

Multivariable Risk Modelling and Survival Analysis with Machine Learning in SARS-CoV-2 Infection

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. CT-Acquisition Parameters and Interpretation
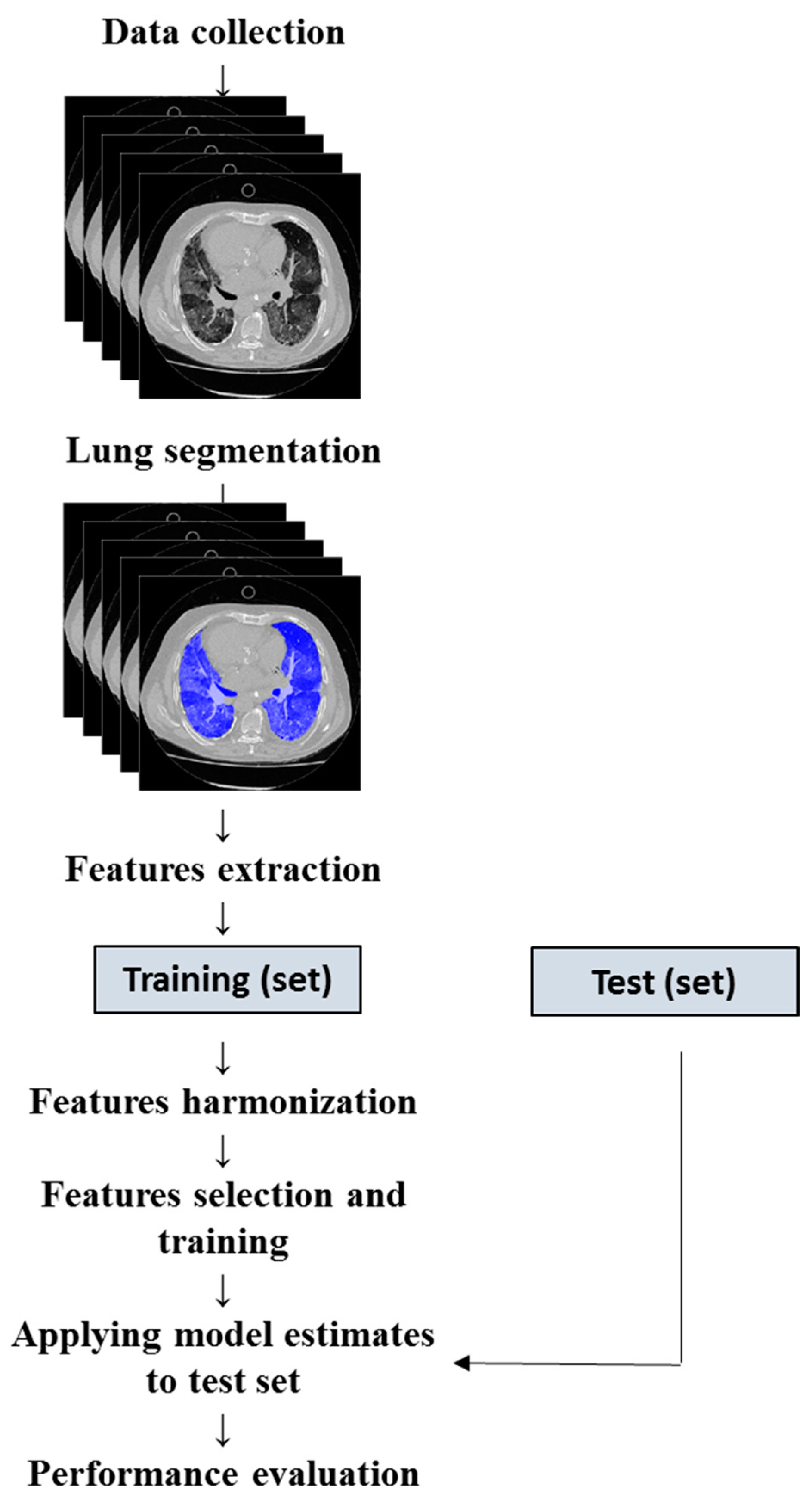
2.3. Image Analysis and Texture Features Extraction
2.4. Feature Selection and Classification
2.5. Model Design
2.6. Model Validation and Calibration
2.7. Statistical Analysis
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese center for disease control and prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Lambrou, A.S.; Shirk, P.; Steele, M.K.; Paul, P.; Paden, C.R.; Cadwell, B.; Reese, H.E.; Aoki, Y.; Hassell, N.; Zheng, X.Y.; et al. Genomic surveillance for SARS-CoV-2 variants: Predominance of the delta (b.1.617.2) and omicron (b.1.1.529) variants—United states, June 2021–January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Delerce, J.; Burel, E.; Dahan, J.; Jouffret, A.; Fenollar, F.; Yahi, N.; Fantini, J.; La Scola, B.; Raoult, D. Emergence in southern france of a new SARS-CoV-2 variant harbouring both n501y and e484k substitutions in the spike protein. Arch. Virol. 2022, 167, 1185–1190. [Google Scholar] [CrossRef] [PubMed]
- Vadiati, M.; Beynaghi, A.; Bhattacharya, P.; Bandala, E.R.; Mozafari, M. Indirect effects of covid-19 on the environment: How deep and how long? Sci. Total Environ. 2022, 810, 152255. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Ceasovschih, A.; Sorodoc, V.; Shor, A.; Haliga, R.E.; Roth, L.; Lionte, C.; Onofrei Aursulesei, V.; Sirbu, O.; Culis, N.; Shapieva, A.; et al. Distinct Features of Vascular Diseases in COVID-19. J. Inflamm. Res. 2023, 16, 2783–2800. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of Covid-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef]
- Esposito, A.; Palmisano, A.; Cao, R.; Rancoita, P.; Landoni, G.; Grippaldi, D.; Boccia, E.; Cosenza, M.; Messina, A.; La Marca, S.; et al. Quantitative assessment of lung involvement on chest CT at admission: Impact on hypoxia and outcome in COVID-19 patients. Clin. Imaging 2021, 77, 194–201. [Google Scholar] [CrossRef]
- Bonanad, C.; Garcia-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-Gonzalez, V.; Facila, L.; Ariza, A.; Nunez, J.; Cordero, A. The Effect of Age on Mortality in Patients With COVID-19: A Meta-Analysis With 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Huang, I.; Pranata, R.; Lim, M.A.; Oehadian, A.; Alisjahbana, B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: A meta-analysis. Ther. Adv. Respir. Dis. 2020, 14, 1753466620937175. [Google Scholar] [CrossRef]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, E86–E96. [Google Scholar] [CrossRef]
- Huang, L.; Han, R.; Ai, T.; Yu, P.; Kang, H.; Tao, Q.; Xia, L. Serial Quantitative Chest CT Assessment of COVID-19: A Deep Learning Approach. Radiol. Cardiothorac. Imaging 2020, 2, e200075. [Google Scholar] [CrossRef] [PubMed]
- Revel, M.P.; Boussouar, S.; de Margerie-Mellon, C.; Saab, I.; Lapotre, T.; Mompoint, D.; Chassagnon, G.; Milon, A.; Lederlin, M.; Bennani, S.; et al. Study of Thoracic CT in COVID-19: The STOIC Project. Radiology 2021, 301, E361–E370. [Google Scholar] [CrossRef] [PubMed]
- Zhan, J.; Li, H.; Yu, H.; Liu, X.; Zeng, X.; Peng, D.; Zhang, W. 2019 novel coronavirus (COVID-19) pneumonia: CT manifestations and pattern of evolution in 110 patients in Jiangxi, China. Eur. Radiol. 2021, 31, 1059–1068. [Google Scholar] [CrossRef]
- Zhao, C.; Xu, Y.; He, Z.; Tang, J.; Zhang, Y.; Han, J.; Shi, Y.; Zhou, W. Lung Segmentation and Automatic Detection of COVID-19 Using Radiomic Features from Chest CT Images. Pattern Recognit. 2021, 119, 108071. [Google Scholar] [CrossRef]
- Jiao, Z.; Choi, J.W.; Halsey, K.; Tran, T.M.L.; Hsieh, B.; Wang, D.; Eweje, F.; Wang, R.; Chang, K.; Wu, J.; et al. Prognostication of patients with COVID-19 using artificial intelligence based on chest x-rays and clinical data: A retrospective study. Lancet Digit. Health 2021, 3, e286–e294. [Google Scholar] [CrossRef]
- Tan, H.B.; Xiong, F.; Jiang, Y.L.; Huang, W.C.; Wang, Y.; Li, H.H.; You, T.; Fu, T.T.; Lu, R.; Peng, B.W. The study of automatic machine learning base on radiomics of non-focus area in the first chest CT of different clinical types of COVID-19 pneumonia. Sci. Rep. 2020, 10, 18926. [Google Scholar] [CrossRef]
- Shiri, I.; Sorouri, M.; Geramifar, P.; Nazari, M.; Abdollahi, M.; Salimi, Y.; Khosravi, B.; Askari, D.; Aghaghazvini, L.; Hajianfar, G.; et al. Machine learning-based prognostic modeling using clinical data and quantitative radiomic features from chest CT images in COVID-19 patients. Comput. Biol. Med. 2021, 132, 104304. [Google Scholar] [CrossRef]
- Guiot, J.; Vaidyanathan, A.; Deprez, L.; Zerka, F.; Danthine, D.; Frix, A.N.; Thys, M.; Henket, M.; Canivet, G.; Mathieu, S.; et al. Development and Validation of an Automated Radiomic CT Signature for Detecting COVID-19. Diagnostics 2020, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Kelly, B.; Lee, E.H.; Wang, H.; Zheng, J.; Zhang, W.; Halabi, S.; Liu, J.; Tian, Y.; Han, B.; et al. Multi-classifier-based identification of COVID-19 from chest computed tomography using generalizable and interpretable radiomics features. Eur. J. Radiol. 2021, 136, 109552. [Google Scholar] [CrossRef] [PubMed]
- Shiri, I.; Salimi, Y.; Pakbin, M.; Hajianfar, G.; Avval, A.H.; Sanaat, A.; Mostafaei, S.; Akhavanallaf, A.; Saberi, A.; Mansouri, Z.; et al. COVID-19 prognostic modeling using CT radiomic features and machine learning algorithms: Analysis of a multi-institutional dataset of 14,339 patients. Comput. Biol. Med. 2022, 145, 105467. [Google Scholar] [CrossRef]
- Zorzi, G.; Berta, L.; Rizzetto, F.; De Mattia, C.; Felisi, M.M.J.; Carrazza, S.; Nerini Molteni, S.; Vismara, C.; Scaglione, F.; Vanzulli, A.; et al. Artificial intelligence for differentiating COVID-19 from other viral pneumonias on CT: Comparative analysis of different models based on quantitative and radiomic approaches. Eur. Radiol. Exp. 2023, 7, 3. [Google Scholar] [CrossRef]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA—Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A Postreconstruction Harmonization Method for Multicenter Radiomic Studies in PET. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Society. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Ge, G.; Zhang, J. Feature selection methods and predictive models in CT lung cancer radiomics. J. Appl. Clin. Med. Phys. 2023, 24, e13869. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Yin, Y.; Wang, H.; Chang, Z.; Liu, Z.; Cui, L. A review of original articles published in the emerging field of radiomics. Eur. J. Radiol. 2020, 127, 108991. [Google Scholar] [CrossRef] [PubMed]
- Glmnet. Available online: http://cran.r-project.org/web/packages/glmnet (accessed on 1 March 2020).
- Dobbin, K.K.; Simon, R.M. Optimally splitting cases for training and testing high dimensional classifiers. BMC Med. Genom. 2011, 4, 31. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Steyerberg, E.W. Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating; Springer International Publishing: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef]
- Sun, Q.; Qiu, H.; Huang, M.; Yang, Y. Lower mortality of COVID-19 by early recognition and intervention: Experience from Jiangsu Province. Ann. Intensive Care 2020, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Goyal, D.K.; Mansab, F.; Iqbal, A.; Bhatti, S. Early intervention likely improves mortality in COVID-19 infection. Clin. Med. 2020, 20, 248–250. [Google Scholar] [CrossRef]
- Yang, N.; Liu, F.; Li, C.; Xiao, W.; Xie, S.; Yuan, S.; Zuo, W.; Ma, X.; Jiang, G. Diagnostic classification of coronavirus disease 2019 (COVID-19) and other pneumonias using radiomics features in CT chest images. Sci. Rep. 2021, 11, 17885. [Google Scholar] [CrossRef]
- Mouhat, B.; Besutti, M.; Bouiller, K.; Grillet, F.; Monnin, C.; Ecarnot, F.; Behr, J.; Capellier, G.; Soumagne, T.; Pili-Floury, S.; et al. Elevated D-dimers and lack of anticoagulation predict PE in severe COVID-19 patients. Eur. Respir. J. 2020, 56, 2001811. [Google Scholar] [CrossRef]
- Soni, M.; Gopalakrishnan, R.; Vaishya, R.; Prabu, P. D-dimer level is a useful predictor for mortality in patients with COVID-19: Analysis of 483 cases. Diabetes Metab. Syndr. 2020, 14, 2245–2249. [Google Scholar] [CrossRef]
- Poudel, A.; Poudel, Y.; Adhikari, A.; Aryal, B.B.; Dangol, D.; Bajracharya, T.; Maharjan, A.; Gautam, R. D-dimer as a biomarker for assessment of COVID-19 prognosis: D-dimer levels on admission and its role in predicting disease outcome in hospitalized patients with COVID-19. PLoS ONE 2021, 16, e0256744. [Google Scholar] [CrossRef]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.J.; Luo, X.L.; Xu, W.; Mao, B.; Dai, R.X.; Li, C.W.; Yu, L.; Gu, F.; Liang, S.; Lu, H.W.; et al. Viral infection in community acquired pneumonia patients with fever: A prospective observational study. J. Thorac. Dis. 2018, 10, 4387–4395. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Guan, B.; Su, T.; Liu, W.; Chen, M.; Bin Waleed, K.; Guan, X.; Gary, T.; Zhu, Z. Impact of cardiovascular disease and cardiac injury on in-hospital mortality in patients with COVID-19: A systematic review and meta-analysis. Heart 2020, 106, 1142–1147. [Google Scholar] [CrossRef] [PubMed]
- Borges do Nascimento, I.J.; Cacic, N.; Abdulazeem, H.M.; von Groote, T.C.; Jayarajah, U.; Weerasekara, I.; Esfahani, M.A.; Civile, V.T.; Marusic, A.; Jeroncic, A.; et al. Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis. J. Clin. Med. 2020, 9, 941. [Google Scholar] [CrossRef]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.X. Susceptibility and prognosis of COVID-19 patients with cardiovascular disease. Open Heart 2020, 7, e001310. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Limkin, E.J.; Vakalopoulou, M.; Dercle, L.; Champiat, S.; Han, S.R.; Verlingue, L.; Brandao, D.; Lancia, A.; Ammari, S.; et al. A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: An imaging biomarker, retrospective multicohort study. Lancet. Oncol. 2018, 19, 1180–1191. [Google Scholar] [CrossRef]
- Ciarmiello, A.; Giovannini, E.; Pastorino, S.; Ferrando, O.; Foppiano, F.; Mannironi, A.; Tartaglione, A.; Giovacchini, G.; Alzheimer’s Disease Neuroimaging, I. Machine Learning Model to Predict Diagnosis of Mild Cognitive Impairment by Using Radiomic and Amyloid Brain PET. Clin. Nucl. Med. 2023, 48, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ciarmiello, A.; Giovannini, E.; Florimonte, L.; Bonatto, E.; Bareggi, C.; Milano, A.; Aschele, C.; Castellani, M. Machine learning radiomics for prediction of survival in non-small cell lung cancer patients studied with PET/CT and FDG. Ann. Oncol. 2021, 32, S926. [Google Scholar] [CrossRef]
- Hu, Z.; Yang, Z.; Lafata, K.J.; Yin, F.F.; Wang, C. A radiomics-boosted deep-learning model for COVID-19 and non-COVID-19 pneumonia classification using chest x-ray images. Med. Phys. 2022, 49, 3213–3222. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Observed Outcome | |||||
|---|---|---|---|---|---|
| Variable | Overall N = 694 | Alive N = 537 (77%) | Deceased N = 157 (23%) | Statistic | p-Value 1 |
| Age | 213 | <0.001 | |||
| Median (Range) | 64 (20–107) | 59 (20–94) | 80 (51–107) | ||
| Gender, n (%) | 0.07 | 0.8 | |||
| Female | 247 (36%) | 193 (36%) | 54 (34%) | ||
| Male | 447 (64%) | 344 (64%) | 103 (66%) | ||
| Hospital stay | 10 | 0.001 | |||
| Median (Range) | 11 (3–86) | 10 (3–86) | 13 (3–62) | ||
| CT findings, n (%) | 11 | 0.001 | |||
| Negative/Atypical | 284 (41%) | 238 (44%) | 46 (29%) | ||
| Typical | 410 (59%) | 299 (56%) | 111 (71%) | ||
| C-reactive protein | 19 | <0.001 | |||
| Median (Range) | 3 (0–37) | 3 (0–27) | 5 (1–37) | ||
| Lactate dehydrogenase | 97 | <0.001 | |||
| Median (Range) | 486 (78–3745) | 484 (78–3745) | 494 (141–3631) | ||
| D-dimer | 68 | <0.001 | |||
| Median (Range) | 1133 (96–152,015) | 1133 (96–55,660) | 6006 (168–152,015) | ||
| Comorbidity | Alive, N = 537 1 | Deceased, N = 157 1 | Odds Ratio 2 | 95% CI 2,3 | p-Value 2 |
|---|---|---|---|---|---|
| Cardiovascular disease | 90 (17%) | 74 (47%) | 4.42 | 2.95, 6.63 | <0.001 |
| Cancer | 2 (0%) | 9 (6%) | 16.2 | 3.30, 155 | <0.001 |
| Cerebrovascular disease | 9 (2%) | 14 (9%) | 5.72 | 2.25, 15.3 | <0.001 |
| Haematological disease | 14 (3%) | 13 (8%) | 3.36 | 1.42, 7.91 | 0.003 |
| Chronic obstructive pulmonary disease | 24 (4%) | 16 (10%) | 2.42 | 1.17, 4.90 | 0.011 |
| Blood cancer | 11 (2%) | 1 (1%) | 0.31 | 0.01, 2.14 | 0.3 |
| Hypertension | 66 (12%) | 16 (10%) | 0.81 | 0.42, 1.47 | 0.6 |
| Type 2 diabetes | 77 (14%) | 20 (13%) | 0.87 | 0.49, 1.50 | 0.7 |
| Obesity | 11 (2%) | 3 (2%) | 0.93 | 0.16, 3.59 | >0.9 |
| Observed | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Predicted | N | Deceased 1 | Alive 1 | X2 | p 2 | SS 95%CI 3 | SP 95%CI 4 | PPV 95%CI 5 | NPV 95%CI 6 | OR 95%CI 7 |
| Training | 556 | 140 | 2.1 × 10−32 | 97 (92, 99) | 64 (59, 68) | 44 (38, 50) | 99 (96, 100) | 48 (18, 125) | ||
| High risk | 122 (97%) | 156 (36%) | ||||||||
| Low risk | 4 (3.2%) | 274 (64%) | ||||||||
| Test | 138 | 24 | 9.8 × 10−7 | 90 (74, 98) | 62 (52, 71) | 41 (29, 53) | 96 (88, 99) | 13 (4, 42) | ||
| High risk | 28 (90%) | 41 (38%) | ||||||||
| Low risk | 3 (9.7%) | 66 (62%) | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciarmiello, A.; Tutino, F.; Giovannini, E.; Milano, A.; Barattini, M.; Yosifov, N.; Calvi, D.; Setti, M.; Sivori, M.; Sani, C.; et al. Multivariable Risk Modelling and Survival Analysis with Machine Learning in SARS-CoV-2 Infection. J. Clin. Med. 2023, 12, 7164. https://doi.org/10.3390/jcm12227164
Ciarmiello A, Tutino F, Giovannini E, Milano A, Barattini M, Yosifov N, Calvi D, Setti M, Sivori M, Sani C, et al. Multivariable Risk Modelling and Survival Analysis with Machine Learning in SARS-CoV-2 Infection. Journal of Clinical Medicine. 2023; 12(22):7164. https://doi.org/10.3390/jcm12227164
Chicago/Turabian StyleCiarmiello, Andrea, Francesca Tutino, Elisabetta Giovannini, Amalia Milano, Matteo Barattini, Nikola Yosifov, Debora Calvi, Maurizo Setti, Massimiliano Sivori, Cinzia Sani, and et al. 2023. "Multivariable Risk Modelling and Survival Analysis with Machine Learning in SARS-CoV-2 Infection" Journal of Clinical Medicine 12, no. 22: 7164. https://doi.org/10.3390/jcm12227164
APA StyleCiarmiello, A., Tutino, F., Giovannini, E., Milano, A., Barattini, M., Yosifov, N., Calvi, D., Setti, M., Sivori, M., Sani, C., Bastreri, A., Staffiere, R., Stefanini, T., Artioli, S., & Giovacchini, G. (2023). Multivariable Risk Modelling and Survival Analysis with Machine Learning in SARS-CoV-2 Infection. Journal of Clinical Medicine, 12(22), 7164. https://doi.org/10.3390/jcm12227164