
The “Aging Effect” of BMI on Cardiorespiratory Fitness: A New Insight on Functional Evaluation in Obesity
 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. CPET Protocol
2.2. Statistical Analyses
3. Results
3.1. Population Characteristics
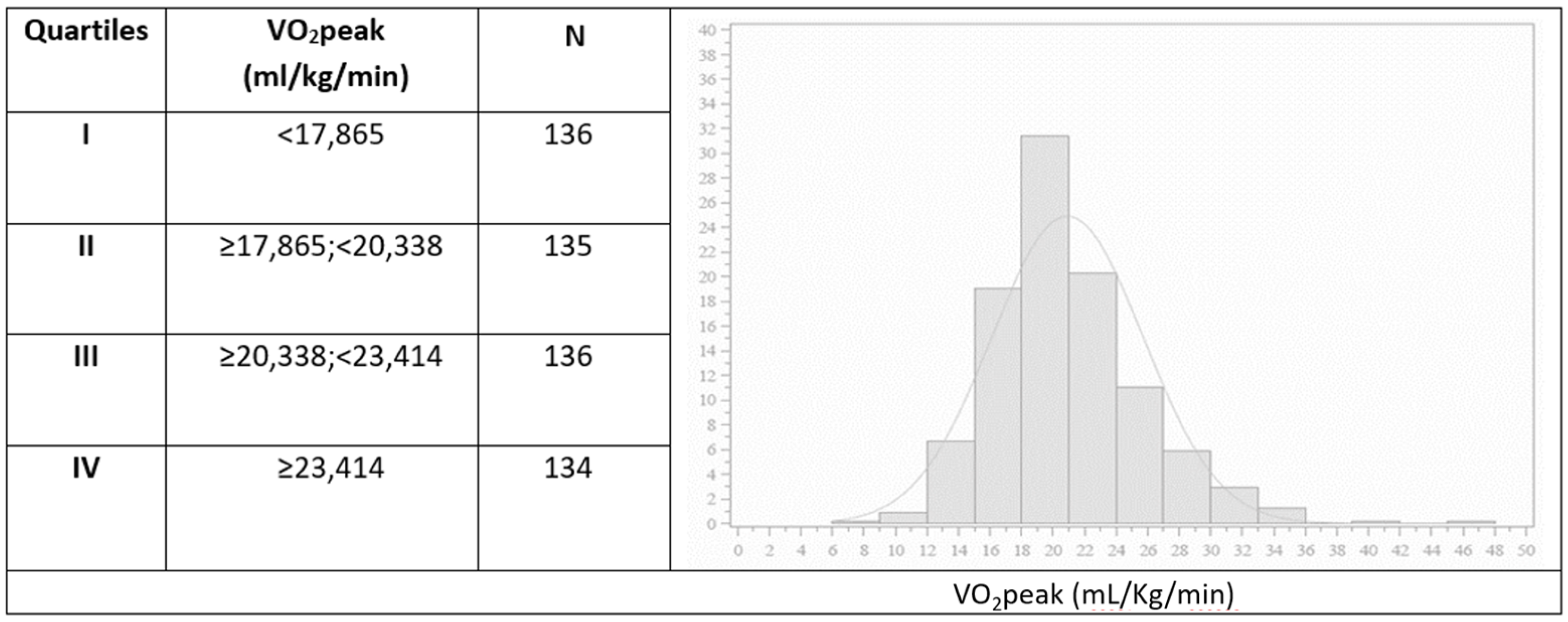
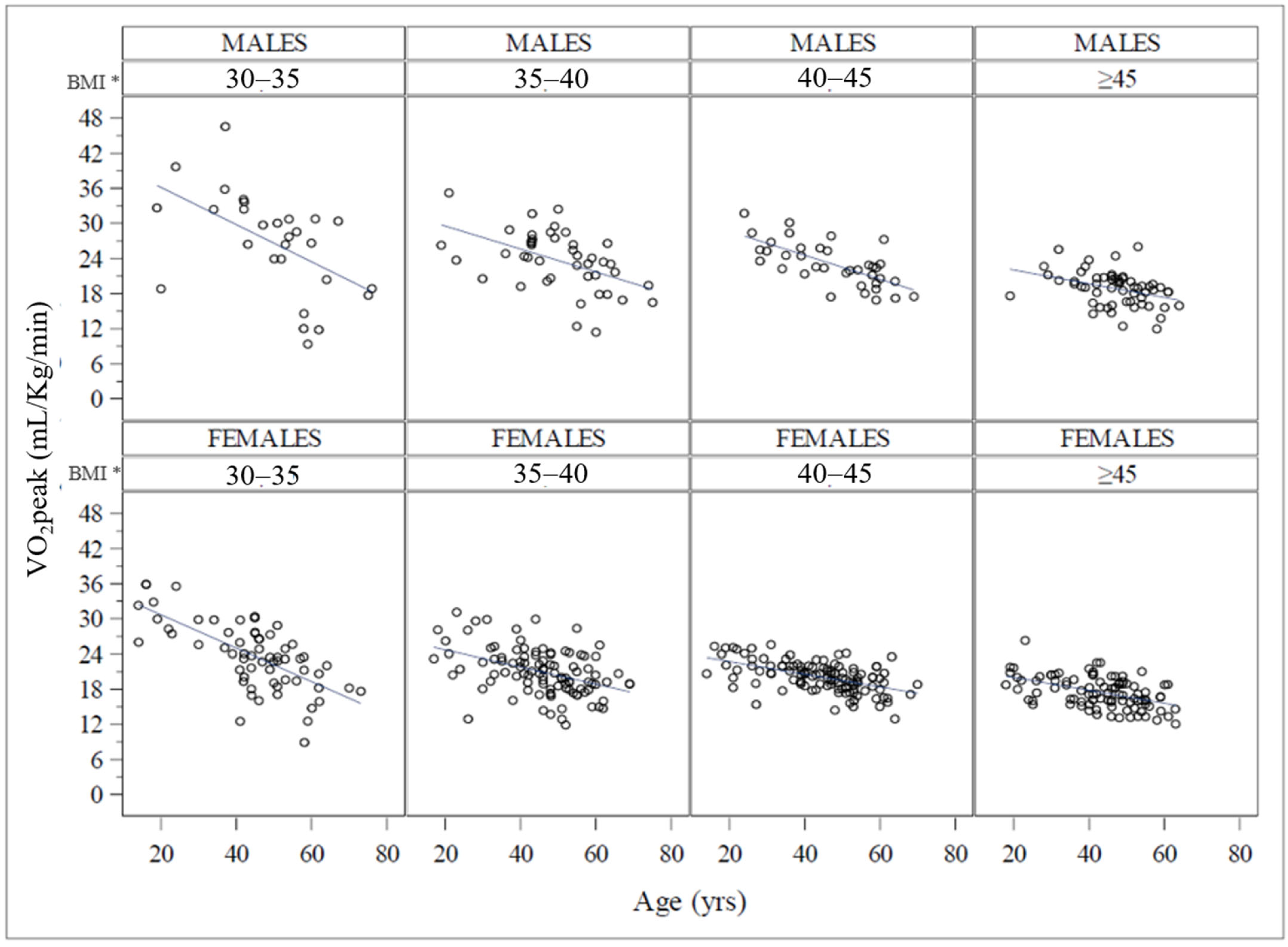
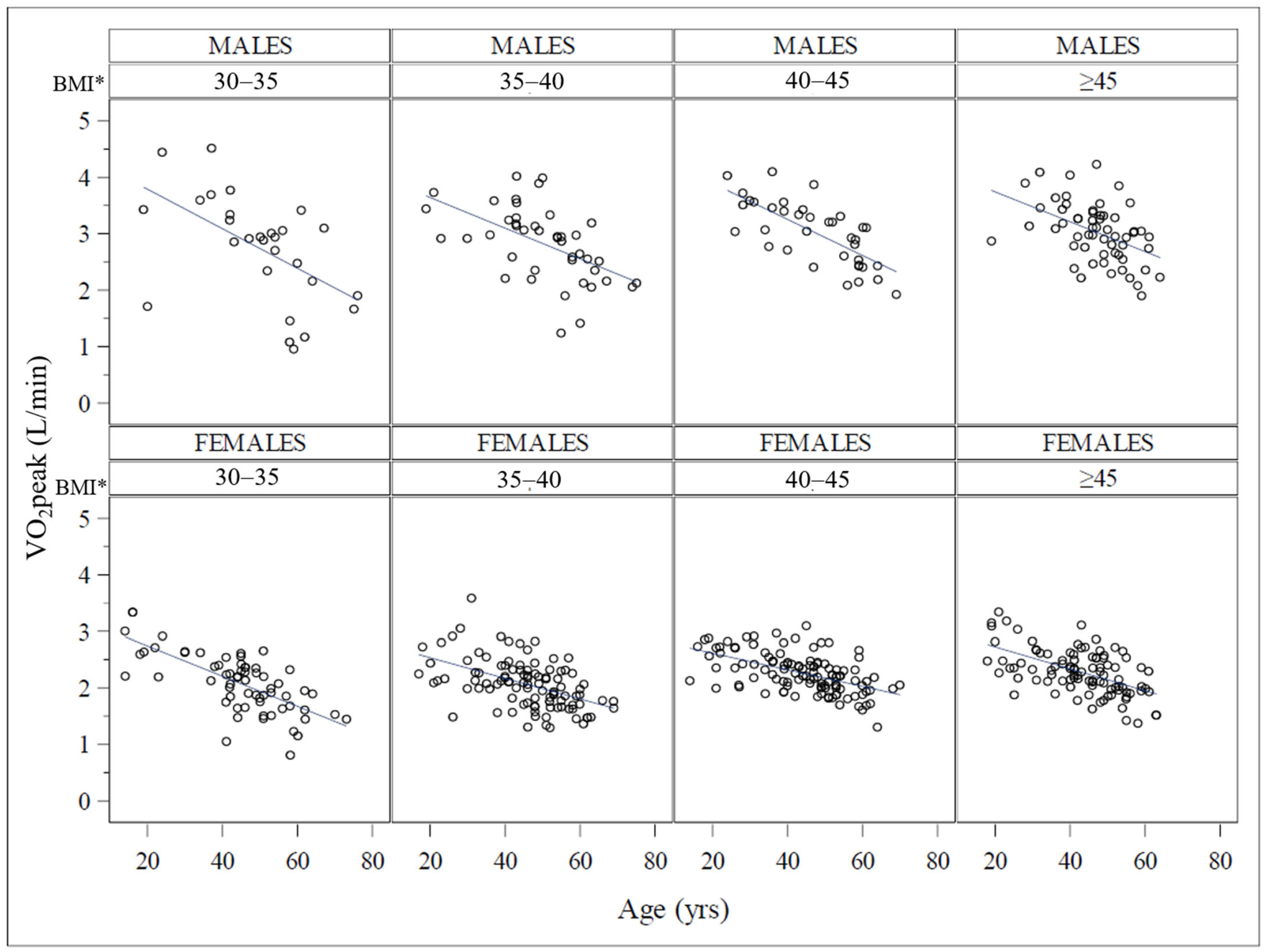
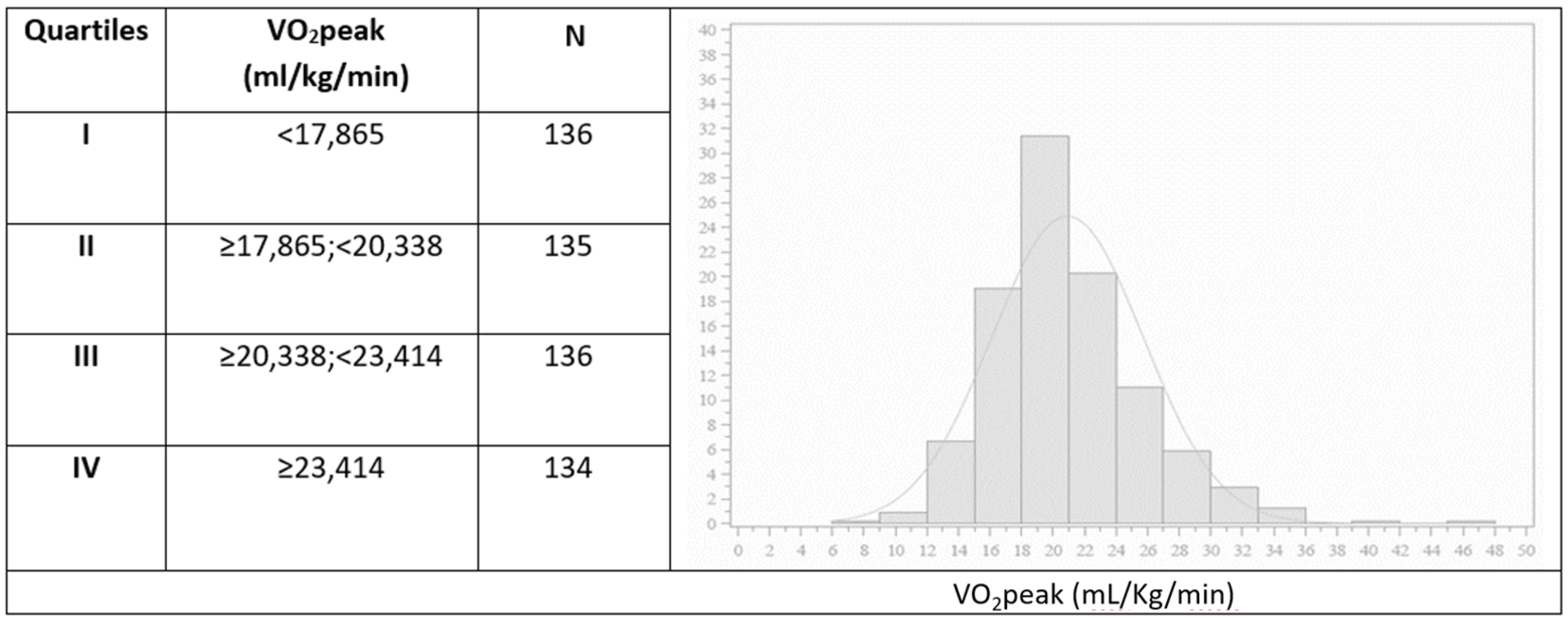
3.2. Functional Capacity: Distribution and Determinants
3.3. Cardiovascular and Cardiopulmonary Efficiency
4. Discussion
Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.J.; Balady, G.J.; Beasley, J.W.; Bricker, J.T.; Duvernoy, W.F.; Froelicher, V.F.; Mark, D.B.; Marwick, T.H.; McCallister, B.D.; Thompson, P.D., Jr.; et al. ACC/AHA Guidelines for Exercise Testing: A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on Exercise Testing). J. Am. Coll. Cardiol. 1997, 30, 260–311. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.C.; Artero, E.G.; Sui, X.; Blair, S.N. Mortality trends in the general population: The importance of cardiorespiratory fitness. J. Psychopharmacol. 2010, 24, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA 1989, 262, 2395–2401. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Kurl, S.; Salonen, R.; Rauramaa, R.; Salonen, J.T. The predictive value of cardiorespiratory fitness for cardiovascular events in men with various risk profiles: A prospective population-based cohort study. Eur. Heart J. 2004, 25, 1374–1375. [Google Scholar] [CrossRef]
- Fogelholm, M. Physical activity, fitness and fatness: Relations to mortality, morbidity and disease risk factors. A systematic review. Obes. Rev. 2010, 11, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Bettini, S.; Quinto, G.; Neunhaeuserer, D.; Battista, F.; Belligoli, A.; Milan, G.; Gasperetti, A.; Vettor, R.; Ermolao, A.; Busetto, L. Edmonton Obesity Staging System: An improvement by cardiopulmonary exercise testing. Int. J. Obes. 2021, 45, 1949–1957. [Google Scholar] [CrossRef]
- Capodaglio, P.; Castelnuovo, G.; Brunani, A.; Vismara, L.; Villa, V.; Capodaglio, E.M. Functional limitations and occupational issues in obesity: A review. Int. J. Occup. Saf. Ergon. 2010, 16, 507–523. [Google Scholar] [CrossRef]
- Ortega, F.B.; Cadenas-Sanchez, C.; Lee, D.; Ruiz, J.R.; Blair, S.N.; Sui, X. Fitness and Fatness as Health Markers through the Lifespan: An Overview of Current Knowledge. Prog. Prev. Med. 2018, 3, e0013. [Google Scholar] [CrossRef]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. Pharmacoeconomics 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Tam, B.T.; Morais, J.A.; Santosa, S. Obesity and ageing: Two sides of the same coin. Obes. Rev. 2020, 21, e12991. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing. Mayo Clin. Proc. 2015, 90, 1515–1523. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Cahalin, L.P. Evaluation of cardiorespiratory fitness and respiratory muscle function in the obese population. Prog. Cardiovasc. Dis. 2014, 56, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Conway, B.; Rene, A. Obesity as a disease: No lightweight matter. Obes. Rev. 2004, 5, 145–151. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory Fitness as a Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Helathy Men and Women: A Meta-Analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- Bouchard, D.R.; McGuire, K.A.; Davidson, L.; Ross, R. Cardiorespiratory fitness, obesity, and functional limitation in older adults. J. Aging Phys. Act. 2011, 19, 336–346. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, D.; Forman, D.E. The importance of physical function as a clinical outcome: Assessment and enhancement. Clin. Cardiol. 2020, 43, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American heart association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef]
- Wasserman, K.; Hansen, J.E.; Sue, D.Y.; Stringer, W.W.; Sietsema, K.E.; Sun, X.-G.; Whipp, B.J. Priciples of Exercise Testing and Interpretation: Including Pathophysiology and Clinical Applications, 5th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: New York, NY, USA, 2011. [Google Scholar]
- Neunhaeuserer, D.; Gasperetti, A.; Savalla, F.; Gobbo, S.; Bullo, V.; Bergamin, M.; Foletto, M.; Vettor, R.; Zaccaria, M.; Ermolao, A. Functional Evaluation in Obese Patients Before and After Sleeve Gastrectomy. Obes. Surg. 2017, 27, 3230–3239. [Google Scholar] [CrossRef]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood Obesity: Causes, Consequences, and Management. Pediatr. Clin. N. Am. 2015, 62, 821–840. [Google Scholar] [CrossRef]
- Jackson, A.S.; Sui, X.; O’Connor, D.P.; Church, T.S.; Lee, D.C.; Artero, E.G.; Blair, S.N. Longitudinal cardiorespiratory fitness algorithms for clinical settings. Am. J. Prev. Med. 2012, 43, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Stathokostas, L.; Jacob-Johnson, S.; Petrella, R.J.; Paterson, D.H. Longitudinal changes in aerobic power in older men and women. J. Appl. Physiol. 2004, 97, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Battista, F.; Belligoli, A.; Neunhaeuserer, D.; Gasperetti, A.; Bettini, S.; Compagnin, C.; Marchese, R.; Quinto, G.; Bergamin, M.; Vettor, R.; et al. Metabolic Response to Submaximal and Maximal Exercise in People with Severe Obesity, Prediabetes, and Diabetes. Obes. Facts 2021, 14, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Borasio, N.; Vecchiato, M.; Quinto, G.; Battista, F.; Neunhaeuserer, D.; Ermolao, A. Correspondence regarding ‘Ventilatory efficiency in athletes, asthma and obesity’: Different ventilatory phenotypes during exercise in obesity? Eur. Respir. Rev. 2022, 31, 21025. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; Barendregt, J.J.; Willekens, F.; Mackenbach, J.P.; Al Mamun, A.; Bonneux, L. Obesity in adulthood and its consequences for life expectancy: A life-table analysis. Ann. Intern. Med. 2003, 138, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; Bonneux, L.; Nusselder, W.J.; de Laet, C.; Barendregt, J.J. Adult obesity and the burden of disability throughout life. Obes. Res. 2004, 12, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Coombes, J.S.; Stowasser, M.; Bailey, T.G. The Role of Exercise in Patients with Obesity and Hypertension. Curr. Hypertens. Rep. 2020, 22, 77. [Google Scholar] [CrossRef]
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Fagerland, M.W.; Johannessen, J.S.; Hansen, B.H.; Jefferis, B.J.; Whincup, P.H.; Diaz, K.M.; Hooker, S.; Howard, V.J.; et al. Joint associations of accelero-meter measured physical activity and sedentary time with all-cause mortality: A harmonised meta-analysis in more than 44 000 middle-aged and older individuals. Br. J. Sports Med. 2020, 54, 1499–1506. [Google Scholar] [CrossRef]
- Oppert, J.M.; Bellicha, A.; van Baak, M.A.; Battista, F.; Beaulieu, K.; Blundell, J.E.; Carraça, E.V.; Encantado, J.; Ermolao, A.; Pramono, A.; et al. Exercise training in the management of overweight and obesity in adults: Synthesis of the evidence and recommendations from the European Association for the Stuy of Obesity Physical Activity Working Group. Obes. Rev. 2021, 22, e13273. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Age, Years | 45.5 ± 12.3 |
| BMI, kg/m2 | 41.7 ± 6.7 |
| Hypertension, N (%) | 183 (33.8) |
| Arthropathy, N (%) | 111 (20.5) |
| Dyslipidemia, N (%) | 106 (19.6) |
| Type 2 diabetes, N (%) | 101 (18.6) |
| Hypothyroidism, N (%) | 76 (14.0) |
| OSAS, N (%) | 76 (14.0) |
| Asthma, N (%) | 45 (8.3) |
| Depression, N (%) | 36 (6.6) |
| CPET | |
| VO2peak/kg (mL/min/kg) | 20.9 ± 4.8 |
| VO2 peak (L/min) | 2.41 ± 0.6 |
| VO2peak% | 101.3 ± 16.7 |
| RER | 1.15 ± 0.09 |
| OUESs (mL/LogL) | 2424.4 ± 651.5 |
| VE/VCO2 slope | 26.3 ± 3.5 |
| BMI (kg/m2) | 30–35 | 35–40 | 40–45 | >45 | ANOVA | |||
|---|---|---|---|---|---|---|---|---|
| N | 92 | 144 | 151 | 155 | p | |||
| VO2peak (L/min) | 2.28 ± 0.74 | * | 2.29 ± 0.61 | * | 2.45 ± 0.52 | 2.56 ± 0.57 | 0.0002 | |
| VO2peak (mL/min/kg) | 24.58 ± 6.85 | *§‡ | 21.76 ± 4.48 | * | 20.83 ± 3.13 | * | 18.0 ± 2.81 | <0.0001 |
| VO2peak% | 103 ± 0.21; | * | 101 ± 0.18 | 105 ± 0.14 | * | 97 ± 0.13 | 0.007 | |
| OUES (ml/LogL) | 2109.6 ± 658.1 | *§ | 2285.3 ± 634.1 | *§ | 2479.9 ± 551.2 | * | 2686.3 ± 645.3 | <0.0001 |
| RER | 1.15 ± 0.08 | 1.16 ± 0.11 | * | 1.15 ± 0.12 | 1.13 ± 0.08 | 0.037 | ||
| VO2/HR% | 107.70 ± 27.55 | *§ | 100.38 ± 22.13 | *§ | 99.20 ± 19.58 | * | 85.02 ± 20.83 | <0.0001 |
| VE/VCO2 slope | 27.16 ± 3.93 | * | 26.17 ± 3.87 | 26.39 ± 4.22 | 25.82 ± 3.16 | 0.031 | ||
| BR | 28.67 ± 17.65 | *§‡ | 27.00 ± 15.10 | *§ | 21.39 ± 13.22 | 21.74 ± 13.58 | <0.0001 |
| VO2peak/kg (mL/kg/min) | |||||
|---|---|---|---|---|---|
| <17.86 (Q1) | >17.86 | OR (95% CI) | p | ||
| Gender | Males | 34 20.5% | 132 79.5% | 1.445 (0.931–2.244) | 0.1011 |
| Females | 102 27.1% | 274 72.9% | |||
| Age (years) | <39 | 15 11.6% | 114 88.4% | - | |
| <39 vs. | 39–47 | 29 20.7% | 111 79.3% | 1.985 (1.010–3.903) | <0.0001 |
| 47–54 | 33 26.0% | 94 74.0% | 2.668 (1.367–5.206) | ||
| >54 | 59 40.4% | 87 59.6% | 5.153 (2.740–9.693) | ||
| BMI (kg/m2) | 30–35 | 14 15.2% | 78 84.8% | - | |
| 30–35 vs. | 35–40 | 27 18.6% | 117 81.4% | 1.286 (0.635–2.605) | <0.0001 |
| 40–45 | 24 15.9% | 127 84.1% | 1.053 (0.514–2.156) | ||
| >45 | 71 45.8% | 84 54.2% | 4.709 (2.457–9.027) | ||
| Number of comorbidities | 0 | 28 16.0% | 147 84.0% | - | |
| 0 vs. | 1 | 37 24.7% | 113 75.3% | 1.719 (0.993–2.976) | 0.0006 |
| 2 | 33 27.6% | 86 72.3% | 2.015 (1.140–3.561) | ||
| >2 | 38 38.8% | 60 61.2% | 3.325 (1.875–5.898) | ||
| OR (95% CI) | p | ||
|---|---|---|---|
| Age (years) <39 vs. | 39–47 | 1.885 (0.909–3.906) | <0.0001 |
| 47–54 | 2.549 (1.205–5.392) | ||
| >54 | 6.132 (2.859–13.153) | ||
| BMI (kg/m2) <35 vs. | 35–40 | 1.154 (0.551–2.418) | <0.0001 |
| 40–45 | 1.064 (0.502–2.255) | ||
| >45 | 5.864 (2.920–11.778) | ||
| Number of comorbidities 0 vs. | 1 | 1.401 (0.762–2.579) | 0.5447 |
| 2 | 1.148 (0.592–2.229) | ||
| >2 | 1.562 (0.774–3.150) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Battista, F.; Neunhaeuserer, D.; Centanini, A.; Gasperetti, A.; Quinto, G.; Vecchiato, M.; Bianchi, E.; Frigo, A.C.; Bettini, S.; Vettor, R.; et al. The “Aging Effect” of BMI on Cardiorespiratory Fitness: A New Insight on Functional Evaluation in Obesity. J. Clin. Med. 2023, 12, 7183. https://doi.org/10.3390/jcm12227183
Battista F, Neunhaeuserer D, Centanini A, Gasperetti A, Quinto G, Vecchiato M, Bianchi E, Frigo AC, Bettini S, Vettor R, et al. The “Aging Effect” of BMI on Cardiorespiratory Fitness: A New Insight on Functional Evaluation in Obesity. Journal of Clinical Medicine. 2023; 12(22):7183. https://doi.org/10.3390/jcm12227183
Chicago/Turabian StyleBattista, Francesca, Daniel Neunhaeuserer, Anna Centanini, Andrea Gasperetti, Giulia Quinto, Marco Vecchiato, Elia Bianchi, Anna Chiara Frigo, Silvia Bettini, Roberto Vettor, and et al. 2023. "The “Aging Effect” of BMI on Cardiorespiratory Fitness: A New Insight on Functional Evaluation in Obesity" Journal of Clinical Medicine 12, no. 22: 7183. https://doi.org/10.3390/jcm12227183
APA StyleBattista, F., Neunhaeuserer, D., Centanini, A., Gasperetti, A., Quinto, G., Vecchiato, M., Bianchi, E., Frigo, A. C., Bettini, S., Vettor, R., Busetto, L., & Ermolao, A. (2023). The “Aging Effect” of BMI on Cardiorespiratory Fitness: A New Insight on Functional Evaluation in Obesity. Journal of Clinical Medicine, 12(22), 7183. https://doi.org/10.3390/jcm12227183