


A Systematic Review and Illustrative Case Presentation of Low-Grade Myofibroblastic Sarcoma (LGMS) of the Extremities
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
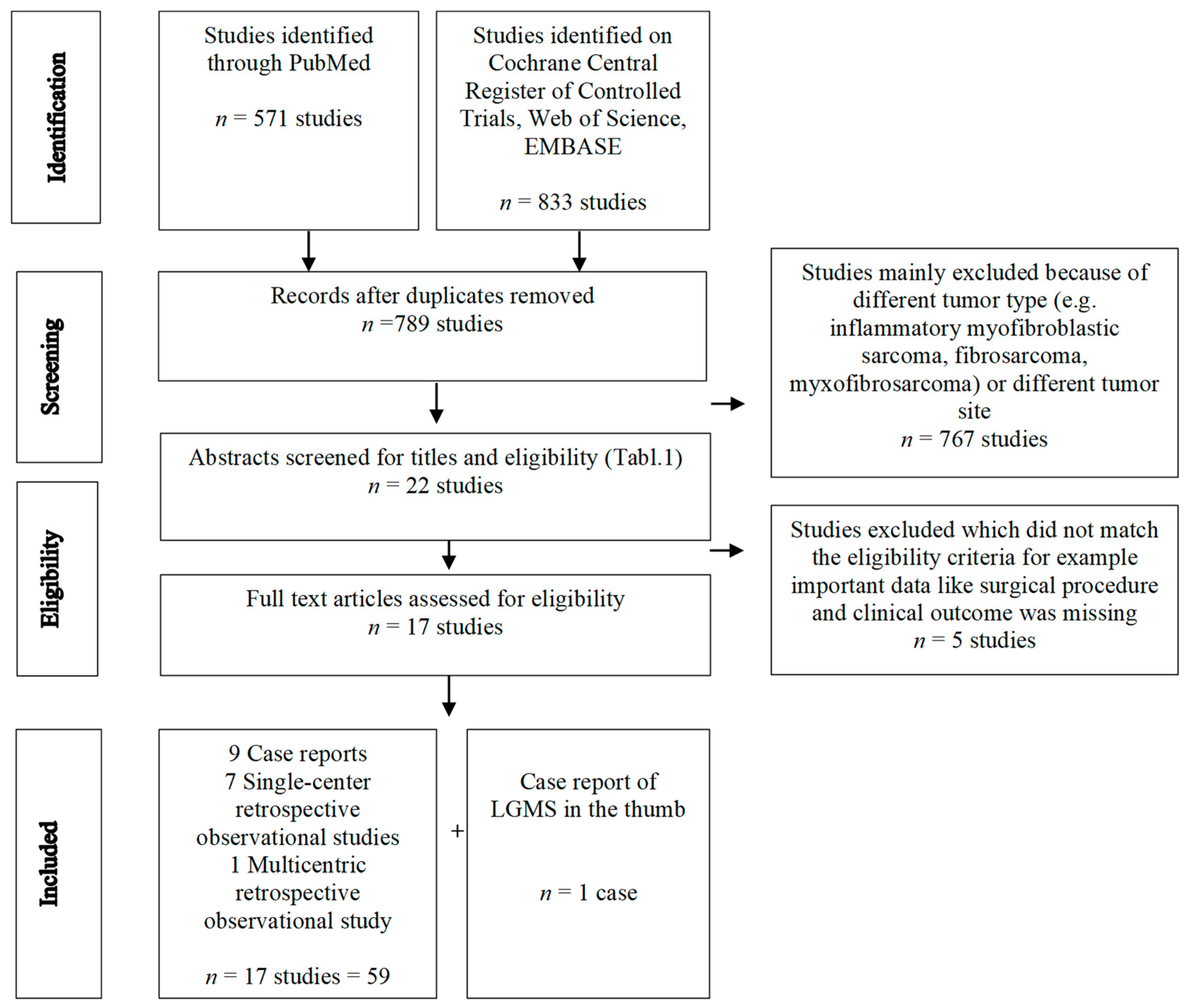
2.1. Literature Search
2.2. Data Extraction and Analysis
2.3. Quality Assessment and Evaluation of the Risk of Biases
3. Results
3.1. Study Characteristics
3.2. Patient and Tumor Characteristics
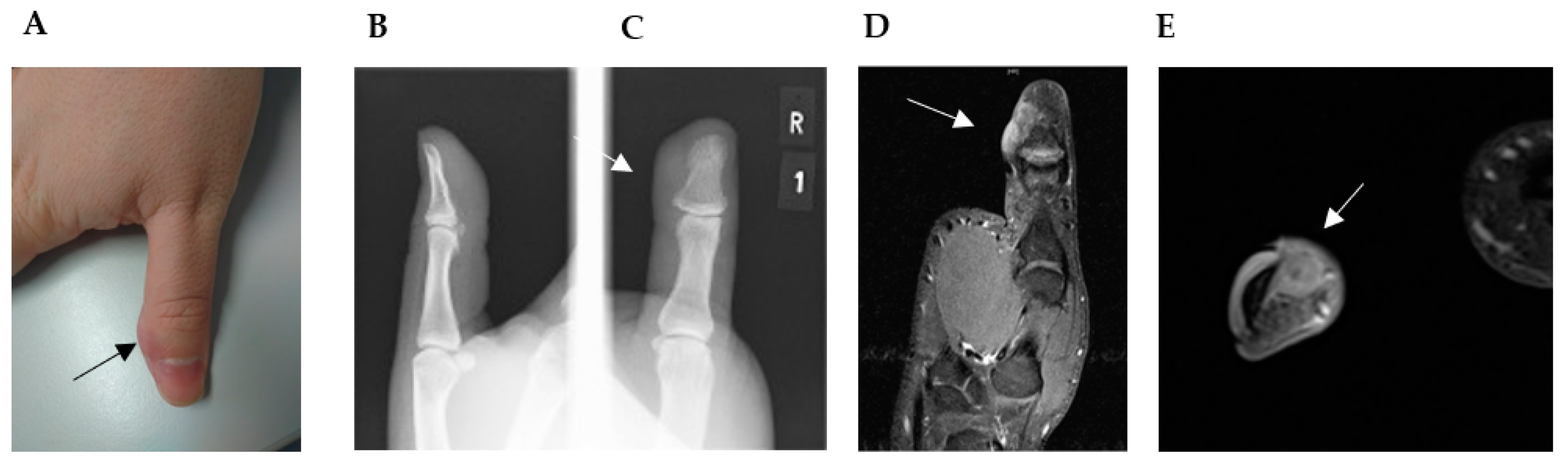
3.3. Imaging Features
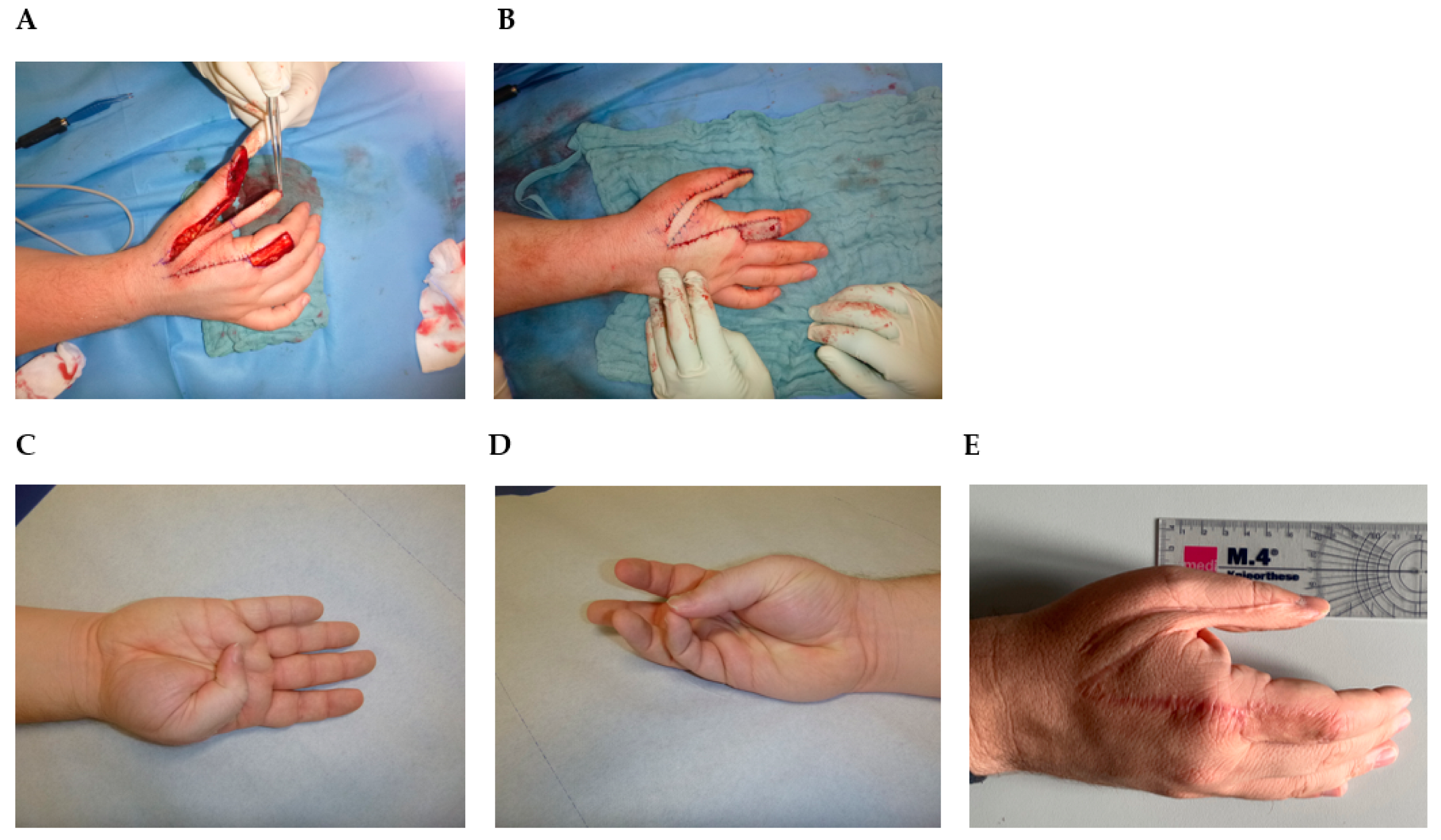
3.4. Treatment Strategy
3.5. Clinical Outcome
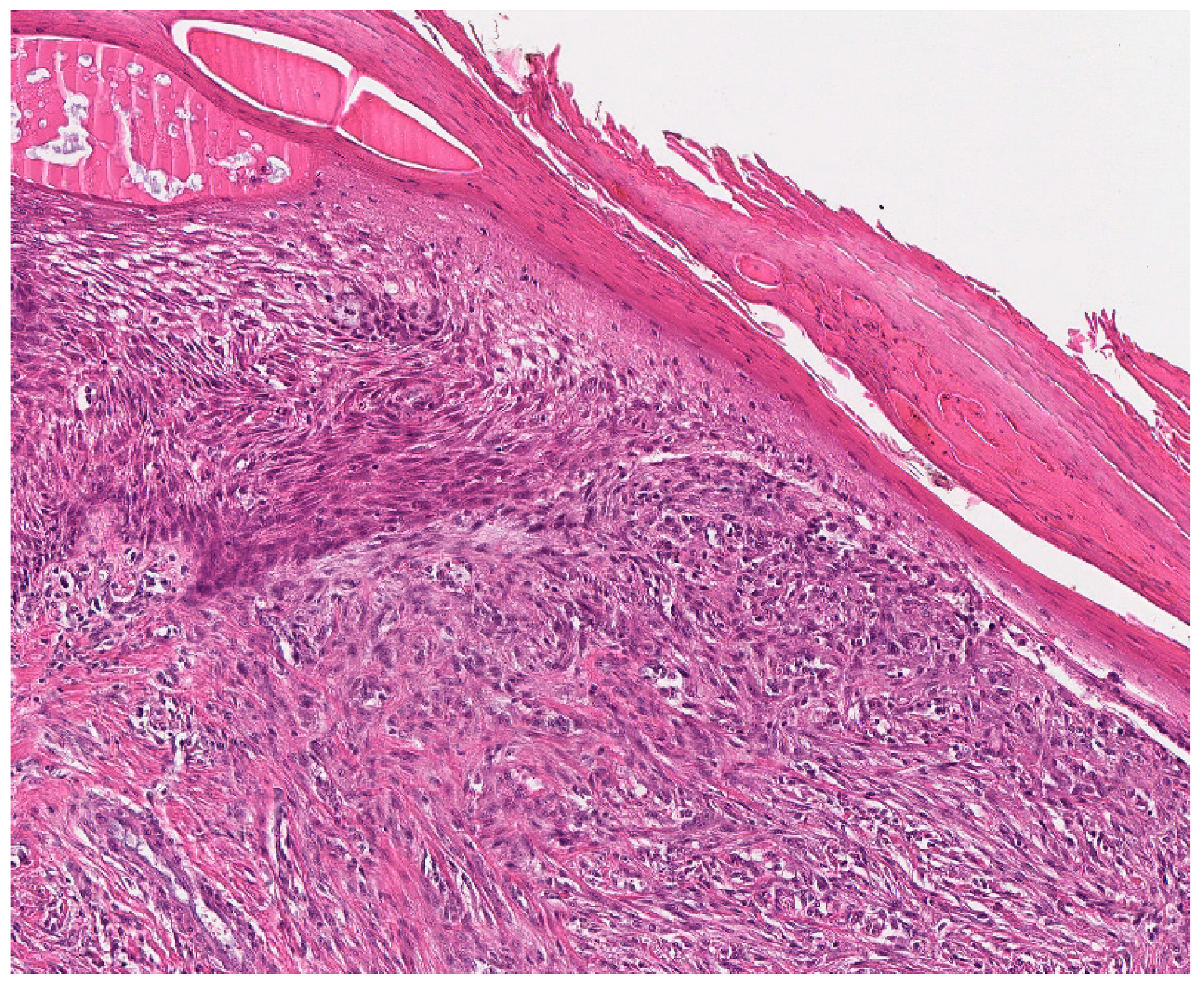
3.6. Case Presentation and Clinicopathological Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vasudev, K.S.; Harris, M. A sarcoma of myofibroblasts: An ultrastructural study. Arch. Pathol. Lab. Med. 1978, 102, 185–188. [Google Scholar] [PubMed]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours: Soft Tissue and Bone Tumours; International Agency for Research on Cancer, IARD Press: Lyon, France, 2020. [Google Scholar]
- Mentzel, T.; Dry, S.; Katenkamp, D.; Fletcher, C.D. Low-grade myofibroblastic sarcoma: Analysis of 18 cases in the spectrum of myofibroblastic tumors. Am. J. Surg. Pathol. 1998, 22, 1228–1238. [Google Scholar] [CrossRef]
- Chan, J.Y.; Gooi, Z.; Wong, E.W.; Ng, S.K.; Tong, M.C.; Vlantis, A.C. Low-grade myofibroblastic sarcoma: A population-based study. Laryngoscope 2017, 127, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Schurch, W.; Seemayer, T.A.; Gabbiani, G. The myofibroblast: A quarter century after its discovery. Am. J. Surg. Pathol. 1998, 22, 141–147. [Google Scholar] [CrossRef]
- Chang, S.E.; Choi, J.H.; Sung, K.J.; Moon, K.C.; Koh, J.K.; Lee, T.J.; Ro, J.Y.; Silverman, J.S. A case of cutaneous low-grade myofibroblastic sarcoma. J. Dermatol. 2001, 28, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Gao, G.; Liu, Y.; Ao, Y.; Wang, J.; Xu, Y. Low-grade myofibroblastic sarcoma of the proximal femur: A case report and literature review. Medicine 2022, 101, e31715. [Google Scholar] [CrossRef]
- Oylumlu, M.; Yildiz, A.; Ercan, S.; Oylumlu, M.; Davutoglu, V. Cardiac metastasis of a low-grade myofibroblastic sarcoma. Echocardiography 2014, 31, E1–E4. [Google Scholar] [CrossRef]
- Wang, L.; Li, L.X.; Chen, D.Q.; Yang, L.; Li, S.K.; Cheng, C. Low-grade Myofibroblastic sarcoma: Clinical and imaging findings. BMC Med. Imaging 2019, 19, 36. [Google Scholar] [CrossRef]
- Yonezawa, H.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Igarashi, K.; Langit, M.B.; Kimura, H.; Shimozaki, S.; Kato, T.; et al. Low-grade myofibroblastic sarcoma of the levator scapulae muscle: A case report and literature review. BMC Musculoskelet. Disord. 2020, 21, 836. [Google Scholar] [CrossRef]
- Magro, G. Differential Diagnosis of Benign Spindle Cell Lesions. Surg. Pathol. Clin. 2018, 11, 91–121. [Google Scholar] [CrossRef]
- Eyden, B.; Banerjee, S.S.; Shenjere, P.; Fisher, C. The myofibroblast and its tumours. J. Clin. Pathol. 2009, 62, 236–249. [Google Scholar] [CrossRef] [PubMed]
- Mentzel, T. Low-grade myofibroblastic sarcoma. In WHO Classification of Tumours of Soft Tissue and Bone; Fletcher, C.D.M., Bridge, J.A., Hogendoorn, P.C.W., Mertens, F., Eds.; International Agency for Reserach on Cancer: Lyon, France, 2013; p. 85. [Google Scholar]
- Mentzel, T.; Schneider-Stock, R. Niedrigmalignes Myofibroblastisches Sarkom. In Pathologie: Kopf-Hals-Region, Weichgewebstumoren, Haut, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Qiu, X.; Montgomery, E.; Sun, B. Inflammatory myofibroblastic tumor and low-grade myofibroblastic sarcoma: A comparative study of clinicopathologic features and further observations on the immunohistochemical profile of myofibroblasts. Hum. Pathol. 2008, 39, 846–856. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, E.; Goldblum, J.R.; Fisher, C. Myofibrosarcoma: A clinicopathologic study. Am. J. Surg. Pathol. 2001, 25, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Demarosi, F.; Bay, A.; Moneghini, L.; Carrassi, A. Low-grade myofibroblastic sarcoma of the oral cavity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C. Soft tissue sarcomas: Diagnosis, classification and prognostic factors. Br. J. Plast. Surg. 1996, 49, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A system for the surgical staging of musculoskeletal sarcoma. Clin. Orthop. Relat. Res. 1980, 153, 106–120. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Meng, G.Z.; Zhang, H.Y.; Bu, H.; Zhang, X.L.; Pang, Z.G.; Ke, Q.; Liu, X.; Yang, G. Myofibroblastic sarcomas: A clinicopathological study of 20 cases. Chin. Med. J. 2007, 120, 363–369. [Google Scholar] [CrossRef]
- Nagata, Y.; Matsuno, T.; Hamada, N.; Shimose, S.; Arihiro, K.; Ochi, M. Low-grade myofibroblastic sarcoma of the palm. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2008, 42, 164–167. [Google Scholar] [CrossRef]
- Nakashima, H.; Yoshida, M.; Miyamoto, K. Anatomical reconstruction of the patellar tendon using the fascia lata attached to the iliac bone following resection for soft tissue sarcoma: A case report. Upsala J. Med. Sci. 2012, 117, 460–464. [Google Scholar] [CrossRef]
- Wechalekar, M.D.; Ayres, O.; Farshid, G.; Clayer, M.; Cleland, L.G. Multicentric myofibroblastic sarcoma. BMJ Case Rep. 2014, 2014, bcr2013201666. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.-G.; Pan, C.-C.; Yu, D.-H.; Feng, Z.-Z.; Ma, L.; Zhao, Y.; Xu, H.-B. Myofibroblastic sarcomas: A clinicopathologic analysis of 15 cases and review of literature. Int. J. Clin. Exp. Pathol. 2016, 9, 1568–1577. [Google Scholar]
- Kim, J.H.; Choi, W.; Cho, H.S.; Lee, K.S.; Park, J.K.; Kim, B.K. Surgical treatment and long-term outcomes of low-grade myofibroblastic sarcoma: A single-center case series of 15 patients. World. J. Surg. Oncol. 2021, 19, 339. [Google Scholar] [CrossRef]
- Kito, M.; Ae, K.; Okamoto, M.; Endo, M.; Ikuta, K.; Takeuchi, A.; Yasuda, N.; Yasuda, T.; Imura, Y.; Morii, T.; et al. Clinical Outcome of low-Grade Myofibroblastic Sarcoma in Japan: A multicenter Study from the Japanese Musculoskeletal Oncology Group. Cancers 2023, 15, 2314. [Google Scholar] [CrossRef]
- Watanabe, K.; Ogura, G.; Tajino, T.; Hoshi, N.; Suzuki, T. Myofibrosarcoma of the bone: A clinicopathologic study. Am. J. Surg. Pathol. 2001, 25, 1501–1507. [Google Scholar] [CrossRef] [PubMed]
- San Miguel, P.; Fernandez, G.; Ortiz-Rey, J.A.; Larrauri, P. Low-grade myofibroblastic sarcoma of the distal phalanx. J. Hand Surg. Am. 2004, 29, 1160–1163. [Google Scholar] [CrossRef]
- Arora, R.; Gupta, R.; Sharma, A.; Dinda, A.K. A rare case of low-grade myofibroblastic sarcoma of the femur in a 38-year-old woman: A case report. J. Med. Case Rep. 2010, 4, 121. [Google Scholar] [CrossRef]
- Saito, T.; Mitomi, H.; Kurisaki, A.; Torigoe, T.; Takagi, T.; Suehara, Y.; Okubo, T.; Kaneko, K.; Yao, T. Low-grade myofibroblastic sarcoma of the distal femur. Int. J. Surg. Case Rep. 2013, 4, 195–199. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Tufanaru, C.; Qureshi, R.; Mattis, P.; Mu, P. Conducting systematic reviews of association (etiology): The Joanna Briggs Institute’s approach. JBI Evid. Implement. 2015, 13, 163–169. [Google Scholar] [CrossRef]
- Foucher, G.; Braun, J.B. A new island flap transfer from the dorsum of the index to the thumb. Plast. Reconstr. Surg. 1979, 63, 344–349. [Google Scholar] [CrossRef]
- Holevich, J. Our technique of pedicle skin flaps and its use in the surgery of the hand and fingers. Acta Chir. Plast. 1960, 2, 271–284. [Google Scholar]
- Holevich, J.; Paneva-Holevich, E. Bipedicled island flap. Acta Chir. Plast. 1971, 13, 106–116. [Google Scholar]
- Diaz-Cascajo, C.; Borghi, S.; Weyers, W.; Metze, D. Fibroblastic/myofibroblastic sarcoma of the skin: A report of five cases. J. Cutan. Pathol. 2003, 30, 128–134. [Google Scholar] [CrossRef]
- Roth, T.M.; Fratkin, J.; Woodring, T.C.; McGehee, R.P. Low-grade myofibroblastic sarcoma of the vulva. Gynecol. Oncol. 2004, 92, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Humphries, W.E., 3rd; Satyan, K.B.; Relyea, K.; Kim, E.S.; Adesina, A.M.; Chintagumpala, M.; Jea, A. Low-grade myofibroblastic sarcoma of the sacrum. J. Neurosurg. Pediatr. 2010, 6, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.B.; Chundru, S.; Hatch, S.S.; Hawkins, H.K.; Adegboyega, P.A.; Eltorky, M.A. Uncommon malignancies: Case 1. Low-grade myofibroblastic sarcoma of the breast. J. Clin. Oncol. 2005, 23, 6249–6251. [Google Scholar] [CrossRef] [PubMed]
- Tavora, F.; Miettinen, M.; Fanburg-Smith, J.; Franks, T.J.; Burke, A. Pulmonary artery sarcoma: A histologic and follow-up study with emphasis on a subset of low-grade myofibroblastic sarcomas with a good long-term follow-up. Am. J. Surg. Pathol. 2008, 32, 1751–1761. [Google Scholar] [CrossRef]
- Meng, G.Z.; Zhang, H.Y.; Zhang, Z.; Wei, B.; Bu, H. Myofibroblastic sarcoma vs nodular fasciitis: A comparative study of chromosomal imbalances. Am. J. Clin. Pathol. 2009, 131, 701–709. [Google Scholar] [CrossRef]
- Peng, L.; Tu, Y.; Li, Y.; Xiao, W. Low-grade myofibroblastic sarcoma of the pancreas: A case report and literature review. J. Cancer Res. Ther. 2018, 14, S796–S799. [Google Scholar] [CrossRef]
- Scalas, G.; Parmeggiani, A.; Martella, C.; Tuzzato, G.; Bianchi, G.; Facchini, G.; Clinca, R.; Spinnato, P. Magnetic resonance imaging of soft tissue sarcoma: Features related to prognosis. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1567–1575. [Google Scholar] [CrossRef]
- Morii, T.; Mochizuki, K.; Sano, H.; Fujino, T.; Harasawa, A.; Satomi, K. Occult myofibroblastic sarcoma detected on FDG-PET performed for cancer screening. Ann. Nucl. Med. 2008, 22, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Niu, R.; Wang, J.F.; Zhang, D.C.; Shao, X.L.; Qiu, C.; Wang, Y.T. Low-grade myofibroblastic sarcoma of gastric cardia on 18F-FDG positron emission tomography/computed tomography: An extremely rare case report. Medicine 2018, 97, e9720. [Google Scholar] [CrossRef] [PubMed]
- Sambri, A.; Caldari, E.; Fiore, M.; Zucchini, R.; Giannini, C.; Pirini, M.G.; Spinnato, P.; Cappelli, A.; Donati, D.M.; De Paolis, M. Margin Assessment in Soft Tissue Sarcomas: Review of the Literature. Cancers 2021, 13, 1687. [Google Scholar] [CrossRef] [PubMed]
- Kandel, R.; Coakley, N.; Werier, J.; Engel, J.; Ghert, M.; Verma, S.; Sarcoma Disease Site Group of Cancer Care Ontario’s Program in Evidence-Based Care. Surgical margins and handling of soft-tissue sarcoma in extremities: A clinical practice guideline. Curr. Oncol. 2013, 20, e247–e254. [Google Scholar] [CrossRef]
- Yamada, T.; Yoshimura, T.; Kitamura, N.; Sasabe, E.; Ohno, S.; Yamamoto, T. Low-grade myofibroblastic sarcoma of the palate. Int. J. Oral Sci. 2012, 4, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Puhaindran, M.E.; Rothrock, C.P.; Athanasian, E.A. Surgical management for malignant tumors of the thumb. Hand 2011, 6, 373–377. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search strategy Pubmed |
| “myofibroblastic sarcoma”[tiab] OR “myofibroblastic sarcomas”[tiab] OR myofibrosarcoma*[tiab] OR “Fibrosarcoma/surgery”[Mesh] AND “Extremities”[Mesh] NOT (animals [mh] NOT humans [mh]) 571 hits |
| Search strategy Embase |
| ‘myofibroblastic sarcoma’ OR ‘myofibroblastic sarcomas’ OR myofibrosarcoma* OR ‘fibrosarcoma’/’surgery’/exp AND ‘extremities’/exp 411 hits |
| Search strategy Central (Cochrane Central Register of Controlled Trials) |
| (“myofibroblastic sarcoma” OR “myofibroblastic sarcomas” OR myofibrosarcoma*):ti,ab,kw OR MeSH descriptor: [Fibrosarcoma] explode all trees 18 hits |
| Search strategy Web of Science |
| TS = (“myofibroblastic sarcoma” OR “myofibroblastic sarcomas” OR myofibrosarcoma*) 404 hits |
| Patients | Histology of LGMS in the extremities, excluding tumors of the trunk |
| Intervention | Surgical treatment |
| Comparison | Wide resection vs. marginal resection of the tumor |
| Outcome | Local recurrence, metastasis, evidence of disease |
| Study design | Randomized controlled trials, prospective trials, retrospective studies, case reports, systematic reviews |
| Authors | Study Design | Year | Case no. | Gender | Age | Site of Tumor | Size (cm) | Treatment | Local Recurrence | Metastases | Outcome | FU (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (a) Patient characteristics, treatment and outcome of cases of LGMS of the extremities located in the soft tissue | ||||||||||||
| Mentzel et al. [3] | RS | 1998 | 1 | F | 29 | Right supraclavicular | 8 | LE | (−) | (−) | NSR | 20 |
| 2 | M | 31 | Left thigh | 4 | LE | (−) | (−) | NSR | 22 | |||
| 3 | M | 52 | Left shoulder | 4 | LE | (−) | (−) | NA | NA | |||
| 4 | M | 50 | Right arm | 3 | LE + RT | (−) | (−) | NA | NA | |||
| 5 | F | 33 | Left inner thigh | 3.2 | LE + RT | (−) | (−) | NSR | 12 | |||
| Montgomery et al. [16] | RS | 2001 | 6 | M | 42 | Axilla subcutis | 5 | LE | (−) | (−) | NSR | 36 |
| 7 | M | 69 | Leg | NA | WR + CT | (+) | (−) | LR at 8 months, then RT, further LR at 70 months, then amp | 70 | |||
| 8 | M | 57 | Anterior thigh | 4 | WR + RT | (−) | (−) | NSR | 144 | |||
| 9 | M | 64 | Arm | 1.5 | LE | (−) | (−) | NSR | 48 | |||
| Meng et al. [22] | RS | 2007 | 10 | F | 30 | Shoulder | 3.7 | NA (SP) | (−) | (−) | NSR | 22 |
| 11 | M | 9 | Scapular area | 3 | NA (SP) | (−) | (−) | NSR | 41 | |||
| 12 | F | 40 | Groin | 3 | NA (SP) + CT | (−) | (−) | NSR | 34 | |||
| Nagata et al. [23] | CR | 2008 | 13 | M | 36 | Palm (ST) | 2.5 × 1.5 | LE | (−) | (−) | NSR | 25 |
| Nakashima et al. [24] | CR | 2012 | 14 | F | 43 | Parapatellar tendon | 3 | WR + RT | (−) | (−) | NSR | 36 |
| Oylumlu et al. [8] | CR | 2014 | 15 | M | 36 | Inguinal region | NA | NA (SP) | (+) | (+) | LR and death | NA |
| Wechalekar et al. [25] | CR | 2014 | 16 | M | 62 | Multicentric (knees, shoulder, hips, sartorius muscle) | NA | LE (ME) | (−) | (−) | NA | NA |
| Cai et al. [26] | RS | 2016 | 17 | M | 6 | Left hip | 5 | WR | (−) | (−) | NSR | 11 |
| Wang et al. [9] | RS | 2019 | 18 | NA | Right shoulder | 8.9 × 6.8 | NA (SP) | (+) | (−) | LR | 48 | |
| 19 | NA | Right thigh | 5.6 × 7.4 | NA (SP) | (+) | (−) | IMT translate into LGMS after LR for 3 times, 8 LR within 8 years | 192 | ||||
| Yonezawa et al. [10] | CR | 2020 | 20 | F | 69 | Left M. levator scapulae | 2.5 × 3.5 | WR | (−) | (−) | NSR | NA |
| Kim et al. [27] | RS | 2021 | 21 | F | 57 | Lt. medial elbow | 2.9 × 2.4 × 2.0 | WR | (−) | (−) | NSR | NA |
| 22 | M | 68 | Rt. Deltoid | 2.9 × 1.2 × 1.1 | WR | (−) | (−) | NSR | 18 | |||
| 23 | M | 50 | Lt. shoulder | 0.7 × 0.5 × 0.4 | WR | (−) | (−) | NSR | 25 | |||
| 24 | F | 45 | Rt. forearm | NA | WR | (−) | (−) | NSR | 18 | |||
| 25 | F | 20 | Lt. shoulder | 2.8 × 2.4 × 2.0 | WR | (−) | (−) | NSR | 24 | |||
| 26 | M | 68 | Rt. shoulder | 2.3 × 2.1 × 1.2 | WR | (−) | (−) | NSR | 60 | |||
| 27 | F | 36 | Lt. lateral thigh | 1.7 × 1.4 × 0.8 | WR | (−) | (−) | NSR | 15 | |||
| 28 | M | 62 | Rt. Inguinal | 5.9 × 5.8 × 4.9 | WR | (−) | (−) | NSR | 10 | |||
| 29 | M | 61 | Rt. Forearm | 3.7 × 3.3 × 2.8 | WR | (−) | (−) | NSR | 38 | |||
| 30 | M | 58 | Lt. hand 2nd webspace | 3.9 × 3.7 × 2.6 | LE (En bloc excision) | (−) | (−) | NSR | 18 | |||
| 31 | F | 70 | Distal thigh | 2.3 × 2.0, 0.5 | WR | (−) | (−) | NSR | 15 | |||
| 32 | F | 46 | Rt. Forearm | 1.2 × 0.5 × 1.1 | WR | (−) | (−) | NSR | 20 | |||
| Present case | CR | 2020 | 33 | M | 28 | Thumb | 2 × 1.5 | WR + PS | (+) | (−) | NSR | 38 |
| Kito et al. [28] | RS, MCS | 2023 | 34 | F | 30 | Ankle | 1.6 | LE (ME) | (−) | (−) | NSR | 83 |
| 35 | M | 11 | Upper Arm | 2.8 | WR | (−) | (−) | NSR | 96 | |||
| 36 | F | 19 | Thigh | 3.7 | WR | (−) | (−) | NSR | 94 | |||
| 37 | M | 12 | Foot | 2.8 | WR | (−) | (−) | NSR | 118 | |||
| 38 | F | 79 | Forearm | 4 | WR + RT (48 Gy) | (−) | (−) | NSR | 50 | |||
| 39 | F | 27 | Upper Arm (Relapse at initial presentation) | 2.5 | WR | (−) | (−) | NSR | 32 | |||
| 40 | F | 19 | Groin | 3 | WR | (−) | (−) | NSR | 55 | |||
| 41 | F | 74 | Lower leg | 9.5 | WR + RT (60 Gy) | (+) | (−) | AED | 54 | |||
| 42 | M | 33 | Thigh | 2.8 | WR | (−) | (−) | NSR | 73 | |||
| 43 | F | 26 | Axilla | 7 | LE (ME) | (+) | (−) | NSR | 181 | |||
| 44 | F | 86 | Thigh | 10 | WR + RT (66 Gy) | (−) | (−) | NSR | 88 | |||
| (b) Patient characteristics, treatment and outcome of cases of LGMS of the extremities with local tissue invasion of the bone. | ||||||||||||
| Montgomery et al. [16] | RS | 2001 | 45 | M | 65 | Tibia (B) | 11 | LE | (+) | (−) | LR at 24 months, then amp, then NSR 172 at months | 172 |
| Watanabe et al. [29] | RS | 2001 | 46 | M | 60 | Distal Femur (B) | 5 | WR + CT | (−) | (−) | NSR | NA |
| 47 | F | 63 | Distal Femur (B) | 9 | LE | (−) | (−) | NSR | NA | |||
| San Miguel et al. [30] | CR | 2004 | 48 | F | 51 | Distal Phalanx | 1.8 | Amp | (−) | (−) | NSR | 28 |
| Meng et al. [22] | RS | 2007 | 49 | M | 14 | Femur | 10 | NA (SP) + CT | (+) | (−) | LR | 20 |
| 50 | F | 30 | Femur | 4 | NA (SP) + CT | (+) | (−) | LR 2x | 29 | |||
| Arora et al. [31] | CR | 2010 | 51 | F | 38 | Femur (B) | 20 × 10 | WR + prosthesis | (−) | (−) | AED | NA |
| Saito et al. [32] | CR | 2013 | 52 | F | 50 | Distal femur (B) | NA | WR + prosthesis | (−) | (−) | NSR | 15 |
| Cai et al. [26] | RS | 2016 | 53 | F | 43 | Right tibia (B) | 4 | LE (ILR + bone graft) | (+) | (−) | LR | 33 |
| Wang et al. [9] | RS | 2019 | 54 | NA | Right scapula (B) | 13 × 13.5 | NA (SP) | (−) | (+) | Pulmonary metastasis before operation | NA | |
| 55 | NA | Left distal femur (B) | NA | NA (SP) | (−) | (+) | Pulmonary metastasis after 8 months of operation | NA | ||||
| 56 | NA | Right distal femur (B) | NA | NA (SP) | (−) | (+) | Pulmonary metastasis after 56 months of operation | 56 | ||||
| 57 | NA | Left distal femur (B) | NA | NA (SP) | (+) | (+) | LR and bone metastasis at 17 months | 17 | ||||
| Kim et al. [27] | RS | 2021 | 58 | M | 27 | Rt.3rd finger proximal phalanx (B) | 2.2 × 2.0 × 1.0 | LE (ME, En bloc excision limb salvage surgery) | (+) | (−) | LR | 71 |
| Gao et al. [7] | CR | 2022 | 59 | F | 30 | Femoral head neck junction (B) | LE (ILE, Hip arthroscopy) | (−) | (−) | NSR | 6 | |
| Author | Case No. | Study Design | Were the Patient’s Demographic Characteristics Clearly Described? | Was the Patient’s History Clearly Described and Presented as a Timeline? | Was the Current Clinical Condition of the Patient on Presentation Clearly Described? | Were Diagnostic Tests or Assessment Methods and the Results Clearly Described? | Was the Intervention(s) or Treatment Procedure(s) Clearly Described? | Was the Post-Intervention Clinical Condition Clearly Described? | Were Adverse Events (Harms) or Unanticipated Events Identified and Described? | Does the Case Report Provide Takeaway Lessons? | Overall Appraisal: Include Exclude Seek further Info |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mentzel et al. [3] | 1 | RS | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Include |
| 2 | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Include | ||
| 3 | Yes | Yes | No | Yes | Yes | No | No | Yes | Include | ||
| 4 | Yes | Yes | No | Yes | Yes | No | No | Yes | Include | ||
| 5 | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Include | ||
| Montgomery et al. [16] | 6 | RS | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Include |
| 7 | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Include | ||
| 8 | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Include | ||
| 9 | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Include | ||
| 10 | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Include | ||
| Watanabe et al. [29] | 11 | RS | Yes | No | No | Yes | Yes | Yes | No | Yes | Include |
| 12 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| San Miguel et al. [30] | 13 | CR | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include |
| Meng et al. [22] | 14 | RS | Yes | No | No | Yes | Yes | Yes | No | Yes | Include |
| 15 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 16 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 17 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 18 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| Nagata et al. [23] | 19 | CR | Yes | Yes | Yes | Yes | No | No | No | Yes | Include |
| Arora et al. [31] | 20 | CR | Yes | Yes | Yes | Yes | No | No | No | Yes | Include |
| Nakashima et al. [24] | 21 | CR | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include |
| Saito et al. [32] | 22 | CR | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Include |
| Oylumlu et al. [8] | 23 | CR | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Include |
| Wechalekar et al. [25] | 24 | CR | Yes | Yes | Yes | Yes | No | No | No | Yes | Include |
| Cai et al. [26] | 25 | RS | Yes | No | No | Yes | Yes | Yes | No | Yes | Include |
| 26 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| Wang et al. [9] | 27 | RS | No | No | No | Yes | No | No | Yes | Yes | Include |
| 28 | No | No | No | Yes | No | No | Yes | Yes | Include | ||
| 29 | No | No | No | Yes | No | Yes | Yes | Yes | Include | ||
| 30 | No | No | No | Yes | No | Yes | Yes | Yes | Include | ||
| 31 | No | No | No | Yes | No | Yes | Yes | Yes | Include | ||
| 32 | No | No | No | Yes | No | Yes | Yes | Yes | Include | ||
| Yonezawa et al. [10] | 33 | CR | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include |
| Kim et al. [27] | 34 | RS | Yes | No | No | Yes | Yes | Yes | No | Yes | Include |
| 35 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 36 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 37 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 38 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 39 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 40 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 41 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 42 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 43 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 44 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 45 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 46 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| Present case | 47 | CR | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Include |
| Gao et al. [7] | 48 | CR | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Include |
| Kito et al. [28] | 49 | RS, MC | Yes | No | No | Yes | Yes | Yes | No | Yes | Include |
| 50 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 51 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 52 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 53 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 54 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 55 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 56 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 57 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 58 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include | ||
| 59 | Yes | No | No | Yes | Yes | Yes | No | Yes | Include |
| Marker | Results of Immunhistochemistry |
|---|---|
| Smooth muscle actin | +++ |
| Desmin | +++ |
| CD10 | +++ |
| CD34 | + (10% of tumor cells) |
| D2-40 | ++ |
| ERG | +++ |
| INI-1 (nuclear) | +++ |
| TFE3 | + (focal) |
| p53 | wild type |
| Ki-67 | 15–20% |
| ALK1 | − |
| Caldesmon | − |
| Calponin | − |
| ß-Catenin | − |
| CD31 | − |
| EMA | − |
| FosB | − |
| H3K27me3 | − |
| HHV8 | − |
| Muc-4 | unspecific |
| S-100 | − |
| Stat-6 | − |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schenker, A.; Gutjahr, E.; Lehner, B.; Mechtersheimer, G.; Wardelmann, E.; Klotz, R.; Kalkum, E.; Schiltenwolf, M.; Harhaus, L.; Renkawitz, T.; et al. A Systematic Review and Illustrative Case Presentation of Low-Grade Myofibroblastic Sarcoma (LGMS) of the Extremities. J. Clin. Med. 2023, 12, 7027. https://doi.org/10.3390/jcm12227027
Schenker A, Gutjahr E, Lehner B, Mechtersheimer G, Wardelmann E, Klotz R, Kalkum E, Schiltenwolf M, Harhaus L, Renkawitz T, et al. A Systematic Review and Illustrative Case Presentation of Low-Grade Myofibroblastic Sarcoma (LGMS) of the Extremities. Journal of Clinical Medicine. 2023; 12(22):7027. https://doi.org/10.3390/jcm12227027
Chicago/Turabian StyleSchenker, Astrid, Ewgenija Gutjahr, Burkhard Lehner, Gunhild Mechtersheimer, Eva Wardelmann, Rosa Klotz, Eva Kalkum, Marcus Schiltenwolf, Leila Harhaus, Tobias Renkawitz, and et al. 2023. "A Systematic Review and Illustrative Case Presentation of Low-Grade Myofibroblastic Sarcoma (LGMS) of the Extremities" Journal of Clinical Medicine 12, no. 22: 7027. https://doi.org/10.3390/jcm12227027
APA StyleSchenker, A., Gutjahr, E., Lehner, B., Mechtersheimer, G., Wardelmann, E., Klotz, R., Kalkum, E., Schiltenwolf, M., Harhaus, L., Renkawitz, T., & Panzram, B. (2023). A Systematic Review and Illustrative Case Presentation of Low-Grade Myofibroblastic Sarcoma (LGMS) of the Extremities. Journal of Clinical Medicine, 12(22), 7027. https://doi.org/10.3390/jcm12227027