
Association of Tumor Necrosis Factor Inhibitors with the Risk of Nontuberculous Mycobacterial Infection in Patients with Rheumatoid Arthritis: A Nationwide Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Ethical Approval
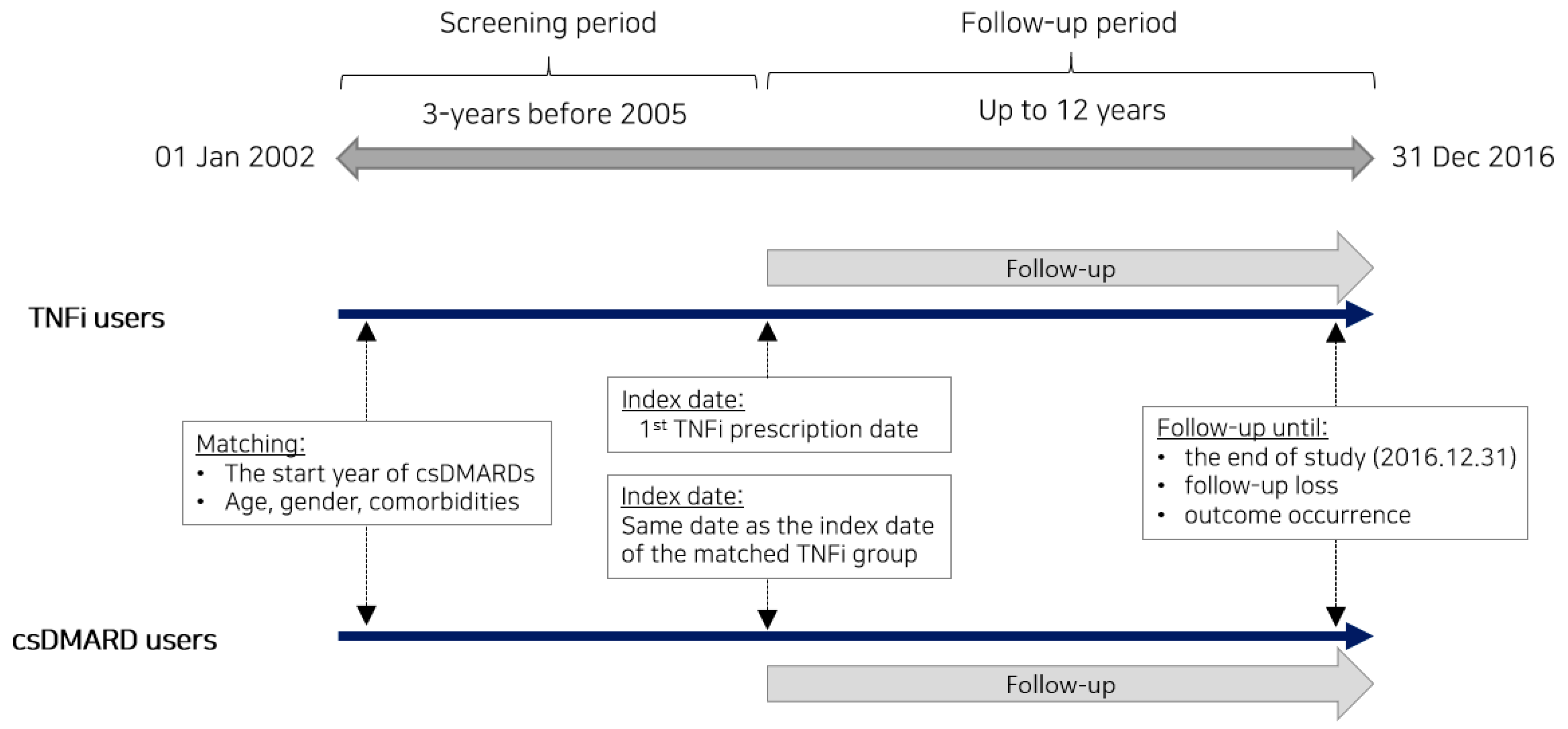
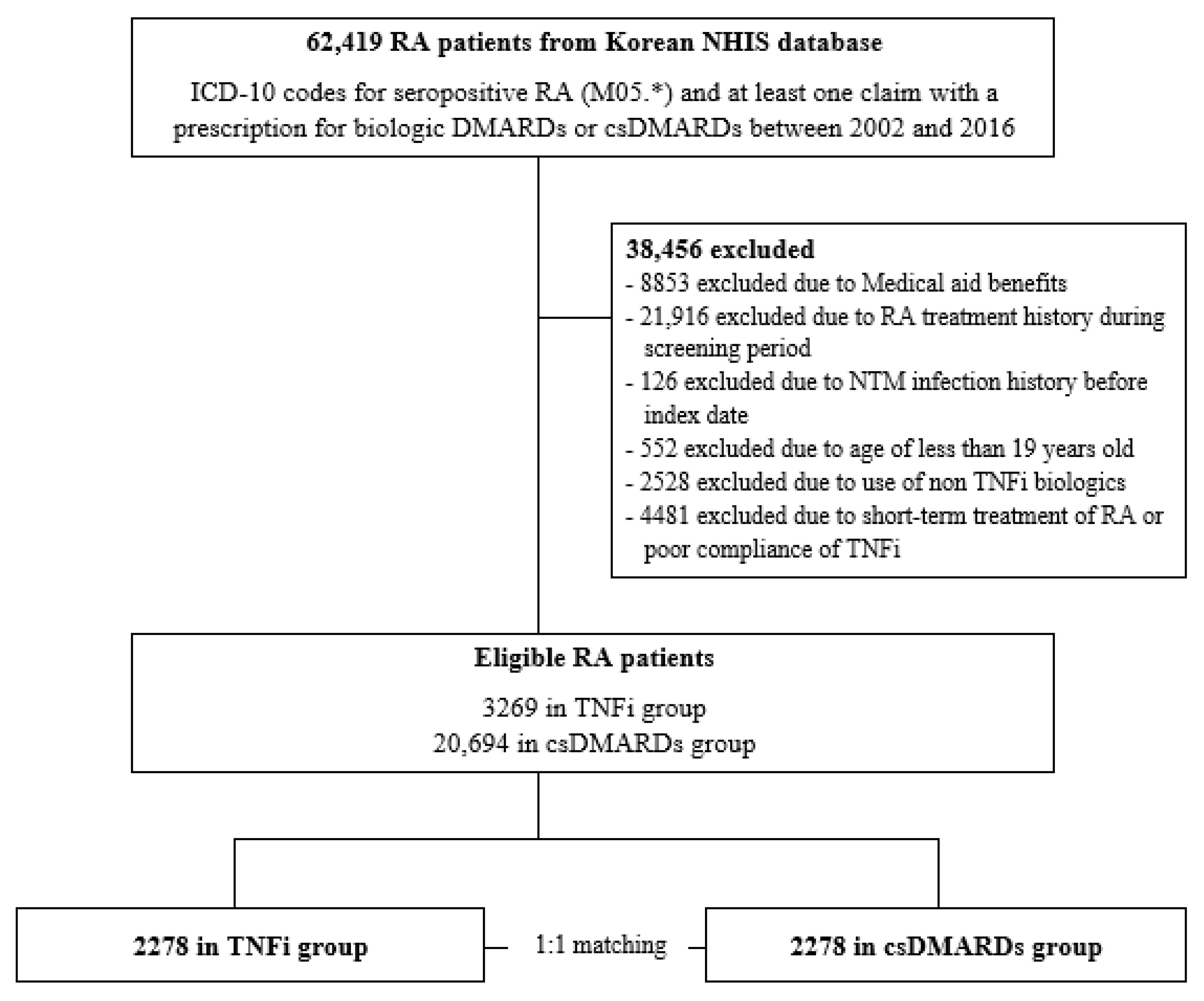
2.3. Study Cohort
2.4. Main Outcome and Confounding Variables
2.5. Statistical Analysis
2.6. Subgroup Analyses and Sensitivity Analysis
3. Results
3.1. Baseline Characteristics
3.2. The Risk of NTM Infection in TNFi Users Compared to csDMARD Users
3.3. Subgroup Analyses and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Bonfiglioli, K.R.; de Medeiros Ribeiro, A.C.; Carnieletto, A.P.; Pereira, I.; Domiciano, D.S.; da Silva, H.C.; Pugliesi, A.; Pereira, L.R.; Guimaraes, M.F.R.; Giorgi, R.D.N.; et al. Extra-articular manifestations of rheumatoid arthritis remain a major challenge: Data from a large, multi-centric cohort. Adv. Rheumatol. 2023, 63, 34. [Google Scholar] [CrossRef]
- Lin, C.T.; Huang, W.N.; Tsai, W.C.; Chen, J.P.; Hung, W.T.; Hsieh, T.Y.; Chen, H.H.; Hsieh, C.W.; Lai, K.L.; Tang, K.T.; et al. Predictors of drug survival for biologic and targeted synthetic DMARDs in rheumatoid arthritis: Analysis from the TRA Clinical Electronic Registry. PLoS ONE 2021, 16, e0250877. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J.S. Diagnosis and Management of Rheumatoid Arthritis: A Review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef]
- Law, S.T.; Taylor, P.C. Role of biological agents in treatment of rheumatoid arthritis. Pharmacol. Res. 2019, 150, 104497. [Google Scholar] [CrossRef]
- Holdsworth, E.A.; Donaghy, B.; Fox, K.M.; Desai, P.; Collier, D.H.; Furst, D.E. Biologic and Targeted Synthetic DMARD Utilization in the United States: Adelphi Real World Disease Specific Programme for Rheumatoid Arthritis. Rheumatol. Ther. 2021, 8, 1637–1649. [Google Scholar] [CrossRef]
- Ruyssen-Witrand, A.; Boudali, Y.; Pane, I.; Cantagrel, A.; Thevenot, P.; Soubrier, M.; Morel, J.; Houvenagel, E.; Saraux, A.; Basch, A.; et al. Changes in etanercept and adalimumab biosimilar prescriptions for the initial treatment of rheumatoid arthritis in France: Data from the ART-SFR Registry. Jt. Bone Spine 2022, 89, 105310. [Google Scholar] [CrossRef]
- Park, S.C.; Kang, M.J.; Han, C.H.; Lee, S.M.; Kim, C.J.; Lee, J.M.; Kang, Y.A. Prevalence, incidence, and mortality of nontuberculous mycobacterial infection in Korea: A nationwide population-based study. BMC Pulm. Med. 2019, 19, 140. [Google Scholar] [CrossRef]
- Ratnatunga, C.N.; Lutzky, V.P.; Kupz, A.; Doolan, D.L.; Reid, D.W.; Field, M.; Bell, S.C.; Thomson, R.M.; Miles, J.J. The Rise of Non-Tuberculosis Mycobacterial Lung Disease. Front. Immunol. 2020, 11, 303. [Google Scholar] [CrossRef]
- Namkoong, H.; Kurashima, A.; Morimoto, K.; Hoshino, Y.; Hasegawa, N.; Ato, M.; Mitarai, S. Epidemiology of Pulmonary Nontuberculous Mycobacterial Disease, Japan. Emerg. Infect. Dis. 2016, 22, 1116–1117. [Google Scholar] [CrossRef]
- Verma, A.K.; Arora, V.K. Non-tuberculous mycobacterial infections in geriatric patients-A neglected and emerging problem. Indian J. Tuberc. 2022, 69 (Suppl. 2), S235–S240. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rheumatoid Arthritis. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/rheumatoid-arthritis (accessed on 15 October 2023).
- Liao, T.L.; Lin, C.F.; Chen, Y.M.; Liu, H.J.; Chen, D.Y. Risk Factors and Outcomes of Nontuberculous Mycobacterial Disease among Rheumatoid Arthritis Patients: A Case-Control study in a TB Endemic Area. Sci. Rep. 2016, 6, 29443. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.J.; Wang, Y.C.; Sung, F.C.; Kao, C.H. Rheumatoid arthritis increases the risk of nontuberculosis mycobacterial disease and active pulmonary tuberculosis. PLoS ONE 2014, 9, e110922. [Google Scholar] [CrossRef] [PubMed]
- Brode, S.K.; Jamieson, F.B.; Ng, R.; Campitelli, M.A.; Kwong, J.C.; Paterson, J.M.; Li, P.; Marchand-Austin, A.; Bombardier, C.; Marras, T.K. Risk of mycobacterial infections associated with rheumatoid arthritis in Ontario, Canada. Chest 2014, 146, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Liao, T.L.; Lin, C.H.; Shen, G.H.; Chang, C.L.; Lin, C.F.; Chen, D.Y. Risk for Mycobacterial Disease among Patients with Rheumatoid Arthritis, Taiwan, 2001–2011. Emerg. Infect. Dis. 2015, 21, 1387–1395. [Google Scholar] [CrossRef]
- Dahl, V.N.; Molhave, M.; Floe, A.; van Ingen, J.; Schon, T.; Lillebaek, T.; Andersen, A.B.; Wejse, C. Global trends of pulmonary infections with nontuberculous mycobacteria: A systematic review. Int. J. Infect. Dis. 2022, 125, 120–131. [Google Scholar] [CrossRef]
- Xu, J.; Li, P.; Zheng, S.; Shu, W.; Pang, Y. Prevalence and risk factors of pulmonary nontuberculous mycobacterial infections in the Zhejiang Province of China. Epidemiol. Infect. 2019, 147, e269. [Google Scholar] [CrossRef]
- Zhang, Z.; Fan, W.; Yang, G.; Xu, Z.; Wang, J.; Cheng, Q.; Yu, M. Risk of tuberculosis in patients treated with TNF-alpha antagonists: A systematic review and meta-analysis of randomised controlled trials. BMJ Open 2017, 7, e012567. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Chang, E.; Yamashita, S.; Iademarco, M.F.; LoBue, P.A. Nontuberculous mycobacteria infections and anti-tumor necrosis factor-alpha therapy. Emerg. Infect. Dis. 2009, 15, 1556–1561. [Google Scholar] [CrossRef]
- Lee, S.K.; Kim, S.Y.; Kim, E.Y.; Jung, J.Y.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; Kang, Y.A. Mycobacterial infections in patients treated with tumor necrosis factor antagonists in South Korea. Lung 2013, 191, 565–571. [Google Scholar] [CrossRef]
- Brode, S.K.; Jamieson, F.B.; Ng, R.; Campitelli, M.A.; Kwong, J.C.; Paterson, J.M.; Li, P.; Marchand-Austin, A.; Bombardier, C.; Marras, T.K. Increased risk of mycobacterial infections associated with anti-rheumatic medications. Thorax 2015, 70, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Park, D.W.; Kim, Y.J.; Sung, Y.K.; Chung, S.J.; Yeo, Y.; Park, T.S.; Lee, H.; Moon, J.Y.; Kim, S.H.; Kim, T.H.; et al. TNF inhibitors increase the risk of nontuberculous mycobacteria in patients with seropositive rheumatoid arthritis in a mycobacterium tuberculosis endemic area. Sci. Rep. 2022, 12, 4003. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.C.; Wu, M.F.; Pan, S.W.; Wu, T.S.; Lai, H.C.; Lin, M.C. Host immune response against environmental nontuberculous mycobacteria and the risk populations of nontuberculous mycobacterial lung disease. J. Formos. Med. Assoc. 2020, 119 (Suppl. 1), S13–S22. [Google Scholar] [CrossRef] [PubMed]
- Squire, J.D.; Libertin, C.R.; Powers, H.; Nelson, J.; Brumble, L.; Laham, F.R.; Agharahimi, A.; Freeman, A.F.; Leiding, J.W. Disseminated mycobacterial infections after tumor necrosis factor inhibitor use, revealing inborn errors of immunity. Int. J. Infect. Dis. 2023, 131, 162–165. [Google Scholar] [CrossRef]
- Seong, C.S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Cho, S.K.; Sung, Y.K.; Choi, C.B.; Kwon, J.M.; Lee, E.K.; Bae, S.C. Development of an algorithm for identifying rheumatoid arthritis in the Korean National Health Insurance claims database. Rheumatol. Int. 2013, 33, 2985–2992. [Google Scholar] [CrossRef]
- McHorney, C.A.; Crivera, C.; Laliberte, F.; Germain, G.; Wynant, W.; Lefebvre, P. Adherence to rivaroxaban versus apixaban among patients with non-valvular atrial fibrillation: Analysis of overall population and subgroups of prior oral anticoagulant users. PLoS ONE 2018, 13, e0194099. [Google Scholar] [CrossRef]
- Verhoef, L.M.; van den Bemt, B.J.; van der Maas, A.; Vriezekolk, J.E.; Hulscher, M.E.; van den Hoogen, F.H.; Jacobs, W.C.; van Herwaarden, N.; den Broeder, A.A. Down-titration and discontinuation strategies of tumour necrosis factor-blocking agents for rheumatoid arthritis in patients with low disease activity. Cochrane Database Syst. Rev. 2019, 5, CD010455. [Google Scholar] [CrossRef]
- Kim, Y.H.; Cho, K.H.; Kim, K.H.; Ryu, E.J.; Han, K.D.; Kim, J.S. Predicting hypertension among Korean cancer survivors: A nationwide population-based study. Eur. J. Cancer Care 2018, 27, e12803. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, H.J.; Lim, H.; Kong, I.G.; Kim, M.; Choi, H.G. Bidirectional association between gastroesophageal reflux disease and depression: Two different nested case-control studies using a national sample cohort. Sci. Rep. 2018, 8, 11748. [Google Scholar] [CrossRef] [PubMed]
- Jallow, A.; Ljunggren, G.; Wandell, P.; Wahlstrom, L.; Carlsson, A.C. HIV-infection and psychiatric illnesses—A double edged sword that threatens the vision of a contained epidemic: The Greater Stockholm HIV Cohort Study. J. Infect. 2017, 74, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Park, I.; Kim, Y.; Choi, Y.; Kim, S.; Kim, E.; Won, S.; Kang, S. Development of Advanced TB Case Classification Model Using NHI Claims Data. J. Digit. Converg. 2013, 11, 289–299. [Google Scholar]
- Dahiya, M.; Eboreime, E.; Hyde, A.; Rahman, S.; Sebastianski, M.; Carbonneau, M.; Tapper, E.B.; Tandon, P. International Classification of Diseases Codes are Useful in Identifying Cirrhosis in Administrative Databases. Dig. Dis. Sci. 2022, 67, 2107–2122. [Google Scholar] [CrossRef]
- Akmatov, M.K.; Ermakova, T.; Holstiege, J.; Steffen, A.; von Stillfried, D.; Batzing, J. Comorbidity profile of patients with concurrent diagnoses of asthma and COPD in Germany. Sci. Rep. 2020, 10, 17945. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Park, H.J.; Kim, S.; Kim, Y.J.; Kim, H.C. Epidemiology and comorbidities in idiopathic pulmonary fibrosis: A nationwide cohort study. BMC Pulm. Med. 2023, 23, 54. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Yoo, K.H.; Rhee, C.K.; Yoon, H.K.; Kim, Y.S.; Lee, S.W.; Oh, Y.M.; Lee, S.D.; Lee, J.H.; Kim, K.J.; et al. Health care use and economic burden of patients with diagnosed chronic obstructive pulmonary disease in Korea. Int. J. Tuberc. Lung Dis. 2014, 18, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Dolomisiewicz, A.; Ali, H.; Roul, P.; Yang, Y.; Cannon, G.W.; Sauer, B.; Baker, J.F.; Mikuls, T.R.; Michaud, K.; England, B.R. Updating and Validating the Rheumatic Disease Comorbidity Index to Incorporate ICD-10-CM Diagnostic Codes. Arthritis Care Res. 2023, 75, 2199–2206. [Google Scholar] [CrossRef] [PubMed]
- Winthrop, K.L.; Baxter, R.; Liu, L.; Varley, C.D.; Curtis, J.R.; Baddley, J.W.; McFarland, B.; Austin, D.; Radcliffe, L.; Suhler, E.; et al. Mycobacterial diseases and antitumour necrosis factor therapy in USA. Ann. Rheum. Dis. 2013, 72, 37–42. [Google Scholar] [CrossRef]
- Takei, H.; Nishina, N.; Namkoong, H.; Suzuki, K.; Uwamino, Y.; Hasegawa, N.; Takeuchi, T. Rheumatoid arthritis with nontuberculous mycobacterial pulmonary disease: A retrospective, single-centre cohort study. Mod. Rheumatol. 2022, 32, 534–540. [Google Scholar] [CrossRef]
- Salt, E.; Wiggins, A.T.; Rayens, M.K.; Huaman, M.A.; Mannino, D.; Schwieterman, P.; Merkley, S.A.; Jones, A.R.; Crofford, L.J. Risk Factors for Targeted Fungal and Mycobacterial Infections in Patients Taking Tumor Necrosis Factor Inhibitors. Arthritis Rheumatol. 2016, 68, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.W.; Jo, K.W.; Kang, B.H.; Kim, M.Y.; Yoo, B.; Lee, C.K.; Kim, Y.G.; Yang, S.K.; Byeon, J.S.; Kim, K.J.; et al. Mycobacterial diseases developed during anti-tumour necrosis factor-alpha therapy. Eur. Respir. J. 2014, 44, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Henkle, E.; Winthrop, K.L. Nontuberculous mycobacteria infections in immunosuppressed hosts. Clin. Chest Med. 2015, 36, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Roach, D.R.; Bean, A.G.; Demangel, C.; France, M.P.; Briscoe, H.; Britton, W.J. TNF regulates chemokine induction essential for cell recruitment, granuloma formation, and clearance of mycobacterial infection. J. Immunol. 2002, 168, 4620–4627. [Google Scholar] [CrossRef]
- Shamaei, M.; Mirsaeidi, M. Nontuberculous Mycobacteria, Macrophages, and Host Innate Immune Response. Infect. Immun. 2021, 89, e0081220. [Google Scholar] [CrossRef]
- Bhandari, S.; Baral, M.R.; Barbery, M.; Rudinskaya, A.; Sostin, O. Hematologic side effects of biologics and kinase inhibitors used in rheumatologic diseases: A review of the current evidence. Ann. Hematol. 2022, 101, 1897–1904. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, G.T.; Suh, Y.S.; Kim, H.O.; Lee, H.N.; Lee, S.G. The Impact of the Amendment of the Korean National Health Insurance Reimbursement Criteria for Anti-tumor Necrosis Factor-α Agents on Treatment Pattern, Clinical Response and Persistence in Patients with Rheumatoid Arthritis. J. Rheum. Dis. 2020, 27, 159–167. [Google Scholar] [CrossRef]
- Accortt, N.A.; Bonafede, M.M.; Collier, D.H.; Iles, J.; Curtis, J.R. Risk of Subsequent Infection Among Patients Receiving Tumor Necrosis Factor Inhibitors and Other Disease-Modifying Antirheumatic Drugs. Arthritis Rheumatol. 2016, 68, 67–76. [Google Scholar] [CrossRef]
- Galloway, J.B.; Hyrich, K.L.; Mercer, L.K.; Dixon, W.G.; Fu, B.; Ustianowski, A.P.; Watson, K.D.; Lunt, M.; Symmons, D.P.; Consortium, B.C.C.; et al. Anti-TNF therapy is associated with an increased risk of serious infections in patients with rheumatoid arthritis especially in the first 6 months of treatment: Updated results from the British Society for Rheumatology Biologics Register with special emphasis on risks in the elderly. Rheumatology 2011, 50, 124–131. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Z.; Wu, X.; Zhou, J.; Meng, D.; Zhu, P. Risk of Adverse Events After Anti-TNF Treatment for Inflammatory Rheumatological Disease. A Meta-Analysis. Front. Pharmacol. 2021, 12, 746396. [Google Scholar] [CrossRef]
- Atzeni, F.; Sarzi-Puttini, P.; Botsios, C.; Carletto, A.; Cipriani, P.; Favalli, E.G.; Frati, E.; Foschi, V.; Gasparini, S.; Giardina, A.; et al. Long-term anti-TNF therapy and the risk of serious infections in a cohort of patients with rheumatoid arthritis: Comparison of adalimumab, etanercept and infliximab in the GISEA registry. Autoimmun. Rev. 2012, 12, 225–229. [Google Scholar] [CrossRef]
- Hur, J.W.; Choe, J.Y.; Kim, D.W.; Kim, H.A.; Kim, S.H.; Kim, W.U.; Kim, Y.S.; Lee, H.S.; Lee, S.H.; Park, S.H.; et al. Rheumatoid arthritis patients fulfilling Korean National Health Insurance reimbursement guidelines for anti-tumor necrosis factor-alpha treatment and comparison to other guidelines. Rheumatol. Int. 2015, 35, 1817–1823. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Matched Cohort | ||
|---|---|---|---|
| TNFi n = 2278 | csDMARDs n = 2278 | SMD | |
| Female gender | 1815 (79.6) | 1815 (79.6) | 0 |
| Age (years) | 51.2 ± 13.04 | 51.2 ± 13.04 | 0 |
| Comorbidities * | |||
| Diabetes | 123 (5.3) | 123 (5.3) | 0 |
| CLD | 200 (8.7) | 200 (8.7) | 0 |
| LD | 329 (14.4) | 329 (14.4) | 0 |
| GERD | 500 (21.9) | 500 (21.9) | 0 |
| ISD | 24 (1.0) | 24 (1.0) | 0 |
| hTB | 1 (0.04) | 1 (0.04) | 0 |
| Number of comorbid diseases | 0 | ||
| 0 | 1320 (57.9) | 1320 (57.9) | |
| 1 | 759 (33.3) | 759 (33.3) | |
| 2 or more | 199 (8.7) | 199 (8.7) | |
| Charlson comorbidity index score | - | ||
| 1 | 702 (30.8) | 753 (33.0) | |
| 2 | 707 (31.0) | 641 (28.1) | |
| 3 or more | 869 (38.1) | 884 (38.8) | |
| Duration of csDMARD treatment before the index date (months) | 35.4 ± 29.92 | 35.3 ± 29.96 | 0.003 |
| TNFi treatment ** | |||
| Adalimumab | 1097 (48.1) | - | |
| Etanercept | 860 (37.7) | - | |
| Golimumab | 279 (12.2) | - | |
| Infliximab | 467 (20.5) | - | |
| Duration of TNFi treatment (months) | 37.7 ± 24.99 | - | |
| PDC of TNFi | 0.98 ± 0.043 | - | |
| csDMARD treatment ** | |||
| Methotrexate | 2130 (93.5) | 1756 (77.0) | |
| Hydroxychloriquine | 1831 (80.3) | 1914 (84.0) | |
| Sulfasalazine | 1595 (70.0) | 1143 (50.1) | |
| Leflunomide | 1263 (55.4) | 872 (38.2) | |
| Number of csDMARDs | 3.6 ± 1.34 | 3.3 ± 1.37 | |
| Duration of csDMARDs (months) | 40.3 ± 26.77 | 35.5 ± 25.98 | |
| PDC of csDMARDs | 0.88 ± 0.284 | 0.80 ± 0.337 | |
| Anti-inflammatory treatment ** | |||
| PDC of oral corticosteroid | 0.75 ± 0.346 | 0.66 ± 0.387 | |
| PDC of NSAIDs | 0.86 ± 0.251 | 0.72 ± 0.351 | |
| Type of institution | - | ||
| Tertiary hospital | 2099 (92.1) | 1539 (67.5) | |
| General hospital | 118 (5.1) | 274 (12.0) | |
| Community hospital/clinics/others | 61 (2.6) | 465 (20.4) | |
| Income levels *** | - | ||
| High | 668 (29.3) | 564 (24.7) | |
| Intermediate | 906 (39.7) | 959 (42.0) | |
| Low | 704 (30.9) | 755 (33.1) | |
| Matched Cohort | ||
|---|---|---|
| TNFi | csDMARDs | |
| NTM infection event number | 22 | 32 |
| IR (1000 person years) | 2.47 | 3.66 |
| Matched Cohort | ||||
|---|---|---|---|---|
| Variables | aHR | 95% CI | p-Value | |
| TNFi treatment | 0.517 | 0.205 | 1.301 | 0.161 |
| Charlson comorbidity index score | 0.703 | 0.323 | 1.528 | 0.373 |
| Duration of csDMARD treatment before the index date (months) | 0.960 | 0.803 | 1.147 | 0.650 |
| RA treatments | ||||
| Number of csDMARDs | 1.775 | 0.750 | 4.202 | 0.191 |
| PDC of csDMARDs | 0.015 | 0.001 | 0.388 | 0.011 |
| PDC of oral corticosteroid | 0.754 | 0.093 | 6.127 | 0.792 |
| PDC of NSAIDs | 5.646 | 0.633 | 50.364 | 0.121 |
| Methotrexate user | 0.427 | 0.059 | 3.112 | 0.401 |
| Hydroxychloroquine user | 1.075 | 0.130 | 8.880 | 0.946 |
| Sulfasalazine user | 0.268 | 0.070 | 1.023 | 0.054 |
| Leflunomide user | 0.864 | 0.198 | 3.772 | 0.845 |
| Income levels | ||||
| High vs. low | 1.309 | 0.332 | 5.158 | 0.701 |
| Intermediate vs. low | 0.347 | 0.097 | 1.238 | 0.103 |
| Variables | aHR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age group * | ||||
| Less than 65 | 0.665 | 0.330 | 1.337 | 0.252 |
| 65 or more | 1.176 | 0.386 | 3.584 | 0.775 |
| Gender * | ||||
| Female | 0.648 | 0.336 | 1.251 | 0.196 |
| Male | 1.591 | 0.317 | 7.982 | 0.572 |
| Duration of csDMARD treatment before the index date (months) * | ||||
| <12 months | 1.069 | 0.366 | 3.121 | 0.903 |
| 12 ≤ months < 36 | 1.415 | 0.491 | 4.084 | 0.520 |
| ≥36 months | 0.349 | 0.116 | 1.047 | 0.060 |
| TNF inhibitor ** | ||||
| Adalimumab | 0.596 | 0.291 | 1.220 | 0.156 |
| Etanercept | 1.351 | 0.417 | 4.377 | 0.616 |
| Infliximab | 1.224 | 0.262 | 5.721 | 0.797 |
| Duration of TNF inhibitor use ** | ||||
| <24 months | 1.051 | 0.320 | 3.454 | 0.935 |
| ≥24 months | 0.635 | 0.317 | 1.271 | 0.199 |
| csDMARDs * | ||||
| Methotrexate | 0.773 | 0.412 | 1.450 | 0.422 |
| Hydroxychloroquine | 0.655 | 0.343 | 1.251 | 0.199 |
| Sulfasalazine | 0.683 | 0.319 | 1.462 | 0.326 |
| Leflunomide | 0.893 | 0.389 | 2.052 | 0.790 |
| Duration of csDMARD use * | ||||
| <18 months | 0.802 | 0.359 | 1.795 | 0.591 |
| ≥18 months | 0.765 | 0.311 | 1.877 | 0.557 |
| Time to NTM infection incidence * | ||||
| <48 months | 1.039 | 0.519 | 2.084 | 0.913 |
| ≥48 months | 0.381 | 0.110 | 1.322 | 0.128 |
| Variables | aHR | 95% CI | p-Value | |
|---|---|---|---|---|
| NTM infection monitoring time | ||||
| 3 months | 0.584 | 0.310 | 1.102 | 0.097 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.J.; Choi, B.; Song, Y.-K.; Oh, Y.-J.; Lee, E.B.; Kim, I.-W.; Oh, J.M. Association of Tumor Necrosis Factor Inhibitors with the Risk of Nontuberculous Mycobacterial Infection in Patients with Rheumatoid Arthritis: A Nationwide Cohort Study. J. Clin. Med. 2023, 12, 6998. https://doi.org/10.3390/jcm12226998
Park HJ, Choi B, Song Y-K, Oh Y-J, Lee EB, Kim I-W, Oh JM. Association of Tumor Necrosis Factor Inhibitors with the Risk of Nontuberculous Mycobacterial Infection in Patients with Rheumatoid Arthritis: A Nationwide Cohort Study. Journal of Clinical Medicine. 2023; 12(22):6998. https://doi.org/10.3390/jcm12226998
Chicago/Turabian StylePark, Hyun Jin, Boyoon Choi, Yun-Kyoung Song, Yoon-Jeong Oh, Eun Bong Lee, In-Wha Kim, and Jung Mi Oh. 2023. "Association of Tumor Necrosis Factor Inhibitors with the Risk of Nontuberculous Mycobacterial Infection in Patients with Rheumatoid Arthritis: A Nationwide Cohort Study" Journal of Clinical Medicine 12, no. 22: 6998. https://doi.org/10.3390/jcm12226998
APA StylePark, H. J., Choi, B., Song, Y.-K., Oh, Y.-J., Lee, E. B., Kim, I.-W., & Oh, J. M. (2023). Association of Tumor Necrosis Factor Inhibitors with the Risk of Nontuberculous Mycobacterial Infection in Patients with Rheumatoid Arthritis: A Nationwide Cohort Study. Journal of Clinical Medicine, 12(22), 6998. https://doi.org/10.3390/jcm12226998