
Role of the NeuroCuple™ Device for the Postoperative Pain Management of Patients Undergoing Unilateral Primary Total Knee and Hip Arthroplasty: A Pilot Prospective, Randomized, Open-Label Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Desing and Participants
2.2. Randomization and Treatment Application
2.3. Primary Outcomes
2.4. Secondary Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shah, R.; Kuo, Y.F.; Westra, J.; Lin, Y.L.; Raji, M.A. Opioid Use and Pain Control After Total Hip and Knee Arthroplasty in the US, 2014 to 2017. JAMA Netw. Open 2020, 3, e2011972. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, C.J.; Pelt, C.E.; Gililland, J.M.; Peters, C.L. Perioperative Pain Management in Hip and Knee Arthroplasty. Orthop. Clin. N. Am. 2017, 48, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Sun, E.C.; Darnall, B.D.; Baker, L.C.; Mackey, S. Incidence of and Risk Factors for Chronic Opioid Use Among Opioid-Naïve Patients in the Postoperative Period. JAMA Intern. Med. 2016, 176, 1286–1293. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.; Luo, F.; Rice, K. The economic burden of opioid use disorder and fatal opioid overdose in the United States, 2017. Drug Alcohol Depend. 2021, 218, 108350. [Google Scholar] [CrossRef] [PubMed]
- Bedard, N.A.; Pugely, A.J.; Westermann, R.W.; Duchman, K.R.; Glass, N.A.; Callaghan, J.J. Opioid use after total knee arthroplasty: Trends and risk factors for prolonged use. J. Arthroplasty. 2017, 32, 2390–2394. [Google Scholar] [CrossRef] [PubMed]
- Brummett, C.M.; Waljee, J.F.; Goesling, J.; Moser, S.; Lin, P.; Englesbe, M.J.; Nallamothu, B.K. New persistent opioid use after minor and major surgical procedures in US adults. JAMA Surg. 2017, 152, e170504. [Google Scholar] [CrossRef] [PubMed]
- Baird, C.J. COVID-19 and Opioid Overdoses: A Pandemic Leads to the Resurgence of an Epidemic. J. Addict. Nurs. 2021, 32, 165–166. [Google Scholar] [CrossRef]
- Marino, J.; Russo, J.; Herenstein, R.; Kenny, M.; Chelly, J.E. Continuous psoas compartment block vs. continuous femoral block or PCA for total hip arthroplasty. J. Bone Jt. Surg. Am. 2009, 1, 29–37. [Google Scholar] [CrossRef]
- Kozub, E.; Uttermark, A.; Skoog, R.; Dickey, W.J. Preventing Postoperative Opioid-induced respiratory depression Through Implementation of an Enhanced Monitoring Program. J. Healthc. Qual. 2021, 44, e7–e14. [Google Scholar] [CrossRef]
- Crockett, S.D.; Greer, K.B.; Heidelbaugh, J.J.; Falck-Ytter, Y.; Hanson, B.J.; Sultan, S. American Gastroenterological Association Institute Guideline on the Medical Management of Opioid-Induced Constipation. Gastroenterology 2019, 156, 218–226. [Google Scholar] [CrossRef]
- Farmer, A.D.; Holt, C.B.; Downes, T.J.; Ruggeri, E.; Del Vecchio, S.; De Giorgio, R. Pathophysiology, diagnosis, and management of opioid-induced constipation. Lancet Gastroenterol. Hepatol. 2018, 3, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Gudin, J.A.; Dietze, D.T.; Hurwitz, P.L. Improvement of pain and function after use of a topical pain relieving patch: Results of the RELIEF study. J. Pain Res. 2020, 13, 1557–1568. [Google Scholar] [CrossRef] [PubMed]
- George, S.Z.; Bolognesi, M.P.; Ryan, S.P.; Horn, M.E. Sleep disturbance, dyspnea, and anxiety following total joint arthroplasty: An observational study. J. Orthop. Surg. Res. 2022, 17, 396. [Google Scholar] [CrossRef] [PubMed]
- Bistolfi, A.; Bettoni, E.; Aprato, A.; Milani, P.; Berchialla, P.; Graziano, E.; Massazza, G.; Lee, G.C. The presence and influence of mild depressive symptoms on post-operative pain perception following primary total knee arthroplasty. Knee Surg. Sports Traum. Arth. 2017, 25, 2792–2800. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsson, P.; Nakonezny, P.A.; Lin, J.; Owhonda, R.; Richard, H.; Wells, J. Functional improvement in hip pathology is related to improvement in anxiety, depression, and pain catastrophizing: An intricate link between physical and mental well-being. BMC Musculoskelet. Disord. 2021, 22, 133. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.; Albelo, F.; Zhang, T.; Schneider, M.B.; Foster, M.J.; Aneizi, A.; Hasan, S.A.; Gilotra, M.N.; Henn, R.F., 3rd. PROMIS Depression and Anxiety in shoulder surgery patients. Bone Jt. J. 2022, 104, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Speed, T.J.; Mun, C.J.; Smith, M.T.; Khanuja, H.S.; Sterling, R.S.; Letzen, J.E.; Haythornthwaite, J.A.; Edwards, R.R.; Campbell, C.M. Temporal Association of Pain Catastrophizing and Pain Severity Across the Perioperative Period: A Cross-Lagged Panel Analysis After Total Knee Arthroplasty. Pain Med. 2021, 22, 1727–1734. [Google Scholar] [CrossRef]
- Sullivan, M.; Bishop, S.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Leung, L. Pain catastrophizing: An updated review. Indian J. Psychol. Med. 2012, 34, 204–217. [Google Scholar] [CrossRef]
- Santosa, K.B.; Hu, H.-M.; Brummett, C.M.; Olsen, M.A.; Englesbe, M.J.; Williams, E.A.; Waljee, J.F. New persistent opioid use among older patients following surgery: A Medicare claims analysis. Surgery 2020, 167, 732–742. [Google Scholar] [CrossRef]
- Roebke, A.J.; Via, G.G.; Everhart, J.S.; Munsch, M.A.; Goyal, K.S.; Glassman, A.H.; Li, M. Inpatient and outpatient opioid requirements after total joint replacement are strongly influenced by patient and surgical factors. Bone Jt. Open 2020, 1, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Nethi, S.K.; Das, S.; Patra, C.R.M. Recent advances in inorganic nanomaterials for wound-healing applications. Biomater. Sci. 2019, 7, 2652–2674. [Google Scholar] [CrossRef] [PubMed]
- Girija, A.R.; Balasubramanian, S.; Cowin, A.J. Nanomaterials-based Drug Delivery Approaches for Wound Healing. Curr. Pharm. Des. 2022, 28, 711–726. [Google Scholar] [CrossRef] [PubMed]
- Ashtikar, M.; Wacker, M.G. Nanopharmaceuticals for wound healing–Lost in translation? Adv. Drug Deliv. Rev. 2018, 129, 194–218. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, D.; Ghosh, B.; Mukhopadhyay, M. Development of nanotechnology for advancement and application in wound healing: A review. IET Nanobiotechnol. 2019, 13, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Alberti, T.; Coelho, D.S.; Voytena, A.; Pitz, H.; de Pra, M.; Mazzarino, L.; Kuhnen, S.; Ribeiro-do-Valle, R.M.; Maraschin, M.; Veleirinho, B. Nanotechnology: A Promising Tool Towards Wound Healing. Curr. Pharm. Des. 2017, 23, 3515–3528. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Fernandez, B.; Castano, O.; Mateos-Timoneda, M.Á.; Engel, E.; Pérez-Amodio, S. Nanotechnology Approaches in Chronic Wound Healing. Adv. Wound Care 2021, 10, 234–256. [Google Scholar] [CrossRef]
- Angle, M.R.; Cui, B.; Melosh, N.A. Nanotechnology and neurophysiology. Curr. Opin. Neurobiol. 2015, 32, 132–140. [Google Scholar] [CrossRef]
- Batool, S.; Nabipour, H.; Ramakrishna, S.; Mozafari, M. Nanotechnology and quantum science enabled advances in neurological medical applications: Diagnostics and treatments. Med. Biol. Eng. Comput. 2022, 60, 3341–3356. [Google Scholar] [CrossRef]
- Liu, X.; Chen, P.; Ding, X.; Liu, A.; Li, P.; Sun, C.; Guan, H. A narrative review of cortical visual prosthesis systems: The latest progress and significance of nanotechnology for the future. Ann. Transl. Med. 2022, 10, 716. [Google Scholar] [CrossRef]
- Jahed, Z.; Yang, Y.; Tsai, C.T.; Foster, E.P.; McGuire, A.F.; Yang, H.; Liu, A.; Forro, C.; Yan, Z.; Jiang, X.; et al. Nanocrown electrodes for parallel and robust intracellular recording of cardiomyocytes. Nat. Commun. 2022, 13, 2253. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Votruba, A.R.; Farokhzad, O.C.; Langer, R. Nanotechnology in drug delivery and tissue engineering: From discovery to applications. Nano Lett. 2010, 10, 3223–3230. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.; Dusek, J.A.; Taylor-Swanson, L.; Tick, H. Acupuncture Therapy as an Evidence-Based Nonpharmacologic Strategy for Comprehensive Acute Pain Care: The Academic Consortium Pain Task Force White Paper Update. Pain Med. 2022, 23, 1582–1612. [Google Scholar] [CrossRef] [PubMed]
- Crespin, D.J.; Griffin, K.H.; Johnson, J.R.; Miller, C.; Finch, M.D.; Rivard, R.L.; Anseth, S.; Dusek, J.A. Acupuncture Provides Short-term Pain Relief for Patients in a Total Joint Replacement Program. Pain Med. 2015, 16, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Fathi, M.; Ariamanesh, A.S.; Joudi, M.; Joudi, M.; Sadrossadati, F.; Izanloo, A. Hypnosis as an Approach to Control Pain and Anxiety in Anterior Cruciate Ligament Reconstruction and Meniscal Surgeries: Two Case Presentations. Anesth. Pain Med. 2019, 9, e89277. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.I.; Paley, C.A.; Jones, G.; Mulvey, M.R.; Wittkopf, P.G. Efficacy and safety of transcutaneous electrical nerve stimulation (TENS) for acute and chronic pain in adults: A systematic review and meta-analysis of 381 studies (the meta-TENS study). BMJ Open 2022, 12, e051073. [Google Scholar] [CrossRef] [PubMed]
- Gibson, W.; Wand, B.M.; Meads, C.; Catley, M.J.; O’Connell, N.E. Cochrane Pain, Palliative and Supportive Care Group. Transcutaneous electrical nerve stimulation (TENS) for chronic pain–an overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 2019, CD011890. [Google Scholar] [CrossRef]
- Chelly, J.E.; Orebaugh, S.L.; Rodosky, M.W.; Groff, Y.J.; Norton, B.E.; Monroe, A.L.; Alimi, D.; Sadhasivam, S.K.; Vogt, K.M. The Effect of Cryo-auriculotherapy on Post-Operative Pain Management following Rotator Cuff Surgery: A Randomized, Placebo-Controlled Study. medRxiv 2022. [Google Scholar] [CrossRef]
- Boye Larsen, D.; Laursen, M.; Simonsen, O.; Arendt-Nielsen, L.; Petersen, K.K. The association between sleep quality, preoperative risk factors for chronic postoperative pain and postoperative pain intensity 12 months after knee and hip arthroplasty. Br. J. Pain 2021, 15, 486–496. [Google Scholar] [CrossRef]
- Abeyrathne, C.D.; Halgamuge, M.N.; Farrell, P.M.; Skafidas, E. An ab-initio computational method to determine dielectric properties of biological materials. Sci. Rep. 2013, 3, 1796. [Google Scholar] [CrossRef]
- Fukada, E.; Ueda, H.; Rinaldi, R. Piezoelectric and related properties of hydrated collagen. Biophys. J. 1976, 16, 911–918. [Google Scholar] [CrossRef]
- Zhou, S.-A.; Uesaka, M. Bioelectrodynamics in living organisms. Int. J. Eng. Sci. 2006, 44, 67–92. [Google Scholar] [CrossRef]
- Tulip, P.R.; Clark, S.J. Lattice dynamical and dielectric properties of L-amino acids. Phys. Rev. B 2006, 74, 064301. [Google Scholar] [CrossRef]
- Netto, T.G.; Zimmerman, R.L. Effect of water on piezoelectricity in bone and collagen. Biophys. J. 1975, 15, 573–576. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All n = 69 | Control n = 31 | Treatment n = 38 | p-Value | |
|---|---|---|---|---|
| Sex | 0.47 | |||
| Male | 39 (57%) | 19 (61%) | 20 (53%) | |
| Female | 30 (43%) | 12 (39%) | 18 (47%) | |
| Age (years) | 68.7 (8.9) | 69.6 (9.0) | 68.0 (8.9) | 0.45 |
| Race | 0.23 | |||
| White | 60 (87%) | 25 (81%) | 35 (92%) | |
| African American | 7 (10%) | 5 (16%) | 2 (5%) | |
| American Indian/Alaska Native | 1 (1%) | 1 (3%) | 0 (0%) | |
| Asian | 1 (1%) | 0 (0%) | 1 (3%) | |
| Hispanic | 1 (1%) | 0 (0%) | 1 (3%) | 0.36 |
| Weight (kg) | 89.6 (14.2) | 89.1 (17.8) | 89.9 (10.6) | 0.82 |
| Height (cm) | 169.5 (11.3) | 169.0 (11.5) | 170.0 (11.4) | 0.71 |
| BMI (kg/m2) | 31.2 (4.7) | 30.9 (4.7) | 31.4 (4.8) | 0.60 |
| Surgery Type | 0.14 | |||
| Total Knee Arthroplasty | 60 (87%) | 29 (94%) | 31 (82%) | |
| Total Hip Arthroplasty | 9 (13%) | 2 (6%) | 7 (18%) | |
| PROMIS®—Anxiety | 46.2 (7.0) | 44.1 (7.5) | 48.0 (6.0) | 0.041 |
| PROMIS®—Emotional Distress—Depression | 41.3 (6.2) | 40.4 (4.7) | 41.9 (7.1) | 0.57 |
| PROMIS®—Sleep Disturbance | 49.6 (8.3) | 47.4 (9.3) | 51.4 (7.0) | 0.06 |
| Pain Catastrophizing | 6.3 (7.2) | 6.8 (8.4) | 5.8 (6.1) | 0.92 |
| Function | 3.6 (0.8) | 3.5 (1.0) | 3.7 (0.6) | 0.68 |
| Variable | Control (n = 31) | Treatment (n = 38) | Reduction % Compared with Control | p-Value |
|---|---|---|---|---|
| Pain at rest AUC | ||||
| n = 31 | n = 36 | |||
| POD 1-30 | 101.5 (75.8) | 59.4 (41.6) | 41% | 0.027 |
| n = 31 | n = 36 | |||
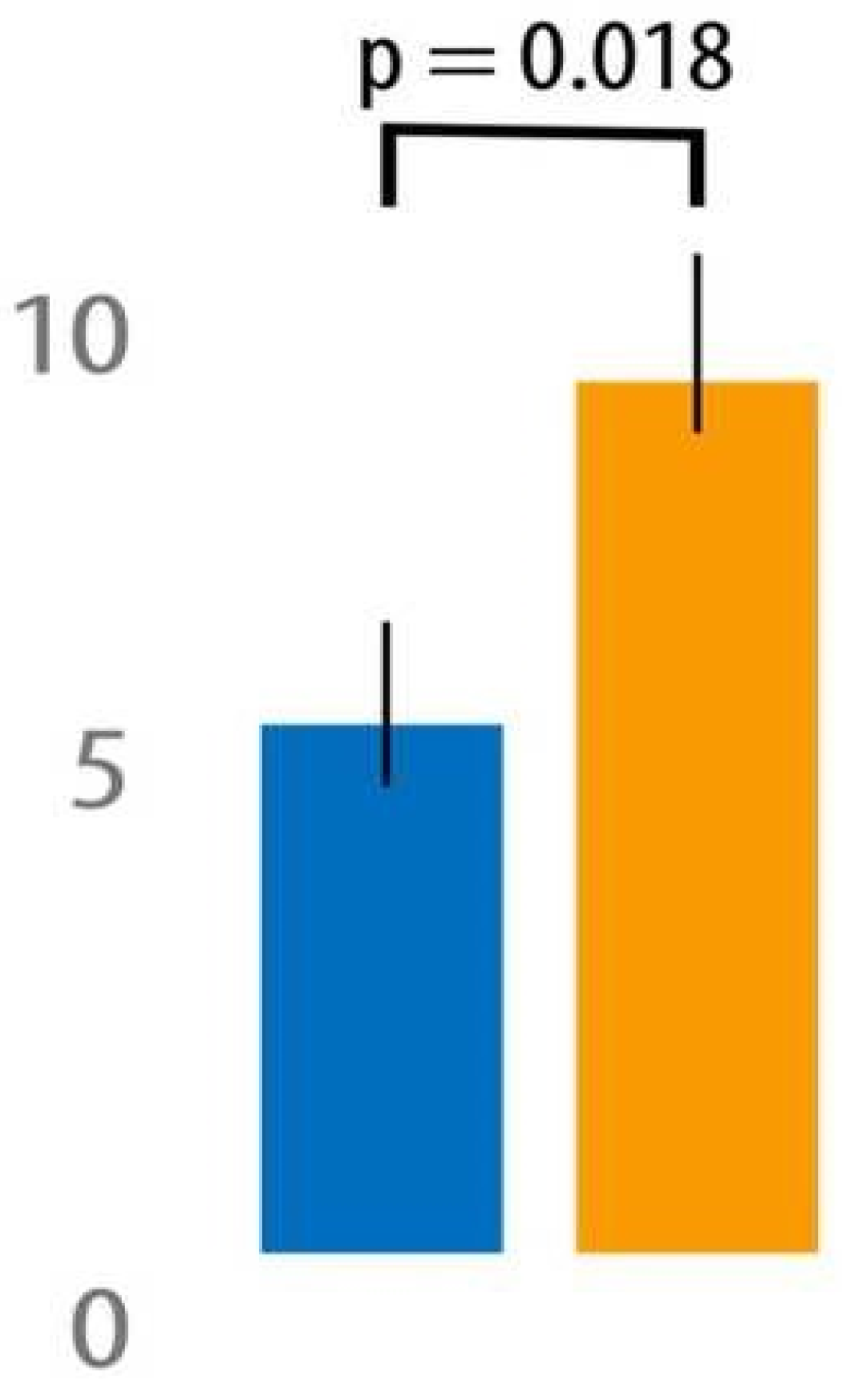
| POD 1-3 | 9.5 (5.6) | 6.3 (3.7) | 34% | 0.018 |
| n = 31 | n = 34 | |||
| POD 7-30 | 75.4 (61.2) | 44.0 (28.8) | 42% | 0.07 |
| Pain with movement AUC | ||||
| n = 31 | n = 36 | |||
| POD 1-30 | 140.2 (73.7) | 114.7 (54.5) | 18% | 0.12 |
| n = 31 | n = 36 | |||
| POD 1-3 | 13.7 (4.7) | 12.0 (4.7) | 12% | 0.12 |
| n = 31 | n = 34 | |||
| POD 7-30 | 101.5 (61.7) | 85.4 (38.2) | 16% | 0.35 |
| Total opioid OME (mg) | ||||
| n = 31 | n = 38 | |||
| POD 1-30 | 102.6 (74.0) | 82.1 (80.3) | 20% | 0.15 |
| n = 31 | n = 38 | |||
| POD 1-3 | 70.2 (53.8) | 63.6 (62.1) | 9% | 0.37 |
| n = 31 | n = 36 | |||
| POD 7-30 | 32.4 (41.7) | 19.5 (26.5) | 40% | 0.26 |
| Opioid refill after POD 3 | ||||
| n = 31 | n = 38 | |||
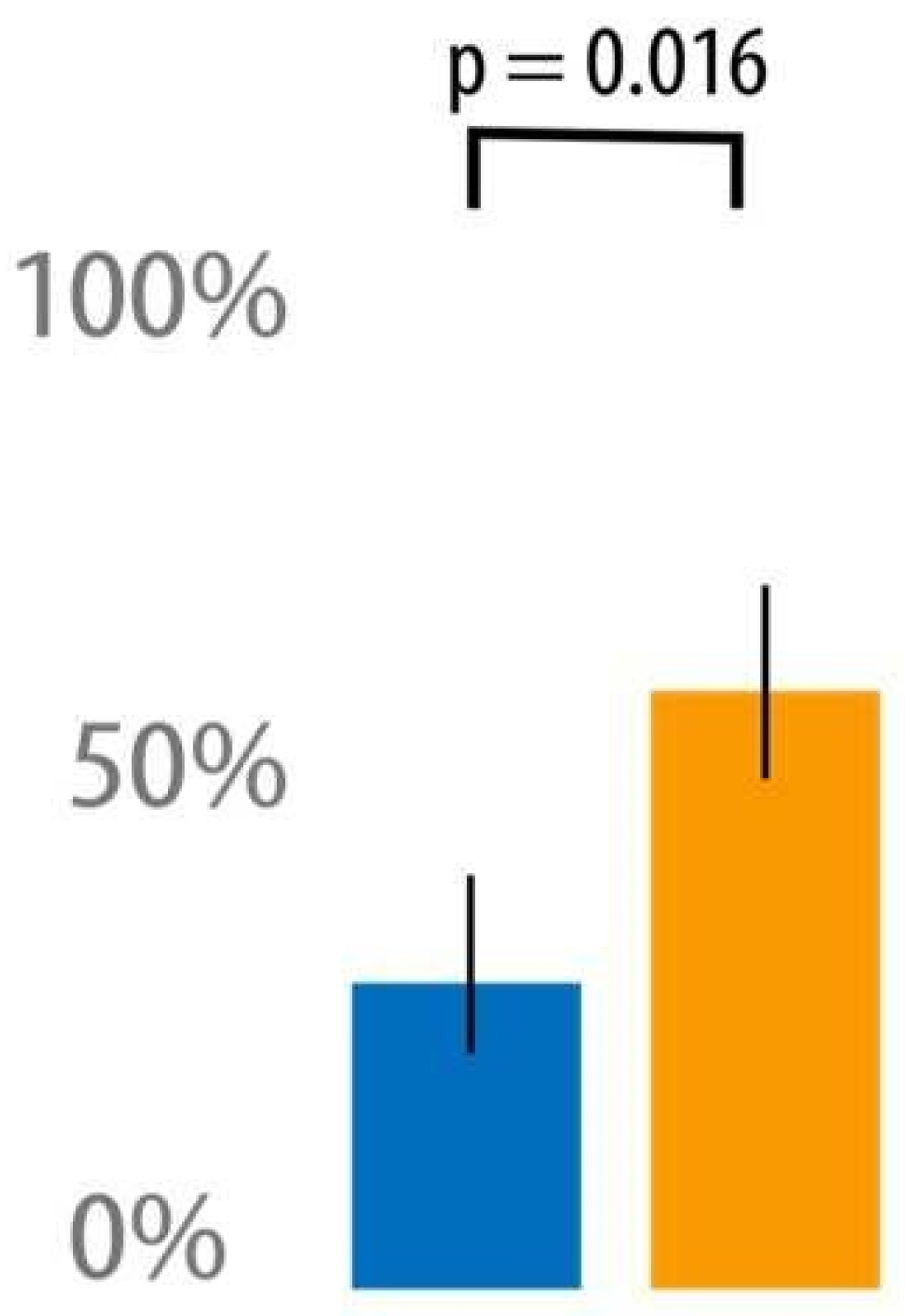
| POD 3-30 | 17 (55%) | 10 (26%) | 52% | 0.016 |
| n = 31 | n = 38 | |||
| Acetaminophen (mg) | ||||
| n = 31 | n = 38 | |||
| POD 1-30 | 10632.7 (4228.2) | 9801.3 (5130.1) | 8% | 0.53 |
| n = 31 | n = 38 | |||
| POD 1-3 | 5944.0 (2622.7) | 5750.7 (2805.3) | 3% | 0.68 |
| n = 31 | n = 35 | |||
| POD 7-30 | 4688.7 (2964.6) | 4397.9 (2964.7) | 6% | 0.62 |
| Ibuprofen (mg) | ||||
| n = 31 | n = 38 | |||
| POD 1-30 | 616.1 (1814.6) | 426.3 (964.1) | 31% | 0.82 |
| n = 31 | n = 38 | |||
| POD 1-3 | 409.7 (956.2) | 189.5 (351.7) | 54% | 0.98 |
| n = 31 | n = 35 | |||
| POD 7-30 | 206.5 (1011.2) | 257.1 (901.7) | (25%) | 0.50 |
| Gabapentin (mg) | ||||
| n = 31 | n = 38 | |||
| POD 1-30 | 391.9 (629.8) | 263.2 (341.2) | 33% | 0.61 |
| n = 31 | n = 38 | |||
| POD 1-3 | 314.5 (375.8) | 218.4 (244.8) | 31% | 0.53 |
| n = 31 | n = 35 | |||
| POD 7-30 | 77.4 (328.3) | 48.6 (150.2) | 37% | 0.84 |
| PACU min to discharge | n = 31 | n = 38 | ||
| 194.4 (72.9) | 166.5 (76.7) | 14% | 0.13 | |
| Hospital hours to discharge | n = 31 | n = 37 | ||
| 40.9 (36.2) | 31.6 (21.7) | 23% | 0.62 | |
| Satisfaction with care at discharge | n = 30 | n = 38 | ||
| 9.4 (1.6) | 9.7 (0.7) | (3%) | 0.97 | |
| Satisfaction for care at POD 30 | n = 30 | n = 34 | ||
| 9.3 (1.7) | 9.4 (1.1) | (1%) | 0.79 | |
| Satisfaction for pain management at POD 30 | n = 30 | n = 33 | ||
| 8.1 (2.7) | 9.0 (1.8) | (11%) | 0.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chelly, J.E.; Klatt, B.A.; Groff, Y.; O’Malley, M.; Lin, H.-H.S.; Sadhasivam, S. Role of the NeuroCuple™ Device for the Postoperative Pain Management of Patients Undergoing Unilateral Primary Total Knee and Hip Arthroplasty: A Pilot Prospective, Randomized, Open-Label Study. J. Clin. Med. 2023, 12, 7394. https://doi.org/10.3390/jcm12237394
Chelly JE, Klatt BA, Groff Y, O’Malley M, Lin H-HS, Sadhasivam S. Role of the NeuroCuple™ Device for the Postoperative Pain Management of Patients Undergoing Unilateral Primary Total Knee and Hip Arthroplasty: A Pilot Prospective, Randomized, Open-Label Study. Journal of Clinical Medicine. 2023; 12(23):7394. https://doi.org/10.3390/jcm12237394
Chicago/Turabian StyleChelly, Jacques E., Brian A. Klatt, Yram Groff, Michael O’Malley, Hsing-Hua Sylvia Lin, and Senthilkumar Sadhasivam. 2023. "Role of the NeuroCuple™ Device for the Postoperative Pain Management of Patients Undergoing Unilateral Primary Total Knee and Hip Arthroplasty: A Pilot Prospective, Randomized, Open-Label Study" Journal of Clinical Medicine 12, no. 23: 7394. https://doi.org/10.3390/jcm12237394
APA StyleChelly, J. E., Klatt, B. A., Groff, Y., O’Malley, M., Lin, H.-H. S., & Sadhasivam, S. (2023). Role of the NeuroCuple™ Device for the Postoperative Pain Management of Patients Undergoing Unilateral Primary Total Knee and Hip Arthroplasty: A Pilot Prospective, Randomized, Open-Label Study. Journal of Clinical Medicine, 12(23), 7394. https://doi.org/10.3390/jcm12237394