
Association between Physical Activity and Reduced Mortality in Inoperable Lung Cancer

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Data Collection
2.3. Outcomes
2.3.1. Physical Activity and Sedentary Behaviour
2.3.2. Muscle Force
2.3.3. Clinical Covariates
2.3.4. 12-Month Mortality
2.4. Sample Size
2.5. Statistical Analysis
3. Results
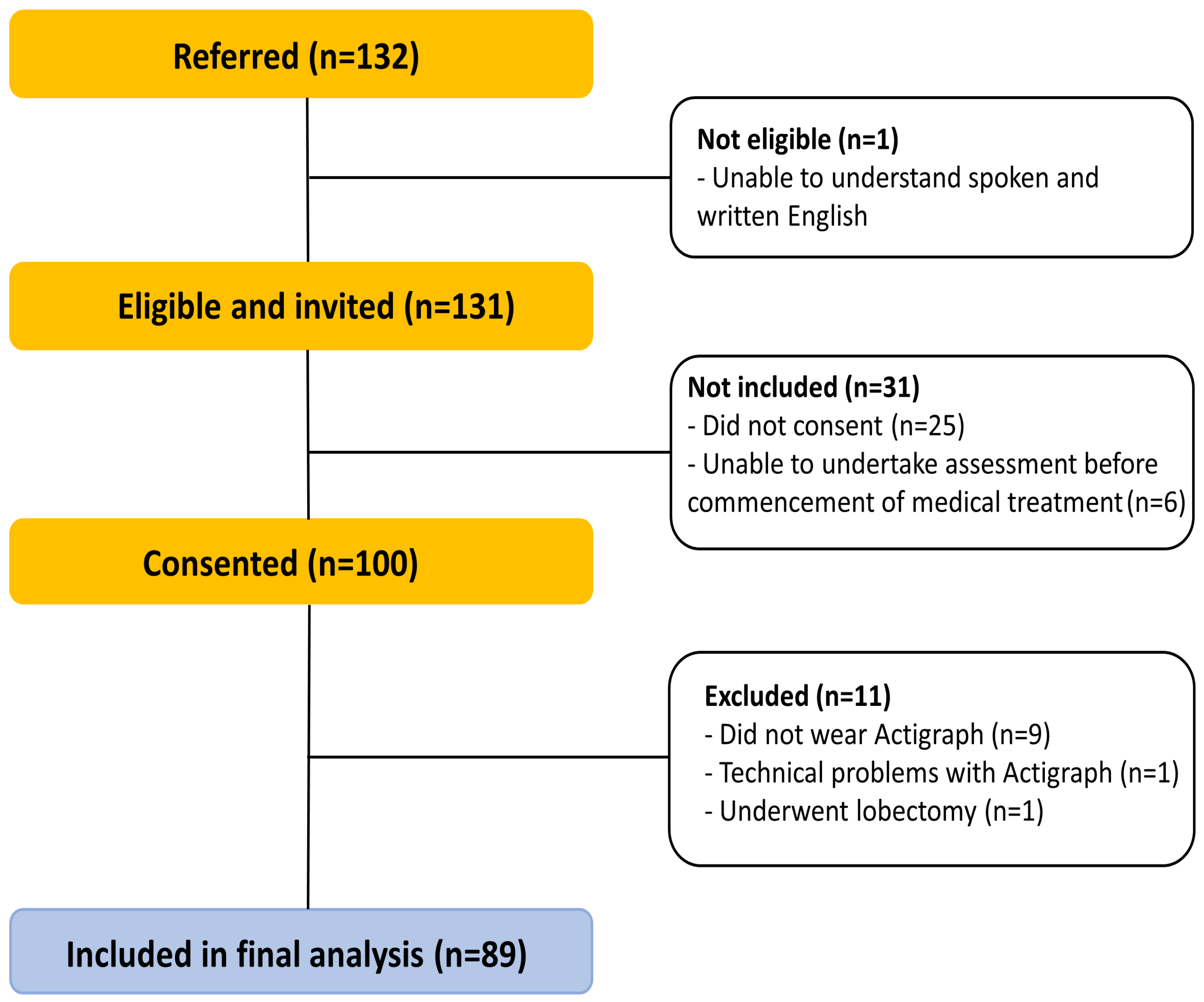
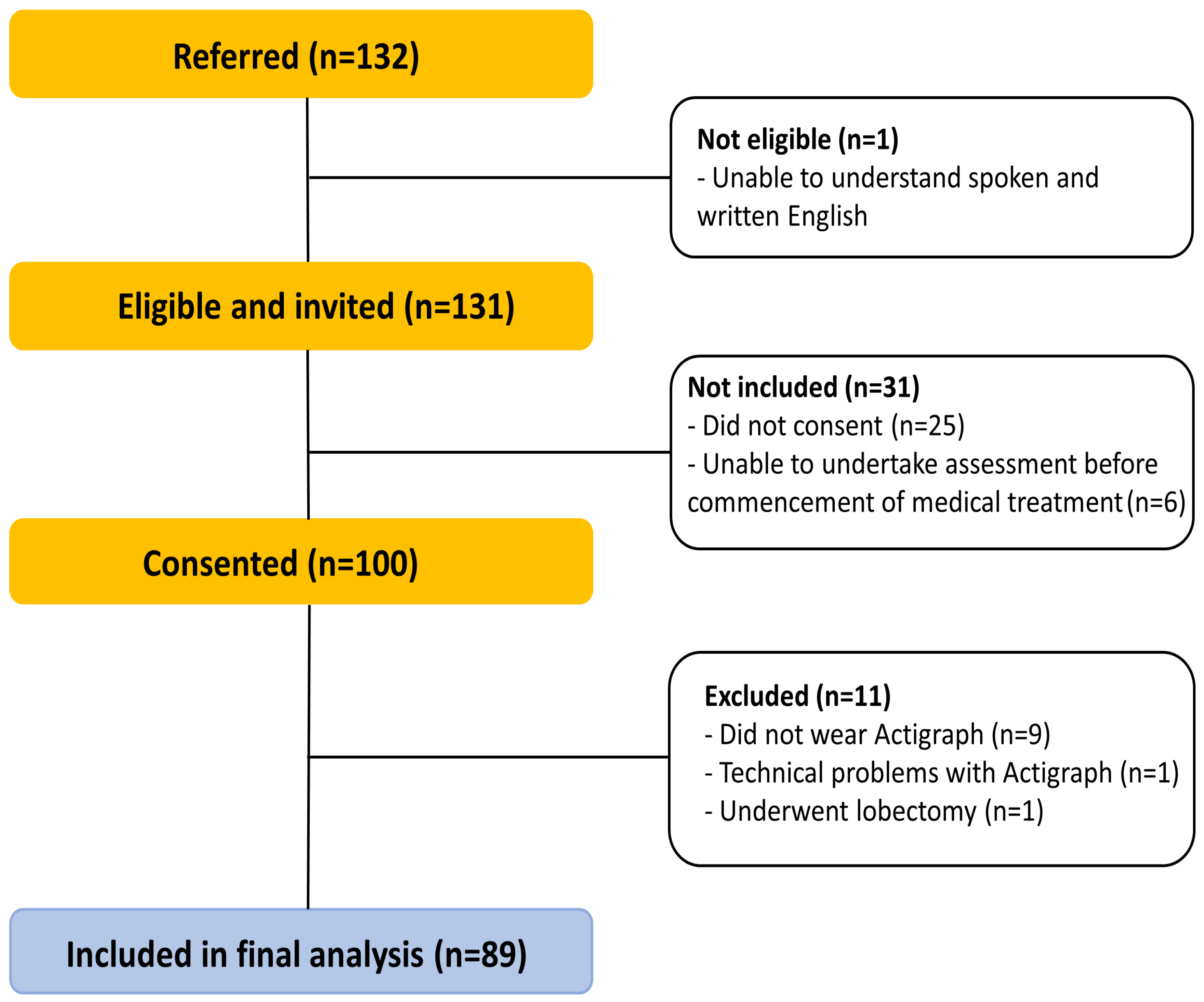
3.1. Participants
3.2. Participant Characteristics, Mortality Rate and Group Comparison
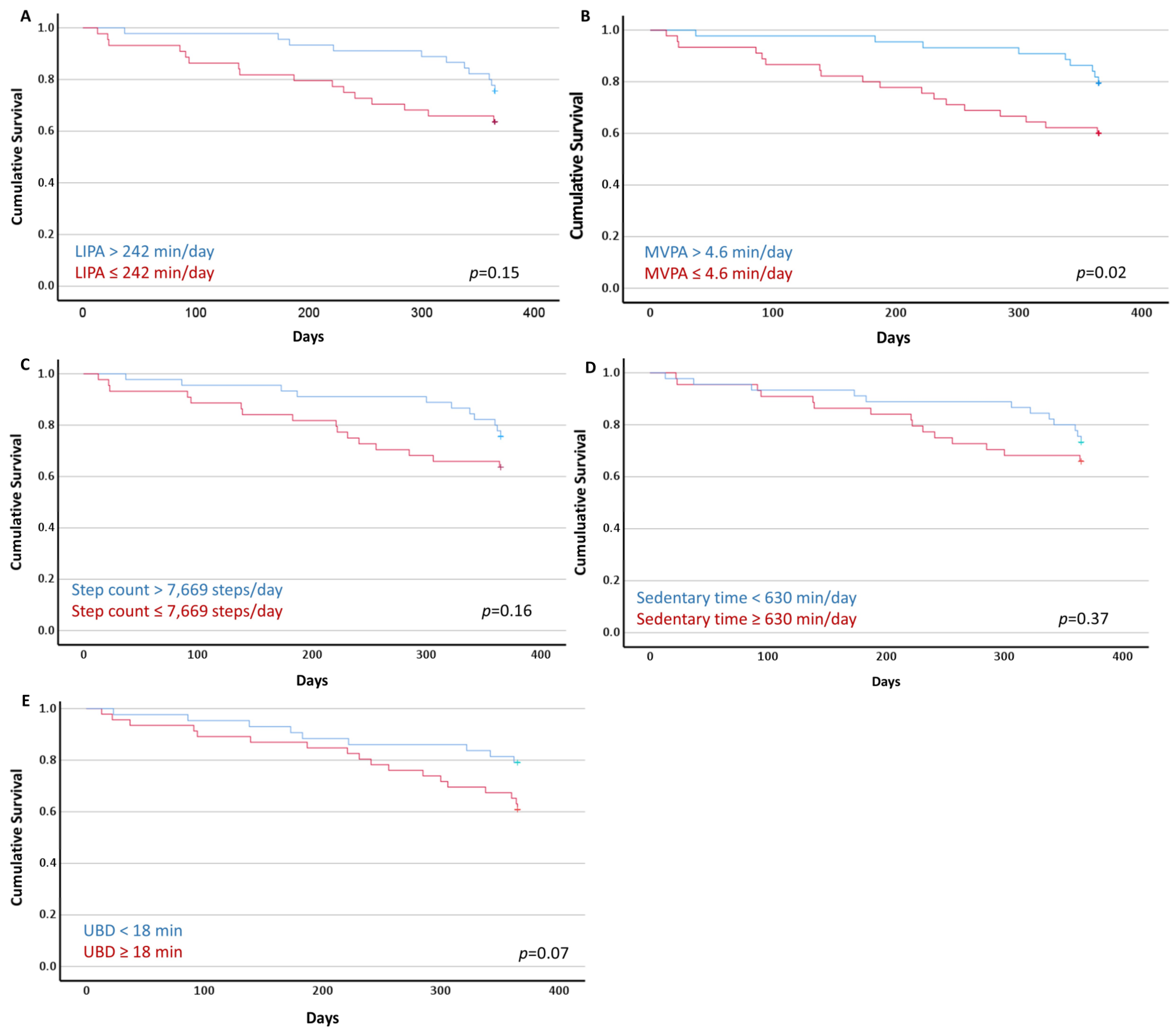
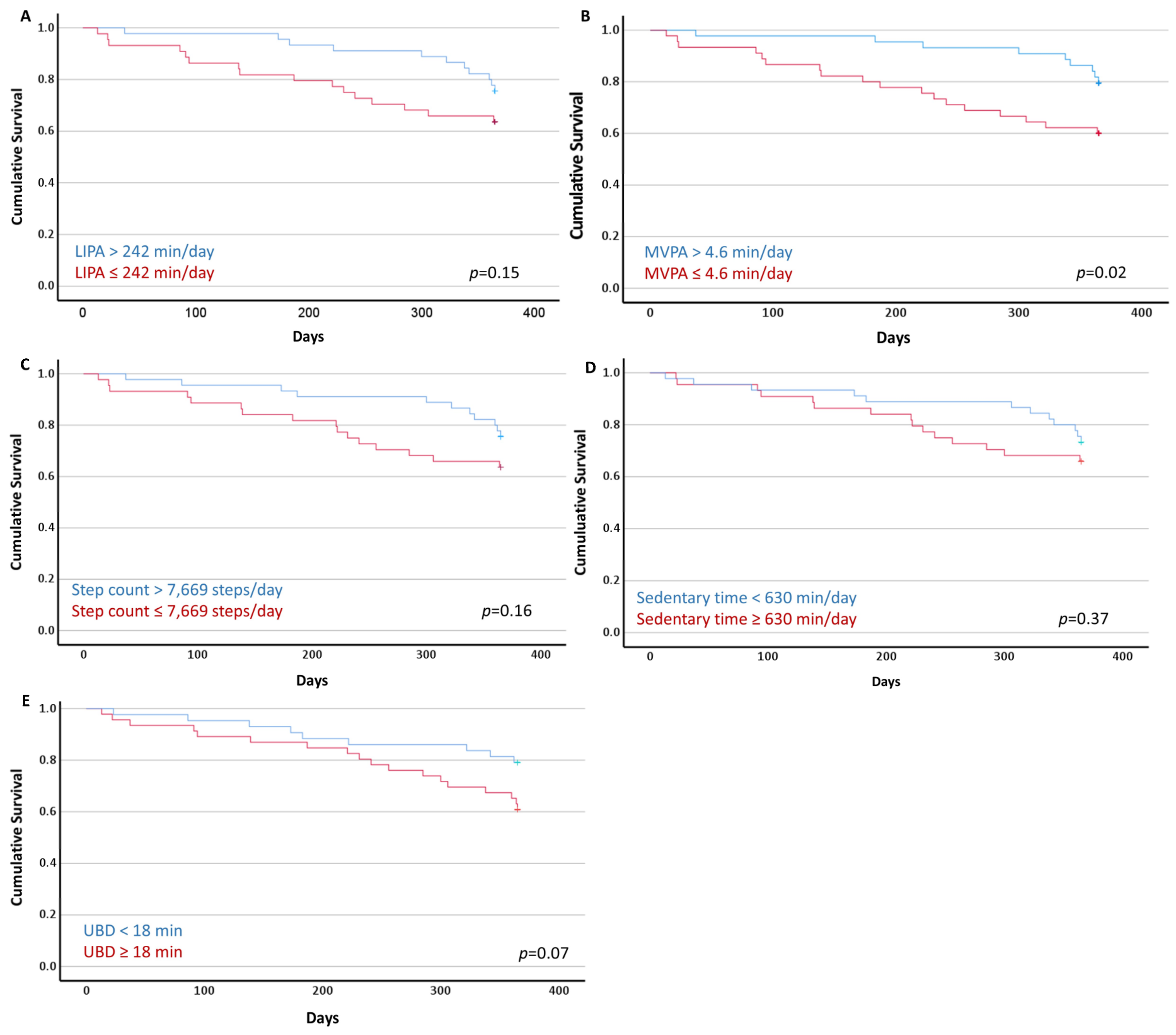
3.3. Survivor Curves and Cox Regression Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Cancer. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 8 November 2023).
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Non-Small Cell Lung Cancer Treatment (PDQ®)–Health Professional Version. 2023. Available online: https://www.cancer.gov/types/lung/hp/non-small-cell-lung-treatment-pdq#_4 (accessed on 8 November 2023).
- Cavalheri, V.; Jenkins, S.; Cecins, N.; Phillips, M.; Sanders, L.H.; Hill, K. Patterns of sedentary behaviour and physical activity in people following curative intent treatment for non-small cell lung cancer. Chronic Respir. Dis. 2016, 13, 82–85. [Google Scholar] [CrossRef]
- Edbrooke, L.; Granger, C.L.; Clark, R.A.; Denehy, L. Physical activity levels are low in inoperable lung cancer: Exploratory analyses from a randomised controlled trial. J. Clin. Med. 2019, 8, 1288. [Google Scholar] [CrossRef]
- Athey, V.L.; Suckling, R.J.; Tod, A.M.; Walters, S.J.; Rogers, T.K. Early diagnosis of lung cancer: Evaluation of a community-based social marketing intervention. Thorax 2012, 67, 412–417. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.; Matthews, C.; Ligibel, J.; Gerber, L.; et al. Exercise guidelines for cancer survivors: Consensus statement from international multidisciplinary roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Kari, B.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, diet, and weight management during cancer treatment: ASCO guideline. J. Clin. Oncol. 2022, 40, 2491–2507. [Google Scholar] [CrossRef]
- Cheryl, L.R.; Thomson, C.A.; Kristen, R.S.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar]
- Ch’ng, S.N.; McVeigh, J.A.; Manners, D.; Boyle, T.; Peddle-McIntyre, C.J.; Thomas, R.; Leong, J.; Bowyer, S.; Mooney, K.; Straker, L.; et al. Sedentary behaviour, physical activity, and their associations with health outcomes at the time of diagnosis in people with inoperable lung cancer. J. Clin. Med. 2022, 11, 5870. [Google Scholar] [CrossRef]
- Arem, H.; Pfeiffer, R.M.; Engels, E.A.; Alfano, C.M.; Hollenbeck, A.; Park, Y.; Matthews, C.E. Pre- and postdiagnosis physical activity, television viewing, and mortality among patients with colorectal cancer in the National Institutes of Health-AARP Diet and Health Study. J. Clin. Oncol. 2015, 33, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Lee, H. Rationale for promoting physical activity among cancer survivors: Literature review and epidemiologic examination. Oncol. Nurs. Forum 2014, 41, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Waschki, B.; Kirsten, A.; Holz, O.; Müller, K.-C.; Meyer, T.; Watz, H.; Magnussen, H. Physical activity is the strongest predictor of all-cause mortality in patients with chronic obstructive pulmonary disease: A prospective cohort study. Chest 2011, 140, 331–342. [Google Scholar] [CrossRef]
- Furlanetto, K.C.; Donária, L.; Schneider, L.P.; Lopes, J.R.; Ribeiro, M.; Fernandes, K.B.; Hernandes, N.A.; Sedentary, F.P. behavior is an independent predictor of mortality in subjects with chronic obstructive pulmonary disease. Respir. Care 2017, 62, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Qian, L.; Cui, J. Value of neutrophil-to-lymphocyte ratio for predicting lung cancer prognosis: A meta-analysis of 7219 patients. Mol. Clin. Oncol. 2017, 7, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Chen, Y.-J.; Narsavage, G.L.; Ducatman, A. Predictors of survival in patients with non-small cell lung cancer. Oncol. Nurs. Forum 2012, 39, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Maione, P.; Perrone, F.; Gallo, C.; Manzione, L.; Piantedosi, F.; Barbera, S.; Cigolari, S.; Rosetti, F.; Piazza, E.; Robbiati, S.F.; et al. Pretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non-small-cell lung cancer receiving chemotherapy: A prognostic analysis of the multicenter Italian lung cancer in the elderly study. J. Clin. Oncol. 2005, 23, 6865–6872. [Google Scholar] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Pitta, F.; Troosters, T.; Spruit, M.A.; Probst, V.S.; Decramer, M.; Gosselin, R. Characteristics of physical activities in daily life in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2005, 171, 972–977. [Google Scholar] [CrossRef] [PubMed]
- McVeigh, J.A.; Winkler, E.A.H.; Healy, G.N.; Slater, J.; Eastwood, P.R.; Straker, L.M. Validity of an automated algorithm to identify waking and in-bed wear time in hip-worn accelerometer data collected with a 24 h wear protocol in young adults. Physiol. Meas. 2016, 37, 1636–1652. [Google Scholar] [CrossRef]
- Matthew, C.E. Calibration of accelerometer output for adults. Med. Sci. Sports Exerc. 2005, 37, S512–S522. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Chastin, S.F.; Granat, M.H. Methods for objective measure, quantification and analysis of sedentary behaviour and inactivity. Gait Posture 2010, 31, 82–86. [Google Scholar] [CrossRef]
- Spruit, M.A.; Sillen, M.J.H.; Groenen, M.T.J.; Wouters, E.F.M.; Franssen, F.M.E. New normative values for handgrip strength: Results from the UK Biobank. J. Am. Med. Dir. Assoc. 2013, 14, 775.e5–775.e11. [Google Scholar] [CrossRef]
- Bade, B.C.; Hyer, J.M.; Bevill, B.T.; Pastis, A.; Rojewski, A.M.; Toll, B.A.; Silvestri, G.A. A patient-centered activity regimen improves participation in physical activity interventions in advanced-stage lung cancer. Integr. Cancer Ther. 2018, 17, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.; Ricci, C.; Leitzmann, M.F. Associations of objectively assessed physical activity and sedentary time with all-cause mortality in US adults: The NHANES study. PLoS ONE 2015, 10, e0119591. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Wang, Q.; Neilson, H.K.; Kopciuk, K.A.; McGregor, S.E.; Courneya, K.S. Physical activity and survival after prostate cancer. Eur. Urol. 2016, 70, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Kamiyama, Y.; Kasai, H.; Kodama, T. A phase II study of first-line chemotherapy with weekly carboplatin plus gemcitabine in advanced non-small cell lung cancer. Chemotherapy 2012, 58, 78–83. [Google Scholar] [CrossRef]
- Novello, S.; Falcone, A.; Crino, L.; Rinaldi, M.; Nardi, M.; De Marinis, F.; Tonato, M.; Tibaldi, C.; Tinazzi, A.; Russo, F.; et al. Randomised multicenter phase II study of two schedules of docetaxel and gemcitabine or cisplatin/gemcitabine followed by docetaxel as first line treatment for advanced non-small cell lung cancer. Lung Cancer 2009, 66, 327–332. [Google Scholar] [CrossRef]
- Granger, C.L.; McDonald, C.F.; Irving, L.; Clark, R.A.; Gough, K.; Murnane, A.; Mileshkin, L.; Krishnasamy, M.; Denehy, L. Low physical activity levels and functional decline in individuals with lung cancer. Lung Cancer 2014, 83, 292–299. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | All Participants (n = 89) | Survivors (n = 62) | Deceased (n = 27) | a MD [95% CI] or p Value |
|---|---|---|---|---|
| Participants characteristics | ||||
| Age, yr | 70 ± 10 | 69 ± 11 | 73 ± 9 | 3.4 [−8.3–1.2] |
| Sex, female (%) | 34 (38%) | 26 (42%) | 8 (30%) | p = 0.34 |
| BMI, kg/m2 | 25.1 [22.0–30.6] | 25.5 [22.2–30.8] | 24.8 [21.9–29.5] | p = 0.67 |
| Smoking status, n (%) | ||||
| Current; ex; never | 22 (24%); 58 (65%); 9 (10%) | 16 (26%); 41 (66%); 5 (8%) | 6 (22%); 17 (63%); 4 (15%) | p = 0.61 |
| Type of cancer, n (%) | ||||
| NSCLC; SCLC; Poorly diff CA | 83 (93%); 5 (6%); 1 (1%) | 58 (94%); 3 (5%); 1 (1%) | 25 (93%); 2 (7%); 0 (0%) | p = 0.63 |
| Lung cancer stage, n (%) | ||||
| Early/Limited | 33 (37%) | 27 (43%) | 6 (22%) | p = 0.05 |
| Advanced/Extensive | 56 (63%) | 35 (57%) | 21 (78%) | |
| Treatment intent | ||||
| Radical; Palliative | 47 (53%); 42 (47%) | 35 (57%); 27 (44%) | 12 (44%); 25 (56%) | p = 0.36 |
| ECOG status, n (%) | ||||
| 0–1; 2 | 74 (83%); 15 (17%) | 52 (84%); 10 (16%) | 22 (81%); 5 (19%) | p = 0.35 |
| Handgrip force (%pred) | 97 ± 24 | 99 ± 24 | 93 ± 25 | 6.8 [−4.8–18.4] |
| Blood cell count | ||||
| Platelets (×109/L) | 308 ± 134 | 315 ± 126 | 293 ± 151 | 22 [−40–83] |
| Neutrophils (×109/L) | 6.6 ± 3.8 | 6.0 ± 2.4 | 8.0 ± 5.7 | −1.9 [−3.7–−0.2] |
| Lymphocytes (×109/L) | 1.92 ± 1.37 | 2.05 ± 1.54 | 1.62 ± 0.83 | 0.4 [−0.2–1.1] |
| Neutrophil-to-lymphocyte ratio | 3.3 [2.4–5.6] | 3.1 [2.3–4.6] | 4.3 [2.5–7.0] | p = 0.03 |
| Physical activity level | ||||
| Number of valid days | 7 [6–7] | 7 [7–7] | 7 [6–7] | p = 0.09 |
| Waking wear time, min/day | 887 ± 97 | 896 ± 98 | 866 ± 91 | 29 [−14–74] |
| Time spent in LIPA, min/day | 246 ± 87 | 259 ± 86 | 218 ± 83 | 40 [1–80] |
| Time spent in MVPA, min/day | 4.6 [1–15] | 7.0 [1–20] | 2.2 [0.4–5.3] | p = 0.01 |
| Daily step count, steps/day | 7848 ± 3737 | 8420 ± 3834 | 6534 ± 3195 | 1885 [210–3560] |
| Time spent sedentary, min/day | 629 ± 112 | 623 ± 105 | 641 ± 127 | −18 [−69–33] |
| UBD, min | 18 [14–24] | 16 [13–22] | 22 [16–25] | p = 0.04 |
| Variable | Hazard Ratio (95% CI) |
|---|---|
| Age, yr | 1.03 [0.99–1.07] |
| Lung cancer stage, early/limited | 0.42 [0.17–1.05] |
| Neutrophil-to-lymphocyte ratio | 1.04 [1.01–1.07] |
| Time spent in LIPA, min/day (10-min increments) | 0.94 [0.90–0.99] |
| Time spent in LIPA, (>242 min/day) | 0.57 [0.26–1.23] |
| Time spent in MVPA, min/day | 0.96 [0.93–0.99] |
| Time spent in MVPA, (>4.6 min/day) | 0.41 [0.19–0.93] |
| Daily step count, steps/day (500 step increments) | 0.93 [0.88–0.99] |
| Daily step count, (>7669 steps/day) | 0.58 [0.27–1.25] |
| Time spent sedentary, hr/day | 1.11 [0.90–1.36] |
| Time spent sedentary, (≥630 min/day) | 1.41 [0.66–3.02] |
| UBD, min | 1.04 [1.01–1.07] |
| UBD, (≥18 min) | 2.06 [0.93–4.60] |
| Variable | Hazard Ratio (95% CI) |
|---|---|
| Time spent in LIPA, min/day (10-min increments) | 0.95 [0.89–1.03] |
| Time spent in MVPA, (>4.6 min/day) | 0.40 [0.16–0.96] |
| Daily step count, steps/day (500 step increments) | 0.93 [0.85–1.01] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalheri, V.; Grigoletto, I.; McVeigh, J.; Manners, D.; Boyle, T.; Peddle-McIntyre, C.J.; Thomas, R.; Leong, J.; Bowyer, S.; Mooney, K.; et al. Association between Physical Activity and Reduced Mortality in Inoperable Lung Cancer. J. Clin. Med. 2023, 12, 7346. https://doi.org/10.3390/jcm12237346
Cavalheri V, Grigoletto I, McVeigh J, Manners D, Boyle T, Peddle-McIntyre CJ, Thomas R, Leong J, Bowyer S, Mooney K, et al. Association between Physical Activity and Reduced Mortality in Inoperable Lung Cancer. Journal of Clinical Medicine. 2023; 12(23):7346. https://doi.org/10.3390/jcm12237346
Chicago/Turabian StyleCavalheri, Vinicius, Isis Grigoletto, Joanne McVeigh, David Manners, Terry Boyle, Carolyn J. Peddle-McIntyre, Rajesh Thomas, Jeanie Leong, Samantha Bowyer, Kirsten Mooney, and et al. 2023. "Association between Physical Activity and Reduced Mortality in Inoperable Lung Cancer" Journal of Clinical Medicine 12, no. 23: 7346. https://doi.org/10.3390/jcm12237346
APA StyleCavalheri, V., Grigoletto, I., McVeigh, J., Manners, D., Boyle, T., Peddle-McIntyre, C. J., Thomas, R., Leong, J., Bowyer, S., Mooney, K., Straker, L., & Galvão, D. A. (2023). Association between Physical Activity and Reduced Mortality in Inoperable Lung Cancer. Journal of Clinical Medicine, 12(23), 7346. https://doi.org/10.3390/jcm12237346