

Osseodensification: An Alternative to Conventional Osteotomy in Implant Site Preparation: A Systematic Review

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Extracting Sample Data
2.2. Study Quality and Risk of Bias
2.3. Sample Characteristics for Study Quality
3. Results
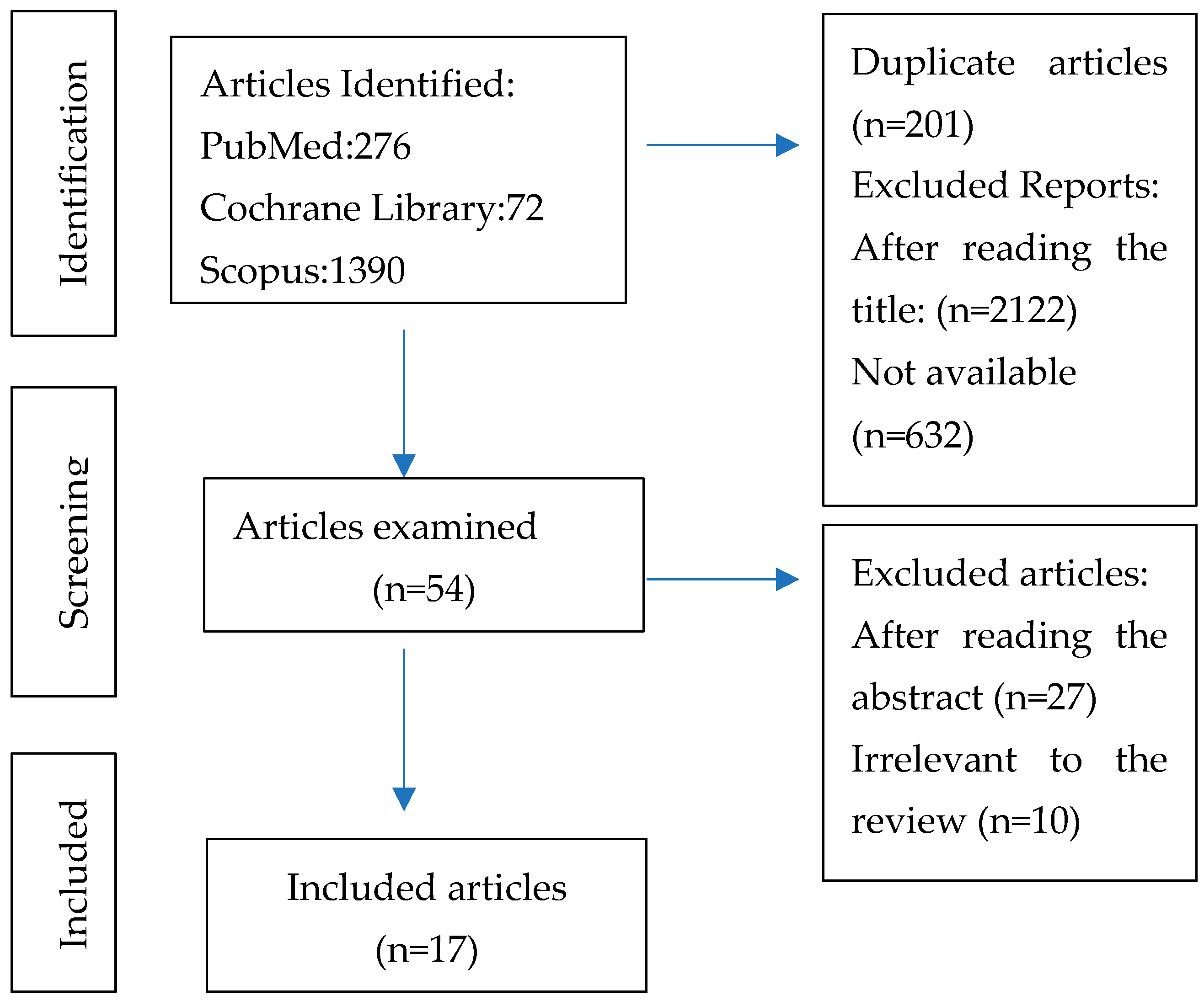
3.1. Search Results
3.2. Characteristics of the Included Studies

{kind=link}
| Authors | Study Design | Inclusion Criteria | Exclusion Criteria | Study Aim | Study Group | Study Duration | No. Implants | Osteotomy Sequence | Anatomical Zone | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Lahens et al. [21], 2016 | Experimental study | NR | NR | To investigate the effect of osseodensification on the initial stability and early osseointegration of implants in low-density bone. | Sheep | NR | 30 | Group SD: Pilot drill 2.0 mm; Twist drill 3.2 mm; Twist drill 3.8 mm. Group OD with Densah® burs: CW and CCW Pilot drill 2.0 mm; Drill 2.8 mm; Drill 3.8 mm. | Iliac bone | The OD technique showed greater primary stability and greater bone density around the implants compared to the SD technique. Statistical analysis showed that the osseodensification technique promoted a significant increase in the primary stability of the implants (p < 0.05). The OD technique showed a higher BIC compared to the SD technique (p < 0.05) (±70% and ±50%, respectively). No statistically significant difference in BAFO compared to traditional osteotomy technique (p = 0.22); cylindrical implant showed statistically high levels of BAFO compared to conical implants (p = 0001). |
| Trisi et al. [18], 2016 | Experimental study | NR | NR | To evaluate a new surgical technique for preparing the implant bed that would improve bone density, ridge width, and secondary implant stability. | Sheep | 2 months | 20 | Group SD: Drilling sequence recommended by the manufacturer. Group OD with Densah® burs: Pilot drill 2.0 mm; Drill 2.8 mm; Drill 3.8 mm. | Iliac crest | The OD technique (test group) showed greater primary stability than the SD technique (control group). There was no statistically significant difference in % BIC between the control and test groups (46.19 ± 3.98 vs. 49.58 ± 3.19; p > 0.05). Analysis of % BV revealed an increase in bone density of approximately 30 per cent in the test group compared to the control group (37.63 ± 4.25 vs. 28.28 ± 4.74; p < 0.05). The test group showed significantly better biomechanical performance (around 30 to 40 per cent higher) than the control group in the parameters assessed, such as RTV (172.70 ± 16.07 vs. 126.63 ± 9.52, p < 0.05) and VAM (60.45 ± 5.29 vs. 94.88 ± 10.94, p < 0.05). |
| Huwais and Meyer. [8], 2017 | Experimental study | NR | NR | To study the hypothesis that the OD technique would increase primary stability, bone density, and % BIC. | Pigs | NR | 72 | Group SD: Pilot drill 1.7 mm; Drill 2.2 mm; Drill 3.2 mm; Drill 4.2 mm; Drill 5.2 mm. Group ED: Tapered, multi-fluted bur design. OD group: Pilot drill 1.7 mm; Drill 2.8 mm; Drill 3.8 mm; Drill 4.8 mm; Drill 5.8 mm. | Tibial plateau bone samples | The OD technique showed greater primary stability, bone density, and % BIC compared to the SD and ED techniques. The % BIC was increased by approximately three times for osteotomies prepared with OD compared to SD and ED. |
| Lopez et al. [22], 2017 | Experimental study | NR | NR | To investigate the effectiveness of OD in improving the fixation of spinal surgical material. | Sheep | 6 Weeks | 36 | Group SD (left-sided vertebral body): Pilot drill 2.0 mm; Drill 3.2 mm; Drill 3.8 mm. Group OD (right-sided vertebral body): Densah® burs Drill 2.8 mm Drill 3.8 mm | C2, C3, and C4 vertebral bodies | Pullout strength demonstrated that osseodensification drilling provided superior anchoring when compared to the SD group collapsed over time with statistical significance (p < 0.01). % BIC analysis demonstrated an OD group with significantly higher values relative to the SD group (p < 0.01). % BAFO presented significantly higher values for the OD group compared to the SD group (p = 0.024). |
| Huwais et al. [16], 2018 | Multicenter retrospective clinical study | Atrophic partially edentulous posterior maxilla requiring dental implant placement. All patients had crestal sinus augmentation utilising OD and implant placement. Routine: A minimum subsinus vertical bone height of 2 mm. Patients with a minimum of 6 months follow-up from time of augmentation | Sinus pathology that precludes routine sinus augmentation, such as acute sinusitis, history of previous sinus surgery, and bisphosphonate or chronic steroid medications. | To evaluate the effectiveness and predictability of the osseous densification instrumentation method and its ability to facilitate transcrestal sinus elevation with simultaneous implant placement. | 115 women,107 men | May 2012 and September 2017 | 261 | Densah® drills: Pilot drill 1.7 mm; 3.0 mm drill. | Posterior maxilla | The baseline subsinus residual bone height was 5.4 mm (range: 2–10 mm). Sinus graft augmentation procedure achieved a significant vertical increase of 7 mm (SD: 2.49; p < 0.05). No sinus complications were found, such as membrane perforations, and late implant failure was observed in the follow-up period from 6 to 64 months. The cumulative implant survival rate was 97%. |
| Alifarag et al. [19], 2018 | Experimental study | NR | NR | To investigate the effects of OD drilling techniques on implant stability and osseointegration using TM and TSV implants in low-density bone. | Sheep | NR | 72:36 TM; 36 TSV. | Group SD: Drill 2.0 mm; Drill 2.8 mm; Drill 3.4 mm. Group OD with Densah® burs: Pilot drill 1.7 mm; Drill 2.8 mm; Drill 3.8 mm. | Ilia | TM implants yielded a significantly lower IT (Ncm) relative to the TSV implants (p = 0.002). No statistically significant differences across surgical techniques within the TM group despite higher mean values were observed for the OD (CCW and CW) techniques relative to SD. The IT as a function of drilling technique showed implants subjected to SD drilling yielded a significantly lower IT relative to samples implanted in OD (CW/CCW) sites (p < 0.05). Histomorphometric analysis showed that OD presented significantly greater values of BIC and BAFO (p < 0.05). |
| Slete et al. [2], 2018 | Experimental study | NR | NR | To compare the histomorphometric structure of SD, SO, and a new osteotomy method without bone removal called OD. | Pigs | NR | 18 | Group SD: Pilot drill 1.7 mm; Manufacturer’s sequence for the appropriate implant size (4.7 mm). Group SO: Pilot drill 1.7 mm; Instrumentation sizes I, II, and III of the set. Group OD with Densah® burs: Pilot drill 1.7 mm; Drill 2.5 mm; Drill 3.5 mm; Drill 4.5 mm. | Tibia | OD preparation produced 60.3% of BIC, SO 40.7%, and SD 16.3% of implant perimeter in contact with bone. % BV within 2 mm of implant produced was 62% for OD, 49% for SO. and 54% for SD (compared to SO (40.7%) and SD (16.3%)), with a statistically significant value (p < 0.05). |
| Oliveira et al. [7], 2018 | Experimental study | NR | NR | To investigate the effect of OD on the primary stability and osseointegration of machined and acid-etched implants in low-density bone. | Goats | 6 Weeks | 60 | Group SD: Pilot drill 2.0 mm; Drill 3.2 mm; Drill 3.8 mm. Group OD with Densah® burs CW and CCW: Pilot drill 2.0 mm; Drill 2.8 mm; Drill 3.8 mm. | Iliac bone | The IT values were approximately 10 Ncm for the SD technique and showed subsequent increases for CW (~53 Ncm) and CCW (~78 Ncm), with statistically significant data as a result of the technique (CCW > CW > SD, p < 0.005), regardless of implant surface. % BIC as a function of time (3 vs. 6 weeks); no statistical significance was noted (p = 0.577). % BAFO values showed a significant increase in values from 3 to 6 weeks in vivo (p = 0.014). Results demonstrated that BIC values for the CCW and CW groups were comparable to all acid-etched implant drilling groups, while the SD drilling for machined groups resulted in significantly lower % BIC values (p < 0.01). No significant differences were depicted between acid-etched and machined surfaces when % BAFO values collapsed over time and drilling technique was assessed (p = 0.053). Regardless of implant surface, insertion torque significantly increased when OD drilling was used in low-density bone. |
| Mello-Machado et al. [15], 2018 | Case report | NR | NR | To observe whether the clinical and radiographic results obtained could support the hypothesis of gaining primary stability, as well as whether a compaction graft can be achieved using this technique. | Humans | NR | 1 | Densah® burs Pilot drill 1.7 mm; Drill 2.3 mm; Drill 3.0 mm; Drill 3.3 mm. | Maxilla | The OD served to increase primary stability and enhance BIC. The implant was adequately placed and with a sufficient stability, reflected in the ISQ (≥70), which is an indicator of an immediate provisional protocol. |
| Witek et al. [20], 2019 | Case report | NR | NR | To qualitatively and quantitatively evaluate the effect of osteotomy preparation by conventional (control group) or OD (OD group) instrumentation on osteotomy healing. | Sheep | NR | 15 | Group SD: Pilot drill 2, 3.2, and 3.8 mm twist drills. Group OD Densah® Burs OD-CW: Pilot drill 2.0, 2.8 and 3.8 mm multi-fluted tapered burs. OD-CCW: Pilot drill 2.0, 2.8, and 3.8 mm multi-fluted tapered burs. | Left ilium | The mean % BAFO for SD instrumentation was ~11.5%, while both OD techniques (OD-CW and OD-CCW) resulted in statistically homogeneous values: 11.3% and 9.1%, respectively (p = 0.78). BAFO values confirmed that there were no healing differences when utilising different instrumentations. |
| Tian et al. [23], 2019 | Experimental study | NR | NR | Comparing the osseointegration of implants placed in atrophic mandibular alveolar ridges with the alveolar ridge expansion surgical protocol. | Pigs | 12 + 4 Weeks | 12 | Conventional osteotomes Densah® Burs | Atrophic jaw | The mean % BIC value was approximately 62.5% in the osseodensification group and 31.4% in the regular instrumentation group. Statistical analysis showed a significant effect of the drilling technique (p = 0.018). There was no statistical difference in BAFO as a function of drilling technique (p = 0.198). |
| da Rosa et al. [13], 2019 | Case report | NR | NR | To describe whether the combined use of IDR and osteotomy through the RE can improve the primary stability of the immediate implant in periodontally compromised extraction sites. | Humans | 2 years | 2 | NR | Maxilla | The combination of the IDR technique with the osseodensification implant site preparation method allowed for an increase in implant primary stability, as demonstrated by the higher insertion torque achieved. |
| Lahens et al. [24], 2019 | Experimental study | NR | NR | To investigate the effects of OD osteotomy on the stability and osseointegration of implants in low-density bone. | Sheep | 12 Weeks | 72 | Group SD: Pilot drill 2.0 mm; Twist drill 3.2 mm; Twist drill 3.8 mm. Group OD Densah® Burs (CW and CCW): Pilot drill 2.0 mm; Drill 2.8 mm; Drill 3.8 mm. | Iliac Crest | OD insertion torque was higher in the CCW and CW drilling compared to the SD (p < 0.001). BIC was significantly higher for CW (p = 0.024) and CCW drilling (p = 0.006) compared to the SD technique. BIC values were significantly lower for the SD surgical technique relative to the CCW and CW surgical techniques (p < 0.024). The acid-etched surface treatment yielded a significantly higher % BIC than the machine-cut implants (p < 0.001). No statistical difference in the BIC as a function of time between the 3-week and 12-week time points (p > 0.5). Osseodensification drilling techniques (CW and CCW) yielded significantly higher % BAFO than the SD technique for the acid-etched implants (p < 0.01), while in the machine cut implant, the CCW drilling technique yielded a significantly higher BAFO than the SD technique (p < 0.01). In low-density bone, OD drilling presented higher stability and no osseointegration impairments compared to the SD technique, regardless of evaluation time or implant surface. |
| Jarikian et al. [6], 2021 | Randomised controlled clinical trial | Good oral hygiene; presence of an edentulous site with an initial width of the alveolar crest between 4 and 5 mm with a minimum of 2 mm of trabecular bone core between the cortical plates. | Uncontrolled systemic conditions or systemic disorders that could compromise osseointegration;consumption of medication that could affect bone metabolism. | To compare the ridge expansion obtained using two different techniques, the OD technique and TET. | Humans | NR | 40 | TET Group: Pilot drill 1.7 mm; Expander 2.5 mm; Expander 3.1 mm; Expander 3.6 mm. Group OD: Densah® Burs Pilot drill 1.7 mm; Drill 2.0 mm; Drill 2.3 mm; Drill 3.3 mm; Drill 3.5 mm. | Alveolar bone | Both techniques were useful in achieving expansion, and all implants placed were successful. The amount of achieved expansion was significantly higher in the OD group, where the average expansion was 2.36 mm (2.36 ± 0.31, p < 0.05), while the average amount of expansion in the threaded expanders group was 1.5 mm (1.5 ± 0.28, p < 0.05). The Densah bur drilling was superior to manually threaded expanders. |
| Salgar et al. [17], 2021 | Case report | Healthy, non-smoking individuals; requires maxillary sinus augmentation;maximum residual bone height of 1.5 mm. | NR | Presentation of a minimally invasive technique that facilitates bone graft augmentation of the maxillary sinus. | Humans | 4 months | 5 | Group OD: Densah® Burs Drill 3.0 mm; Drill 4.0 mm; Drill 5.0 mm; Drill 5.3 mm. | Maxilla | The vertical increase in sinus bone height ranged from 10.3 to 13.6 mm.The rise in bone height is comparable to that obtained with lateral window procedures. The osseodensified crestal sinus window technique may be proposed as a possible alternative procedure for the lateral sinus window technique for maxillary sinus bone augmentation. |
| Torroni et al. [25], 2021 | Case-controlled split model | NR | NR | Comparison of conventional instrumentation vs. OD osteotomy instrumentation in posterior lumbar fixation in an ovine model to determine the feasibility and potential advantages of the OD drilling technique in terms of mechanical and histomorphology outcomes. | Sheep | 6 to 12 months | 64 | Group SD: Pilot drill; Twist drill 4.0 mm. Group OD: Densah® Burs Drill 2.8 mm; Drill 3.8 mm. | Lumbar region (spinous processes of L2 to L5) | Considerable mechanical stability differences were observed between OD and SD groups at 6- (387 N vs. 292 N) and 12-week (312 N vs. 212 N) time points. The % BAFO did not yield any significant differences when evaluated as a function of the insertion technique (OD vs. SD (p = 0.457)) and time in vivo (p = 0.957) The histometric analysis showed no statistical differences in BAFO between SD and OD groups. Mechanical pullout testing demonstrated that OD drilling provided greater degrees of implant anchoring as a function of time, whereas a significant reduction was observed for the SD group. |
| Mello-Machado et al. [12], 2021 | Randomised controlled trial | Patients older than 18 years of age requiring oral rehabilitation of the upper jaw. | Insufficient bone for implant placement; lack of primary stability at implant insertion; metabolic diseases; impeded/ hampered hygiene motor difficulties; pregnancy; uncontrolled periodontal disease.; smoking habits, radio-therapy, and use of bisphosphonates. | To compare the stability of dental implants placed in low-quality bone prepared for the healing chamber with the osseodensification technique and a standard undersized drilling. | Humans | 7 months | 55 | Group SD: Pilot drill 2.0 mm; Drill 2.5 mm; Drill 2.8 mm. Group OD: Densah® Burs Pilot drill 1.6 mm; Drill 2.3 mm; Drill 3.0 mm; Drill 3.3 mm. | Upper jaw | The OD group showed higher IT (39.0 ± 6.4 Ncm) than the SD group (32.0 ± 3.4 Ncm) (p < 0.001). ISQ values were similar (p > 0.05) at the implant insertion (67.1 ± 3.2 and 65.5 ± 2.7, OD vs. SD, respectively). After six months of healing, implant survival was equally comparable in both groups (p > 0.05), and ISQ values were greater than those of implant insertion (p < 0.001) but similar (p > 0.05) for both groups (74.0 ± 3.6 and 73.3 ± 3.2 for OD and SD, respectively) OD instrumentation allowed for the bone-healing chamber concept in low-quality bone without any reduction in implant stability and success rate. |
4. Discussion
4.1. Insertion Torque and Primary Stability
4.2. Bone-to-Implant Contact (BIC) and Bone Area Fraction Occupancy (BAFO)
4.3. Osseointegration
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brånemark, P.I.; Adell, R.; Albrektsson, T.; Lekholm, U.; Lundkvist, S.; Rockler, B. Osseointegrated titanium fixtures in the treatment of edentulousness. Biomaterials 1983, 4, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Slete, F.B.; Olin, P.; Prasad, H. Histomorphometric comparison of 3 osteotomy techniques. Implant. Dent. 2018, 27, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.M. A Brief Historical Perspective on Dental Implants, Their Surface Coatings and Treatments. Open Dent. J. 2014, 8, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Adell, R.; Lekholm, U.; Rockler, B.; Brånemark, P.I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Branemark, P.; Hansson, H.; Lindstrom, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Jarikian, S.; Jaafo, M.-H.; Al-Nerabieah, Z. Clinical evaluation of two techniques for narrow alveolar ridge expansion: Clinical study. Int. J. Dent. Oral Sci. 2021, 8, 1047–1052. [Google Scholar] [CrossRef]
- Oliveira, P.G.F.P.; Bergamo, E.T.P.; Neiva, R.; Bonfante, E.A.; Witek, L.; Tovar, N.; Coelho, P.G. Osseodensification outperforms conventional implant subtractive instrumentation: A study in sheep. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 90, 300–307. [Google Scholar] [CrossRef]
- Huwais, S.; Meyer, E. A Novel Osseous Densification Approach in Implant Osteotomy Preparation to Increase Biomechanical Primary Stability, Bone Mineral Density, and Bone-to-Implant Contact. Int. J. Oral Maxillofac. Implant. 2017, 32, 27–36. [Google Scholar] [CrossRef]
- Al-Jetaily, S.; Al-dosari, A.A.F. Assessment of OsstellTM and Periotest® systems in measuring dental implant stability (in vitro study). Saudi Dent. J. 2011, 23, 17–21. [Google Scholar] [CrossRef]
- Kanathila, H.; Pangi, A. An insight into the concept of osseodensification-enhancing the implant stability and success. J. Clin. Diagnostic Res. 2018, 12, ZE01–ZE03. [Google Scholar] [CrossRef]
- Bertollo, N.; Robert, W. Drilling of Bone: Practicality, Limitations and Complications Associated with Surgical Drill-Bits. Biomech. Appl. 2011, 45–82. [Google Scholar] [CrossRef]
- Mello-Machado, R.C.; Mourão, C.F.d.A.B.; Javid, K.; Ferreira, H.T.; Montemezzi, P.; Calasans-Maia, M.D.; Senna, P.M. Clinical assessment of dental implants placed in low-quality bone sites prepared for the healing chamber with osseodensification concept: A double-blind, randomized clinical trial. Appl. Sci. 2021, 11, 640. [Google Scholar] [CrossRef]
- Rosa, J.C.M.; Rosa, A.C.P.O.; Huwais, S. Use of the Immediate Dentoalveolar Restoration Technique Combined with Osseodensification in Periodontally Compromised Extraction Sites. Int. J. Periodontics Restor. Dent. 2019, 39, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Mello-Machado, R.; da Gama, C.; Batista, S.; Rizzo, D.; Valiense, H.; Moreira, R. Tomographic and clinical findings, pre-, trans-, and post-operative, of osseodensification in immediate loading. Int. J. Growth Factors Stem Cells Dent. 2018, 1, 101. [Google Scholar] [CrossRef]
- Huwais, S.; Mazor, Z.; Ioannou, A.; Gluckman, H.; Neiva, R. A Multicenter Retrospective Clinical Study with Up-to-5-Year Follow-up Utilizing a Method that Enhances Bone Density and Allows for Transcrestal Sinus Augmentation through Compaction Grafting. Int. J. Oral Maxillofac. Implant. 2018, 33, 1305–1311. [Google Scholar] [CrossRef]
- Salgar, N. Osseodensified crestal sinus window augmentation: An alternative procedure to the lateral window technique. J. Oral Implantol. 2021, 47, 45–55. [Google Scholar] [CrossRef]
- Trisi, P.; Berardini, M.; Falco, A.; Podaliri Vulpiani, M. New osseodensification implant site preparation method to increase bone density in low-density bone: In vivo evaluation in sheep. Implant. Dent. 2016, 25, 24–31. [Google Scholar] [CrossRef]
- Alifarag, A.M.; Lopez, C.D.; Neiva, R.F.; Tovar, N.; Witek, L.; Coelho, P.G. Atemporal osseointegration: Early biomechanical stability through osseodensification. J. Orthop. Res. 2018, 36, 2516–2523. [Google Scholar] [CrossRef]
- Witek, L.; Neiva, R.; Alifarag, A.; Shahraki, F.; Sayah, G.; Tovar, N.; Lopez, C.; Gil, L.; Coelho, P. Absence of Healing Impairment in Osteotomies Prepared via Osseodensification Drilling. Int. J. Periodontics Restor. Dent. 2019, 39, 65–71. [Google Scholar] [CrossRef]
- Lahens, B.; Neiva, R.; Tovar, N.; Alifarag, A.M.; Jimbo, R.; Bonfante, E.A.; Bowers, M.M.; Cuppini, M.; Freitas, H.; Witek, L.; et al. Biomechanical and histologic basis of osseodensification drilling for endosteal implant placement in low density bone. An experimental study in sheep. J. Mech. Behav. Biomed. Mater. 2016, 63, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.D.; Alifarag, A.M.; Torroni, A.; Tovar, N.; Diaz-Siso, J.R.; Witek, L.; Rodriguez, E.D.; Coelho, P.G. Osseodensification for enhancement of spinal surgical hardware fixation. J. Mech. Behav. Biomed. Mater. 2017, 69, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.H.; Neiva, R.; Coelho, P.G.; Witek, L.; Tovar, N.M.; Lo, I.C.; Gil, L.F.; Torroni, A. Alveolar ridge expansion: Comparison of osseodensification and conventional osteotome techniques. J. Craniofacial Surg. 2019, 30, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Lahens, B.; Lopez, C.D.; Neiva, R.F.; Bowers, M.M.; Jimbo, R.; Bonfante, E.A.; Morcos, J.; Witek, L.; Tovar, N.; Coelho, P.G. The effect of osseodensification drilling for endosteal implants with different surface treatments: A study in sheep. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 107, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Torroni, A.; Parente, P.E.L.; Witek, L.; Hacquebord, J.H.; Coelho, P.G. Osseodensification drilling vs conventional manual instrumentation technique for posterior lumbar fixation: Ex-vivo mechanical and histomorphological analysis in an ovine model. J. Orthop. Res. 2021, 39, 1463–1469. [Google Scholar] [CrossRef]
- Mele, R.E.; Kurtzman, G.M. Feline dental implants: New paradigm shift in maxillary alveolar osteitis treatment planning with osseodensification. J. Osseointegration 2019, 11, 485–492. [Google Scholar] [CrossRef]
- Lu, J.Y.; Yu, J.Y.; Xie, C.Y.; Gao, J.; Yu, H.Y. Immediate precision of the digital osteotomy template in the digital stackable template: A clinical study. Hua Xi Kou Qiang Yi Xue Za Zhi 2021, 39, 732–738, English, Chinese. [Google Scholar] [CrossRef]
| P | Population | Patients who need sub-antral bone grafts or have narrow bone ridges, low-density bone (type IV), and post-extraction implants. |
| I | Intervention | Use of the OD technique in implant placement. |
| C | Comparison | Implants placed using other conventional techniques. |
| O | Outcomes | To analyse the OD technique in oral implantology. |
| Was the Attribution Sequence Generated and Applied Properly? | Were the Groups Similar at Baseline, or Were They Adjusted for Confounding Factors in the Analysis? | Has the Distribution of the Different Groups Been Adequately Concealed? | Were the Animals Housed Randomly during the Experiment? | Were the Carers and/or Researchers Blind to the Intervention of Each Animal Received during the Experiment? | Were the Animals Randomly Selected to Evaluate the Results? | Were the Results Assessed or Blind? | Have Incomplete Results Data Been Handled Appropriately? | Are the Study Reports Exempt from Selective Results Reporting? | Was the Study Apparently Free of Other Problems that Could Result in a High Risk of Bias? | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lahens et al. [21], 2016 | N | Y | UN | N | N | N | UN | Y | N | N |
| Trisi et al. [18], 2016 | N | Y | UN | N | Y | N | Y | Y | Y | Y |
| Huwais and Meyer [8], 2017 | N | Y | N | UN | N | N | N | N | N | N |
| Lopez et al. [22], 2017 | N | Y | UN | N | N | N | N | N | UN | N |
| Alifarag et al. [19], 2018 | N | Y | N | UN | N | N | N | Y | Y | N |
| Slete et al. [2], 2018 | N | Y | UN | N | N | N | Y | Y | N | N |
| Oliveira et al. [7], 2018 | UN | Y | UN | UN | N | UNr | UN | UN | N | N |
| Tian et al. [23], 2019 | N | Y | UN | UN | N | N | N | Y | UN | UN |
| Witek et al. [20] 2019 | N | Y | N | Y | N | N | N | Y | N | N |
| Lahens et al. [21], 2019 | N | Y | N | UN | N | N | N | Y | N | N |
| Torroni et al. [25], 2021 | N | Y | UN | N | N | N | N | N | N | N |
| Have the Demographic Characteristics Been Clearly Described? | Was the Patient’s History Clearly Described and Presented as a Timeline? | Was the Patient’s Current Clinical Condition at the Time of Presentation Clearly Described? | Have the Diagnostic Tests or Methods and the Results Been Clearly Described? | Was the Intervention or Treatment Procedure Clearly Described? | Was the Post-Intervention Clinical State Clearly Described? | Have Adverse Events or Unforeseen Events Been Identified and Described? | Does the Case Report Provide Relevant Data to Draw from? | |
|---|---|---|---|---|---|---|---|---|
| Mello-Machado et al. [15], 2018 | Y | Y | Y | Y | Y | Y | NA | Y |
| Huwais et al. [16], 2018 | N | Y | Y | Y | Y | Y | N | Y |
| da Rosa et al. [13], 2019 | N | N | N | Y | Y | Y | N | Y |
| Salgar et al. [17], 2021 | Y | Y | Y | Y | Y | Y | Y | Y |
| Was the Randomisation Method Appropriate? | Was the Allocation Method Appropriate? | Were the Groups Similar at the Start of the Study? | Were the Participants Blinded? | Were the Professionals Who Administered the Interventions Blinded? | Were the Outcome Assessors Blinded? | Were the Interventions Clearly Described and Applied Equally to the Groups? | Was the Primary Outcome Clearly Defined and Measured? | Was there an Intention-to-Treat Analysis? | Have Losses and Exclusions Been Described? | Were there any Complications or Adverse Events Reported? | Were the Results of the Study Accurate and Reliable? | Were the Results of the Study Relevant to Clinical Practice? | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jarikian et al. [6], 2021 | Y | Y | Y | N | N | Y | Y | Y | Y | N | Y | UN | UN |
| Mello-Machado et al. [12], 2021 | UN | UN | Y | N | N | Y | Y | Y | N | Y | N | UN | UN |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fontes Pereira, J.; Costa, R.; Nunes Vasques, M.; Salazar, F.; Mendes, J.M.; Infante da Câmara, M. Osseodensification: An Alternative to Conventional Osteotomy in Implant Site Preparation: A Systematic Review. J. Clin. Med. 2023, 12, 7046. https://doi.org/10.3390/jcm12227046
Fontes Pereira J, Costa R, Nunes Vasques M, Salazar F, Mendes JM, Infante da Câmara M. Osseodensification: An Alternative to Conventional Osteotomy in Implant Site Preparation: A Systematic Review. Journal of Clinical Medicine. 2023; 12(22):7046. https://doi.org/10.3390/jcm12227046
Chicago/Turabian StyleFontes Pereira, João, Rosana Costa, Miguel Nunes Vasques, Filomena Salazar, José Manuel Mendes, and Marco Infante da Câmara. 2023. "Osseodensification: An Alternative to Conventional Osteotomy in Implant Site Preparation: A Systematic Review" Journal of Clinical Medicine 12, no. 22: 7046. https://doi.org/10.3390/jcm12227046
APA StyleFontes Pereira, J., Costa, R., Nunes Vasques, M., Salazar, F., Mendes, J. M., & Infante da Câmara, M. (2023). Osseodensification: An Alternative to Conventional Osteotomy in Implant Site Preparation: A Systematic Review. Journal of Clinical Medicine, 12(22), 7046. https://doi.org/10.3390/jcm12227046