


Physical Exercise and Dietary Supplementation in Middle-Aged and Older Women: A Systematic Review

 ,
, 
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Eligibility Criteria
- Inclusion Criteria
- -
- Randomised and non-randomised clinical trials.
- -
- Meta-analysis.
- -
- Studies carried out in adult menopausal women, according to the guidelines of the W.H.O., who are not on hormone replacement therapy; healthy or with menopausal complications: osteoporosis, dyslipidaemia, hypertension, obesity, etc.
- -
- Articles published less than 5 years ago, regardless of language.
- Exclusion Criteria
- Reviews, both systematic reviews and review articles. We did not exclude articles that were systematic reviews with meta-analysis. Studies conducted in patients with other serious diseases that could affect the results (e.g., cancer).
- Studies in which menopause and exercise or dietary supplements did not appear as keywords in the abstract or title; or in which both interventions did not occur in the study population.
- Studies of low methodological quality: PEDro scale score less than 4 points or low AMSTAR-2 scale score.
2.3. Search Strategy and Information Sources
- -
- (menopause) OR (natural language) AND (“dietary supplements”) OR (natural language).
- -
- (menopause) OR (natural language) AND (exercise) OR (natural language).
2.4. Selection Process of the Studies
2.5. Data Extraction Process
2.6. Methodological Quality Control Tools
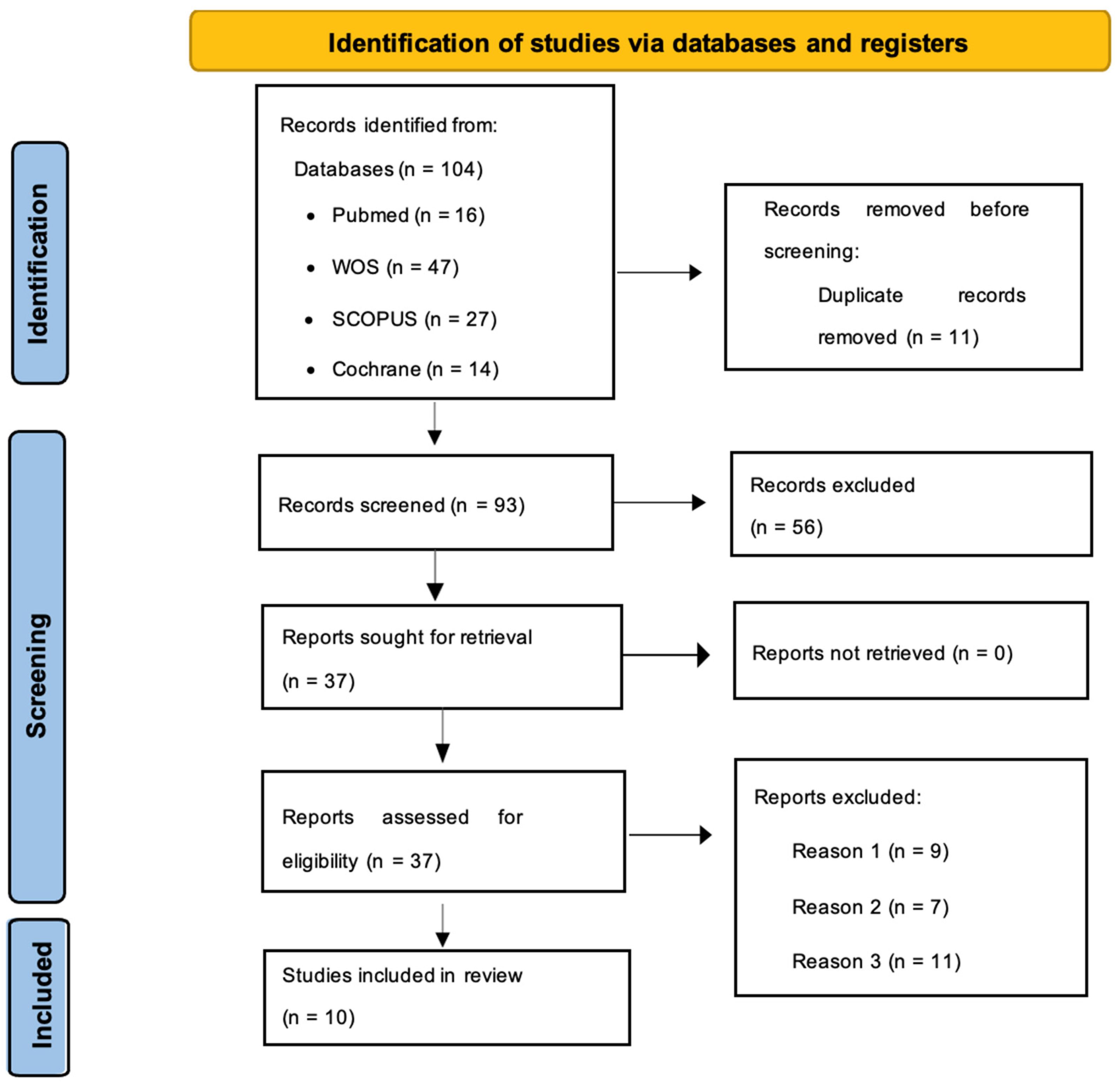
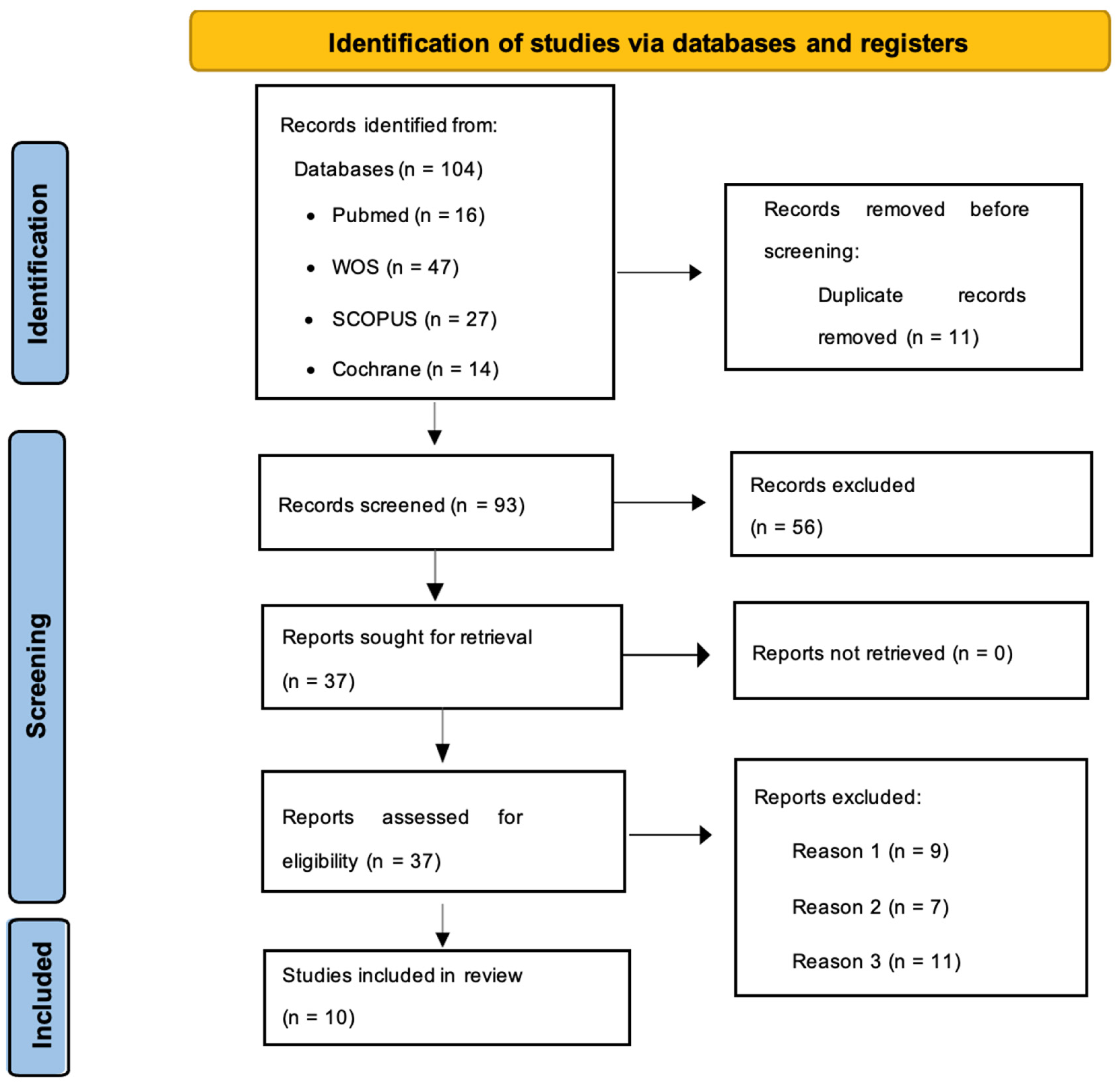
3. Results
- -
- Scientific evidence no older than 5 years. Meta-analysis or clinical trials.
- -
- The study sample is healthy middle-aged women or women with middle-aged pathologies (due to or common during menopause) such as osteoporosis, dyslipidaemia, hypertension, and sarcopenia, among others.
- -
- They provide evidence for the benefits of a specific exercise program, a dietary supplement, or a combination of both.
- -
- Author, country, and year.
- -
- Type and duration of the study.
- -
- Sample and main characteristics of the sample.
- -
- Aims of the study.
- -
- Main findings.
- -
- Conclusions.
4. Discussion
5. Conclusions
- -
- Both strength and aerobic training, as well as supplementation with calcium and vitamin D, increase bone mineral density.
- -
- Combined strength and resistance training provide cardiovascular benefits, increase strength and muscle mass, and reduce the risk of sarcopenia.
- -
- Physical exercise has a synergistic effect with some supplements, enhancing their effectiveness.
- -
- Moderate physical activity enhances the effects of calcium on the skeleton, further reducing bone loss.
- -
- Supplements such as whey protein or Zataria multiflora appear to be ineffective without an appropriate exercise regimen.
- -
- Other supplements such as calcium, isoflavones, or omega-3 can enhance their effects when combined with a workout routine.
- -
- Calcium and vitamin D are effective supplements against bone demineralization, especially when consumed in enriched dairy products.
- -
- Recommended exercises include 2 days of strength training and 2 days of aerobic resistance training per week.
- -
- Bodyweight exercises such as yoga or tai chi are also beneficial for improving balance and flexibility.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. 2022. Available online: https://www.who.int/es/news-room/fact-sheets/detail/menopause (accessed on 21 May 2023).
- Ghanbari-Niaki, A.; Saeidi, A.; Gharahcholo, L.; Moradi-Dehbaghi, K.; Zare-Kookandeh, N.; Ahmadian, M.; Zouhal, H.; Hackney, A.C. Influence of resistance training and herbal supplementation on plasma apelin and metabolic syndrome risk factors in postmenopausal women. Sci. Sports 2020, 35, 109.e1–109.e5. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, N.; Juliá, M.D.; Galliano, D.; Coronado, P.; Díaz, B.; Fontes, J.; Gallo, J.L.; García, A.; Guinot, M.; Munnamy, M.; et al. Consenso español sobre menopausia prematura. Maturitas 2015, 80, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Menopausia: MedlinePlus en Español. Available online: https://medlineplus.gov/spanish/menopause.html (accessed on 7 August 2023).
- Vitale, S.G.; Caruso, S.; Rapisarda AM, C.; Cianci, S.; Cianci, A. Isoflavones, calcium, Vitamin D and inulin improve quality of life, sexual function, body composition and metabolic parameters in menopausal women: Result from a prospective, randomized, placebo-controlled, parallel-group study. Prz. Menopauzalny 2018, 17, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, N.; De Teresa, C.; Cano, A.; Godoy, D.; Hita-Contreras, F.; Lapotka, M.; Llaneza, P.; Manonelles, P.; Martínez-Amat, A.; Ocón, O.; et al. Benefits of physical exercise in postmenopausal women. Maturitas 2016, 93, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Rostami-Moez, M.; Masoumi, S.Z.; Otogara, M.; Farahani, F.; Alimohammadi, S.; Oshvandi, K. Examining the Health-Related Needs of Females during Menopause: A Systematic Review Study. J. Menopausal Med. 2023, 29, 1. [Google Scholar] [CrossRef] [PubMed]
- Santoro, N.; Sutton-Tyrrell, K. The SWAN Song: Study of Women’s Health Across the Nation’s Recurring Themes. Obstet. Gynecol. Clin. N. Am. 2011, 38, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Bansal, R.; Aggarwal, N. Menopausal hot flashes: A concise review. J. Mid-Life Health 2019, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Management of menopausal symptoms. Obstet. Gynecol. 2014, 23, 202–216. [Google Scholar] [CrossRef]
- NAMS. The 2017 hormone therapy position statement of the North American Menopause Society. Menopause 2017, 24, 728–753. [Google Scholar] [CrossRef]
- Zaheer, S.; LeBoff, M.; Lewiecki, E.M. Denosumab for the treatment of osteoporosis. Expert Opin. Drug Metab. Toxicol. 2015, 11, 461–470. [Google Scholar] [CrossRef]
- Hettchen, M.; Kohl, M.; Murphy, M.H.; Shojaa, M.; Ghasemikaram, M.; Bragonzoni, L.; Benvenuti, F.; Ripamonti, C.; Benedetti, M.G.; Julin, M.; et al. Changes in Menopausal Risk Factors in Early Postmenopausal Osteopenic Women after 13 Months of High-Intensity Exercise: The Randomized Controlled ACTLIFE-RCT. Dovepress 2021, 16, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Dupuit, M.; Maillard, F.; Pereira, B.; Marquezi, M.L.; Lancha, A.H., Jr.; Boisseau, N. Effect of high intensity interval training on body composition in women before and after menopause: A meta-analysis. Exp. Physiol. 2020, 105, 1470–1490. [Google Scholar] [CrossRef] [PubMed]
- Slater, G.; Phillips, S.M. Nutrition guidelines for strength sports: Sprinting, weightlifting, throwing events, and bodybuilding. J. Sports Sci. 2011, 29, S67–S77. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.L.; Holland, D.J.; Spathis, J.G.; Beetham, K.S.; Wisløff, U.; Keating, S.E.; Coombes, J.S. Guidelines for the delivery and monitoring of high intensity interval training in clinical populations. Prog. Cardiovasc. Dis. 2019, 62, 140–146. [Google Scholar] [CrossRef] [PubMed]
- de Antuñano, N.P.G.; Marqueta, P.M.; Redondo, R.B.; Fernández, C.C.; Bonafonte, L.F.; Aurrekoetxea, T.G.; González, B.M.; de Teresa Galván, C.; del Valle Soto, M.; Grupo de Trabajo sobre Nutrición en el Deporte de la Federación Española; et al. Suplementos nutricionales para el deportista. Ayudas ergogénicas en el deporte—2019. Documento de consenso de la Sociedad Española de Medicina del Deporte. Arch. Med. Deporte 2019, 36 (Suppl. S1), 7–83. [Google Scholar]
- Liu, C.; Kuang, X.; Li, K.; Guo, X.; Deng, Q.; Li, D. Effects of combined calcium and vitamin D supplementation on osteoporosis in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Food Funct. 2020, 11, 10817–10827. [Google Scholar] [CrossRef] [PubMed]
- Soler Salazar, A.; Cardona García, A.M. Suplementos nutricionales en la industria del fitness. Rev. Nutr. Clínica Metab. 2019, 2, 60–66. [Google Scholar] [CrossRef]
- Villanova Colmenero, M.; Martínez-Sanz, J.M.; Norte Navarro, A.; Ortíz-Moncada, R.; Hurtado, J.A.; Baladia, E. Variables utilizadas en cuestionarios de consumo de suplementos ergonutricionales. Nutr. Hosp. 2015, 32, 556–572. [Google Scholar]
- Lu, C.; Lu, T.; Ge, L.; Yang, N.; Yan, P.; Yang, K. Use of AMSTAR-2 in the methodological assessment of systematic reviews: Protocol for a methodological study. Ann. Transl. Med. 2020, 8, 652. [Google Scholar] [CrossRef]
- Sherrington, C.; Herbert, R.D.; Maher, C.G.; Moseley, A.M. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man. Ther. 2000, 5, 223–226. [Google Scholar] [CrossRef]
- García-Gomáriz, C.; Blasco, J.M.; Macián-Romero, C.; Guillem-Hernández, E.; Igual-Camacho, C. Effect of 2 years of endurance and high-impact training on preventing osteoporosis in postmenopausal women: Randomized clinical trial. Menopause 2018, 25, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Giolo, J.S.; Costa, J.G.; Da Cunha-Junior, J.P.; Pajuaba, A.C.A.M.; Taketomi, E.A.; De Souza, A.V.; Caixeta, D.C.; Peixoto, L.G.; De Oliveira, E.P.; Everman, S.; et al. The Effects of Isoflavone Supplementation Plus Combined Exercise on Lipid Levels, and Inflammatory and Oxidative Stress Markers in Postmenopausal Women. Nutrients 2018, 10, 424. [Google Scholar] [CrossRef] [PubMed]
- Félix-Soriano, E.; Martínez-Gayo, A.; Cobo, M.J.; Pérez-Chávez, A.; Ibáñez-Santos, J.; Palacios Samper, N.; Goikoetxea Galarza, I.; Cuervo, M.; García-Unciti, M.; González-Muniesa, P.; et al. Effects of DHA-Rich n-3 Fatty Acid Supplementation and/or Resistance Training on Body Composition and Cardiometabolic Biomarkers in Overweight and Obese Post-Menopausal Women. Nutrients 2021, 12, 2465. [Google Scholar] [CrossRef]
- Hayashi, K.; Yamaguchi, H.; Amaoka, H.; Takahara, T.; Kunisa, S.; Tamai, N.; Maejima, N.; Watanabe, N.; Kobayashi, Y.; Tanaka, H. Equol-producing status affects exercise training-induced improvement in arterial compliance in postmenopausal women. J. Appl. Physiol. 2021, 130, 827–835. [Google Scholar] [CrossRef]
- Kemmler, W.; Shojaa, M.; Kohl, M.; von Stengel, S. Effects of Different Types of Exercise on Bone Mineral Density in Postmenopausal Women: A Systematic Review and Meta-analysis. Calcif. Tissue Int. 2020, 107, 409–439. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.Y.; Chang, H.Y.; Huang, Y.C.; Liu, C.W. Effect of Whey Protein Supplementation in Postmenopausal Women: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4210. [Google Scholar] [CrossRef]
- Nakamura, K.; Saito, T.; Kobayashi, R.; Oshiki, R.; Kitamura, K.; Watanabe, Y. Physical activity modifies the effect of calcium supplements on bone loss in perimenopausal and postmenopausal women: Subgroup analysis of a randomized controlled trial. Arch. Osteoporos. 2019, 14, 1–5. [Google Scholar] [CrossRef]
- ElDeeb, A.M.; Abdel-Aziem, A.A. Effect of Whole-Body Vibration Exercise on Power Profile and Bone Mineral Density in Postmenopausal Women with Osteoporosis: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2020, 43, 384–393. [Google Scholar] [CrossRef]
- Xi, H.; He, Y.; Niu, Y.; Sui, X.; Zhang, J.; Zhu, R.; Xu, H.; Zhang, S.; Li, Y.; Yuan, Y.; et al. Effect of combined aerobic and resistance exercise on blood pressure in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Exp. Gerontol. 2021, 155, 111560. [Google Scholar] [CrossRef]
- Morato-Martínez, M.; López-Plaza, B.; Santurino, C.; Palma-Milla, S.; Gómez-Candela, C. A dairy product to reconstitute enriched with bioactive nutrients stops bone loss in high-risk menopausal women without pharmacological treatment. Nutrients 2020, 12, 2203. [Google Scholar] [CrossRef]
- Kopiczko, A. Determinants of bone health in adults Polish women: The influence of physical activity, nutrition, sun exposure and biological factors. PLoS ONE 2020, 15, e0238127. [Google Scholar] [CrossRef] [PubMed]
- Dechichi, J.G.C.; Mariano, I.M.; Giolo, J.S.; Batista, J.P.; Amaral, A.L.; Ribeiro, P.A.B.; de Oliveira, E.P.; Puga, G.M. Isoflavone supplementation does not potentiate the effect of combined exercise training on resting and ambulatory blood pressure in non-obese postmenopausal women: A randomized double-blind controlled trial-a pilot study. Nutrients 2020, 12, 3495. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors, Year. Country | Type of Study and Duration | Sample and Characteristics | Characteristics of the Study | Objective of the Study | Main Findings | Conclusions |
|---|---|---|---|---|---|---|
| García-Gomáriz et al., 2018 [23]. Spain | Randomised clinical trial, 2 years. | n = 34 (IG = 17; CG = 17) Healthy menopausal women over 50 years of age supplemented with Ca (1000 mg/day) and Vit. D (880 IU) | IG; high-intensity strength training (2 sessions per week) + supplementation with Ca and Vit. D CG; brisk walking (3–5 times a week) + Ca and Vit. D supplementation | To analyse the differences in bone density level between a high-intensity strength exercise programme recommended by the AEEM and brisk walking to prevent osteoporosis in menopausal women. Both groups were supplemented with Ca and vitamin D. | The CG showed an increase in T-Score at the lumbar spine (+0.27), while the strength training group increased T-Score at both the lumbar spine (+0.47) and femoral neck (+0.28). | Although both training plans are effective in reducing the risk of osteoporosis in addition to Ca and vitamin D supplementation, strength training proved to be more effective in preventing osteoporosis at both the lumbar and femoral levels. |
| Giolo et al., 2018 [24]. Brazil | Randomised clinical trial, 10 weeks. | n = 32 (IG = 16; CG = 16) Healthy menopausal women aged 50–70 years undergoing a strength and endurance exercise routine 3 times a week. | IG; supplementation with 100 mg isoflavones per day + strength and endurance training. CG; placebo + strength and endurance training. | To assess the effect of isoflavone supplementation and a strength and endurance exercise routine on blood cholesterol levels, inflammatory markers, and oxidative stress. | There were no significant differences between the two groups. Oxidative stress markers and inflammatory markers were very similar at baseline and at the end of the study, except for cholesterol and interleukin-8 levels. Cholesterol levels in the placebo group decreased and interleukin-8 levels increased. | Isoflavone supplementation shows no benefit in terms of reducing cholesterol levels, inflammatory markers, or oxidative stress. However, physical exercise appears to be effective in reducing cholesterol levels; although it may increase some inflammatory markers such as interleukin-8. |
| Félix-Soriano et al., 2021 [25]. Spain | Randomised clinical trial, 16 weeks. | n = 124 (IG1 = 31; IG2 = 31; CG1 = 31; CG2 = 31) Overweight menopausal women aged 55–70 years supplemented with DHA-rich Omega-3 or placebo. | IG1; Omega 3 (1950 mg/day). IG2; Omega 3 (1950 mg/day) + strength training (2 times per week). CG1; Placebo. CG2; Placebo + strength training (2 times per week). | To study the benefits of DHA-rich Omega-3 supplementation and strength training in overweight menopausal women. | A reduction in body fat percentage was observed in addition to an increase in bone mineral content, muscle mass, strength, and glucose tolerance. For Omega-3 supplementation, a decrease in BP, triglyceride levels, and an increase in muscle mass were observed. | Both DHA-rich omega-3 supplementation and strength exercise show a number of cardiovascular, bone, and muscle benefits in combating menopausal complications. |
| Hayashi et al., 2021 [26]. Japan | Randomised clinical trial, 8 weeks. | n = 43 (IG = 27; CG = 16) Healthy menopausal women aged 45–69 years supplemented with soy isoflavones. | IG: supplementation with isoflavones (25 mg/day) + aerobic training (2–3 days per week). CG: supplementation with isoflavones (25 mg/day). | To determine whether the production of equol (a metabolite of isoflavones with oestrogen-like behaviour) by the gut microbiota exerts a synergistic effect with physical exercise in increasing arterial distensibility in menopausal women. | The increase in arterial compliance in the IG group was significantly higher (0.117 ± 0.035 mm2/mmHg) compared to the CG. The IG microbiota produced equol naturally with isoflavone supplementation and exercise. | Regular aerobic exercise exerts a synergistic effect with isoflavone intake, producing more equol and thus further increasing arterial compliance compared to isoflavone supplementation alone. The combination of both interventions may help to reduce cardiovascular problems such as hypertension. |
| Kemmler et al., 2020 [27]. Germany | Metaanalysis of studies. ≥6 months. | n = 5112 (IG = 2793; CG = 2319) Healthy menopausal women or women with osteoporosis aged 51–80 years on daily Ca and/or vitamin D supplementation. | IG; women who exercise and supplement with Ca and/or Vit. D. CG; non-exercising women who supplement with Ca and/or Vit. D. | To study the effect of different types of exercise: aerobic or anaerobic exercises with BW, DS exercises with machines, or a combination of both (BW + DS); on BMD of the femoral neck, lumbar spine, or hip in menopausal women. The training plan had to last more than 6 months and was compared with a sedentary group. | The 3 exercise programmes increased BMD in the hip, femur, and spine in different ways. Each programme increased BMD to a greater or lesser extent depending on the bone region measured. Physical exercise produces more improvements in BMD if it is practiced during early menopause, the older the age, the less benefit. | Physical exercise increases BMD significantly, but we cannot be sure that there is one particular exercise programme that increases BMD more than another. |
| Kuo et al., 2022 [28]. Taiwan | Metaanalysis of studies. 12–72 weeks. | n = 776 Healthy menopausal or sarcopenic women over 55 years of age on whey protein supplementation and with a sedentary lifestyle or leading a strength training routine. | IG: menopausal women supplemented with WP, 20–30 g per day + strength training for 12–72 weeks. CG: menopausal women supplemented with WP, 20–30 g per day. | To investigate the changes in strength and body composition that WP can produce in menopausal women, in combination with a strength routine or a sedentary lifestyle. | WP supplementation (20–40 g per day) had significant effects in the upper and lower body strength training groups, contributing to the increase in biceps curl strength, with a SMD: 0.6805, 95% CI, and increasing muscle mass in the lower limbs: SMD: 1.103, 95% CI. | WP is effective in combating sarcopenia and increasing strength in menopausal women if accompanied by a strength exercise programme. Taking it on its own has no significant effect on strength or improved body composition. |
| Nakamura et al., 2019 [29]. Japan | Randomised clinical trial, 2 years | n = 450 (IG1 = 150; IG2 = 150; CG = 150) Healthy menopausal women aged 50–75 years who engage in moderate (4 METs) or vigorous (6 METs) physical activity. | IG1; supplementation with 250 mg per day of Ca. IG2; supplementation with 500 mg per day of Ca. CG; placebo | To investigate whether a plan of vigorous (6 METs) or moderate (4 METs) physical activity can modify the effect of Ca supplementation on bone metabolism, with 250 mg, 500 mg, or placebo supplementation. | In the moderate physical activity group, namely 4 METs per week, spinal BMD decreased significantly less in the group consuming 500 mg Ca per day (−0.029 g/cm2, p = 0.042) compared to the placebo group (−0.045 g/cm2). In the vigorous physical activity group, there were no significant differences between supplementation and placebo groups. | Moderate physical activity modifies the effect of calcium supplementation on BMD in menopausal women, increasing its effect on bone metabolism. |
| Ghanbari-Niaki et al., 2020 [2]. Iran | Randomised clinical trial, 8 weeks. | n = 96 (IG = 48; CG = 48) Healthy menopausal women over 53 years of age. | IG; subdivided into 4 groups of n = 12 according to the level of training (from 0 to 85% intensity). All of them supplemented with 500 mg of ZM per day. CG; subdivided into 4 groups of n = 12 according to the level of training (from 0 to 85% intensity). None of them supplemented with ZM. | To assess the effects of strength training in menopausal women in addition to supplementation with 500 mg of ZM. | Strength training increases insulin sensitivity and plasma apelin levels (a peptide that produces cardiovascular benefits). ZM lowers blood glucose levels, so it could be synergistic with strength training. | Strength training decreases risk factors for metabolic syndrome and ZM may be helpful in lowering blood glucose levels when combined with strength training. The combination of both interventions produces cardiovascular benefits. |
| Hettchen et al., 2021 [13]. Germany | Randomised clinical trial, 18 months. | n = 54 (IG = 27; CG = 27) Menopausal women with osteoporosis aged 48–60 years supplemented with Ca (1000 mg/day) and Vit. D (800 IU/day). | IG; Ca and Vit. D supplementation + strength training with high-intensity weights 3 or 2 times a week. CG; Ca and Vit. D supplementation + strength training with low-intensity weights once a week. | To investigate the changes produced by strength training with weights together with Ca (1000 mg/day) and Vit. D (800 IU) supplementation in menopausal women. | The IG showed several improvements compared to the CG: a significant increase in BMD at the spine level (0.002 ± 0.018 mg/cm2), increased lean mass (0.39 ± 1.08 kg) and strength, decreased body fat (−1.44 ± 1.49 kg) and improved menopausal symptoms as measured by the MRS II (p = 0.002). | High-impact strength training is a good strategy to combat various negative effects of menopause. |
| ElDeeb y Abdel-Aziem. 2020 [30]. Egypt | Randomised clinical trial, 24 weeks. | n = 44 (IG = 22; CG = 22) Menopausal women aged 50–60 years with low BMD and supplemented with Ca (1200 mg/day) and Vit. D (800 IU/day). | IG; using vibration platforms 2 times a week + supplementation with Ca and Vit. D CG; no use of vibration platforms + supplementation with Ca and Vit. D | To study the effect of vibration platform training on muscle work and BMD in menopausal women consuming 1200 mg Ca per day and 800 IU Vit D per day. | The IG showed a greater increase in BMD at the lumbar and femoral levels than the CG (p > 0.05). It also showed increased strength in the muscle groups involved in gait, which was not reflected in the CG. | Vibration platform therapy increases hip, knee, and ankle strength and increases BMD in the lumbar spine and femur in menopausal women. |
| Authors | Criteria | Total | Methodological Quality Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Nakamura et al. [29] | + | - | + | - | - | - | + | + | + | + | 6 | Good |
| García-Gomáriz et al. [23] | + | + | - | + | - | - | - | + | - | + | 5 | Regular |
| Félix-Soriano et al. [25] | + | - | + | - | - | - | - | - | + | + | 4 | Regular |
| Hettchen et al. [13] | + | + | + | - | - | + | + | + | + | + | 9 | Excellent |
| Ghanbari-Niaki et al. [2] | + | - | + | - | - | - | + | + | + | + | 7 | Good |
| ElDeeb y Abdel-Aziem. [30] | + | + | + | - | - | - | + | - | + | + | 6 | Good |
| Giolo et al. [24] | + | + | + | - | - | - | + | + | + | + | 7 | Good |
| Hayashi et al. [26] | + | - | + | - | - | - | + | + | + | + | 6 | Good |
| Authors | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | General Confidence Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kemmler et al. [27] | + | + | - | + partial | + | + | + | + partial | + | + | + | - | + | + | + | + | Medium |
| Kuo et al. [28] | - | + | - | + partial | + | + | + | + partial | + partial | - | + partial | - | + | + | + | + | Medium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-García, J.C.; López Hernández, D.; Piqueras-Sola, B.; Cortés-Martín, J.; Reinoso-Cobo, A.; Menor-Rodríguez, M.J.; Rodríguez-Blanque, R. Physical Exercise and Dietary Supplementation in Middle-Aged and Older Women: A Systematic Review. J. Clin. Med. 2023, 12, 7271. https://doi.org/10.3390/jcm12237271
Sánchez-García JC, López Hernández D, Piqueras-Sola B, Cortés-Martín J, Reinoso-Cobo A, Menor-Rodríguez MJ, Rodríguez-Blanque R. Physical Exercise and Dietary Supplementation in Middle-Aged and Older Women: A Systematic Review. Journal of Clinical Medicine. 2023; 12(23):7271. https://doi.org/10.3390/jcm12237271
Chicago/Turabian StyleSánchez-García, Juan Carlos, Daniel López Hernández, Beatriz Piqueras-Sola, Jonathan Cortés-Martín, Andrés Reinoso-Cobo, María José Menor-Rodríguez, and Raquel Rodríguez-Blanque. 2023. "Physical Exercise and Dietary Supplementation in Middle-Aged and Older Women: A Systematic Review" Journal of Clinical Medicine 12, no. 23: 7271. https://doi.org/10.3390/jcm12237271
APA StyleSánchez-García, J. C., López Hernández, D., Piqueras-Sola, B., Cortés-Martín, J., Reinoso-Cobo, A., Menor-Rodríguez, M. J., & Rodríguez-Blanque, R. (2023). Physical Exercise and Dietary Supplementation in Middle-Aged and Older Women: A Systematic Review. Journal of Clinical Medicine, 12(23), 7271. https://doi.org/10.3390/jcm12237271