
Clinical Outcomes of Next-Generation Microwave Thermosphere Ablation for Hepatocellular Carcinoma with Primarily Hepatitis-Related Etiology

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
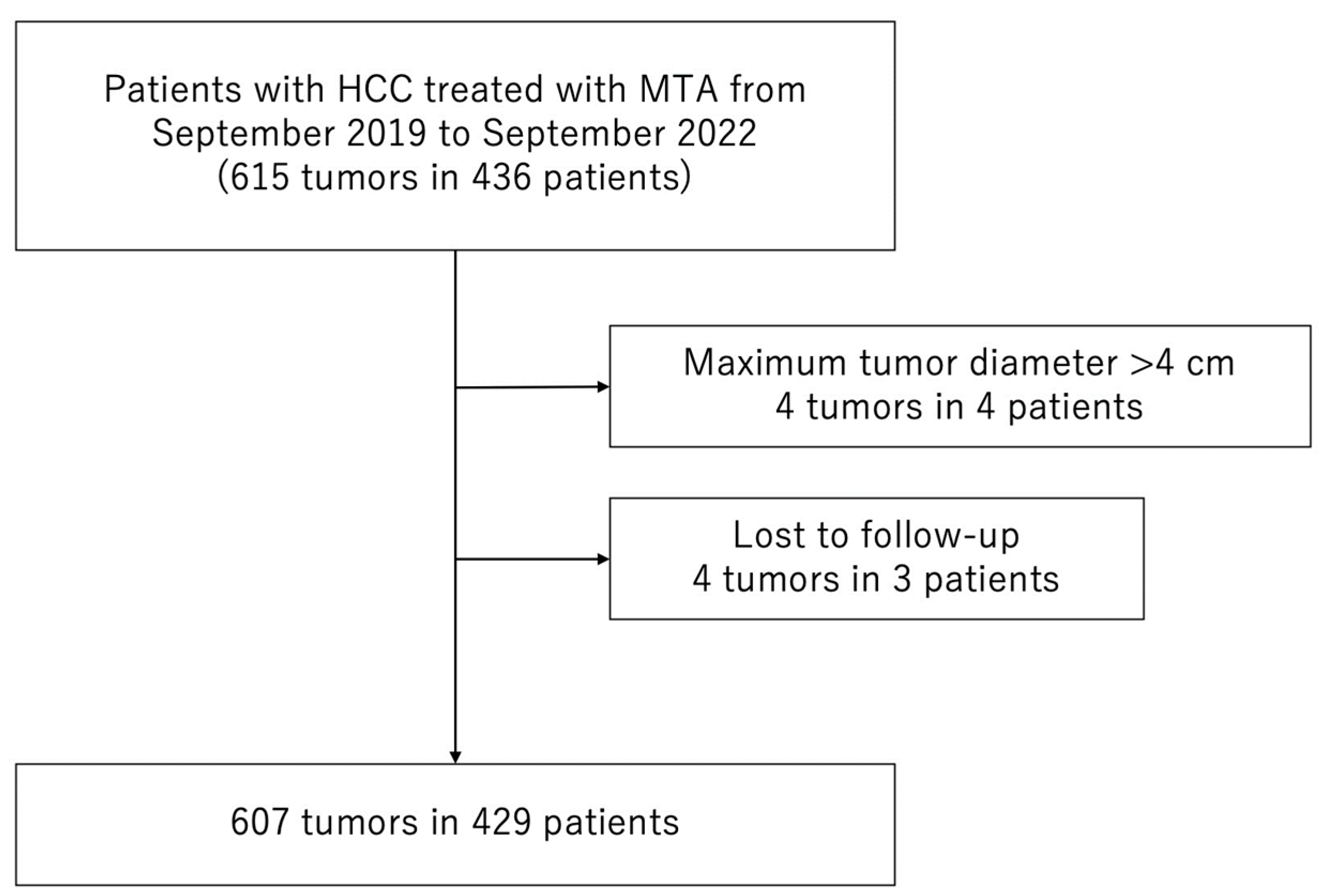
2.1. Patients
2.2. Diagnosis and Treatment of HCC
2.3. MTA Technique
2.4. Evaluation of Treatment Efficacy
2.5. Surveillance for HCC Recurrence after MTA Therapy
2.6. Evaluation of Outcomes after MTA Therapy
2.7. Safety Evaluation
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
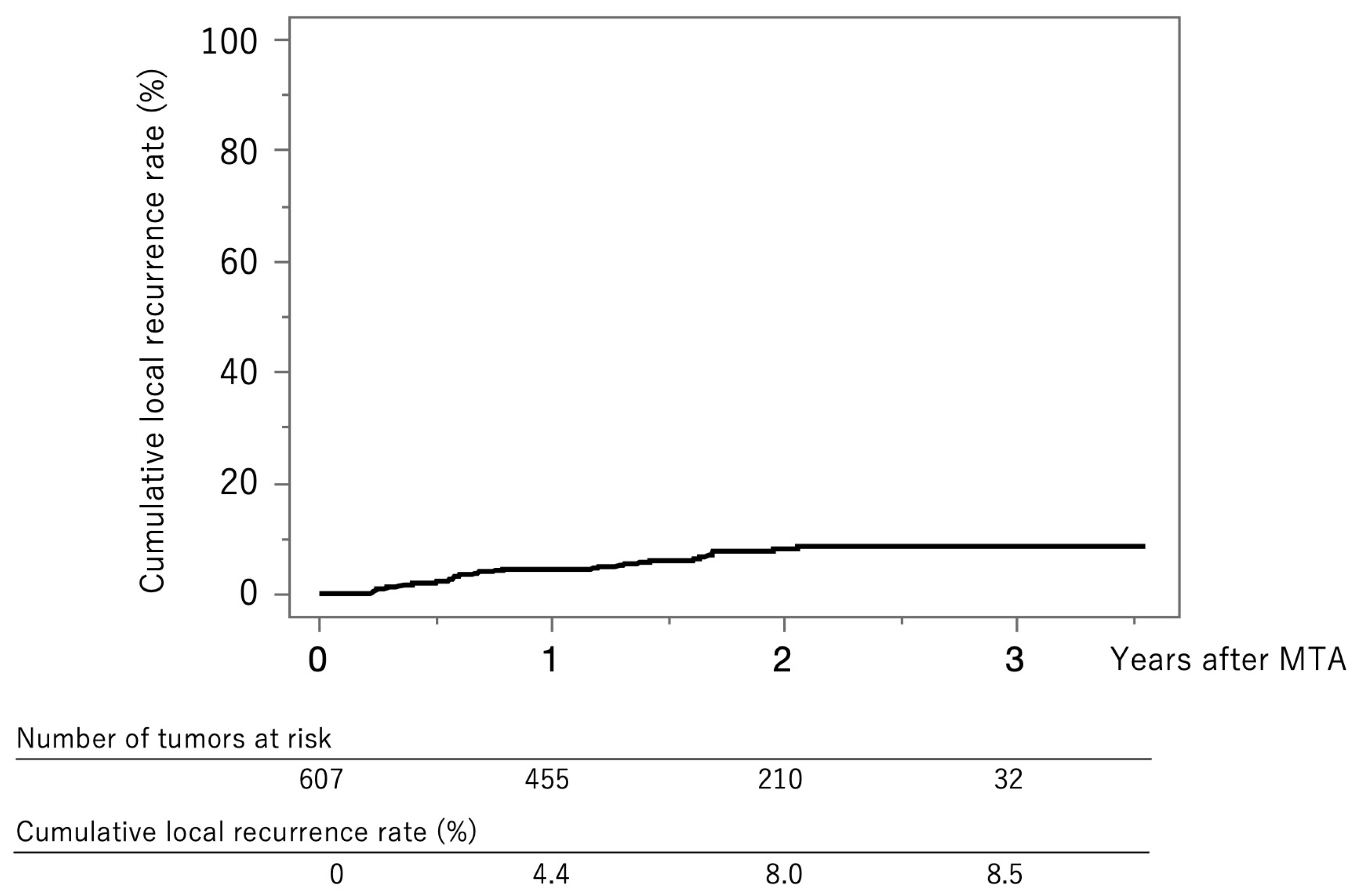
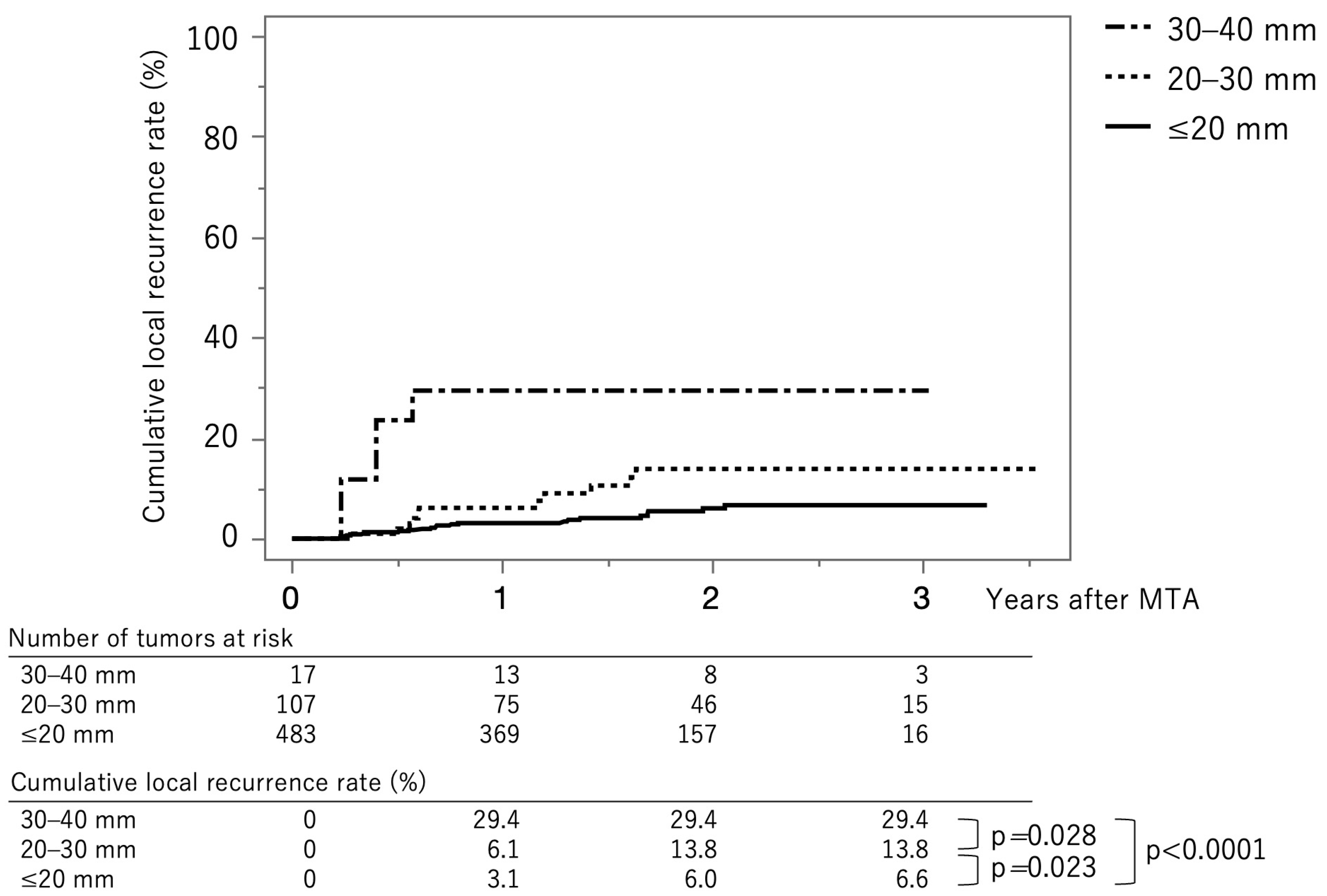
3.2. Local Tumor Recurrence
3.3. Clinical Factors Associated with Local Tumor Recurrence
3.4. Extrahepatic Metastasis
3.5. Safety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCC | hepatocellular carcinoma |
| BCLC | Barcelona Clinic Liver Cancer |
| RFA | radiofrequency ablation |
| MTA | microwave thermosphere ablation |
| MWA | microwave ablation |
| AFP | α-fetoprotein |
| AFP-L3 | Lens culinaris agglutinin-reactive α-fetoprotein |
| DCP | Des-γ-carboxy prothrombin |
| CECT | contrast-enhanced computed tomography |
| Gd-EOB-DTPA | gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid |
| MRI | magnetic resonance imaging |
| CEUS | contrast-enhanced ultrasonography |
| ECOG-PS | Eastern Cooperative Oncology Group performance status |
| HR | hazard ratio |
| CI | confidence interval |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bru, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. Trial Design and Endpoints in Hepatocellular Carcinoma: AASLD Consensus Conference. Hepatology 2021, 73 (Suppl. 1), 158–191. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Crocetti, L. Local-regional treatment of hepatocellular carcinoma. Radiology 2012, 262, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bruix, J. Novel advancements in the management of hepatocellular carcinoma in 2008. J. Hepatol. 2008, 48 (Suppl. 1), S20–S37. [Google Scholar] [CrossRef] [PubMed]
- Shiina, S.; Teratani, T.; Obi, S.; Sato, S.; Tateishi, R.; Fujishima, T.; Ishikawa, T.; Koike, Y.; Yoshida, H.; Kawabe, T.; et al. A randomized controlled trial of radiofrequency ablation with ethanol injection for small hepatocellular carcinoma. Gastroenterology 2005, 129, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Local ablation therapy for hepatocellular carcinoma: Current status and future perspectives. J. Gastroenterol. 2004, 39, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Ravetta, V.; Rosa, L.; Ghittoni, G.; Viera, F.T.; Garbagnati, F.; Silini, E.M.; Dionigi, P.; Calliada, F.; Quaretti, P.; et al. Repeated radiofrequency ablation for management of patients with cirrhosis with small hepatocellular carcinomas: A long-term cohort study. Hepatology 2011, 53, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Lubner, M.G.; Brace, C.L.; Hinshaw, J.L.; Lee, F.T., Jr. Microwave tumor ablation: Mechanism of action, clinical results, and devices. J. Vasc. Interv. Radiol. JVIR 2010, 21, S192–S203. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver, D. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. Practice Guidelines Committee AAftSoLD. Management of hepatocellular carcinoma. Hepatology 2005, 42, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Takemura, N.; Yamashita, T.; Watadani, T.; Kaibori, M.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Aikata, H.; et al. Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2021 version (5th JSH-HCC Guidelines). Hepatol. Res. 2023, 53, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Kawamura, Y.; Hasegawa, K.; Tateishi, R.; Kariyama, K.; Shiina, S.; Toyoda, H.; Imai, Y.; Hiraoka, A.; Ikeda, M.; et al. Management of Hepatocellular Carcinoma in Japan: JSH Consensus Statements and Recommendations 2021 Update. Liver Cancer 2021, 10, 181–223. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Di Maso, M.; Muscatiello, N. Microwave ablation versus radiofrequency ablation for the treatment of hepatocellular carcinoma: A systematic review and meta-analysis. Int. J. Hyperth. 2016, 32, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Tamai, H.; Okamura, J. New next-generation microwave thermosphere ablation for small hepatocellular carcinoma. Clin. Mol. Hepatol. 2021, 27, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Alonzo, M.; Bos, A.; Bennett, S.; Ferral, H. The Emprint Ablation System with Thermosphere Technology: One of the Newer Next-Generation Microwave Ablation Technologies. Semin. Interv. Radiol. 2015, 32, 335–338. [Google Scholar]
- Saccomandi, P.; Schena, E.; Massaroni, C.; Fong, Y.; Grasso, R.F.; Giurazza, F.; Zobel, B.B.; Buy, X.; Palussiere, J.; Cazzato, R.L. Temperature monitoring during microwave ablation in ex vivo porcine livers. Eur. J. Surg. Oncol. 2015, 41, 1699–1705. [Google Scholar] [CrossRef] [PubMed]
- Hübner, F.; Schreiner, R.; Reimann, C.; Bazrafshan, B.; Kaltenbach, B.; Schüßler, M.; Jakoby, R.; Vogl, T.J. Ex vivo validation of microwave thermal ablation simulation using different flow coefficients in the porcine liver. Med. Eng. Phys. 2019, 66, 56–64. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Age at admission (years) | 76.0 (71.0–82.0) |
| Gender (male/female) * | 293/136 |
| HCC etiology (hepatitis B virus/hepatitis C virus/B + C/non-B, non-C) | 31/259/2/137 |
| Child-Pugh classification (A/B) | 379/50 |
| ECOG-PS (0/1/2) | 384/41/4 |
| Maximum tumor diameter (mm) * | 15.0 (10.0–21.0) |
| Number of tumors (1/2/3/≥4) | 304/81/24/20 |
| Number of prior treatments for HCC (0/1/≥2) | 120/99/210 |
| α-fetoprotein (ng/mL) * | 6.1 (3.3–13.4) |
| Lens culinaris agglutinin-reactive α-fetoprotein (%) * | 0.0 (0.0–9.6) |
| Des-γ-carboxy prothrombin (mAU/mL) * | 28.0 (19.0–64.1) |
| Characteristics | |
|---|---|
| Age at first MTA * | 76.0 (71.0–81.0) |
| Gender (male/female) * | 201/103 |
| Etiology (hepatitis B virus/hepatitis C virus/B+C/non-B, non-C) | 25/176/2/101 |
| Follow-up duration (months) * | 23.0 (15.3–30.7) |
| Areas of the Liver | Number of Tumors |
|---|---|
| Primary and secondary branches of intrahepatic portal vein | 26 |
| Adjacent to the heart | 25 |
| Adjacent to the inferior vena cava | 19 |
| Adjacent to the gallbladder | 17 |
| Caudate lobe | 9 |
| Adjacent to the duodenum | 5 |
| Adjacent to the esophagus | 1 |
| Adjacent to a collateral vein | 1 |
| Factors | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Difficult-to-treat location (yes) | 1.72 | 0.79–3.75 | 0.170 | 1.28 | 0.58–2.84 | 0.535 |
| Tumor size (>15 mm) | 2.59 | 1.35–4.98 | 0.004 | 2.15 | 1.11–4.16 | 0.023 |
| Ablative margin (<3 mm) | 3.45 | 1.81–6.57 | <0.001 | 2.94 | 1.52–5.71 | 0.001 |
| Protruding from the liver surface (yes) | 1.17 | 0.58–2.36 | 0.660 | |||
| Multiple tumors (yes) | 0.65 | 0.34–1.25 | 0.190 | |||
| Prior HCC treatment (yes) | 0.85 | 0.42–1.71 | 0.640 | |||
| α-fetoprotein (>10 ng/mL) | 1.42 | 0.74–2.70 | 0.290 | |||
| Lens culinaris agglutinin-reactive α-fetoprotein (>10%) | 1.58 | 0.62–4.02 | 0.335 | |||
| Des-γ-carboxy prothrombin (>28 mAU/mL) | 0.56 | 0.29–1.07 | 0.080 | |||
| HBV vs. non-virus | 0.83 | 0.18–3.76 | 0.814 | |||
| HCV vs. non-virus | 1.32 | 0.65–2.68 | 0.447 | |||
| ALT (>40 IU/L) | 1.02 | 0.43–2.44 | 0.970 | |||
| Platelet (<100 × 103/μL) | 0.56 | 0.25–1.28 | 0.168 | |||
| Complication (Including Duplications) | Total (n = 607) | Tumor Size Group | ||
|---|---|---|---|---|
| ≤20 mm | 20–30 mm | 30–40 mm | ||
| Any | 33 (5.4%) | 17 (3.5%) | 11 (10.3%) | 5 (29.4%) |
| Portal vein thrombus | 9 (1.5%) | 5 (1.0%) | 4 (3.7%) | 0 (0.0%) |
| Biloma | 9 (1.5%) | 5 (1.0%) | 2 (1.9%) | 2 (11.8%) |
| Bile duct dilatation | 6 (1.0%) | 3 (0.6%) | 2 (1.9%) | 1 (5.9%) |
| Pleural effusion | 4 (0.7%) | 3 (0.6%) | 0 (0.0%) | 1 (5.9%) |
| Hemorrhage | 2 (0.3%) | 1 (0.2%) | 1 (0.9%) | 0 (0.0%) |
| Hepatic infarction | 1 (0.2%) | 1 (0.2%) | 0 (0.0%) | 0 (0.0%) |
| Pneumothorax | 2 (0.3%) | 0 (0.0%) | 2 (1.9%) | 0 (0.0%) |
| Heat injury of the diaphragm | 1 (0.2%) | 1 (0.2%) | 0 (0.0%) | 0 (0.0%) |
| Heat injury of the right kidney | 1 (0.2%) | 0 (0.0%) | 0 (0.0%) | 1 (5.9%) |
| Factors | Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p | Odds Ratio | 95% CI | p | |
| Difficult-to-treat location (yes) | 2.38 | 1.02–5.16 | 0.0460 | 2.01 | 0.83–4.48 | 0.116 |
| Total ablation time (>5 min) | 2.53 | 1.11–5.36 | 0.0278 | 0.90 | 0.29–2.48 | 0.740 |
| Tumor size (>15 mm) | 3.68 | 1.79–8.03 | 0.0004 | 3.41 | 1.53–7.84 | 0.026 |
| Number of punctures (≥2) | 3.50 | 1.34–8.17 | 0.0129 | 2.51 | 0.77–7.97 | 0.126 |
| Ablative margin (≥3 mm) | 0.53 | 0.26–1.10 | 0.0873 | |||
| Protruding from the liver surface (yes) | 1.66 | 0.77–3.41 | 0.190 | |||
| Multiple tumors (yes) | 0.72 | 0.35–1.46 | 0.360 | |||
| Prior HCC treatment (yes) | 0.55 | 0.27–1.18 | 0.120 | |||
| Child-Pugh classification (B) | 0.87 | 0.53–1.29 | 0.500 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, S.; Tada, T.; Sue, M.; Matsuo, Y.; Murakami, S.; Muramatsu, T.; Morii, K.; Okada, H. Clinical Outcomes of Next-Generation Microwave Thermosphere Ablation for Hepatocellular Carcinoma with Primarily Hepatitis-Related Etiology. J. Clin. Med. 2023, 12, 7577. https://doi.org/10.3390/jcm12247577
Nakamura S, Tada T, Sue M, Matsuo Y, Murakami S, Muramatsu T, Morii K, Okada H. Clinical Outcomes of Next-Generation Microwave Thermosphere Ablation for Hepatocellular Carcinoma with Primarily Hepatitis-Related Etiology. Journal of Clinical Medicine. 2023; 12(24):7577. https://doi.org/10.3390/jcm12247577
Chicago/Turabian StyleNakamura, Shinichiro, Toshifumi Tada, Masahiko Sue, Yu Matsuo, Shiho Murakami, Toshiro Muramatsu, Kazuhiko Morii, and Hiroyuki Okada. 2023. "Clinical Outcomes of Next-Generation Microwave Thermosphere Ablation for Hepatocellular Carcinoma with Primarily Hepatitis-Related Etiology" Journal of Clinical Medicine 12, no. 24: 7577. https://doi.org/10.3390/jcm12247577
APA StyleNakamura, S., Tada, T., Sue, M., Matsuo, Y., Murakami, S., Muramatsu, T., Morii, K., & Okada, H. (2023). Clinical Outcomes of Next-Generation Microwave Thermosphere Ablation for Hepatocellular Carcinoma with Primarily Hepatitis-Related Etiology. Journal of Clinical Medicine, 12(24), 7577. https://doi.org/10.3390/jcm12247577