

Self-Reported Physical Inactivity and Mood Disturbances in End-Stage Kidney Disease (ESKD) Patients on Chronic Dialysis Treatment


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Selection
2.2. Physical Activity Self-Assessment
2.3. Mood Disturbance Self-Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Population Characteristics
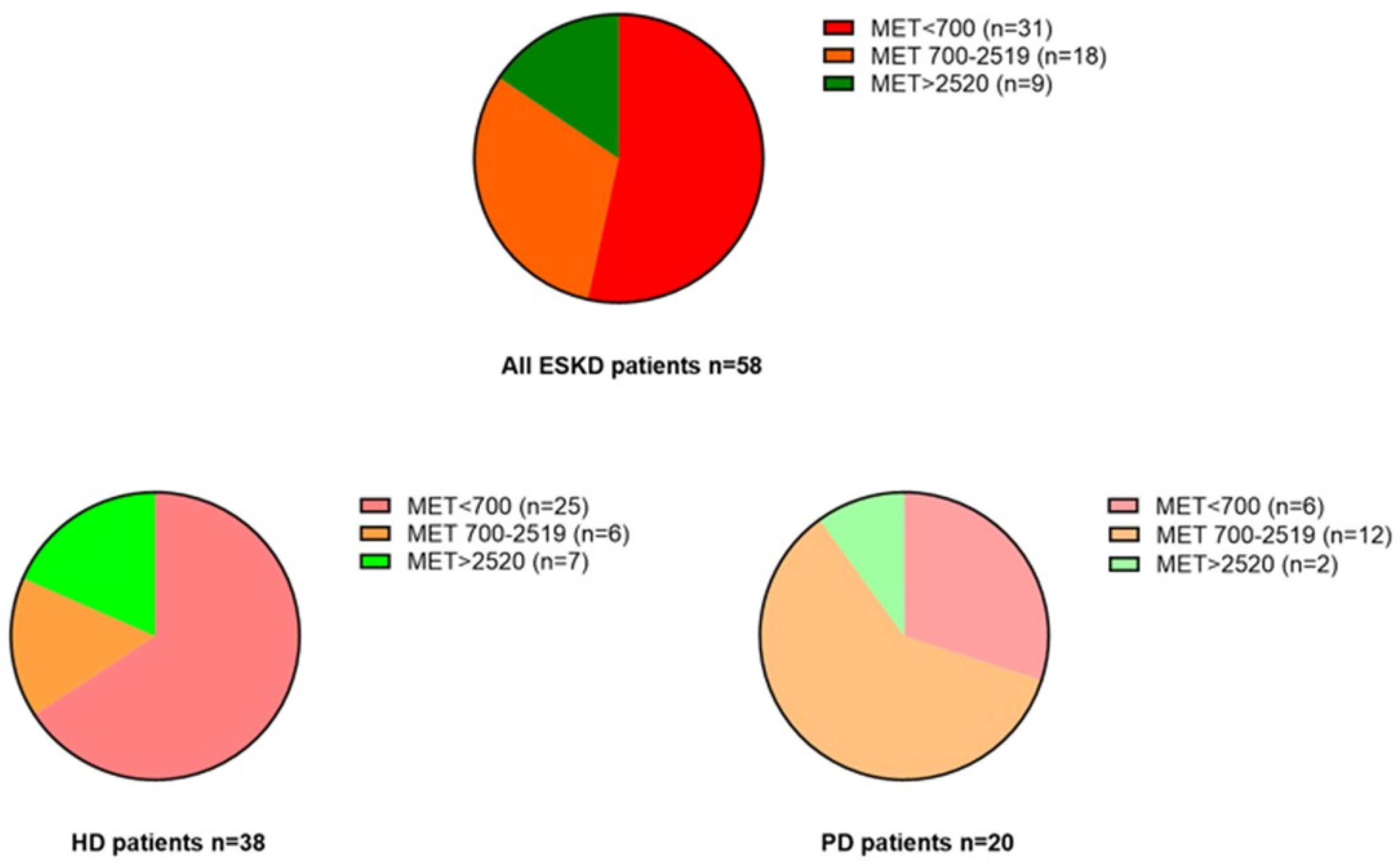
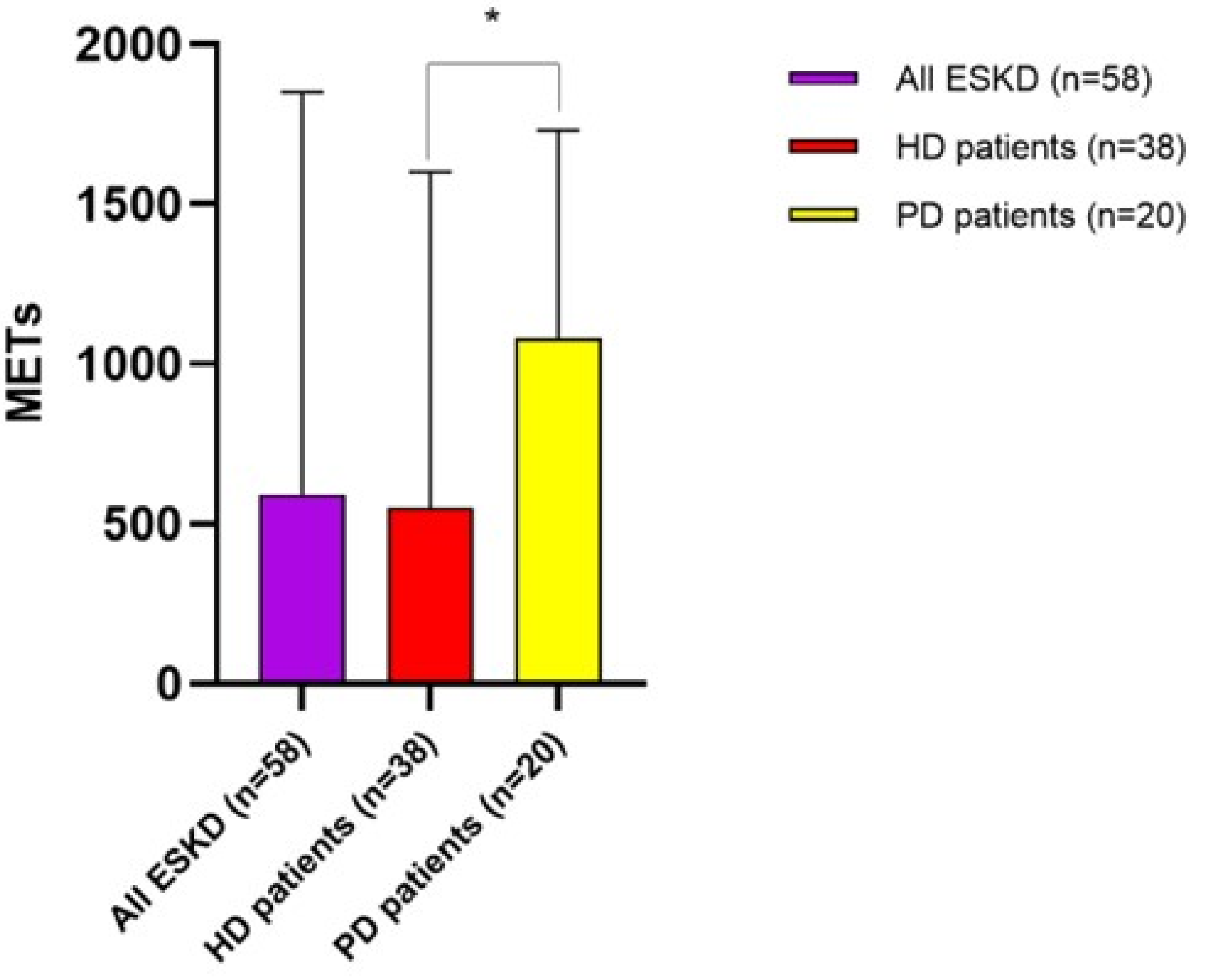
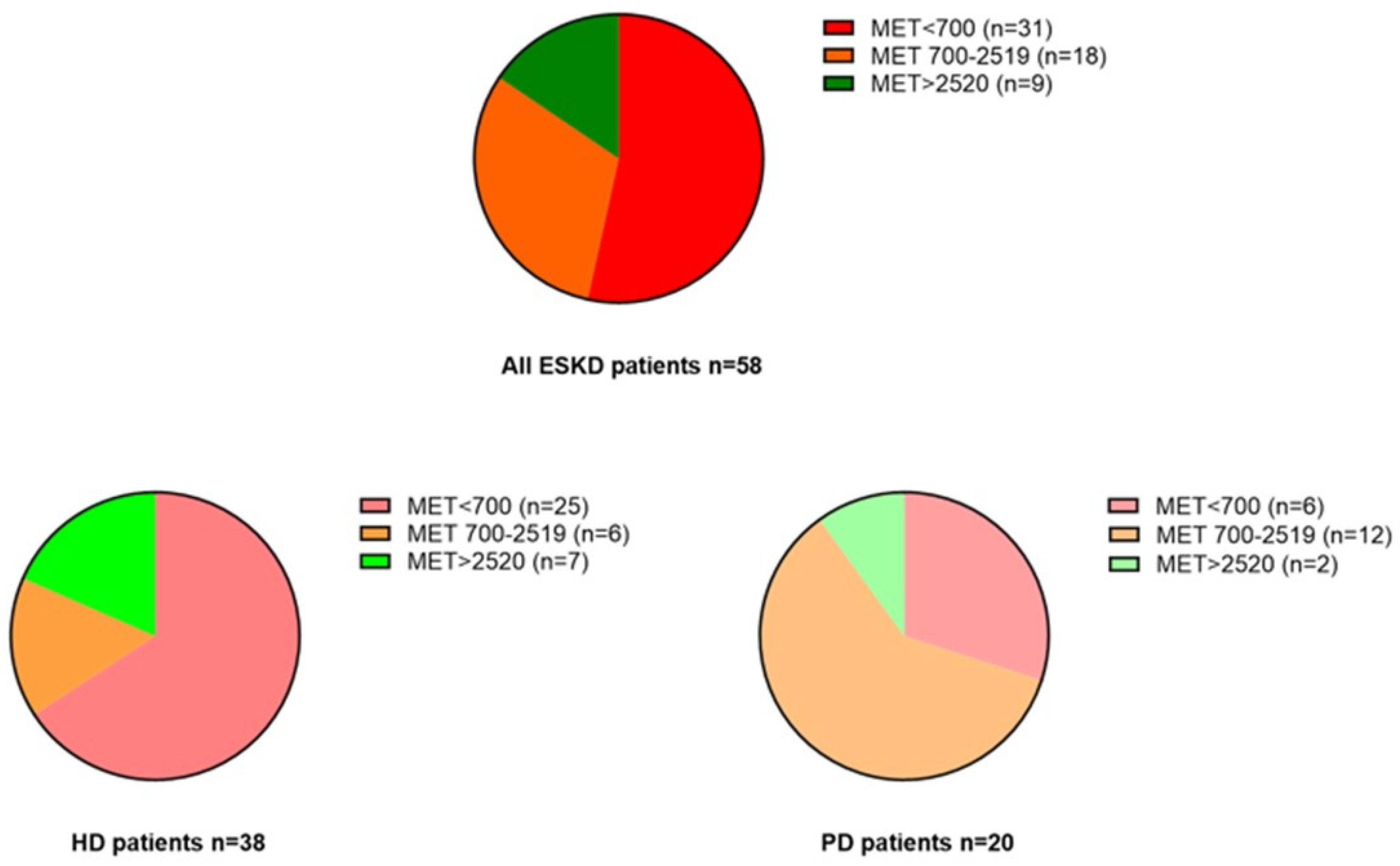
3.2. Self-Reported Degree of Physical Activity in the Study Population
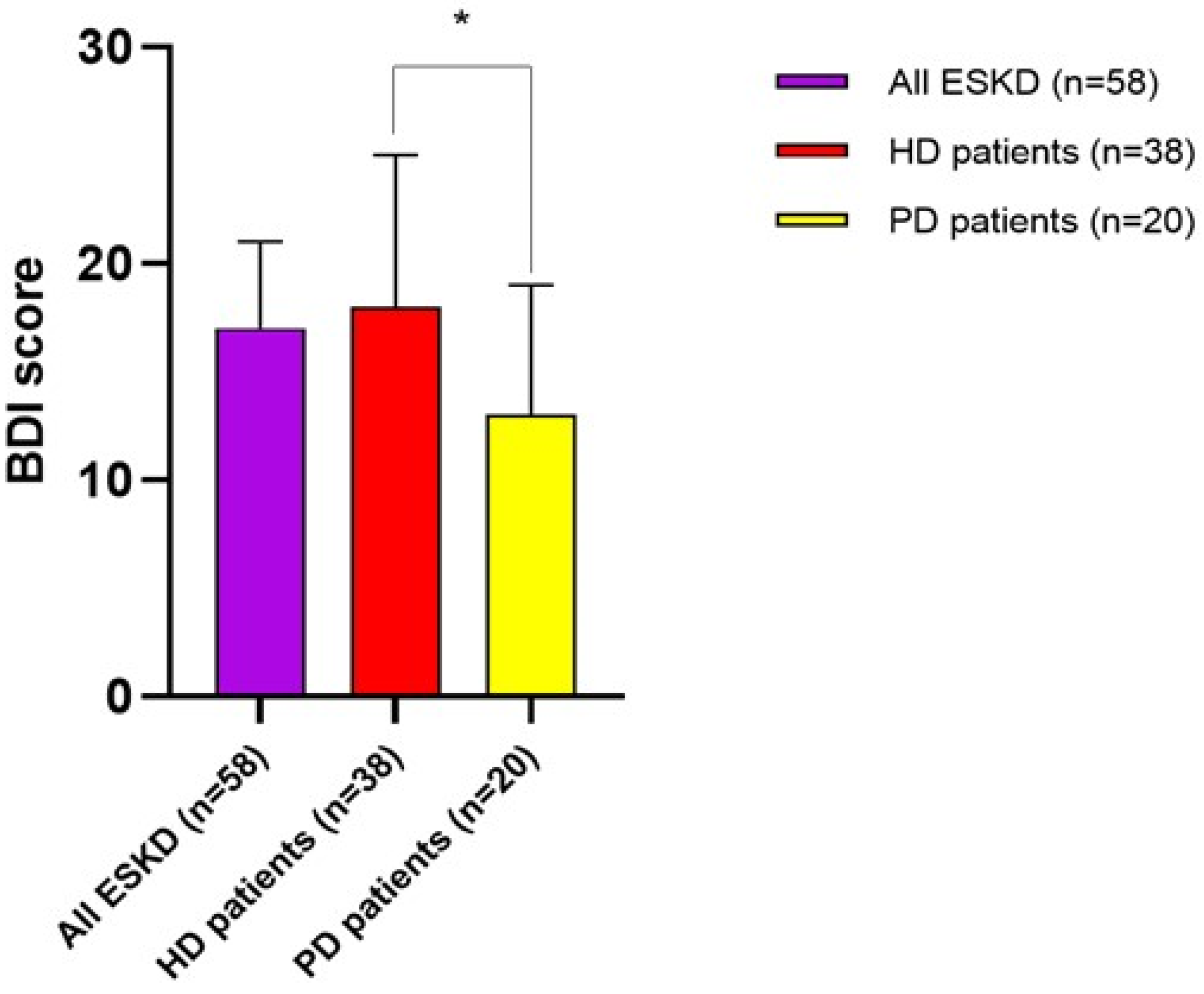
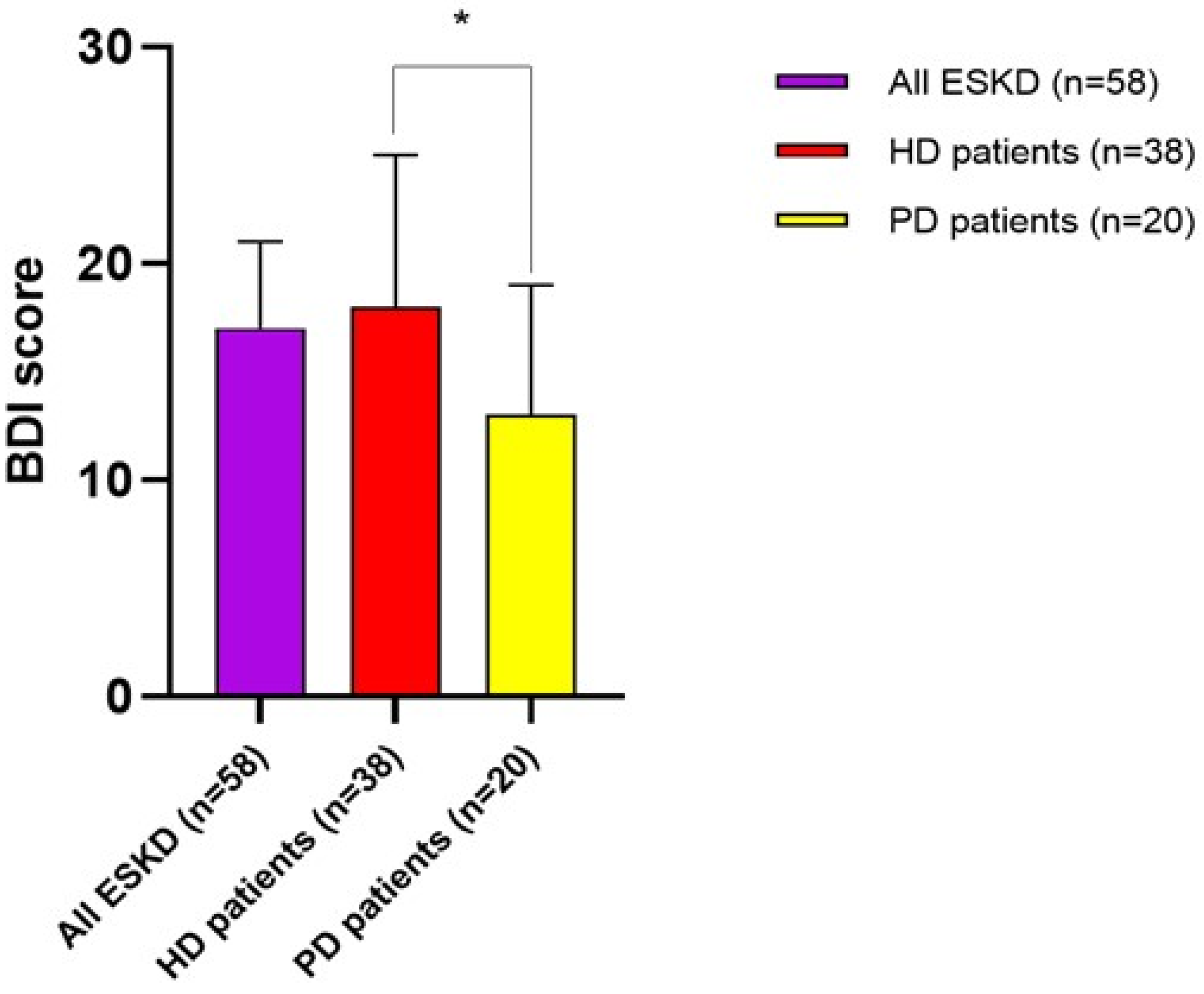
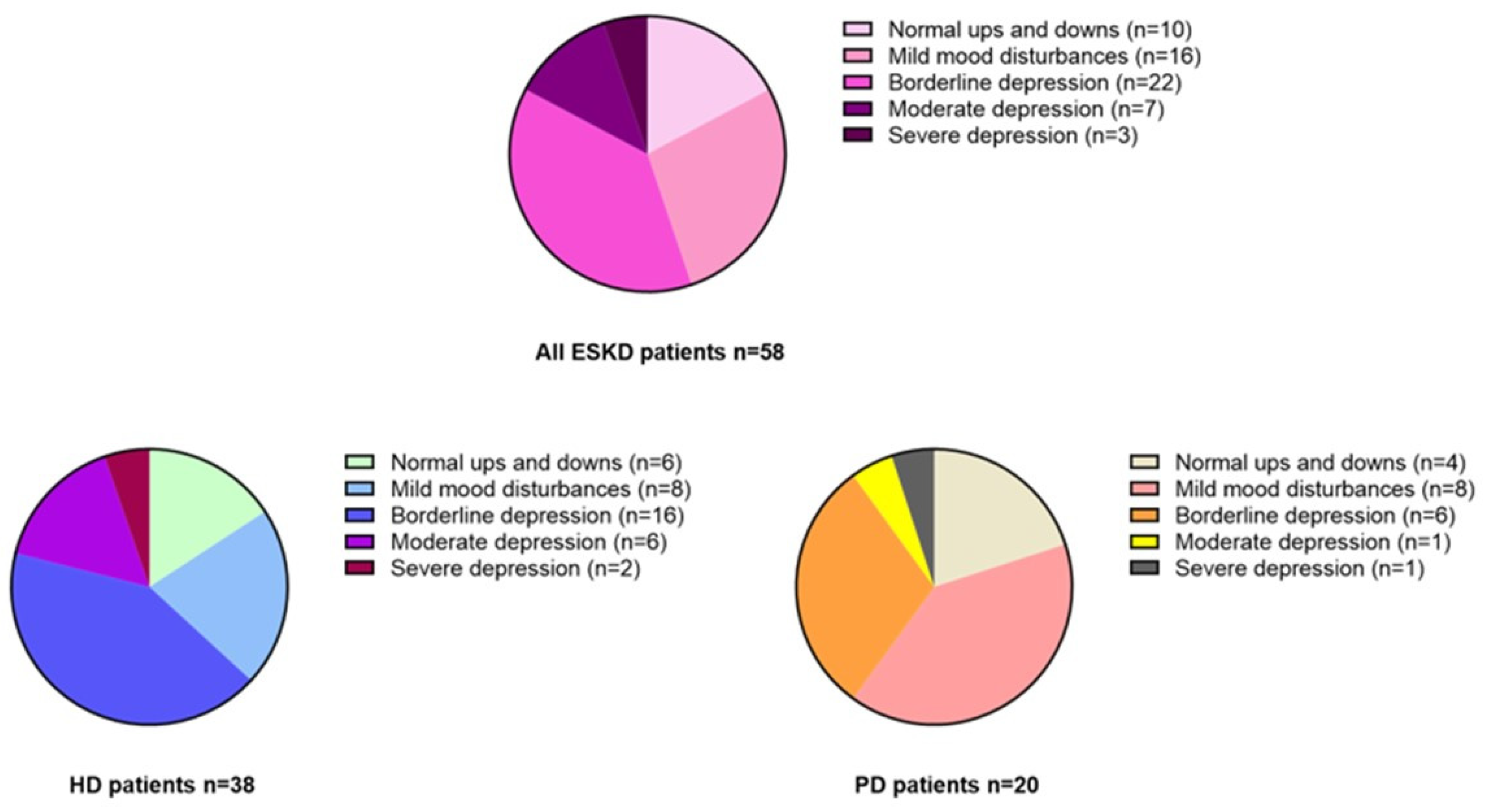
3.3. Self-Reported Degree of Mood Disturbances in the Study Population
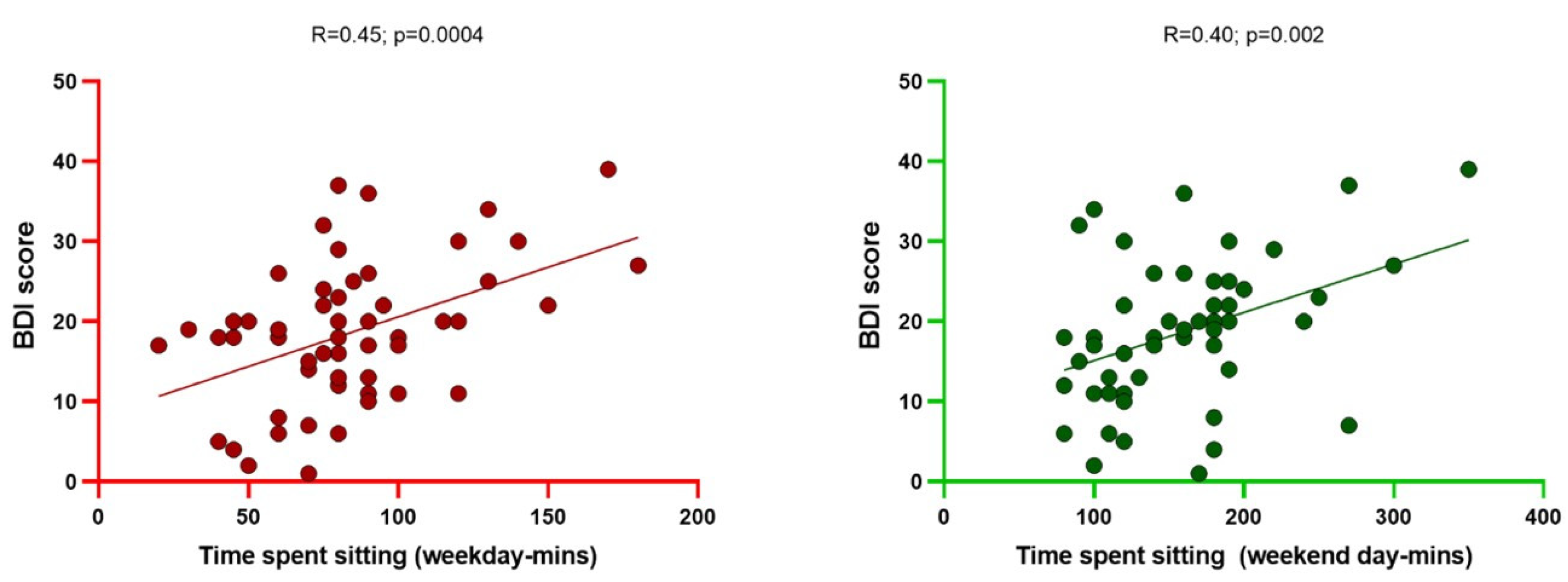
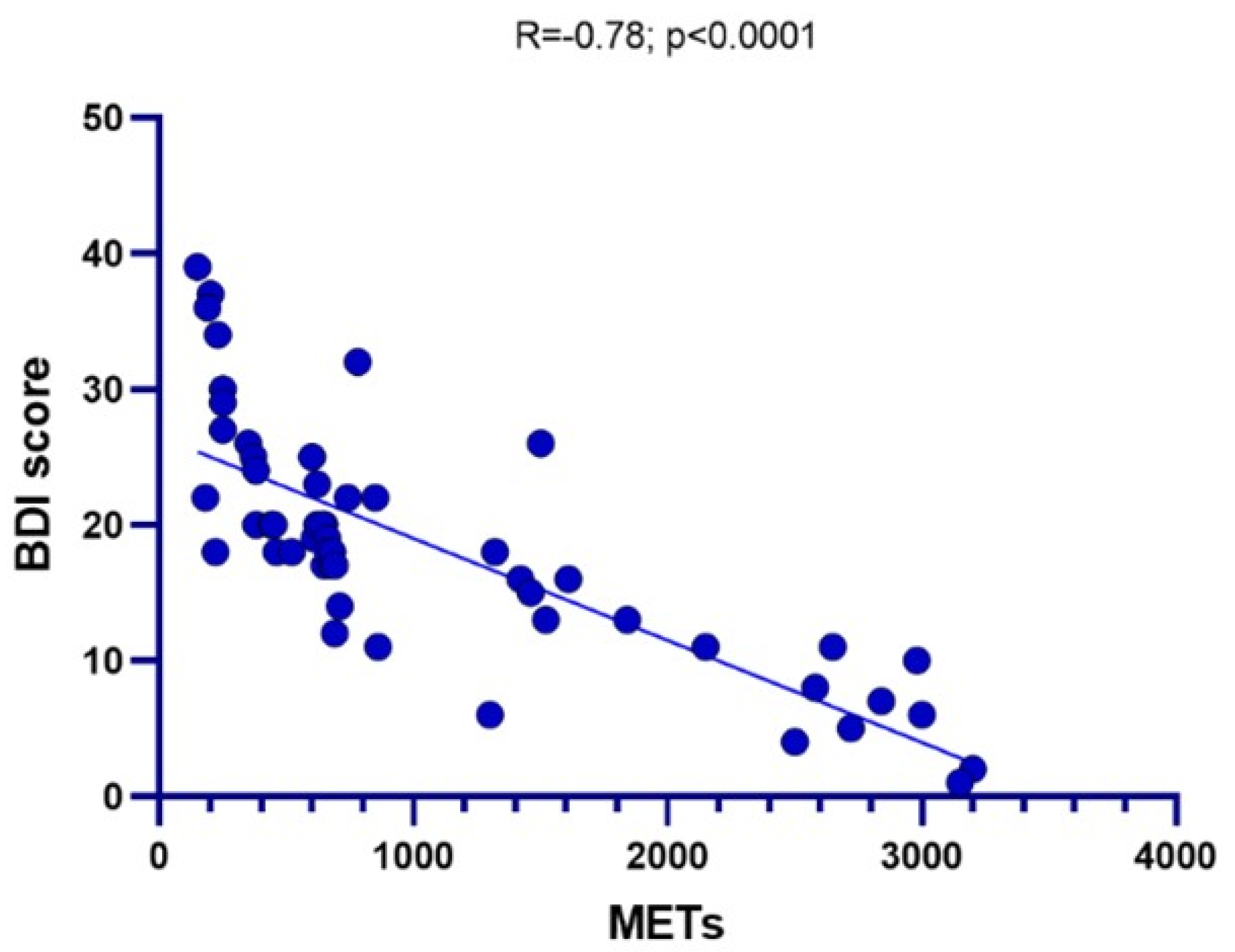
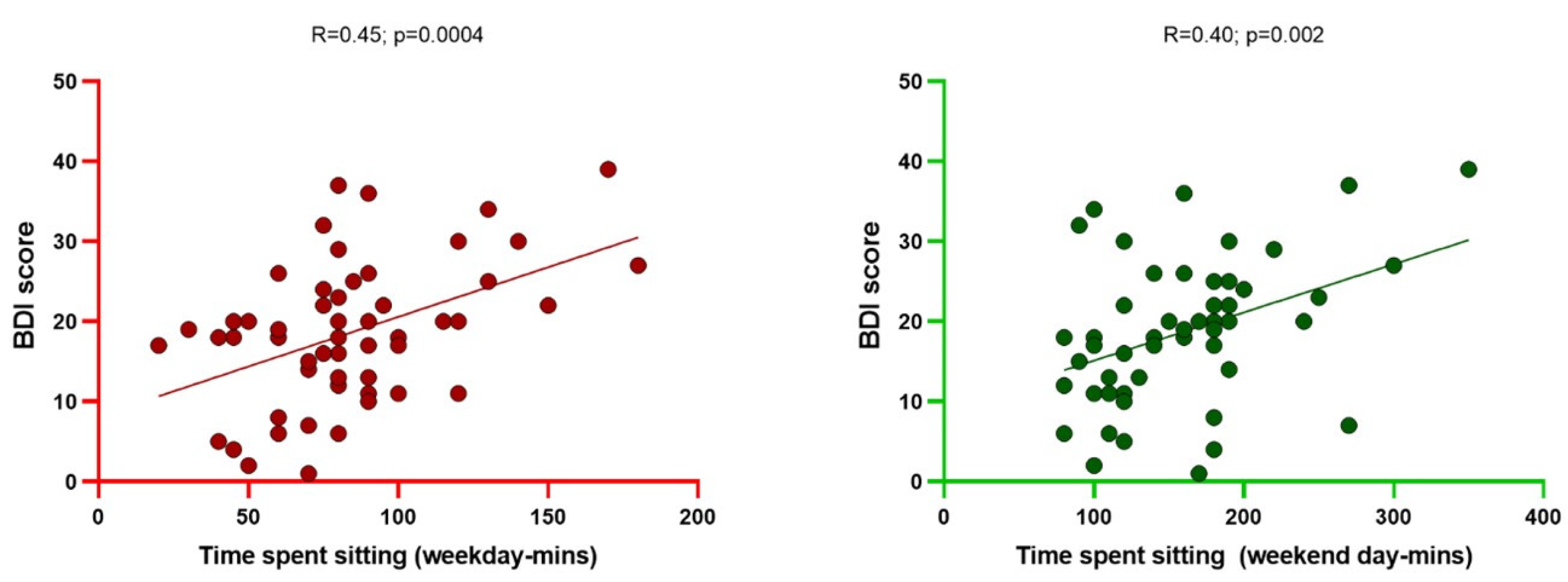
3.4. Correlates of Physical Activity and Severity of Mood Disturbances
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aparicio, M.; Cano, N.; Chauveau, P.; Azar, R.; Canaud, B.; Flory, A.; Laville, M.; Leverve, X. Nutritional status of haemodialysis patients: A French national cooperative study. French Study Group for Nutrition in Dialysis. Nephrol Dial Transpl. 1999, 14, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.C.; Huang, S.H.; Kao, C.L.; Hsu, P.C. Muscle Wasting in Chronic Kidney Disease: Mechanism and Clinical Implications-A Narrative Review. Int. J. Mol. Sci. 2022, 23, 6047. [Google Scholar] [CrossRef] [PubMed]
- Dziubek, W.; Bulinska, K.; Kusztal, M.; Kowalska, J.; Rogowski, L.; Zembron-Lacny, A.; Golebiowski, T.; Ochmann, B.; Pawlaczyk, W.; Klinger, M.; et al. Evaluation of Exercise Tolerance in Dialysis Patients Performing Tai Chi Training: Preliminary Study. Evid. Based Complement. Altern. Med. 2016, 2016, 5672580. [Google Scholar] [CrossRef] [PubMed]
- King-Wing Ma, T.; Kam-Tao Li, P. Depression in dialysis patients. Nephrology 2016, 21, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Ritchie, M.; Andrews, E. Exercise in Individuals With CKD: A Focus Group Study Exploring Patient Attitudes, Motivations, and Barriers to Exercise. Kidney Med. 2019, 1, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Chertow, G.M.; Ng, A.V.; Mulligan, K.; Carey, S.; Schoenfeld, P.Y.; Kent-Braun, J.A. Physical activity levels in patients on hemodialysis and healthy sedentary controls. Kidney Int. 2000, 57, 2564–2570. [Google Scholar] [CrossRef] [PubMed]
- Bakker, E.A.; Zoccali, C.; Dekker, F.W.; Eijsvogels, T.M.H.; Jager, K.J. Assessing physical activity and function in patients with chronic kidney disease: A narrative review. Clin. Kidney J. 2021, 14, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.J.; Johansen, K.L. Are dialysis patients too frail to exercise? Semin. Dial. 2019, 32, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Kirkman, D.L.; Bohmke, N.; Carbone, S.; Garten, R.S.; Rodriguez-Miguelez, P.; Franco, R.L.; Kidd, J.M.; Abbate, A. Exercise intolerance in kidney diseases: Physiological contributors and therapeutic strategies. Am. J. Physiol. Ren. Physiol. 2021, 320, F161–F173. [Google Scholar] [CrossRef] [PubMed]
- Cobo, G.; Gallar, P.; Gama-Axelsson, T.; Di Gioia, C.; Qureshi, A.R.; Camacho, R.; Vigil, A.; Heimburger, O.; Ortega, O.; Rodriguez, I.; et al. Clinical determinants of reduced physical activity in hemodialysis and peritoneal dialysis patients. J. Nephrol. 2015, 28, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Albuhayri, A.H.; Alshaman, A.R.; Alanazi, M.N.; Aljuaid, R.M.; Albalawi, R.I.M.; Albalawi, S.S.; Alsharif, M.O.; Alharthi, N.M.; Prabahar, K. A cross-sectional study on assessing depression among hemodialysis patients. J. Adv. Pharm. Technol. Res. 2022, 13, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, B.M. Peritoneal Dialysis or Haemodialysis for Kidney Failure? J. Nepal. Med. Assoc. 2018, 56, 556–557. [Google Scholar] [CrossRef]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Tucker, W.J.; Fegers-Wustrow, I.; Halle, M.; Haykowsky, M.J.; Chung, E.H.; Kovacic, J.C. Exercise for Primary and Secondary Prevention of Cardiovascular Disease: JACC Focus Seminar 1/4. J. Am. Coll. Cardiol. 2022, 80, 1091–1106. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Kim, J.C.; Li, Y.; Shapiro, B.B.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Martin, D.; Kalantar-Zadeh, K.; et al. Relation between anxiety, depression, and physical activity and performance in maintenance hemodialysis patients. J. Ren. Nutr. 2014, 24, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.A.; March, D.S.; Wilkinson, T.J.; Billany, R.E.; Bishop, N.C.; Castle, E.M.; Chilcot, J.; Davies, M.D.; Graham-Brown, M.P.M.; Greenwood, S.A.; et al. Clinical practice guideline exercise and lifestyle in chronic kidney disease. BMC Nephrol. 2022, 23, 75. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Simeoni, M.; Rizza, P.; Caroleo, M.; Capria, M.; Mazzitello, G.; Sacco, T.; Mazzuca, E.; Panzino, M.T.; Cerantonio, A.; et al. Quality of life, clinical outcome, personality and coping in chronic hemodialysis patients. Ren. Fail. 2017, 39, 45–53. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All ESKD (n = 58) | HD Patients (n = 38) | PD Patients (n = 20) | p for Difference | |
|---|---|---|---|---|
| Age (yrs) | 64.5 ± 12.3 | 66.2 ± 8.8 | 63.1 ± 10.6 | 0.17 |
| Gender (% male) | 62 | 63.1 | 60 | 0.81 |
| Dry weight (kg) | 62.1 ± 12.3 | 65.1 ± 9.9 | 61.8 ± 13.1 | 0.65 |
| BMI (Kg/m) | 24 ± 4.3 | 23 ± 3.3 | 24.8 ± 4.6 | 0.27 |
| Dialysis vintage (mo.) | 36 [9–46] | 40 [9–68] | 31 [8–33] | 0.09 |
| Diabetes (%) | 35 | 26.3 | 50 | 0.07 |
| Hypertension (%) | 72.4 | 73.6 | 70 | 0.76 |
| Cerebrovascular disease (%) | 8.6 | 10.5 | 5 | 0.47 |
| Ischemic cardiac disease (%) | 46.5 | 47.3 | 40 | 0.59 |
| Heart failure (%) | 22.4 | 26.1 | 15 | 0.32 |
| Peripheral vascular disease (%) | 5.1 | 5.2 | 5 | 0.96 |
| Serum phosphate (mg/dL) | 5.01 ± 0.86 | 4.89 ± 0.91 | 5.12 ± 0.66 | 0.20 |
| Serum calcium (mg/dL) | 9.1 ± 0.77 | 9.36 ± 0.55 | 8.81 ± 0.87 | 0.18 |
| Serum potassium (mg/dL) | 4.81 ± 0.54 | 4.59 ± 0.78 | 5.33 ± 0.81 | 0.07 |
| Serum sodium (mg/dL) | 139.3 ± 3.2 | 140.6 ± 7.5 | 138.8 ± 8.7 | 0.54 |
| Parathormone (pg/mL) | 236.9 [147.8–505.6] | 296.3 [87.6–303.6] | 188.4 [50.8–205.3] | 0.66 |
| Albumin (g/dL) | 3.99 ± 0.79 | 3.66 ± 0.98 | 4.12 ± 0.86 | 0.32 |
| Total cholesterol (mg/dL) | 160.1 ± 41.3 | 164.5 ± 62.5 | 160.5 ± 38.3 | 0.40 |
| Triglycerides (mg/dL) | 139.3 ± 68.9 | 144.1 ± 70 | 138.5 ± 45.2 | 0.21 |
| Creatinine (mg/dL) | 9.2 [8.6–12.2] | 8.6 ± 4.2 | 10.1 [5.5–11.3] | 0.47 |
| Hematocrit (%) | 35.2 ± 6.1 | 34.2 ± 5.9 | 37.1 ± 5.8 | 0.32 |
| Hemoglobin (g/dL) | 11.0 ± 0.7 | 10.9 ± 0.6 | 11.0 ± 0.7 | 0.89 |
| Ferritin (mg/dL) | 203.1 [65.4–312.5] | 233.6 [195.1–310.2] | 188.1 [44.8–195.5] | 0.23 |
| Serum iron (mg/dL) | 60.2 [31.5–92.8] | 59.1 [38.8–66.6] | 61.3 [48.2–80.3] | 0.31 |
| Urea (mg/dL) | 144.8 ± 38.3 | 148.3 ± 40.1 | 141.1 ± 38.1 | 0.08 |
| Activity Indicators | Total | HD | PD | p |
|---|---|---|---|---|
| METs intense activity | 0 | 0 | 0 | - |
| METs moderate activity | 640 ± 190 | 420 ± 180 | 810 ± 240 | 0.001 |
| METs walking | 260 ± 80 | 180 ± 90 | 320 ± 100 | 0.01 |
| Total METs | 590 [460–1850] | 550 [250–1600] | 1080 [750–1730] | 0.003 |
| Sitting time weekday (min) | 90 ± 25 | 95 ± 40 | 88 ± 40 | 0.17 |
| Sitting time weekend day (min) | 190 ± 90 | 200 ± 80 | 190 ± 70 | 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musolino, M.; Presta, P.; Cianfrone, P.; Errante, M.A.; Andreucci, M.; Coppolino, G.; Bolignano, D. Self-Reported Physical Inactivity and Mood Disturbances in End-Stage Kidney Disease (ESKD) Patients on Chronic Dialysis Treatment. J. Clin. Med. 2023, 12, 7160. https://doi.org/10.3390/jcm12227160
Musolino M, Presta P, Cianfrone P, Errante MA, Andreucci M, Coppolino G, Bolignano D. Self-Reported Physical Inactivity and Mood Disturbances in End-Stage Kidney Disease (ESKD) Patients on Chronic Dialysis Treatment. Journal of Clinical Medicine. 2023; 12(22):7160. https://doi.org/10.3390/jcm12227160
Chicago/Turabian StyleMusolino, Michela, Pierangela Presta, Paola Cianfrone, Maria Antonietta Errante, Michele Andreucci, Giuseppe Coppolino, and Davide Bolignano. 2023. "Self-Reported Physical Inactivity and Mood Disturbances in End-Stage Kidney Disease (ESKD) Patients on Chronic Dialysis Treatment" Journal of Clinical Medicine 12, no. 22: 7160. https://doi.org/10.3390/jcm12227160
APA StyleMusolino, M., Presta, P., Cianfrone, P., Errante, M. A., Andreucci, M., Coppolino, G., & Bolignano, D. (2023). Self-Reported Physical Inactivity and Mood Disturbances in End-Stage Kidney Disease (ESKD) Patients on Chronic Dialysis Treatment. Journal of Clinical Medicine, 12(22), 7160. https://doi.org/10.3390/jcm12227160