

Pain Coping and Healthcare Use in Patients with Early Knee and/or Hip Osteoarthritis: 10-Year Follow-Up Data from the Cohort Hip and Cohort Knee (CHECK) Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting and Study Population
2.3. Measurement Instruments
Main Study Parameters
2.4. Other Study Parameters
2.5. Statistical Analysis
3. Results
3.1. Change in Pain Intensity and Health Status
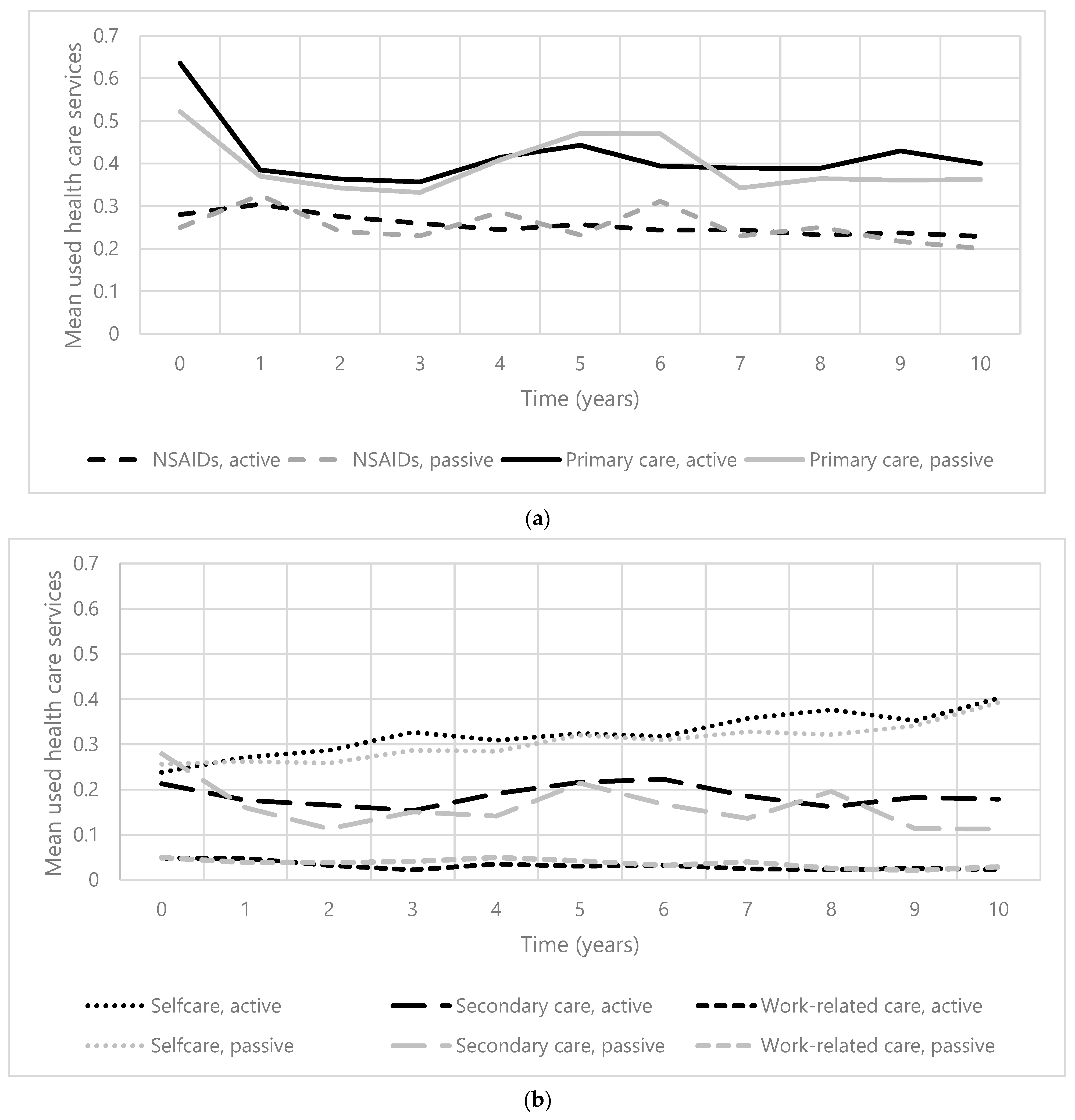
3.2. Course of Healthcare Use
3.3. Relationship Pain Coping Style and HCU
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allen, K.D.; Golightly, Y.M. Epidemiology of osteoarthritis: State of the evidence. Curr. Opin. Rheumatol. 2015, 27, 276–283. [Google Scholar] [CrossRef]
- Wang, S.X.; Ganguli, A.X.; Bodhani, A.; Medema, J.K.; Reichmann, W.M.; Macaulay, D. Healthcare resource utilization and costs by age and joint location among osteoarthritis patients in a privately insured population. J. Med. Econ. 2017, 20, 1299–1306. [Google Scholar] [CrossRef]
- Musumeci, G.; Aiello, F.C.; Szychlinska, M.A.; Di Rosa, M.; Castrogiovanni, P.; Mobasheri, A. Osteoarthritis in the XXIst century: Risk factors and behaviours that influence disease onset and progression. Int. J. Mol. Sci. 2015, 16, 6093–6112. [Google Scholar] [CrossRef]
- Bijlsma, J.W.J.; Berenbaum, F.; Lafeber, F.P.J.G. Osteoarthritis: An update with relevance for clinical practice. Lancet 2011, 377, 2115–2126. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Kovic, B.; Jin, X.; He, X.; Wang, M.; Silvestre, C. Economic and Humanistic Burden of Osteoarthritis: A Systematic Review of Large Sample Studies. Pharmacoeconomics 2016, 34, 1087–1100. [Google Scholar] [CrossRef]
- Luyten, F.P.; Bierma-Zeinstra, S.; Dell’Accio, F.; Kraus, V.B.; Nakata, K.; Sekiya, I.; Arden, N.K.; Lohmander, L.S. Toward classification criteria for early osteoarthritis of the knee. Semin. Arthritis Rheum. 2018, 47, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Im, G.I. The Concept of Early Osteoarthritis and Its Significance in Regenerative Medicine. Tissue Eng. Regen. Med. 2022, 19, 431–436. [Google Scholar] [CrossRef]
- Hoogeboom, T.J.; Snijders, G.F.; Cats, H.A.; De Bie, R.A.; Bierma-Zeinstra, S.M.A.; Van Den Hoogen, F.H.J.; van Riel, P.L.C.M.; Emans, P.J.; Wesseling, J.; den Broeder, A.A.; et al. Prevalence and predictors of health care use in patients with early hip or knee osteoarthritis: Two-year follow-up data from the CHECK cohort. Osteoarthr. Cartil. 2012, 20, 525–531. [Google Scholar] [CrossRef]
- Kampshoff, C.S.; Peter, W.F.H.; van Doormaal, M.C.M.; Knoop, J.; Meerhoff, G.A.; Vliet Vlieland, T.P.M. KNGF-Richtlijn: Artrose Heup-Knie; Koninklijk Genootschap voor Fysiotherapie: Amersfoort, The Netherlands, 2018. [Google Scholar]
- Barten, D.J.J.A.; Swinkels, C.S.; Dorsman, S.A.; Dekker, J.; Veenhof, C.; De Bakker, D.H. Treatment of hip/knee osteoarthritis in Dutch general practice and physical therapy practice: An observational study. BMC Fam. Pract. 2015, 16, 75. [Google Scholar] [CrossRef]
- Picavet, H.; Hoeymans, N. Health related quality of life in multiple musculoskeletal diseases: SF-36 and EQ-5D in the DMC3 study. Ann. Rheum. Dis. 2004, 63, 723. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Carvalho, C.; Costa, E.; Leite, Â.; Almeida, V. Quality of life in chronic pain patients: Illness- and wellness-focused coping as moderators. Psych J. 2021, 10, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Perrot, S.; Poiraudeau, S.; Kabir, M.; Bertin, P.; Sichere, P.; Serrie, A.; Rannou, F. Active or passive pain coping strategies in hip and knee osteoarthritis? Results of a national survey of 4719 patients in a primary care setting. Arthritis Care Res. 2008, 59, 1555–1562. [Google Scholar] [CrossRef]
- Steultjens, M.P.M.; Dekker, J.; Bijlsma, J.W.J. Coping, pain, and disability in osteoarthritis: A longitudinal study. J. Rheumatol. 2001, 28, 1068–1072. [Google Scholar] [PubMed]
- Kraaimaat, F.W.; Evers, A.W.M. Pain-Coping Strategies in Chronic Pain Patients: Psychometric Characteristics of the Pain-Coping Inventory (PCI). Int. J. Beh Med. 2003, 10, 343–363. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.K.; Nicassio, P.M.; Rsyckoloenr, O. Development of a questionnaire for the assessment of active and passive coping strategies in chronic pain patients. Pain 1987, 31, 53–64. [Google Scholar] [CrossRef]
- Aciksoz, S.; Uzun, S. Evaluation of the Coping Strategies Used by Knee Osteoarthritis Patients for Pain and Their Effect on the Disease-Specific Quality of Life. Int. J. Caring Sci. 2016, 9, 80–90. [Google Scholar] [CrossRef]
- Higgins, N.C.; Bailey, S.J.; LaChapelle, D.L.; Harman, K.; Hadjistavropoulos, T. Coping Styles, Pain Expressiveness, and Implicit Theories of Chronic Pain. J. Psychol. 2015, 149, 737–750. [Google Scholar] [CrossRef]
- Pisters, M.F.; Veenhof, C.; van Dijk, G.M.; Heymans, M.W.; Twisk, J.W.R.; Dekker, J. The course of limitations in activities over 5 years in patients with knee and hip osteoarthritis with moderate functional limitations: Risk factors for future functional decline. Osteoarthr. Cartil. 2012, 20, 503–510. [Google Scholar] [CrossRef]
- Büssing, A.; Ostermann, T.; Am Neugebauer, E.; Heusser, P. Adaptive coping strategies in patients with chronic pain conditions and their interpretation of disease. BMC Public. Health 2010, 10, 507. [Google Scholar] [CrossRef]
- Eisenbarth, C. Coping profiles & psychological distress: A cluster analysis. N. Am. J. Psychol. 2012, 14, 485–496. [Google Scholar] [CrossRef]
- Regier, N.G.; Parmelee, P.A.; Hopkins, J. The stability of coping strategies in older adults with osteoarthritis and the ability of these strategies to predict changes in depression, disability, and pain HHS Public Access. Aging Ment. Health 2015, 19, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Smink, A.J.; Dekker, J.; Vliet Vlieland, T.P.M.; Swierstra, B.A.; Kortland, J.H.; Bijlsma, J.W.J.; Teerenstra, S.; Voorn, T.B.; Bierma-Zeinstra, S.M.A.; Schers, H.J.; et al. Health Care Use of Patients with Osteoarthritis of the Hip or Knee After Implementation of a Stepped-Care Strategy: An Observational Study. Arthritis Care Res. 2014, 66, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, J.; Boers, M.; Viergever, M.A.; Hilberdink, W.K.H.A.; Lafeber, F.P.J.G.; Dekker, J.; Bijlsma, J.W. Cohort profile: Cohort Hip and Cohort Knee (CHECK) study. Int. J. Epidemiol. 2016, 45, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Altman, R.; Alarcón, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Feldman, D.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991, 34, 505–514. [Google Scholar] [CrossRef]
- Wesseling, J.; Dekker, J.; Van Den Berg, W.B.; Bierma-Zeinstra, S.M.A.; Boers, M.; Cats, H.A.; Deckers, P.; Gorter, K.J.; Heuts, P.H.T.G.; Hilberdink, W.K.H.A.; et al. CHECK (Cohort Hip and Cohort Knee): Similarities and differences with the Osteoarthritis Initiative. Ann. Rheum. Dis. 2009, 68, 1413–1419. [Google Scholar] [CrossRef]
- Swinkels, H. Het meten van medische consumptie met behulp van enquetes. In Het Meten van Determinanten van Gezondheid: Een Overzicht van Beschikbare Meetinstrumenten; Ned Tijdschr Geneeskd: Assen, The Netherlands, 1995. [Google Scholar]
- Verstappen, S.M.M.; Boonen, A.; Verkleij, H.; Bijlsma, J.W.J.; Buskens, E.; Jacobs, J.W.G. Productivity costs among patients with rheumatoid arthritis: The influence of methods and sources to value loss of productivity. Ann. Rheum. Dis. 2005, 64, 1754–1760. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS) and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, 240–252. [Google Scholar] [CrossRef]
- Gandek, B. Measurement properties of the Western Ontario and McMaster Universities Osteoarthritis Index: A systematic review. Arthritis Care Res. 2015, 67, 216–229. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.E.; Harper, R.; B Jones, N.M.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.W.R. Applied Longitudinal Data Analysis for Epidemiology: A Practical Guide, 1st ed.; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Liu, Y.; De, A. Multiple Imputation by Fully Conditional Specification for Dealing with Missing Data in a Large Epidemiologic Study. Int. J. Stat. Med. Res. 2015, 4, 287–295. [Google Scholar] [CrossRef]
- Marshall, A.; Altman, D.G.; Holder, R.L.; Royston, P. Combining estimates of interest in prognostic modelling studies after multiple imputation: Current practice and guidelines. BMC Med. Res. Methodol. 2009, 9, 1471–1479. [Google Scholar] [CrossRef] [PubMed]
- Thabane, L.; Mbuagbaw, L.; Zhang, S.; Samaan, Z.; Marcucci, M.; Ye, C.; Thabane, M.; Giangregorio, L.; Dennis, B.; Kosa, D.; et al. A tutorial on sensitivity analyses in clinical trials: The what, why, when and how. BMC Med. Res. Methodol. 2013, 13, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Smink, A.J.; Van Den Ende, C.H.M.; Vliet Vlieland, T.P.M.; Swierstra, B.A.; Kortland, J.H.; Bijlsma, J.W.J.; Voorn, T.B.; Schers, H.J.; Bierma-Zeinstra, S.M.A.; Dekker, J. “Beating osteoARThritis”: Development of a stepped care strategy to optimize utilization and timing of non-surgical treatment modalities for patients with hip or knee osteoarthritis. Clin. Rheumatol. 2011, 30, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Legler, J.; Roback, P. Broadening Your Statistical Horizons: Generalized Linear Models and Multilevel Models, 1st ed.; CRC Press: Boco Raton, FL, USA, 2019. [Google Scholar]
- Lee, P.H. Is a cutoff of 10% appropriate for the change-in-estimate criterion of confounder identification? J. Epidemiol. 2014, 24, 161–167. [Google Scholar] [CrossRef]
- Zhang, W.; Nuki, G.; Moskowitz, R.; Abramson, S.; Altman, R.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis: Part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthr. Cartil. 2010, 18, 476–499. [Google Scholar] [CrossRef]
- Barlow, J. How to use education as an intervention in osteoarthritis. Best. Pract. Res. Clin. Rheumatol. 2001, 15, 545–558. [Google Scholar] [CrossRef]
- Brady, T. Strategies to support self-management in osteoarthritis. Am. J. Nurs. 2012, 112, S54–S60. [Google Scholar] [CrossRef]
- McKnight, P.E.; Kasle, S.; Going, S.; Villanueva, I.; Cornett, M.; Farr, J.; Wright, J.; Streeter, C.; Zautra, A. A comparison of strength training, self-management, and the combination for early osteoarthritis of the knee. Arthritis Care Res. 2010, 62, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhou, R.; Zhu, Y.; Zeng, Z.; Ye, Z.; Wang, Z.; Liu, W.; Xu, X. Self-Management for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain. Res. Manag. 2022, 2022, 2681240. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.; Briffa, N.K.; Carroll, G.; Inderjeeth, C.; Cook, N.; McQuade, J. A randomised controlled trial of a self-management education program for osteoarthritis of the knee delivered by health care professionals. Arthritis Res. Ther. 2012, 14, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Ritter, P.; Stewart, A.L.; Sobel, D.S.; Brown, B.W.; Bandura, A.; Gonzalez, V.M.; Laurent, D.D.; Holman, H.R. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med. Care. 2001, 39, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Sobel, D.S.; Ritter, P.L.; Laurent, D.; Hobbs, M. Effect of a self-management program on patients with chronic disease. Eff. Clin. Pract. 2001, 4, 256–262. [Google Scholar] [PubMed]
- Elzen, H.; Slaets, J.P.J.; Snijders, T.A.B.; Steverink, N. The effect of a self-management intervention on health care utilization in a sample of chronically ill older patients in the Netherlands. J. Eval. Clin. Pract. 2008, 14, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Goeppinger, J.; Armstrong, B.; Schwartz, T.; Ensley, D.; Brady, T.J. Self-management education for persons with arthritis: Managing comorbidity and eliminating health disparities. Arthritis Care Res. 2007, 57, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Franek, J. Self-management support interventions for persons with chronic disease: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2013, 13, 1–60. [Google Scholar]
- Michaëlis, C.; Kristiansen, M.; Norredam, M. Quality of life and coping strategies among immigrant women living with pain in Denmark: A qualitative study. BMJ Open. 2015, 5, e8075. [Google Scholar] [CrossRef]
- Tamres, L.K.; Janicki, D.; Helgeson, V.S. Sex Differences in Coping Behavior: A Meta-Analytic Review and an Examination of Relative Coping. Personal. Soc. Psychol. Rev. 2002, 6, 2–30. [Google Scholar] [CrossRef]
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and hip osteoarthritis: The minimal clinically important improvement. Ann. Rheum. Dis. 2005, 64, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Cronan, T.A.; Walen, H.R. Accuracy of self-reported healthcare use in patients with osteoarthritis. J. Rheumatol. 2002, 29, 2181–2184. [Google Scholar] [PubMed]
- Coupé, V.M.H.; Veenhof, C.; Van Tulder, M.W.; Dekker, J.; Bijlsma, J.W.J.; Van Den Ende, C.H.M. The cost effectiveness of behavioural graded activity in patients with osteoarthritis of hip and/or knee. Ann. Rheum. Dis. 2007, 66, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Gore, M.; Tai, K.S.; Sadosky, A.; Leslie, D.; Stacey, B.R. Clinical comorbidities, treatment patterns, and direct medical costs of patients with osteoarthritis in usual care: A retrospective claims database analysis. J. Med. Econ. 2011, 14, 497–507. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics at Baseline | All Participants | Participants with an Active Pain Coping Style | Participants with a Passive Pain Coping Style |
|---|---|---|---|
| Number (%) | 861 | 745 (86.5) | 116 (13.5) |
| Age, mean (SD) | 56 (5.2) | 56 (5.3) | 56 (5.0) |
| Sex, female (%) | 81.1% | 81.2% | 79.9% |
| BMI, median (IQR) | 26 (24–28) | 26 (23–28) | 26 (24–29) |
| Location OA | |||
| Hip | 15.3% | 15.6% | 12.8% |
| Knee | 37.2% | 36.2% | 43.5% |
| Knee and hip | 47.5% | 48.1% | 43.7% |
| Comorbidities | |||
| 0 | 25.9% | 26.2% | 24.0% |
| 1 | 30.2% | 30.0% | 31.7% |
| 2 | 21.4% | 22.0% | 17.6% |
| 3 | 12.7% | 12.3% | 15.3% |
| ≥4 | 9.8% | 9.5% | 11.4% |
| Married/partnership, yes | 83.0% | 83.5% | 79.6% |
| Level of education | |||
| No/primary school | 20.1% | 19.6% | 23.5% |
| Secondary (vocational) education | 46.9% | 47.7% | 42.2% |
| Higher education/university | 33.0% | 32.7% | 34.3% |
| Employed, yes | 39.9% | 40.6% | 35.8% |
| Pain intensity (0–10), mean (SD) | |||
| Right now | 3.2 (2.1) | 3.2 (2.0) | 3.0 (2.2) |
| Past week | 3.7 (2.1) | 3.7 (2.1) | 3.5 (2.1) |
| WOMAC subscales standardized (0–100), median (IQR) | |||
| Pain | 25 (15–35) | 25 (15–35) | 25 (10–40) |
| Stiffness | 37.5 (25–50) | 37.5 (25–50) | 37.5 (12.5–50) |
| Function | 22.1 (11.8–35.3) | 22.1 (11.8–35.3) | 22.1 (13.2–36.8) |
| T10 | Δ T0–T10 | |||
|---|---|---|---|---|
| Active Pain Coping Style | Passive Pain Coping Style | Active Pain Coping Style | Passive Pain Coping Style | |
| Pain intensity (0–10), mean (SD) | ||||
| Right now | 3.3 (2.4) | 2.7 (2.3) | +0.1 | −0.3 |
| Past week | 3.7 (2.4) | 3.2 (2.3) | 0 | −0.3 |
| WOMAC subscales standardized (0–100), median (IQR) | ||||
| Pain | 21 (IQR: 10–35) | 15 (IQR: 5–35) | −4 | −10 |
| Stiffness | 25 (IQR: 20–20) | 25 (IQR: 12.5–50) | −12.5 | −12.5 |
| Function | 20.6 (IQR: 8.8–35.3) | 19.1 (IQR: 8.8–39.7) | −2.5 | −3 |
| Number of Used Healthcare Services | |||
|---|---|---|---|
| Parameters | B [95% CI] | IRR [95% CI] | p |
| Pain coping style (passive = 0; active = 1) | 0.080 [−0.061; 0.329] | 1.083 [0.940; 1.390] | 0.453 |
| Pain coping style * (passive = 0; active = 1) | 0.153 [0.022; 0.283] | 1.165 [1.020; 1.327] | 0.022 |
| Number of Used Healthcare Services | |||
|---|---|---|---|
| Subgroup | B [95% CI] | IRR [95% CI] | p |
| Primary care | 0.169 [0.011–0.327] | 1.184 [1.011–1.387] | 0.037 |
| Secondary care | 0.186 [−0.047–0.420] | 1.204 [0.954–1.522] | 0.117 |
| Self-care | 0.170 [−0.043–0.383] | 1.185 [0.958–1.467] | 0.118 |
| NSAIDs | 0.103 [−0.101–0.307] | 1.108 [0.904–1.359] | 0.324 |
| Work-related care | −0.024 [−0.487–0.440] | 0.976 [0.614–1.553] | 0.920 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Scherpenseel, M.C.; Kloek, C.J.J.; Veenhof, C.; Pisters, M.F. Pain Coping and Healthcare Use in Patients with Early Knee and/or Hip Osteoarthritis: 10-Year Follow-Up Data from the Cohort Hip and Cohort Knee (CHECK) Study. J. Clin. Med. 2023, 12, 7455. https://doi.org/10.3390/jcm12237455
van Scherpenseel MC, Kloek CJJ, Veenhof C, Pisters MF. Pain Coping and Healthcare Use in Patients with Early Knee and/or Hip Osteoarthritis: 10-Year Follow-Up Data from the Cohort Hip and Cohort Knee (CHECK) Study. Journal of Clinical Medicine. 2023; 12(23):7455. https://doi.org/10.3390/jcm12237455
Chicago/Turabian Stylevan Scherpenseel, Meike C., Corelien J. J. Kloek, Cindy Veenhof, and Martijn F. Pisters. 2023. "Pain Coping and Healthcare Use in Patients with Early Knee and/or Hip Osteoarthritis: 10-Year Follow-Up Data from the Cohort Hip and Cohort Knee (CHECK) Study" Journal of Clinical Medicine 12, no. 23: 7455. https://doi.org/10.3390/jcm12237455
APA Stylevan Scherpenseel, M. C., Kloek, C. J. J., Veenhof, C., & Pisters, M. F. (2023). Pain Coping and Healthcare Use in Patients with Early Knee and/or Hip Osteoarthritis: 10-Year Follow-Up Data from the Cohort Hip and Cohort Knee (CHECK) Study. Journal of Clinical Medicine, 12(23), 7455. https://doi.org/10.3390/jcm12237455