

The CHANGED Score—A New Tool for the Prediction of Insulin Dependency in Gestational Diabetes
 , ,
, , 
Abstract
:1. Introduction
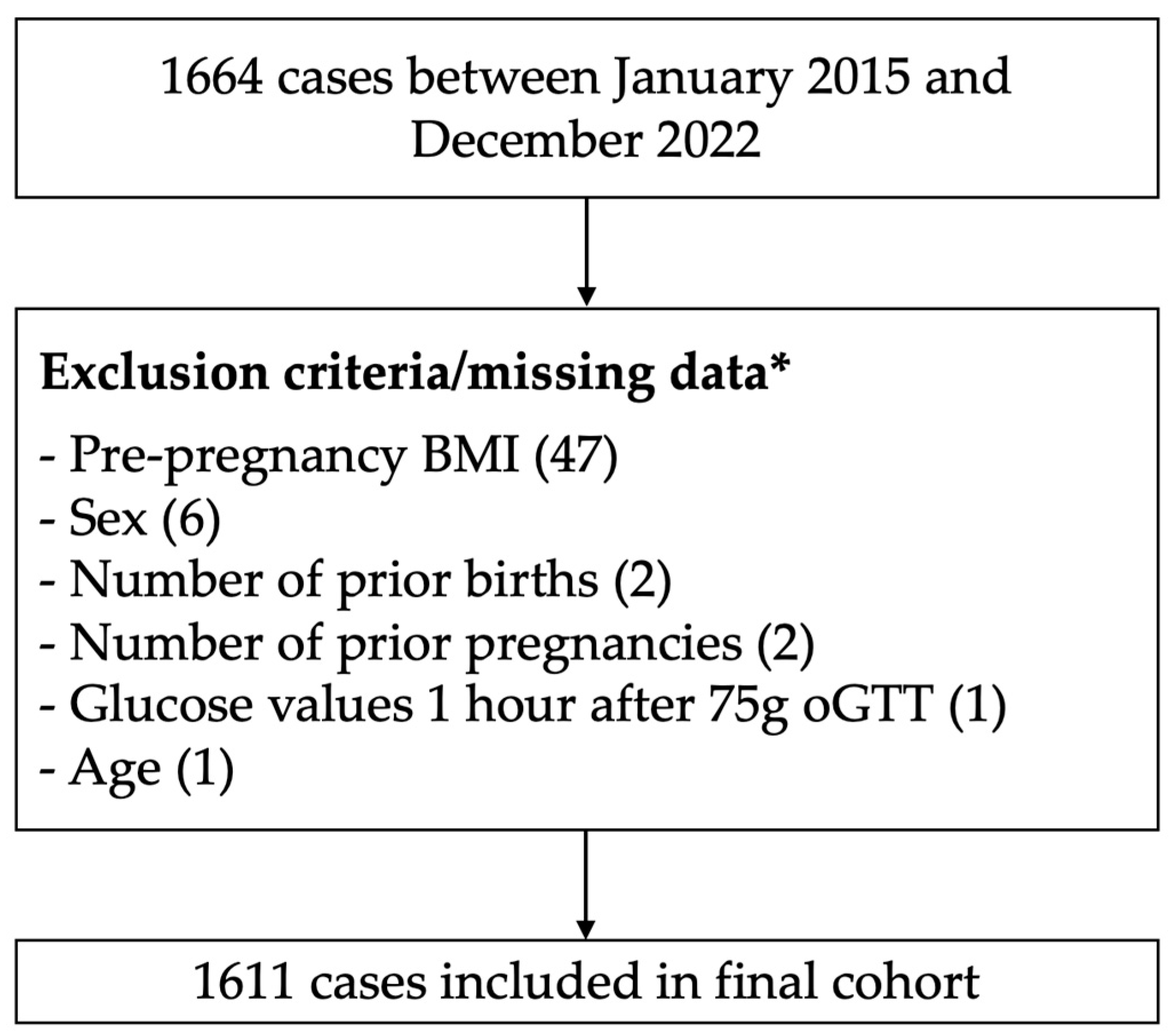
2. Materials and Methods
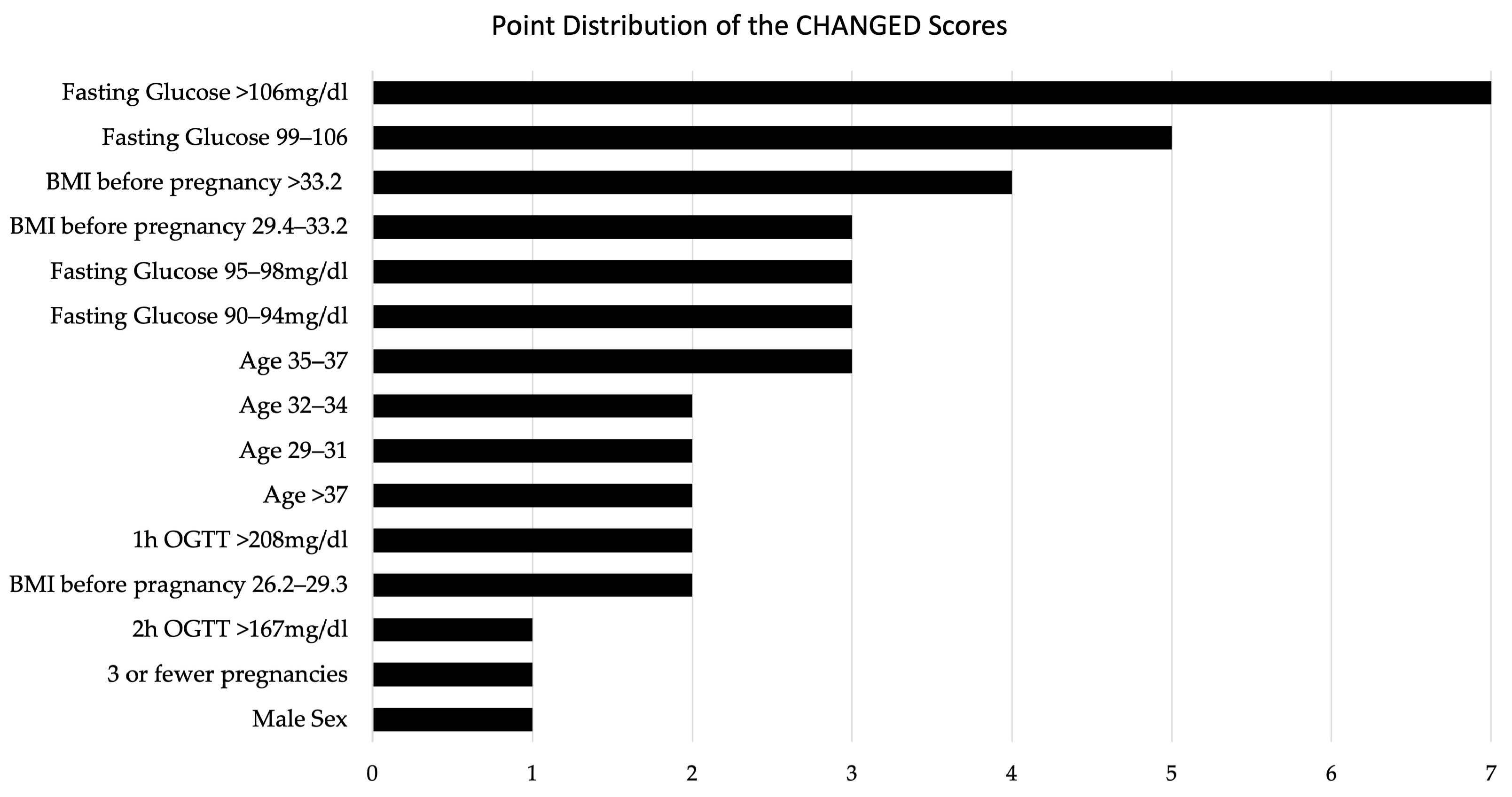
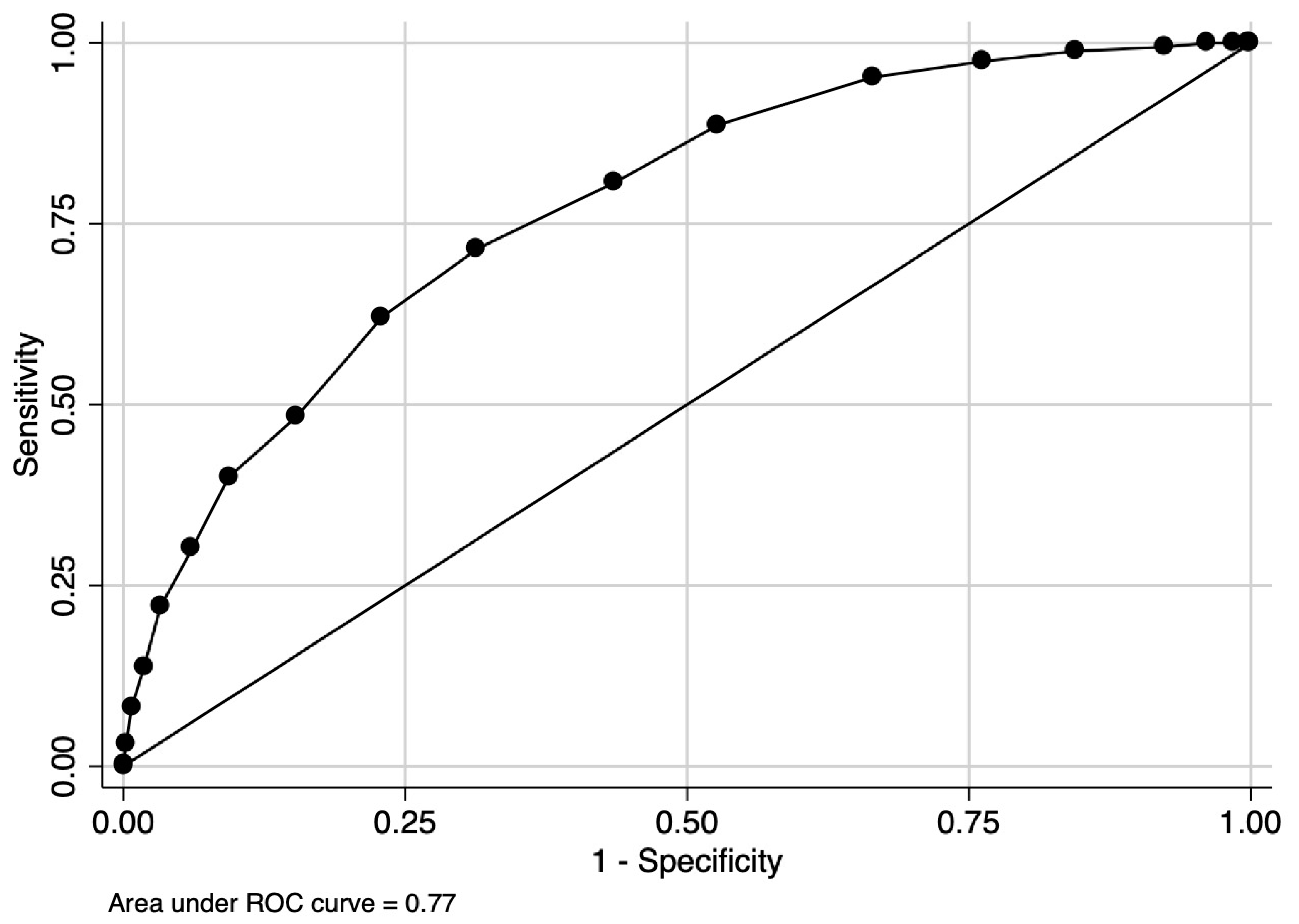
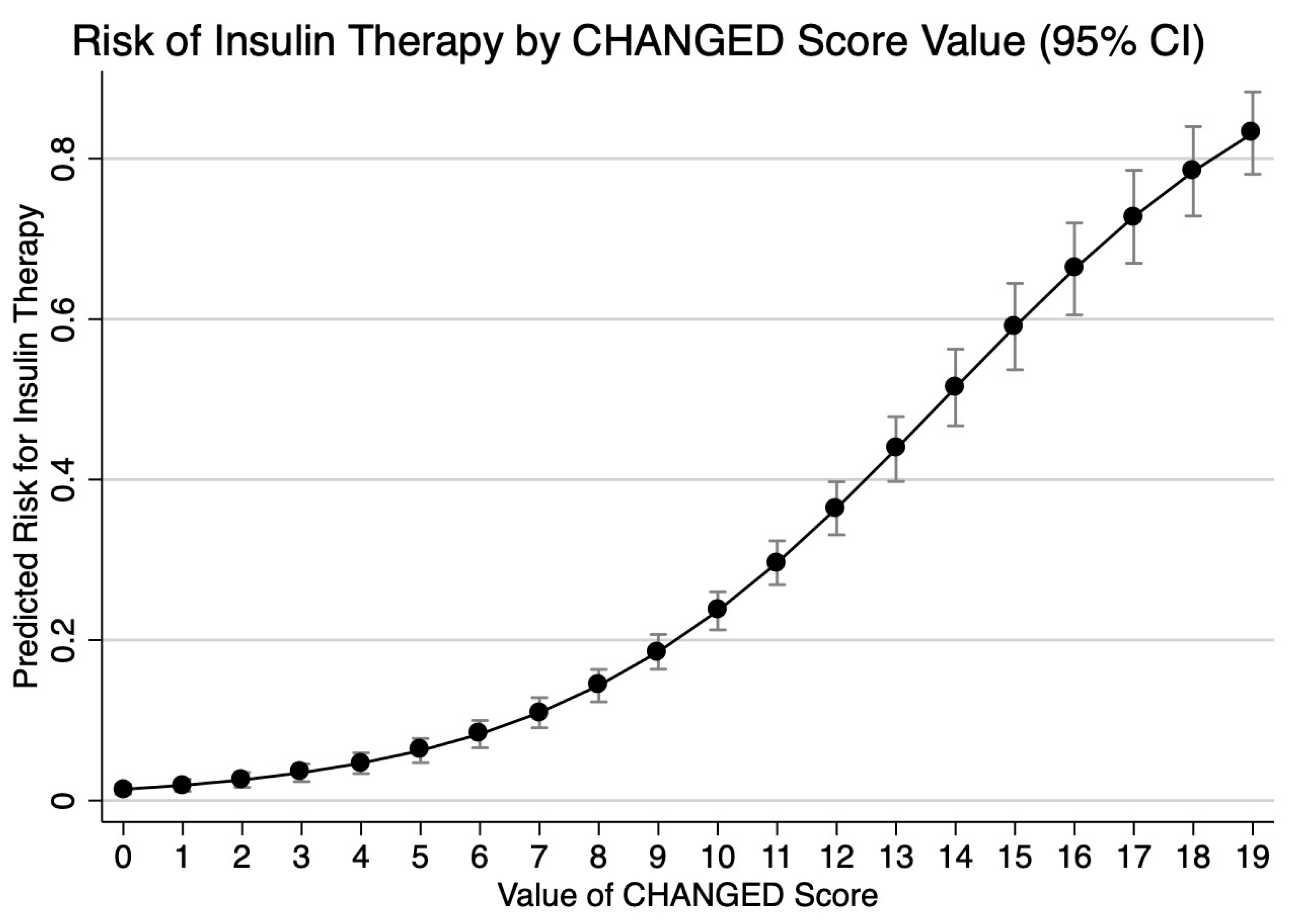
3. Results
4. Discussion
4.1. Main Findings
4.2. Results in Context of the Literature
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goyal, A.; Gupta, Y.; Singla, R.; Kalra, S.; Tandon, N. American Diabetes Association “Standards of Medical Care—2020 for Gestational Diabetes Mellitus”: A Critical Appraisal. Diabetes Ther. Res. Treat. Educ. Diabetes Relat. Disord. 2020, 11, 1639–1644. [Google Scholar] [CrossRef]
- Carr, D.B.; Gabbe, S. Gestational Diabetes: Detection, Management, and Implications. Clin. Diabetes 1998, 16, 4. [Google Scholar]
- Hoffman, L.; Nolan, C.; Wilson, J.D.; Oats, J.J.N.; Simmons, D.; Nolan, F.C.; Wilson, F.J.D.; Dm, F.J.J.N.O. Gestational Diabetes Mellitus—Management Guidelines: The Australasian Diabetes in Pregnancy Society. Med. J. Aust. 1998, 169, 93–97. [Google Scholar] [CrossRef]
- Bulletin, A.P. Clinical Management Guidelines for Obstetrician-Gynecologists Use of Psychiatric Medications during Pregnancy and Lactation. FOCUS 2009, 7, 385–400. [Google Scholar] [CrossRef]
- Guariguata, L.; Linnenkamp, U.; Beagley, J.; Whiting, D.R.; Cho, N.H. Global Estimates of the Prevalence of Hyperglycaemia in Pregnancy. Diabetes Res. Clin. Pract. 2014, 103, 176–185. [Google Scholar] [CrossRef]
- Reitzle, L.; Schmidt, C.; Heidemann, C.; Icks, A.; Kaltheuner, M.; Ziese, T.; Scheidt-Nave, C. Gestational Diabetes in Germany: Development of Screening Participation and Prevalence. J. Health Monit. 2021, 6, 3–18. [Google Scholar] [CrossRef]
- Zhou, T.; Du, S.; Sun, D.; Li, X.; Heianza, Y.; Hu, G.; Sun, L.; Pei, X.; Shang, X.; Qi, L. Prevalence and Trends in Gestational Diabetes Mellitus among Women in the United States, 2006–2017: A Population-Based Study. Front. Endocrinol. 2022, 13, 868094. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ren, X.; He, L.; Li, J.; Zhang, S.; Chen, W. Maternal Age and the Risk of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of over 120 Million Participants. Diabetes Res. Clin. Pract. 2020, 162, 108044. [Google Scholar] [CrossRef]
- Coustan, D.R.; Carpenter, M.W.; O’Sullivan, P.S.; Carr, S.R. Gestational Diabetes: Predictors of Subsequent Disordered Glucose Metabolism. Am. J. Obstet. Gynecol. 1993, 168, 1135–1139. [Google Scholar] [CrossRef]
- Yogev, Y.; Chen, R.; Hod, M.; Coustan, D.R.; Oats, J.J.N.; Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.; McCance, D. Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study: Preeclampsia. Am. J. Obstet. Gynecol. 2010, 202, 255.e1–255.e7. [Google Scholar] [CrossRef]
- Kwik, M.; Seeho, S.K.M.; Smith, C.; McElduff, A.; Morris, J.M. Outcomes of Pregnancies Affected by Impaired Glucose Tolerance. Diabetes Res. Clin. Pract. 2007, 77, 263–268. [Google Scholar] [CrossRef]
- Bérard, J.; Dufour, P.; Vinatier, D.; Subtil, D.; Vanderstichèle, S.; Monnier, J.C.; Puech, F. Fetal Macrosomia: Risk Factors and Outcome. A Study of the Outcome Concerning 100 Cases >4500 G. Eur. J. Obstet. Gynecol. Reprod. Biol. 1998, 77, 51–59. [Google Scholar] [CrossRef]
- Stotland, N.E.; Caughey, A.B.; Breed, E.M.; Escobar, G.J. Risk Factors and Obstetric Complications Associated with Macrosomia. Int. J. Gynecol. Obstet. 2004, 87, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Yogev, Y.; Xenakis, E.M.J.; Langer, O. The Association between Preeclampsia and the Severity of Gestational Diabetes: The Impact of Glycemic Control. Am. J. Obstet. Gynecol. 2004, 191, 1655–1660. [Google Scholar] [CrossRef]
- Riskin-Mashiah, S.; Younes, G.; Damti, A.; Auslender, R. First-Trimester Fasting Hyperglycemia and Adverse Pregnancy Outcomes. Diabetes Care 2009, 32, 1639–1643. [Google Scholar] [CrossRef] [PubMed]
- Bhavadharini, B.; Anjana, R.M.; Deepa, M.; Pradeepa, R.; Uma, R.; Saravanan, P.; Mohan, V. Association between Number of Abnormal Glucose Values and Severity of Fasting Plasma Glucose in IADPSG Criteria and Maternal Outcomes in Women with Gestational Diabetes Mellitus. Acta Diabetol. 2022, 59, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Caughey, A.B.; Turrentine, M. ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 131, e49–e64. [Google Scholar] [CrossRef]
- Hartling, L.; Dryden, D.M.; Guthrie, A.; Muise, M.; Vandermeer, B.; Donovan, L. Benefits and Harms of Treating Gestational Diabetes Mellitus: A Systematic Review and Meta-analysis for the U.S. Preventive Services Task Force and the National Institutes of Health Office of Medical Applications of Research. Ann. Intern. Med. 2013, 159, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriades, M.; Chatzakis, C.; Papachatzopoulou, E.; Papadopoulos, V.; Lambrinoudaki, I.; Dinas, K.; Chrousos, G.; Sotiriadis, A. Prediction of Insulin Treatment in Women with Gestational Diabetes Mellitus. Nutr. Diabetes 2021, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Pertot, T.; Molyneaux, L.; Tan, K.; Ross, G.P.; Yue, D.K.; Wong, J. Can Common Clinical Parameters Be Used to Identify Patients Who Will Need Insulin Treatment in Gestational Diabetes Mellitus? Diabetes Care 2011, 34, 2214–2216. [Google Scholar] [CrossRef]
- Balke, S.; Weid, P.; Fangmann, L.; Rostin, P.; Henrich, W.; Koenigbauer, J.T. Glucose Levels of the Oral Glucose Tolerance Test (OGTT) Can Predict Adverse Pregnancy Outcomes in Women with Gestational Diabetes (GDM). J. Clin. Med. 2023, 12, 3709. [Google Scholar] [CrossRef]
- Josefine Theresia, K.; Laura, F.; Paul, R.; Selina, B.; Petra, W.; Wolfgang, H.; Alexander, W.; Göbl, C. Advanced Maternal Age (AMA) and 75 g OGTT Glucose Levels Are Pedictors for Insulin Therapy in Women with Gestational Diabetes (GDM). J. Perinat. Med. 2023, 51, 1154–1162. [Google Scholar] [CrossRef]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; de Leiva, A.; Hod, M.; Kitzmiler, J.L.; et al. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Schäfer-Graf, U.M.; Gembruch, U.; Kainer, F.; Groten, T.; Hummel, S.; Hösli, I.; Grieshop, M.; Kaltheuner, M.; Bührer, C.; Kautzky-Willer, A.; et al. Gestational Diabetes Mellitus (GDM)—Diagnosis, Treatment and Follow-Up. Guideline of the DDG and DGGG (S3 Level, AWMF Registry Number 057/008, February 2018). Geburtshilfe Frauenheilkd. 2018, 78, 1219–1231. [Google Scholar] [CrossRef] [PubMed]
- Brier, G.W. Verification of Forecasts Expressed in Terms of Probability. Mon. Weather Rev. 1950, 78, 745–753. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Taber, S.; Lemeshow, S. The Importance of Assessing the Fit of Logistic Regression Models: A Case Study. Am. J. Public Health 1991, 81, 1630–1635. [Google Scholar] [CrossRef]
- Liu, X. Classification Accuracy and Cut Point Selection. Stat. Med. 2012, 31, 2676–2686. [Google Scholar] [CrossRef]
- Shin, C.H.; Grabitz, S.D.; Timm, F.P.; Mueller, N.; Chhangani, K.; Ladha, K.; Devine, S.; Kurth, T.; Eikermann, M. Development and Validation of a Score for Preoperative Prediction of Obstructive Sleep Apnea (SPOSA) and Its Perioperative Outcomes. BMC Anesthesiol. 2017, 17, 71. [Google Scholar] [CrossRef]
- Teede, H.J.; Harrison, C.L.; Teh, W.T.; Paul, E.; Allan, C.A. Gestational Diabetes: Development of An Early Risk Prediction Tool to Facilitate Opportunities for Prevention. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 499–504. [Google Scholar] [CrossRef]
- Kotzaeridi, G.; Blätter, J.; Eppel, D.; Rosicky, I.; Linder, T.; Geissler, F.; Huhn, E.A.; Hösli, I.; Tura, A.; Göbl, C.S. Characteristics of Gestational Diabetes Subtypes Classified by Oral Glucose Tolerance Test Values. Eur. J. Clin. Investig. 2021, 51, e13628. [Google Scholar] [CrossRef] [PubMed]
- Torloni, M.R.; Betrán, A.P.; Horta, B.L.; Nakamura, M.U.; Atallah, A.N.; Moron, A.F.; Valente, O. Prepregnancy BMI and the Risk of Gestational Diabetes: A Systematic Review of the Literature with Meta-Analysis. Obes. Rev. 2009, 10, 194–203. [Google Scholar] [CrossRef]
- Maier, J.T.; Schalinski, E.; Gauger, U.; Hellmeyer, L. Antenatal Body Mass Index (BMI) and Weight Gain in Pregnancy—Its Association with Pregnancy and Birthing Complications. J. Perinat. Med. 2016, 44, 397–404. [Google Scholar] [CrossRef]
- Lee, S.-H.; Yu, J.; Han, K.; Lee, S.W.; You, S.Y.; Kim, H.-S.; Cho, J.-H.; Yoon, K.-H.; Kim, M.K. Predicting the Risk of Insulin-Requiring Gestational Diabetes before Pregnancy: A Model Generated from a Nationwide Population-Based Cohort Study in Korea. Endocrinol. Metab. 2023, 38, 129–138. [Google Scholar] [CrossRef]
- Goyal, A.; Gupta, Y.; Kalaivani, M.; Sankar, M.J.; Kachhawa, G.; Bhatla, N.; Gupta, N.; Tandon, N. Long term (>1 year) postpartum Glucose Tolerance Status among Indian Women with History of Gestational Diabetes Mellitus (GDM) Diagnosed by IADPSG Criteria. Diabetes Res. Clin. Pract. 2018, 142, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Landon, M.B.; Spong, C.Y.; Thom, E.; Carpenter, M.W.; Ramin, S.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. A Multicenter, Randomized Trial of Treatment for Mild Gestational Diabetes. N. Engl. J. Med. 2009, 361, 1339–1348. [Google Scholar] [CrossRef]
- Simmons, D.; Immanuel, J.; Hague, W.M.; Teede, H.; Nolan, C.J.; Peek, M.J.; Flack, J.R.; McLean, M.; Wong, V.; Hibbert, E.; et al. Treatment of Gestational Diabetes Mellitus Diagnosed Early in Pregnancy. N. Engl. J. Med. 2023, 388, 2132–2144. [Google Scholar] [CrossRef] [PubMed]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.K.; Cruz, M.; Wong, A.; Davitt, C.; Palatnik, A. The Timing of Initiation of Pharmacotherapy for Women with Gestational Diabetes Mellitus. BMC Pregnancy Childbirth 2020, 20, 773. [Google Scholar] [CrossRef]
- Tartaglione, L.; di Stasio, E.; Sirico, A.; Di Leo, M.; Caputo, S.; Rizzi, A.; Caneschi, A.; De Carolis, S.; Pitocco, D.; Lanzone, A. Continuous Glucose Monitoring in Women with Normal OGTT in Pregnancy. J. Diabetes Res. 2021, 2021, 9987646. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No Insulin (n = 1249) | Insulin (n = 362) | p-Value |
|---|---|---|---|
| Sex, female | 580 (46.4%) | 141 (39.0%) | 0.012 |
| Age, median (IQR) | 32.00 (28.00, 36.00) | 34.00 (30.00, 37.00) | 0.001 |
| BMI_early, median (IQR) | 26.60 (23.10, 31.10) | 30.50 (27.20, 35.30) | <0.001 |
| Glucose_0 h, median (IQR) | 95.00 (89.00, 101.00) | 103.00 (96.00, 111.00) | <0.001 |
| Glucose_1 h, median (IQR) | 181.00 (155.00, 198.00) | 193.00 (169.00, 219.00) | <0.001 |
| Glucose_2 h, median (IQR) | 136.00 (116.00, 158.00) | 149.00 (126.00, 176.00) | <0.001 |
| Parity, median (IQR) | 1.00 (0.00, 2.00) | 1.00 (0.00, 2.00) | 0.002 |
| Gravida, median (IQR) | 3.00 (2.00, 4.00) | 3.00 (2.00, 4.00) | 0.008 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rostin, P.; Balke, S.; Sroka, D.; Fangmann, L.; Weid, P.; Henrich, W.; Königbauer, J.T. The CHANGED Score—A New Tool for the Prediction of Insulin Dependency in Gestational Diabetes. J. Clin. Med. 2023, 12, 7169. https://doi.org/10.3390/jcm12227169
Rostin P, Balke S, Sroka D, Fangmann L, Weid P, Henrich W, Königbauer JT. The CHANGED Score—A New Tool for the Prediction of Insulin Dependency in Gestational Diabetes. Journal of Clinical Medicine. 2023; 12(22):7169. https://doi.org/10.3390/jcm12227169
Chicago/Turabian StyleRostin, Paul, Selina Balke, Dorota Sroka, Laura Fangmann, Petra Weid, Wolfgang Henrich, and Josefine Theresia Königbauer. 2023. "The CHANGED Score—A New Tool for the Prediction of Insulin Dependency in Gestational Diabetes" Journal of Clinical Medicine 12, no. 22: 7169. https://doi.org/10.3390/jcm12227169
APA StyleRostin, P., Balke, S., Sroka, D., Fangmann, L., Weid, P., Henrich, W., & Königbauer, J. T. (2023). The CHANGED Score—A New Tool for the Prediction of Insulin Dependency in Gestational Diabetes. Journal of Clinical Medicine, 12(22), 7169. https://doi.org/10.3390/jcm12227169