne-Maria Laukkanen. 2023. "Validation of the Acoustic Breathiness Index in Speakers of Finnish Language" Journal of Clinical Medicine 12, no. 24: 7607. https://doi.org/10.3390/jcm12247607
APA StyleKankare, E., & Laukkanen, A.-M. (2023). Validation of the Acoustic Breathiness Index in Speakers of Finnish Language. Journal of Clinical Medicine, 12(24), 7607. https://doi.org/10.3390/jcm12247607