

Work Ability in the Year after Rehabilitation—Results from the RehabNytte Cohort
 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
- (1)
- What individual and disease-related factors are associated with work ability 12 months following rehabilitation?
- (2)
- Do patients undergoing specific occupational rehabilitation exhibit significant differences in work ability compared to those receiving standard rehabilitation?
- (3)
- What benefit statuses are associated with work ability at the 12-months follow-up?
- (4)
- What line of work is associated with work ability at the 12-months follow-up?
2. Materials and Methods
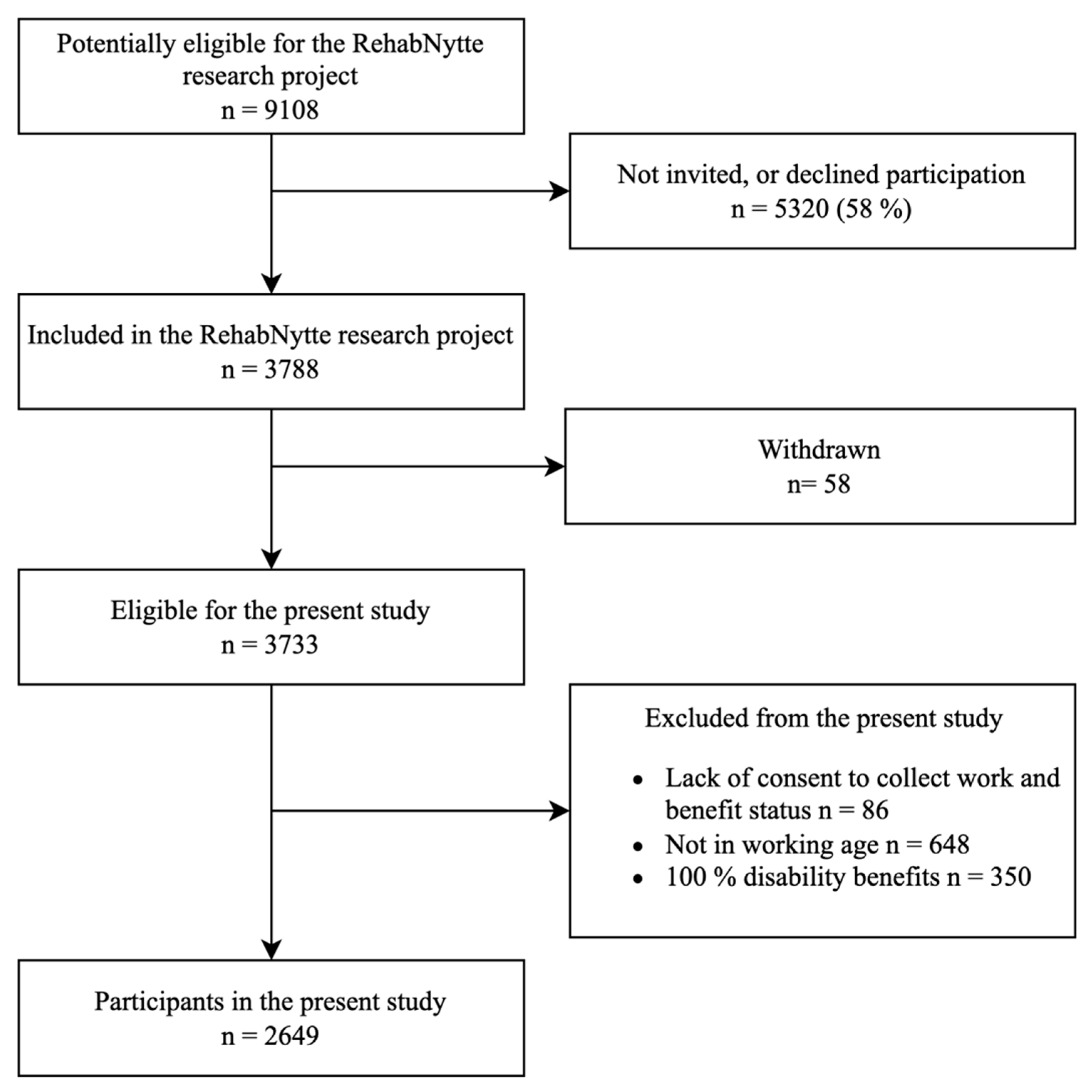
2.1. Study Design and Participants
2.2. Ethical Considrations
Patient Engagement
2.3. Outcome Measure
2.4. Explanatory Variables
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
Work-Related Factors
3.2. Change in Work Ability
3.3. Predicition of Work Ability Score at 12-Months Follow-Up
Subgroup Analyses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| OR (95% CI) | p-Value | |
|---|---|---|
| Independent variable | ||
| Age | ||
| 18–39 years a | 1.0 | |
| 40–49 years | 1.10 (0.48, 2.52) | 0.82 |
| 50–59 years | 3.04 (1.44, 6.40) | 0.003 |
| 60–66 years | 1.65 (0.67, 4.08) | 0.28 |
| Diagnosis | ||
| Other a | 1.0 | |
| Rheumatic and musculoskeletal diseases | 1.04 (0.55, 1.96) | 0.90 |
| Cancer | 0.40 (0.18, 0.88) | 0.02 |
| Comorbidities | ||
| None a | 1.0 | |
| 1–2 | 0.74 (0.29, 1.86) | 0.52 |
| 3–4 | 0.77 (0.29, 1.99) | 0.58 |
| 5 or more | 0.42 (0.12, 1.45) | 0.17 |
| Pain intensity | ||
| 0–5 a | 1.0 | |
| 6–7 | 0.54 (0.31, 0.95) | 0.03 |
| 8–10 | 0.78 (0.39, 1.59) | 0.50 |
| EQ-5D VAS | ||
| 0–39 a | 1.0 | |
| 40–55 | 2.96 (1.61, 5.43) | <0.001 |
| 56–100 | 4.17 (2.15, 8.09) | <0.001 |
| Marital status | ||
| Single a | 1.0 | |
| Married/cohabiting | 0.64 (0.39, 1.07) | 0.09 |
| Benefit status | ||
| Disability pension a | 1.0 | |
| Work assessment allowance | 1.40 (0.49, 3.96) | 0.53 |
| Sick leave | 9.95 (3.90, 25.39) | <0.001 |
| OR (95% CI) | p-Value | |
|---|---|---|
| Independent variable | ||
| Age | ||
| 18–39 years a | 1.0 | |
| 40–49 years | 1.49 (0.86, 2.57) | 0.16 |
| 50–59 years | 2.18 (1.31, 3.65) | 0.003 |
| 60–66 years | 1.74 (0.93, 3.26) | 0.08 |
| Diagnosis | ||
| Other a | 1.0 | |
| Rheumatic and musculoskeletal diseases | 1.11 (0.73, 1.67) | 0.62 |
| Cancer | 0.26 (0.15, 0.56) | <0.001 |
| Comorbidities | ||
| None a | 1.0 | |
| 1–2 | 0.49 (0.27, 0.89) | 0.02 |
| 3–4 | 0.40 (0.22, 0.75) | 0.004 |
| 5 or more | 0.25 (0.11, 0.60) | 0.002 |
| Pain intensity | ||
| 0–5 a | 1.0 | |
| 6–7 | 0.56 (0.38, 0.83) | 0.004 |
| 8–10 | 0.72 (0.42, 1.23) | 0.23 |
| EQ-5D VAS | ||
| 0–39 a | 1.0 | |
| 40–55 | 2.01 (1.29, 3.14) | 0.002 |
| 56–100 | 3.72 (2.38, 5.82) | <0.001 |
| Marital status | ||
| Single a | 1.0 | |
| Married/cohabiting | 0.59 (0.41, 0.86) | 0.005 |
| Main line of work | ||
| Manager and professional a | 1.0 | |
| Technician or associate professional | 0.93 (0.56, 1.57) | 0.79 |
| Service-, sales- or care-worker; craft and related trades worker; or machine operator | 0.59 (0.37, 0.93) | 0.03 |
| Work training or apprentice, elementary occupations and other | 0.83 (0.51, 1.37) | 0.48 |
Appendix B
| Diagnosis in the “Other” Category (n = 927) | n (%) |
|---|---|
| Cardiological diseases | 56 (6.04) |
| Lifestyle-related illnesses | 284 (30.63) |
| Neurology | 274 (29.56) |
| Diseases in the ear | 124 (13.38) |
| Mental illnesses | 69 (7.44) |
| Other * | 120 (12.94) |
References
- Busse, R. Tackling Chronic Disease in Europe: Strategies, Interventions and Challenges; WHO Regional Office Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Kamenov, K.; Mills, J.-A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef]
- Verhoef, J.A.C.; Bal, M.I.; Roelofs, P.; Borghouts, J.A.J.; Roebroeck, M.E.; Miedema, H.S. Effectiveness and characteristics of interventions to improve work participation in adults with chronic physical conditions: A systematic review. Disabil. Rehabil. 2020, 44, 1007–1022. [Google Scholar] [CrossRef]
- van Rijn, R.M.; Carlier, B.E.; Schuring, M.; Burdorf, A. Work as treatment? The effectiveness of re-employment programmes for unemployed persons with severe mental health problems on health and quality of life: A systematic review and meta-analysis. Occup. Environ. Med. 2016, 73, 275–279. [Google Scholar] [CrossRef]
- Belin, A.; Dupont, C.; Oulès, L.; Kuipers, Y.; Elena Fries-Tersch, E. Rehabilitation and Return to Work: Analysis Report on EU Policies, Strategies and Programmes; European Agency for Safety and Health at Work: Luxembourg, 2016; p. 94. [Google Scholar] [CrossRef]
- Wilkie, R.; Bjork, M.; Costa-Black, K.M.; Parker, M.; Pransky, G. Managing work participation for people with rheumatic and musculoskeletal diseases. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101517. [Google Scholar] [CrossRef]
- Ahlstrom, L.; Grimby-Ekman, A.; Hagberg, M.; Dellve, L. The work ability index and single-item question: Associations with sick leave, symptoms, and health—A prospective study of women on long-term sick leave. Scand. J. Work. Environ. Health 2010, 36, 404–412. [Google Scholar] [CrossRef]
- Lundin, A.; Kjellberg, K.; Leijon, O.; Punnett, L.; Hemmingsson, T. The Association between Self-Assessed Future Work Ability and Long-Term Sickness Absence, Disability Pension and Unemployment in a General Working Population: A 7-Year Follow-Up Study. J. Occup. Rehabil. 2016, 26, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. Work ability—A comprehensive concept for occupational health research and prevention. Scand. J. Work. Environ. Health 2009, 35, 1–5. [Google Scholar] [CrossRef]
- Tengland, P.A. The concept of work ability. J. Occup. Rehabil. 2011, 21, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Gould, R.; Ilmarinen, J.; Järvisalo, J.; Koskinen, S. Dimensions of Work Ability: Results of the Health 2000 Survey; Finnish Centre for Pensions (ETK): Eläketurvakeskus, Finland; The Social Insurance Institution (Kela): Helsinki, Finland; National Public Health Institute (KTL): Helsinki, Finland; Finnish Institute of Occupational Health (FIOH): Helsinki, Finland, 2008. [Google Scholar]
- Rueda, S.; Chambers, L.; Wilson, M.; Mustard, C.; Rourke, S.B.; Bayoumi, A.; Raboud, J.; Lavis, J. Association of returning to work with better health in working-aged adults: A systematic review. Am. J. Public. Health 2012, 102, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, T. Which patients with rheumatoid arthritis are still working? Arthritis Res. Ther. 2010, 12, 114. [Google Scholar] [CrossRef][Green Version]
- Loisel, P.; Durand, M.-J.; Berthelette, D.; Vézina, N.; Baril, R.; Gagnon, D.; Larivière, C.; Tremblay, C. Disability prevention: New paradigm for the management of occupational back pain. Dis. Manag. Health Outcomes 2001, 9, 351–360. [Google Scholar] [CrossRef]
- Fadyl, J.K.; McPherson, K.M.; Schlüter, P.J.; Turner-Stokes, L. Factors contributing to work-ability for injured workers: Literature review and comparison with available measures. Disabil. Rehabil. 2010, 32, 1173–1183. [Google Scholar] [CrossRef] [PubMed]
- Ståhl, C.; Karlsson, N.; Gerdle, B.; Sandqvist, J. Predictive validity of general work ability assessments in the context of sickness insurance. J. Rehabil. Med. 2021, 53, 2758. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J. From Work Ability Research to Implementation. Int. J. Environ. Res. Public Health 2019, 16, 2882. [Google Scholar] [CrossRef] [PubMed]
- de Boer, A.G.; Verbeek, J.H.; Spelten, E.R.; Uitterhoeve, A.L.; Ansink, A.C.; de Reijke, T.M.; Kammeijer, M.; Sprangers, M.A.; van Dijk, F.J. Work ability and return-to-work in cancer patients. Br. J. Cancer 2008, 98, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Selb, M.; Kiekens, C.; Todhunter-Brown, A.; Arienti, C.; Stucki, G.; Meyer, T. Rehabilitation Definition for Research Purposes. A Global Stakeholders’ Initiative by Cochrane Rehabilitation. Neurorehabil. Neural Repair. 2022, 36, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Martimo, K.-P.; Takala, E.-P. Concepts of work ability in rehabilitation. In Handbook of Disability, Work and Health; Springer: Cham, Germany, 2020; pp. 1–20. [Google Scholar]
- Norwegian National Advisory Unit on Occupational Rehabilitation. Guidelines for Work-Oriented Rehabilitation in Specialized Health Services: National Advisory Unit on Occupational Rehabilitation. 2020. Available online: https://arbeidoghelse.no/fagveileder/om-arr/arr-i-spesialisthelsetjenesten/definisjon/ (accessed on 9 November 2023).
- Briggs, A.M.; Shiffman, J.; Shawar, Y.R.; Åkesson, K.; Ali, N.; Woolf, A.D. Global health policy in the 21st century: Challenges and opportunities to arrest the global disability burden from musculoskeletal health conditions. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101549. [Google Scholar] [CrossRef]
- Boonen, A.; Webers, C.; Butink, M.; Barten, B.; Betteridge, N.; Black, D.C.; Bremander, A.; Boteva, B.; Brzezińska, O.; Chauhan, L.; et al. 2021 EULAR points to consider to support people with rheumatic and musculoskeletal diseases to participate in healthy and sustainable paid work. Ann. Rheum. Dis. 2023, 82, 57–64. [Google Scholar] [CrossRef]
- Braathen, T.N.; Veiersted, K.B.; Heggenes, J. Improved work ability and return to work following vocational multidisciplinary rehabilitation of subjects on long-term sick leave. J. Rehabil. Med. 2007, 39, 493–499. [Google Scholar] [CrossRef]
- Lyby, P.S.; Johansen, T.; Aslaksen, P.M. Comparison of Two Multidisciplinary Occupational Rehabilitation Programs Based on Multimodal Cognitive Behavior Therapy on Self-Rated Health and Work Ability. Front. Psychol. 2021, 12, 669770. [Google Scholar] [CrossRef]
- Johansen, T.; Jensen, C.; Eriksen, H.R.; Lyby, P.S.; Dittrich, W.H.; Holsen, I.N.; Jakobsen, H.; Øyeflaten, I. Occupational rehabilitation is associated with improvements in cognitive functioning. Front. Psychol. 2019, 10, 2233. [Google Scholar] [CrossRef] [PubMed]
- Leinonen, T.; Viikari-Juntura, E.; Husgafvel-Pursiainen, K.; Juvonen-Posti, P.; Laaksonen, M.; Solovieva, S. The effectiveness of vocational rehabilitation on work participation: A propensity score matched analysis using nationwide register data. Scand. J. Work. Environ. Health 2019, 45, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Bernaers, L.; Cnockaert, E.; Braeckman, L.; Mairiaux, P.; Willems, T.M. Disability and return to work after a multidisciplinary intervention for (sub)acute low back pain: A systematic review. Clin. Rehabil. 2023, 37, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Butink, M.H.P.; Webers, C.; Verstappen, S.M.M.; Falzon, L.; Betteridge, N.; Wiek, D.; Woolf, A.D.; Stamm, T.A.; Burmester, G.R.; Bijlsma, J.W.J.; et al. Non-pharmacological interventions to promote work participation in people with rheumatic and musculoskeletal diseases: A systematic review and meta-analysis from the EULAR taskforce on healthy and sustainable work participation. RMD Open 2023, 9, e002903. [Google Scholar] [CrossRef] [PubMed]
- Nossen, J.P. Tiltaksdeltakere med nedsatt arbeidsevne-hvor går de etterpå? Arb. Og Velferd 2023, 23, 112–128. [Google Scholar]
- Oyeflaten, I.; Hysing, M.; Eriksen, H.R. Prognostic factors associated with return to work following multidisciplinary vocational rehabilitation. J. Rehabil. Med. 2008, 40, 548–554. [Google Scholar] [CrossRef]
- Jensen, C. Hvem deltar på arbeidsettet rehabilitering i spesialisthelsetjenesten? In Arbeidsrettet Rehabilitering-En Vei Mot Deltakelse; Bruvatne, Ø.S.V., Ed.; Fagbokforlaget: Bergen, Norway, 2023; pp. 55–61. [Google Scholar]
- Eftedal, M.; Tveito, T.H.; Gensby, U.; Islam, M.K.; Lie, S.A.; Aasland, G.; Kostveit, S.; Jensen, C. Comparing two interdisciplinary occupational rehabilitation programs for employees on sick leave: A mixed-method design study protocol. BMC Musculoskelet. Disord. 2021, 22, 158. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Ilmarinen, J. The work ability index (WAI). Occup. Med. 2007, 57, 160. [Google Scholar] [CrossRef]
- El Fassi, M.; Bocquet, V.; Majery, N.; Lair, M.L.; Couffignal, S.; Mairiaux, P. Work ability assessment in a worker population: Comparison and determinants of Work Ability Index and Work Ability score. BMC Public Health 2013, 13, 305. [Google Scholar] [CrossRef]
- Boekel, I.; Dutmer, A.L.; Schiphorst Preuper, H.R.; Reneman, M.F. Validation of the work ability index-single item and the pain disability index-work item in patients with chronic low back pain. Eur. Spine J. 2022, 31, 943–952. [Google Scholar] [CrossRef]
- Stienstra, M.; Edelaar, M.J.A.; Fritz, B.; Reneman, M.F. Measurement Properties of the Work Ability Score in Sick-Listed Workers with Chronic Musculoskeletal Pain. J. Occup. Rehabil. 2022, 32, 103–113. [Google Scholar] [CrossRef]
- EuroQol Research Foundation. EQ-5D-5L User Guide Version 3.0: Basic Information on How to Use the EQ-5D-5L Instrument. 2019. Available online: https://euroqol.org/publications/user-guides (accessed on 4 June 2023).
- Klokkerud, M.; Dagfinrud, H.; Uhlig, T.; Dager, T.; Furunes, K.; Klokkeide, Å.; Larsen, M.; Nygård, S.; Nylenna, S.; Øie, L.; et al. Developing and testing a consensus-based core set of outcome measures for rehabilitation in musculoskeletal diseases. Scand. J. Rheumatol. 2018, 47, 225–234. [Google Scholar] [CrossRef]
- Garratt, A.M.; Engen, K.; Kjeldberg, I.R.; Nordvik, J.E.; Ringheim, I.; Westskogen, L.; Becker, F. Use of EQ-5D-5L for Assessing Patient-Reported Outcomes in a National Register for Specialized Rehabilitation. Arch. Phys. Med. Rehabil. 2023. [Google Scholar] [CrossRef] [PubMed]
- Sperandei, S. Understanding logistic regression analysis. Biochem. Medica 2014, 24, 12–18. [Google Scholar] [CrossRef]
- World Health Organization. A Healthy Lifestyle-WHO Recomandations. 2010. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 10 May 2023).
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC.: College Station, TX, USA, 2021. [Google Scholar]
- Saltychev, M.; Laimi, K.; Pentti, J.; Kivimäki, M.; Vahtera, J. Short- and long-term changes in perceived work ability after interdisciplinary rehabilitation of chronic musculoskeletal disorders: Prospective cohort study among 854 rehabilitants. Clin. Rehabil. 2014, 28, 592–603. [Google Scholar] [CrossRef] [PubMed]
- Bordignon, M.; Marziale, M.H.P.; Sutherland, M.A.; Monteiro, I. Factors related to work ability among nursing professionals from urgent and emergency care units: A cross-sectional study. Work 2023, 74, 673–683. [Google Scholar] [CrossRef]
- Hult, M.; Pietilä, A.M.; Koponen, P.; Saaranen, T. Association between good work ability and health behaviours among unemployed: A cross-sectional survey. Appl. Nurs. Res. 2018, 43, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Strazdins, L.; Bammer, G. Women, work and musculoskeletal health. Soc. Sci. Med. 2004, 58, 997–1005. [Google Scholar] [CrossRef]
- Puciato, D.; Rozpara, M. Physical activity and socio-economic status of single and married urban adults: A cross-sectional study. PeerJ 2021, 9, e12466. [Google Scholar] [CrossRef]
- Linge, A.D.; Jensen, C.; Laake, P.; Bjørkly, S.K. Lifestyle and Work-Related Factors Associated with Work Ability and Work Participation for People with Obesity: A Prospective Observational Study after Vocational Rehabilitation. Diabetes Metab. Syndr. Obes. 2021, 14, 2943–2954. [Google Scholar] [CrossRef] [PubMed]
- Bayattork, M.; Jakobsen, M.D.; Sundstrup, E.; Seidi, F.; Bay, H.; Andersen, L.L. Musculoskeletal pain in multiple body sites and work ability in the general working population: Cross-sectional study among 10,000 wage earners. Scand. J. Pain. 2019, 19, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Tisch, A. Health, work ability and work motivation: Determinants of labour market exit among German employees born in 1959 and 1965. J. Labour Mark. Res. 2015, 48, 233–245. [Google Scholar] [CrossRef]
- Ilmarinen, J.; Tuomi, K. Work ability of aging workers. Scand. J. Work. Environ. Health 1992, 18 (Suppl. 2), 8–10. [Google Scholar]
- Garratt, A.M.; Hansen, T.M.; Augestad, L.A.; Rand, K.; Stavem, K. Norwegian population norms for the EQ-5D-5L: Results from a general population survey. Qual. Life Res. 2022, 31, 517–526. [Google Scholar] [CrossRef]
- Arbeidsrettet Rehabilitering i Spesialisthelsetjenesten. 2020. Available online: https://arbeidoghelse.no/fagveileder/ (accessed on 15 October 2023).
- Aasdahl, L.; Fimland, M.S. Is there really a “golden hour” for work disability interventions? A narrative review. Disabil. Rehabil. 2020, 42, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Costa-Black, K.M. Core components of return-to-work interventions. In Handbook of Work Disability: Prevention and Management; Springer: Berlin/Heidelberg, Germany, 2013; pp. 427–440. [Google Scholar]

| All (n = 2649) | WAS Non-Responder (n = 2006) | WAS Responder (n = 643) | |
|---|---|---|---|
| Age, years, mean (SD) | 48.6 (10.9) | 48.2 (11.1) | 49.7 (10.4) ** |
| Gender, female n (%) | 1880 (71.0) | 1380 (68.8) | 500 (77.8) ** |
| Diagnosis, n (%) | |||
| Other | 927 (35.0) | 707 (35.2) | 220 (34.2) |
| Musculoskeletal and rheumatic diseases | 1110 (41.9) | 844 (42.1) | 266 (41.4) |
| Cancer | 612 (23.1) | 455 (22.7) | 157 (24.4) |
| Comorbidities, n (%) | |||
| None | 635 (23.9) | 589 (29.4) | 46 (7.2) ** |
| 1–2 | 1255 (47.4) | 908 (45.3) | 347 (54.0) ** |
| 3–4 | 584 (22.1) | 390 (19.4) | 194 (30.2) ** |
| 5 or more | 175 (6.6) | 119 (5.9) | 56 (8.7) ** |
| BMI, kg/m2, median (25 and 75 percentile) | 28.4 (24.6, 33.6) | Mean (SD) 29.8 (7.2) | Mean (SD) 30.3 (7.1) |
| Smokers, n (%) | |||
| Never | 974 (43.8) | 687 (43.5) | 287 (44.6) |
| Previous/sporadic | 1050 (47.3) | 738 (46.7) | 312 (48.5) |
| Daily | 198 (8.9) | 154 (9.8) | 44 (6.8) |
| Married/cohabiting, n (%) | 1349 (60.7) | 957 (60.5) | 392 (61.0) |
| Caring tasks, yes n (%) | 990 (44.6) | 701 (44.4) | 289 (45.0) |
| Children living at home, n (%) | 965 (43.4) | 705 (44.6) | 260 (40.4) |
| Geographic region, n (%) | |||
| West | 380 (14.4) | 261 (13.0) | 119 (18.5) ** |
| South-East | 1996 (75.4) | 1559 (77.7) | 437 (68.0) ** |
| North and Mid-Norway | 273 (20.3) | 186 (9.3) | 87 (13.5) ** |
| High education level > 12 years, n (%) | 1046 (47.1) | 727 (46.1) | 319 (49.7) |
| Pain in the last week, yes n (%) | 1779 (80.2) | 1272 (71.5) | 507 (28.5) |
| Pain intensity (0–10), mean (SD) | 5.6 (1.9) | 5.6 (1.96) | 5.5 (1.8) |
| EQ-5D VAS (0–100), mean (SD) | 48.1 (19.1) | 48.2 (19.5) | 47.7 (18.3) |
| All (n = 2649) | WAS Non-Responder (n = 2006) | WAS Responder (n = 643) | |
|---|---|---|---|
| Present work situation, n (%) | |||
| Income-generating work | 526 (23.7) | 373 (23.7) | 153 (23.8) |
| Sick leave | 653 (29.4) | 463 (29.4) | 190 (29.6) |
| Disability benefits # | 225 (10.1) | 152 (9.6) | 73 (11.4) |
| Work assessment allowance | 671 (30.2) | 478 (30.3) | 193 (30.0) |
| Student | 33 (1.5) | 29 (1.8) | 4 (0.6) |
| Job seeker | 38 (1.7) | 26 (1.7) | 12 (1.9) |
| Unpaid work | 9 (0.4) | 5 (0.3) | 4 (0.6) |
| Other | 64 (2.9) | 50 (3.2) | 14 (2.2) |
| Work Ability Score (0–10), mean (SD) | 3.5 (3.0) | 3.6 (3.0) | 3.4 (2.9) |
| Current or last main line of work, n (%) | |||
| Manager | 260 (11.8) | 181 (11.6) | 79 (12.3) |
| Professional | 179 (8.1) | 116 (7.4) | 63 (9.8) |
| Technician or associate professional | 453 (20.6) | 327 (21.0) | 126 (20.0) |
| Service-, sales- or care-worker | 392 (14.8) | 278 (17.8) | 114 (17.8) |
| Craft and related trades worker or machine operator | 416 (18.9) | 301 (19.3) | 115 (18.0) |
| Elementary occupations | 111 (5.1) | 79 (5.1) | 32 (5.0) |
| Work training or apprentice | 34 (1.6) | 26 (1.7) | 8 (1.3) |
| Other | 354 (16.1) | 251 (16.0) | 103 (16.1) |
| Amount of work prior to rehabilitation, n (%) | |||
| Full work | 976 (44.1) | 713 (45.4) | 263 (40.9) ** |
| Part-time work | 682 (30.8) | 453 (28.9) | 229 (35.6) ** |
| Not working | 554 (25.1) | 403 (25.7) | 151 (23.5) ** |
| Total | Standard Rehabilitation | Occupational Rehabilitation Program | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Paired t-Test | Mean (SD) | Paired t-Test | Mean (SD) | Paired t-Test | ||||
| Timepoint, n | Mean Difference (SD) | 95% CI of the Difference | Mean Difference (SD) | 95% CI of the Difference | Mean Difference (SD) | 95% CI of the Difference | |||
| Baseline, n = 2211 | 3.53 (2.97) | 3.61 (3.10) # | 3.27 (2.49) | ||||||
| Discharge, n = 1071 | 3.96 (3.02) | 0.42 (1.92) ** | 0.30, 0.53 | 4.0 (3.15) | 0.43 (1.97) ** | 0.29, 0.56 | 3.82 (2.56) | 0.39 (1.77) ** | 0.17, 0.61 |
| 3 months, n = 1672 | 4.22 (3.13) | 0.66 (2.22) ** | 0.55, 0.78 | 4.26 (3.24) | 0.66 (2.23) ** | 0.54, 0.78 | 4.06 (2.69) | 0.65 (2.20) ** | 0.42, 0.89 |
| 6 months, n = 1464 | 4.35 (3.20) | 0.84 (2.56) ** | 0.71, 0.98 | 4.44 (3.28) | 0.87 (2.57) ** | 0.73, 1.02 | 4.00 (2.87) | 0.74 (2.50) ** | 0.45, 1.02 |
| 12 months, n = 1447 | 4.59 (3.31) | 1.0 (2.75) ** | 0.86, 1.14 | 4.67 (3.38) | 1.02 (2.74) ** | 0.86, 1.18 | 4.30 (3.03) | 0.93 (2.79) ** | 0.61, 1.24 |
| Unadjusted Model | Partly Adjusted Model ¤ | Final Model ¤¤ | ||||
|---|---|---|---|---|---|---|
| Independent variable | OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value |
| Age | ||||||
| 18–39 years a | 1.0 | 1.0 | 1.0 | |||
| 40–49 years | 1.24 (0.86, 1.79) | 0.24 | 1.21 (0.78, 1.85) | 0.39 | 1.59 (0.92, 2.74) | 0.10 |
| 50–59 years | 1.36 (0.97, 1.90) | 0.08 | 1.56 (1.04, 2.33) | 0.03 | 2.27 (1.36, 3.78) | 0.002 |
| 60–66 years | 1.30 (0.88, 1.92) | 0.20 | 1.63 (1.01, 2.68) | 0.04 | 1.80 (0.97, 3.37) | 0.06 |
| Diagnosis | ||||||
| Other a | 1.0 | 1.0 | 1.0 | |||
| Rheumatic and musculoskeletal diseases | 0.56 (0.43, 0.72) | <0.001 | 0.83 (0.60, 1.15) | 0.26 | 1.10 (0.73, 1.67) | 0.64 |
| Cancer | 0.50 (0.37, 0.67) | <0.001 | 0.44 (0.31, 0.65) | <0.001 | 0.27 (0.16, 0.47) | <0.001 |
| Comorbidities | ||||||
| None a | 1.0 | 1.0 | 1.0 | |||
| 1–2 | 0.97 (0.73, 1.29) | 0.84 | 0.51 (0.33, 0.78) | 0.02 | 0.49 (0.27, 0.87) | 0.02 |
| 3–4 | 0.77 (0.55, 1.08) | 0.14 | 0.43 (0.27, 0.69) | <0.001 | 0.41 (0.22, 0.76) | 0.005 |
| 5 or more | 0.35 (0.18, 0.67) | 0.001 | 0.21 (0.10, 0.44) | <0.001 | 0.26 (0.11, 0.61) | 0.001 |
| Education | ||||||
| ≤12 years a | 1.0 | 1.0 | ||||
| >12 years | 1.44 (1.13, 1.83) | 0.003 | 1.44 (1.09, 1.90) | 0.01 | ||
| Pain intensity | ||||||
| 0–5 a | 1.0 | 1.0 | 1.0 | |||
| 6–7 | 0.50 (0.36, 0.69) | <0.001 | 0.50 (0.34, 0.72) | <0.001 | 0.56 (0.38, 0.83) | 0.004 |
| 8–10 | 0.44 (0.28, 0.70) | <0.001 | 0.54 (0.33, 0.89) | 0.02 | 0.72 (0.42, 1.23) | 0.23 |
| EQ-5D VAS | ||||||
| 0–39 a | 1.0 | 1.0 | 1.0 | |||
| 40–55 | 1.96 (1.37, 2.80) | <0.001 | 2.13 (1.46 3.13) | <0.001 | 2.01 (1.29, 3.12) | 0.002 |
| 56–100 | 4.97 (3.56, 6.93) | <0.001 | 3.44 (2.36, 5.02) | <0.001 | 3.83 (2.45, 5.96) | <0.001 |
| Marital status | ||||||
| Single a | 1.0 | 1.0 | 1.0 | |||
| Married/cohabiting | 0.84 (0.66, 1.07) | 0.15 | 0.65 (0.49, 0.87) | 0.004 | 0.61 (0.43, 0.88) | 0.009 |
| Smoking | ||||||
| Never a | 1.0 | 1.0 | ||||
| Previous/sporadic | 0.95 (0.74, 1.21) | 0.67 | 0.97 (0.74, 1.29) | 0.86 | ||
| Daily | 0.68 (0.41, 1.14) | 0.15 | 0.75 (0.42, 1.35) | 0.34 | ||
| Caring tasks | ||||||
| No a | 1.0 | |||||
| Yes | 0.86 (0.67, 1.09) | 0.21 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skinnes, M.N.; Moe, R.H.; Johansen, T.; Lyby, P.S.; Dahl, K.; Eid, I.; Fagertun, T.C.; Habberstad, A.; Johnsen, T.J.; Kjeken, I.; et al. Work Ability in the Year after Rehabilitation—Results from the RehabNytte Cohort. J. Clin. Med. 2023, 12, 7391. https://doi.org/10.3390/jcm12237391
Skinnes MN, Moe RH, Johansen T, Lyby PS, Dahl K, Eid I, Fagertun TC, Habberstad A, Johnsen TJ, Kjeken I, et al. Work Ability in the Year after Rehabilitation—Results from the RehabNytte Cohort. Journal of Clinical Medicine. 2023; 12(23):7391. https://doi.org/10.3390/jcm12237391
Chicago/Turabian StyleSkinnes, Mari Nilsen, Rikke Helene Moe, Thomas Johansen, Peter Solvoll Lyby, Kjersti Dahl, Idun Eid, Tor Christian Fagertun, Andreas Habberstad, Tonje Jossie Johnsen, Ingvild Kjeken, and et al. 2023. "Work Ability in the Year after Rehabilitation—Results from the RehabNytte Cohort" Journal of Clinical Medicine 12, no. 23: 7391. https://doi.org/10.3390/jcm12237391
APA StyleSkinnes, M. N., Moe, R. H., Johansen, T., Lyby, P. S., Dahl, K., Eid, I., Fagertun, T. C., Habberstad, A., Johnsen, T. J., Kjeken, I., Klokkerud, M., Linge, A. D., Lyken, A. D., Orpana, A., Rajalahti, T., Wilkie, R., Uhlig, T., & on behalf of the RehabNytte Consortium. (2023). Work Ability in the Year after Rehabilitation—Results from the RehabNytte Cohort. Journal of Clinical Medicine, 12(23), 7391. https://doi.org/10.3390/jcm12237391