

Endovascular Embolization for Epistaxis: A Single Center Experience and Meta-Analysis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Series
2.1.1. Patient Population
2.1.2. Procedure
2.1.3. Outcomes
2.2. Meta Analysis
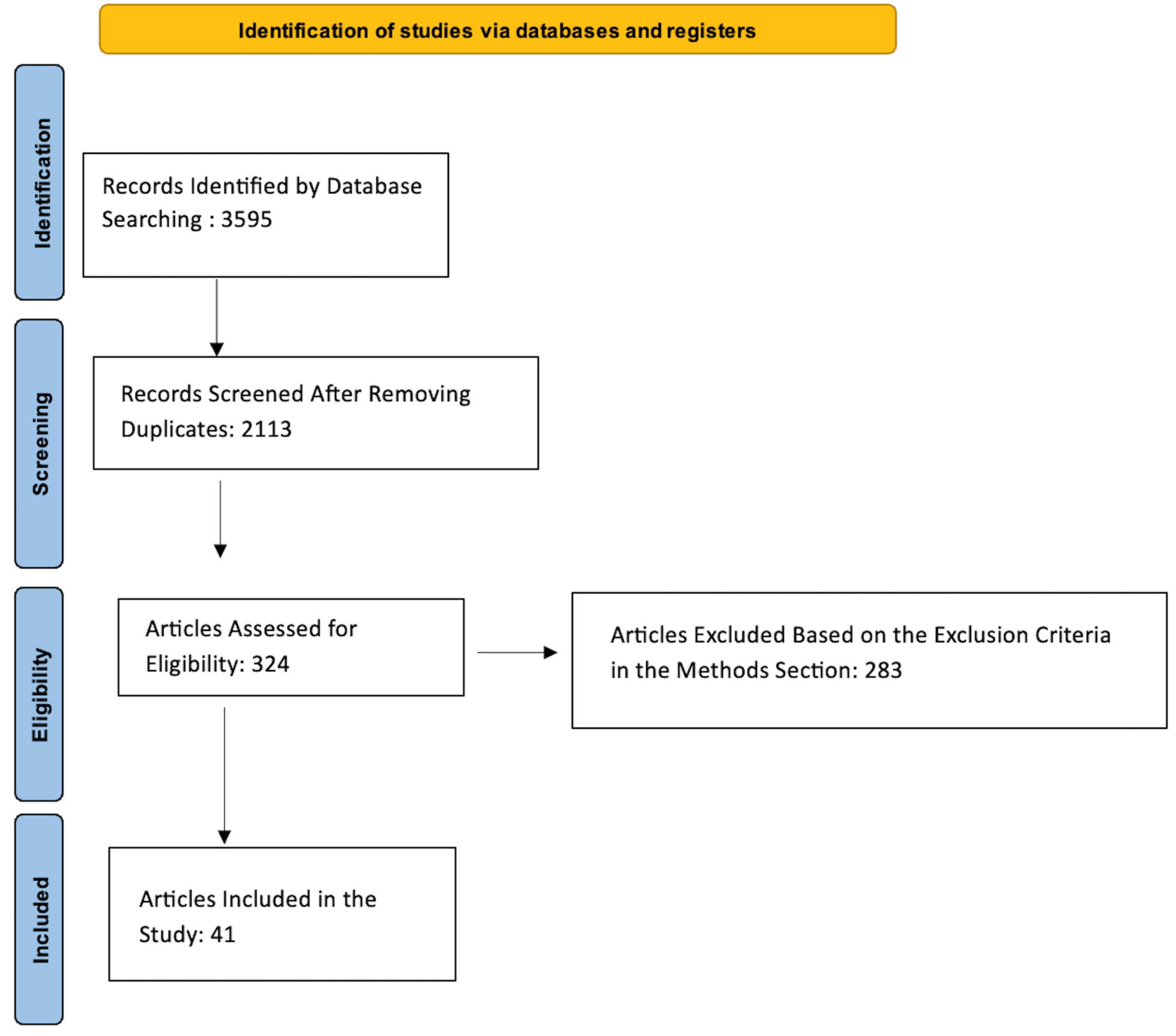
2.2.1. Literature Search
2.2.2. Outcomes
2.2.3. Statistical Analysis
3. Results
3.1. Case Series
3.2. Meta-Analysis
3.2.1. Patient Demographics
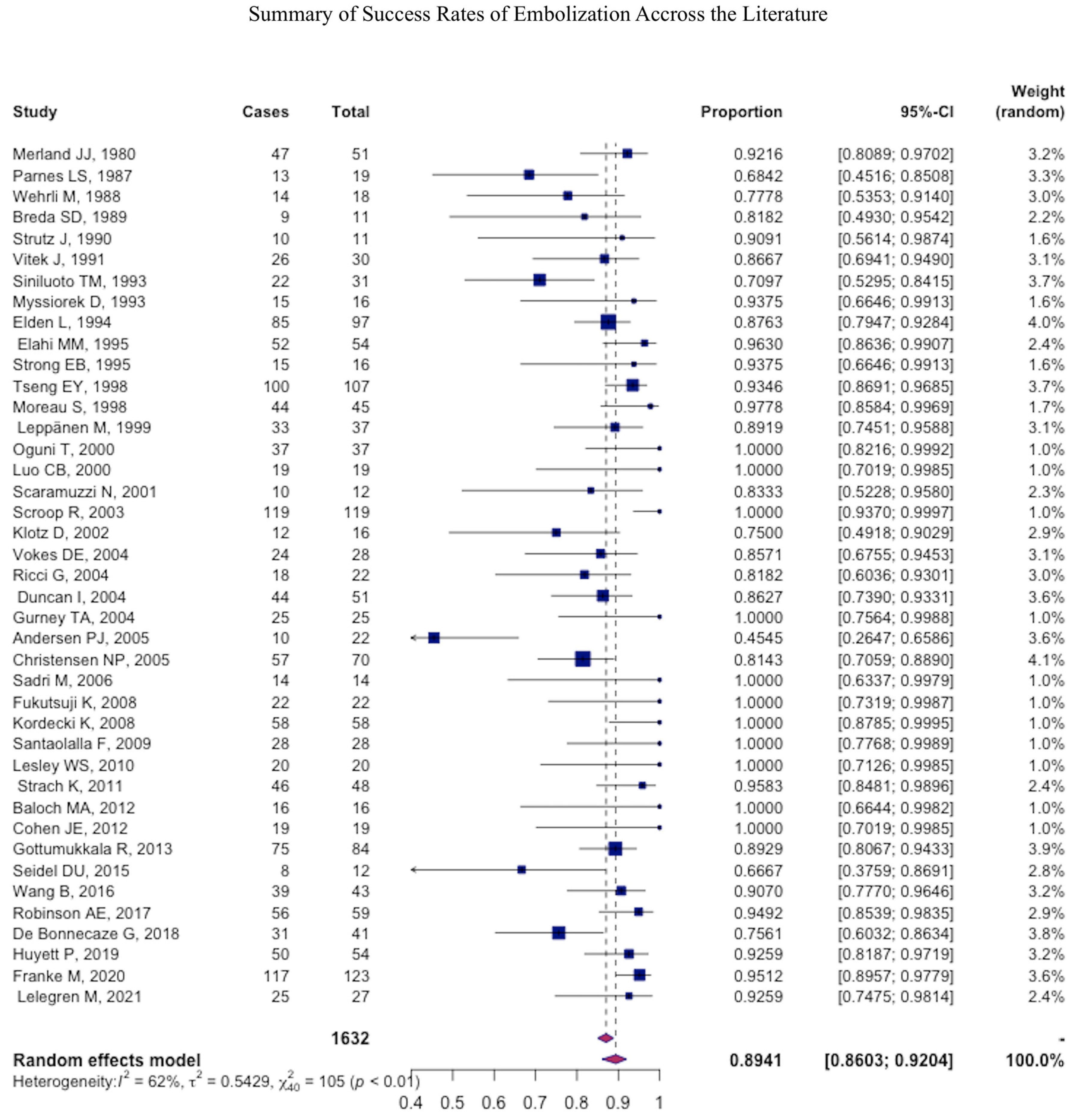
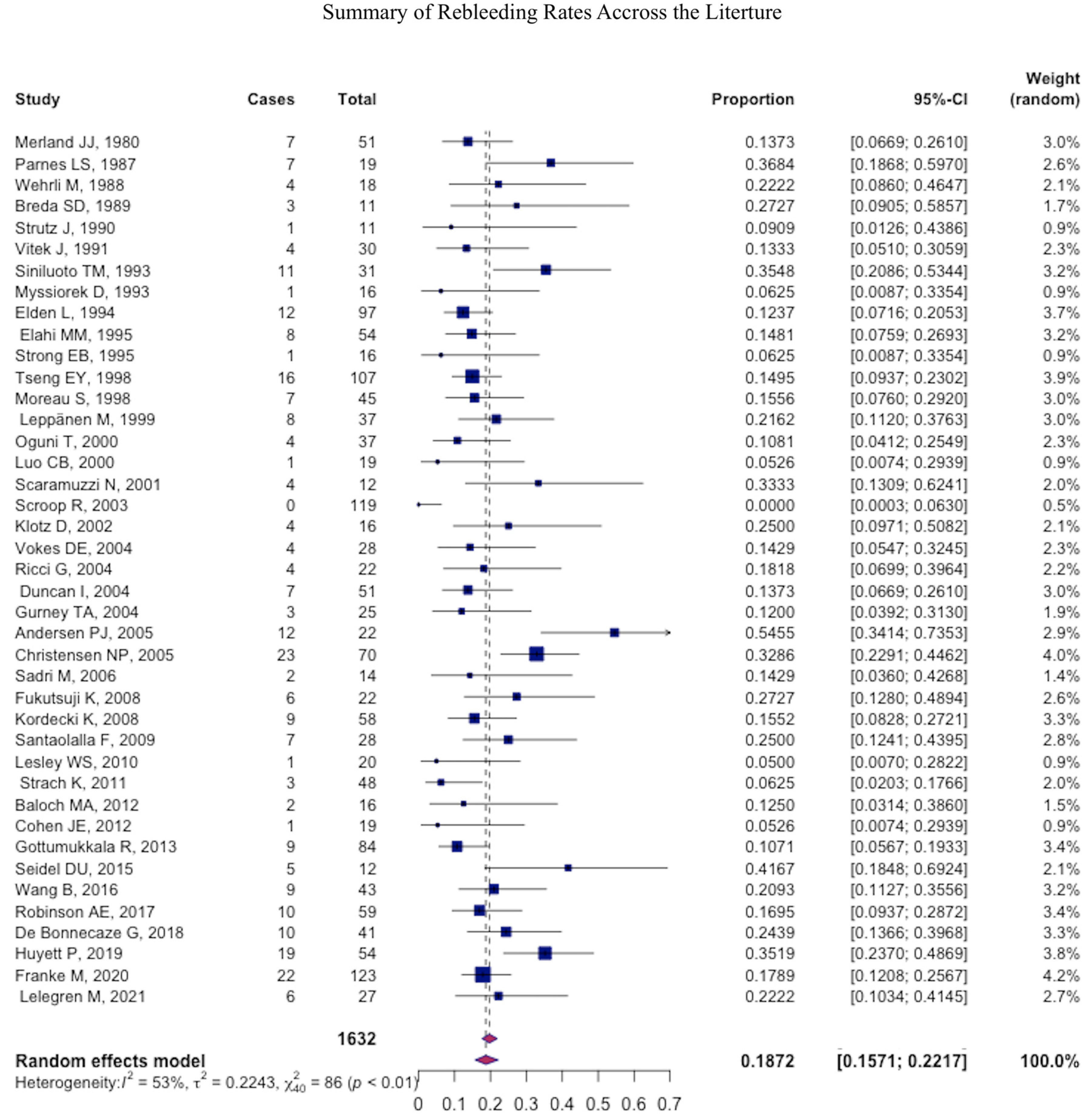
3.2.2. Outcomes
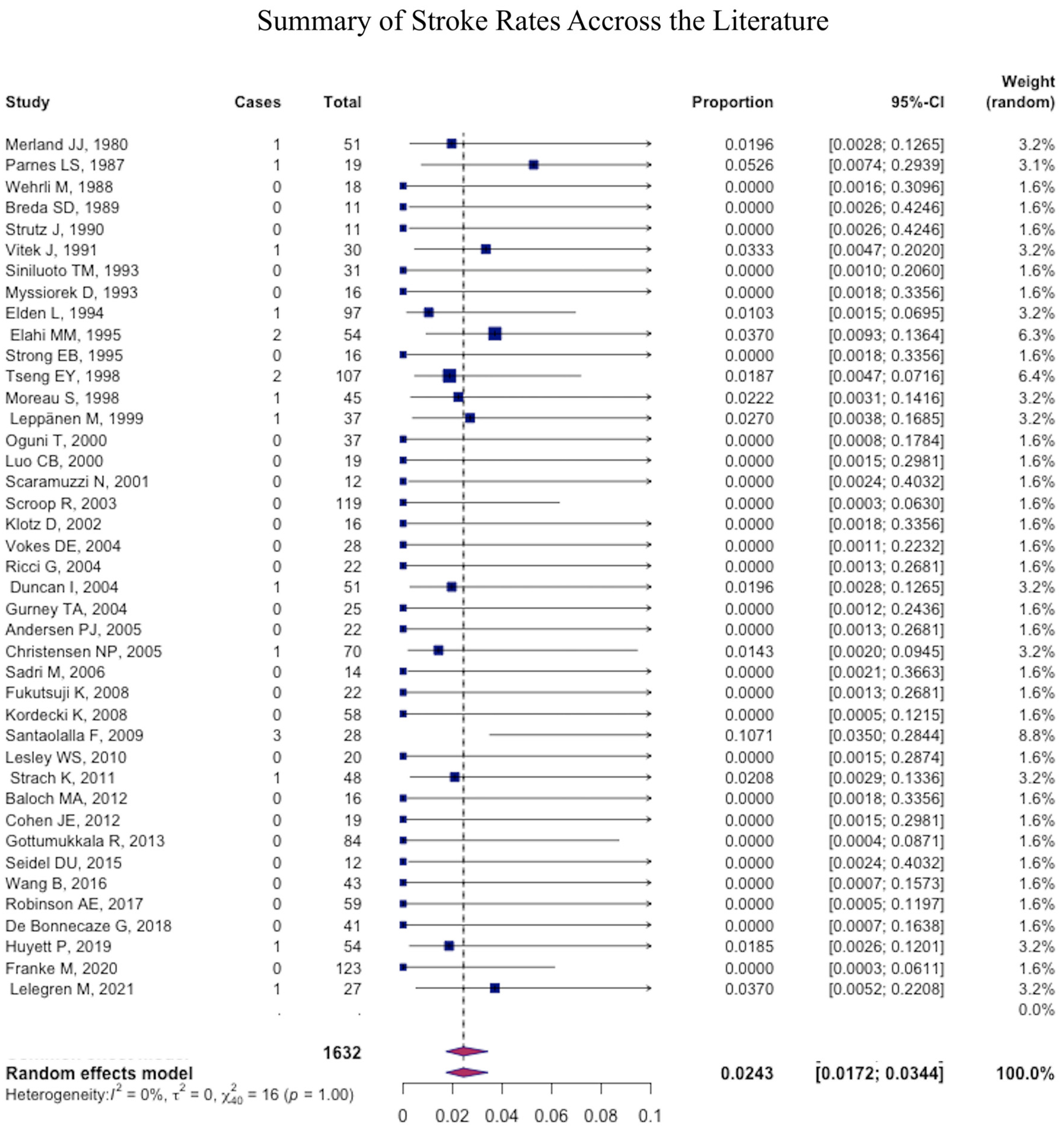
3.2.3. Complications
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schlosser, R.J. Clinical practice. Epistaxis. N. Engl. J. Med. 2009, 360, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Womack, J.P.; Kropa, J.; Jimenez Stabile, M. Epistaxis: Outpatient Management. Am. Fam. Physician 2018, 98, 240–245. [Google Scholar] [PubMed]
- Robinson, A.E.; McAuliffe, W.; Phillips, T.J.; Phatouros, C.C.; Singh, T.P. Embolization for the treatment of intractable epistaxis: 12 month outcomes in a two centre case series. Br. J. Radiol. 2017, 90, 20170472. [Google Scholar] [CrossRef] [PubMed]
- Zayyan, E.; Bajin, M.D.; Aytemir, K.; Yılmaz, T. The effects on cardiac functions and arterial blood gases of totally occluding nasal packs and nasal packs with airway. Laryngoscope 2010, 120, 2325–2330. [Google Scholar] [CrossRef]
- McDonald, T.J.; Pearson, B.W. Follow-up on maxillary artery ligation for epistaxis. Arch. Otolaryngol. 1980, 106, 635–638. [Google Scholar] [CrossRef]
- Fukutsuji, K.; Nishiike, S.; Aihara, T.; Uno, M.; Harada, T.; Gyoten, M.; Imai, S. Superselective angiographic embolization for intractable epistaxis. Acta Otolaryngol. 2008, 128, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Elden, L.; Montanera, W.; Terbrugge, K.; Willinsky, R.; Lasjaunias, P.; Charles, D. Angiographic embolization for the treatment of epistaxis: A review of 108 cases. Otolaryngol. Head Neck Surg. 1994, 111, 44–50. [Google Scholar] [CrossRef]
- Strach, K.; Schröck, A.; Wilhelm, K.; Greschus, S.; Tschampa, H.; Möhlenbruch, M.; Naehle, C.P.; Jakob, M.; Gerstner, A.O.; Bootz, F.; et al. Endovascular treatment of epistaxis: Indications, management, and outcome. Cardiovasc. Interv. Radiol. 2011, 34, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Vitek, J. Idiopathic intractable epistaxis: Endovascular therapy. Radiology 1991, 181, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Vokes, D.E.; McIvor, N.P.; Wattie, W.J.; Chaplin, J.M.; Morton, R.P. Endovascular treatment of epistaxis. ANZ J. Surg. 2004, 74, 751–753. [Google Scholar] [CrossRef]
- Leppänen, M.; Seppänen, S.; Laranne, J.; Kuoppala, K. Microcatheter embolization of intractable idiopathic epistaxis. Cardiovasc. Interv. Radiol. 1999, 22, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Brinjikji, W.; Kallmes, D.F.; Cloft, H.J. Trends in epistaxis embolization in the United States: A study of the Nationwide Inpatient Sample 2003–2010. J. Vasc. Interv. Radiol. 2013, 24, 969–973. [Google Scholar] [CrossRef]
- Reyre, A.; Michel, J.; Santini, L.; Dessi, P.; Vidal, V.; Bartoli, J.M.; Moulin, G.; Varoquaux, A. Epistaxis: The role of arterial embolization. Diagn Interv. Imaging 2015, 96, 757–773. [Google Scholar] [CrossRef] [PubMed]
- Strong, E.B.; Bell, D.A.; Johnson, L.P.; Jacobs, J.M. Intractable epistaxis: Transantral ligation vs. embolization: Efficacy review and cost analysis. Otolaryngol. Head Neck Surg. 1995, 113, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Seidel, D.U.; Remmert, S.; Brassel, F.; Schlunz-Hendann, M.; Meila, D. Superselective microcoil embolization in severe intractable epistaxis: An analysis of 12 consecutive cases from an otorhinolaryngologic and an interventional neuroradiologic point of view. Eur. Arch. Otorhinolaryngol. 2015, 272, 3317–3326. [Google Scholar] [CrossRef]
- Merland, J.J.; Melki, J.P.; Chiras, J.; Riche, M.C.; Hadjean, E. Place of embolization in the treatment of severe epistaxis. Laryngoscope 1980, 90, 1694–1704. [Google Scholar] [CrossRef]
- Parnes, L.S.; Heeneman, H.; Vinuela, F. Percutaneous embolization for control of nasal blood circulation. Laryngoscope 1987, 97, 1312–1315. [Google Scholar] [CrossRef]
- Wehrli, M.; Lieberherr, U.; Valavanis, A. Superselective embolization for intractable epistaxis: Experiences with 19 patients. Clin. Otolaryngol. Allied. Sci. 1988, 13, 415–420. [Google Scholar] [CrossRef]
- Breda, S.D.; Choi, I.S.; Persky, M.S.; Weiss, M. Embolization in the treatment of epistaxis after failure of internal maxillary artery ligation. Laryngoscope 1989, 99, 809–813. [Google Scholar] [CrossRef]
- Strutz, J.; Schumacher, M. Uncontrollable epistaxis. Angiographic localization and embolization. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 697–699. [Google Scholar] [CrossRef]
- Siniluoto, T.M.; Leinonen, A.S.; Karttunen, A.I.; Karjalainen, H.K.; Jokinen, K.E. Embolization for the treatment of posterior epistaxis. An analysis of 31 cases. Arch. Otolaryngol. Head Neck Surg. 1993, 119, 837–841. [Google Scholar] [CrossRef] [PubMed]
- Myssiorek, D.; Lodespoto, M. Embolization of Posterior Epistaxis. Am. J. Rhinol. 1993, 7, 223–226. [Google Scholar] [CrossRef]
- Elahi, M.M.; Parnes, L.S.; Fox, A.J.; Pelz, D.M.; Lee, D.H. Therapeutic Embolization in the Treatment of Intractable Epistaxis. Arch. Otolaryngol.-Head Neck Surg. 1995, 121, 65–69. [Google Scholar] [CrossRef]
- Tseng, E.Y.; Narducci, C.A.; Willing, S.J.; Sillers, M.J. Angiographic embolization for epistaxis: A review of 114 cases. Laryngoscope 1998, 108, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Moreau, S.; De Rugy, M.G.; Babin, E.; Courtheoux, P.; Valdazo, A. Supraselective embolization in intractable epistaxis: Review of 45 cases. Laryngoscope 1998, 108, 887–888. [Google Scholar] [CrossRef] [PubMed]
- Oguni, T.; Korogi, Y.; Yasunaga, T.; Sadanaga, T.; Uozumi, H.; Kawanaka, K.; Sumi, S.; Takahashi, M. Superselective embolisation for intractable idiopathic epistaxis. Br. J. Radiol. 2000, 73, 1148–1153. [Google Scholar] [CrossRef]
- Luo, C.B.; Teng, M.M.; Lirng, J.F.; Chang, F.C.; Chen, S.S.; Guo, W.Y.; Chang, C.Y. Endovascular embolization of intractable epistaxis. Chin. Med. J. 2000, 63, 205–212. [Google Scholar]
- Scaramuzzi, N.; Walsh, R.M.; Brennan, P.; Walsh, M. Treatment of intractable epistaxis using arterial embolization. Clin. Otolaryngol. Allied. Sci. 2001, 26, 307–309. [Google Scholar] [CrossRef]
- Klotz, D.A.; Winkle, M.R.; Richmon, J.; Hengerer, A.S. Surgical management of posterior epistaxis: A changing paradigm. Laryngoscope 2002, 112, 1577–1582. [Google Scholar] [CrossRef]
- Scroop, R.; Venturini, C.; Song, J.; Eskridge, J.M. Endovascular Treatment of Epistaxis. Semin. Interv. Radiol. 2003, 20, 051–058. [Google Scholar] [CrossRef]
- Ricci, G.; Molini, E.; Hamam, M.; Ciorba, A.; Altissimi, G.; Campanella, S.; Fiacca, A.; Pelliccioli, G. Treatment of severe epistaxis by superselective embolization: A review of 22 cases. Rev. Laryngol Otol. Rhinol. (Bord.) 2004, 125, 247–251. [Google Scholar] [PubMed]
- Duncan, I.C.; Fourie, P.A.; le Grange, C.E.; van der Walt, H.A. Endovascular treatment of intractable epistaxis--results of a 4-year local audit. S. Afr. Med. J. 2004, 94, 373–378. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gurney, T.A.; Dowd, C.F.; Murr, A.H. Embolization for the treatment of idiopathic posterior epistaxis. Am. J. Rhinol. 2004, 18, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.J.; Kjeldsen, A.D.; Nepper-Rasmussen, J. Selective embolization in the treatment of intractable epistaxis. Acta Otolaryngol. 2005, 125, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Christensen, N.P.; Smith, D.S.; Barnwell, S.L.; Wax, M.K. Arterial embolization in the management of posterior epistaxis. Otolaryngol. Head Neck Surg. 2005, 133, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Sadri, M.; Midwinter, K.; Ahmed, A.; Parker, A. Assessment of safety and efficacy of arterial embolisation in the management of intractable epistaxis. Eur. Arch. Otorhinolaryngol. 2006, 263, 560–566. [Google Scholar] [CrossRef]
- Kordecki, K.; Janica, J.; Lewszuk, A.; Lebkowska, U.; Ustymowicz, A. Embolization of carotid artery branch in intractable epistaxis. Pol. J. Radiol. 2008, 73, 39–42. [Google Scholar]
- Santaolalla, F.; Araluce, I.; Zabala, A.; López, A.; Garay, M.; Sanchez, J.M. Efficacy of selective percutaneous embolization for the treatment of intractable posterior epistaxis and juvenile nasopharyngeal angiofibroma (JNA). Acta Otolaryngol. 2009, 129, 1456–1462. [Google Scholar] [CrossRef]
- Lesley, W.S.; Rangaswamy, R.; Patel, D.V. Results of epistaxis embosurgery using detachable platinum fibered coils. J. Neurointerv. Surg. 2010, 2, 171–175. [Google Scholar] [CrossRef]
- Baloch, M.A.; Awan, M.S.; Resident, H.N. Angioembolization in itractable epistaxis—A tertiary care experience. J. Pak. Med. Assoc. 2012, 62, 254–256. [Google Scholar]
- Cohen, J.E.; Moscovici, S.; Gomori, J.M.; Eliashar, R.; Weinberger, J.; Itshayek, E. Selective endovascular embolization for refractory idiopathic epistaxis is a safe and effective therapeutic option: Technique, complications, and outcomes. J. Clin. Neurosci. 2012, 19, 687–690. [Google Scholar] [CrossRef] [PubMed]
- Gottumukkala, R.; Kadkhodayan, Y.; Moran, C.J.; Cross de, W.T., 3rd; Derdeyn, C.P. Impact of vessel choice on outcomes of polyvinyl alcohol embolization for intractable idiopathic epistaxis. J. Vasc. Interv. Radiol. 2013, 24, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zu, Q.Q.; Liu, X.L.; Zhou, C.G.; Xia, J.G.; Zhao, L.B.; Shi, H.B.; Liu, S. Transarterial embolization in the management of intractable epistaxis: The angiographic findings and results based on etiologies. Acta Otolaryngol. 2016, 136, 864–868. [Google Scholar] [CrossRef] [PubMed]
- de Bonnecaze, G.; Gallois, Y.; Bonneville, F.; Vergez, S.; Chaput, B.; Serrano, E. Transnasal Endoscopic Sphenopalatine Artery Ligation Compared With Embolization for Intractable Epistaxis: A Long-term Analysis. Am. J. Rhinol. Allergy. 2018, 32, 188–193. [Google Scholar] [CrossRef]
- Huyett, P.; Jankowitz, B.T.; Wang, E.W.; Snyderman, C.H. Endovascular embolization in the treatment of epistaxis. Otolaryngol. Head Neck Surg. 2019, 160, 822–828. [Google Scholar] [CrossRef]
- Franke, M.; Franke, J.; Saager, C.; Barthel, S.; Riemann, R.; Mueckner, K. Not all embolizations are created equally in the management of posterior epistaxis: Discussion of safety mea- sures avoiding neurological complications. Radiol. Res. Pract. 2020, 2020, 5710313. [Google Scholar] [CrossRef]
- Lelegren, M.; Bhat, K.; Sheehan, B.; Lamichhane, R.; Han, J.K.; Lam, K.K. Variations in utilization and clinical outcomes for endoscopic sphenopalatine artery ligation and endovascular arterial embolization in a single multi-hospital network. Am. J. Otolaryngol. 2021, 42, 103066. [Google Scholar] [CrossRef]
- Cullen, M.M.; Tami, T.A. Comparison of internal maxillary artery ligation versus embolization for refractory posterior epistaxis. Otolaryngol. Head Neck Surg. 1998, 118, 636–642. [Google Scholar] [CrossRef]
- Hoffman, H.; Ashok Kumar, A.; Raventhiranathan, N.; Masoud, H.E.; Gould, G.C. Endovascular embolization for the treatment of epistaxis: Systematic review and meta-analysis. Interv. Neuroradiol. 2023, 29, 172–182. [Google Scholar] [CrossRef]
- Shaw, C.B.; Wax, M.K.; Wetmore, S.J. Epistaxis: A comparison of treatment. Otolaryngol. Head Neck Surg. 1993, 109, 60–65. [Google Scholar] [CrossRef]
- Sokoloff, J.; Wickbom, I.; McDonald, D.; Brahme, F.; Goergen, T.C.; Goldberger, L.E. Therapeutic percutaneous embolization in intractable epistaxis. Radiology 1974, 111, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, M.J.; Chung, S.Y.; Guinand, L.A.; Govindan, A.; Baredes, S.; Eloy, J.A. Arterial ligation versus embolization in epistaxis management: Counterintuitive national trends. Laryngoscope 2017, 127, 1017–1020. [Google Scholar] [CrossRef] [PubMed]
- McDermott, A.M.; O’Cathain, E.; Carey, B.W.; O’Sullivan, P.; Sheahan, P. Sphenopalatine Artery Ligation for Epistaxis: Factors Influencing Outcome and Impact of Timing of Surgery. Otolaryngol. Head Neck Surg. 2016, 154, 547–552. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | N (%) Mean (SD, 95% CI, Range) |
|---|---|
| Number of patients | 35 |
| Number of procedures | 40 |
| Number of Arteries embolized | 44 |
| Number of procedures per patient | |
| 30 patients | 1 procedure |
| 4 patients | 2 procedures |
| 1 patient | 3 procedures |
| Age | 66.3 ± 15.4; 95% 61.96–72.56 |
| Gender (Male) | 19 (54.3) |
| Smokers | 2 (5.7) |
| Hypertension | 20 (57.1) |
| Antiplatelet | 14 (40) |
| Single | 10 (28.6) |
| Dual | 4 (11.4) |
| Anticoagulation | 11 (31.4) |
| Bleeding Diathesis | 4 (11.4) |
| Recreational Drugs | 4 (11.4) |
| Previous Surgical Treatment | 33 (94.3) |
| Number of vessels embolized | 1.9 ± 0.9; 95% CI 1.6–2.2 |
| Time From failed SPA Ligation to embolization (days) | 19.1 ± 31.8, 95% CI: 31.8–6.42, 1–148 |
| Laterality | |
| Left | 9 (22.5) |
| Right | 7 (17.5) |
| Bilateral | 24 (60) |
| Arteries Embolized | |
| Internal Maxillary Artery | 38 (86.4) |
| Facial Artery | 6 (13.6) |
| Procedural Complications | 0 |
| Catheters Used | |
| Scepter | 3 (7.5) |
| SL-10 | 20 (50) |
| Echelon | 6 (15) |
| Duo Microcatheter | 5 (12.5) |
| Marathon | 4 (10) |
| Prowler | 1 (2.5) |
| Turbo Track 18 | 1 (2.5) |
| Embolisate | |
| Onyx | 18 (45) |
| Particles | 8 (20) |
| Combination | 14 (35) |
| Complications | |
| Stoke (minor, major) | 0 |
| Vision Change | 5 (12.5) |
| Retroperitoneal Hemorrhage | 0 |
| Groin Hematoma | 1 (2.5) |
| Failed Arterial Access | 0 |
| Palatal Ulcers | 1 (2.5) |
| Nasal/Facial Pain | 8 (20) |
| Nasal/Facial/Palatal Numbness | 5 (12.5) |
| Immediate Success | 39 (97.5) |
| Rebleed | 3 (7.5) |
| Mortality | 0 |
| Length of Follow-up (months) | 17.85 ± 21.79; 95% CI 10.4–25.3 |
| Study/Year | Patients, N | Age, Mean | Male (%) |
|---|---|---|---|
| Merland et al., 1980 [16] | 51 | - | - |
| Parnes et al., 1987 [17] | 19 | - | - |
| Wehrli et al., 1988 [18] | 18 | 57 | 61.1 |
| Breda et al., 1989 [19] | 11 | 56 | 54.5 |
| Strutz et al., 1990 [20] | 11 | 48 | 45.5 |
| Vitek et al., 1991 [9] | 30 | 62 | 70 |
| Siniluoto et al., 1993 [21] | 31 | 49 | 83.9 |
| Myssoirek et al., 1993 [22] | 16 | 40 | 68.8 |
| Elden et al., 1994 [7] | 97 | 53 | 66 |
| Elahi et al., 1995 [23] | 54 | 53 | 63 |
| Strong et al., 1995 [14] | 16 | 61 | 81.3 |
| Tseng et al., 1998 [24] | 107 | 55 | - |
| Moreau et al., 1998 [25] | 45 | 49 | 75.6 |
| Leppänen et al., 1999 [11] | 37 | 53 | 78.4 |
| Oguni et al., 2000 [26] | 37 | 57 | 83.8 |
| Luo et al., 2000 [27] | 19 | 38 | 78.9 |
| Scaramuzzi et al., 2001 [28] | 12 | 51 | 83.3 |
| Klotz et al., 2002 [29] | 16 | - | - |
| Scroop et al., 2003 [30] | 119 | - | 83.2 |
| Vokes et al., 2004 [10] | 28 | 55 | 64.3 |
| Ricci et al., 2004 [31] | 22 | 62 | 63.6 |
| Duncan et al., 2004 [32] | 51 | 54 | 54.9 |
| Gurney et al., 2004 [33] | 25 | 67 | 60 |
| Anderson et al., 2005 [34] | 22 | 59 | 72.7 |
| Christensen et al., 2005 [35] | 70 | 59 | 58.6 |
| Sadri et al., 2006 [36] | 14 | 57 | 85.7 |
| Fukutsuji et al., 2008 [6] | 22 | 57 | 95.5 |
| Kordecki et al., 2008 [37] | 58 | - | |
| Santaolalla et al., 2009 [38] | 28 | 60 | 89.3 |
| Lesley et al., 2010 [39] | 20 | 63 | 65 |
| Strach et al., 2011 [8] | 48 | 57 | 75 |
| Baloch et al., 2012 [40] | 16 | 51 | 87.5 |
| Cohen et al., 2012 [41] | 19 | 61 | 89.5 |
| Gottumukkala et al., 2013 [42] | 84 | 64 | 56 |
| Seidel et al., 2015 [15] | 12 | 58 | 75 |
| Wang et al., 2016 [43] | 43 | 46 | 88.4 |
| Robinson et al., 2017 [3] | 59 | 59 | 72.9 |
| de Bonnecaze et al., 2018 [44] | 41 | 66 | - |
| Huyett et al., 2019 [45] | 54 | 65 | 66.7 |
| Franke et al., 2020 [46] | 123 | 66 | 65 |
| Lelegren et al., 2021 [47] | 27 | 64 | 59.3 |
| Pooled Estimate †, CI | - | 57.5 (57.2–57.8) | 70.4 (69.8–71.0) |
| Study/Year | Immediate Success (%) | Rebleed (%) |
|---|---|---|
| Merland et al., 1980 [16] | 92.2 | 13.7 |
| Parnes et al., 1987 [17] | 68.4 | 36.8 |
| Wehrli et al., 1988 [18] | 77.8 | 22.2 |
| Breda et al., 1989 [19] | 81.8 | 27.3 |
| Strutz et al., 1990 [20] | 90.9 | 9.1 |
| Vitek et al., 1991 [9] | 86.7 | 13.3 |
| Siniluoto et al., 1993 [21] | 71 | 35.4 |
| Myssoirek et al., 1993 [22] | 93.8 | 6.3 |
| Elden et al., 1994 [7] | 87.6 | 12.4 |
| Elahi et al., 1995 [23] | 96.3 | 14.8 |
| Strong et al., 1995 [14] | 93.8 | 6.3 |
| Tseng et al., 1998 [24] | 92.5 | 15 |
| Moreau et al., 1998 [25] | 97.8 | 15.6 |
| Leppänen et al., 1999 [11] | 89.2 | 21.6 |
| Oguni et al., 2000 [26] | 100 | 10.8 |
| Luo et al., 2000 [27] | 100 | 5.3 |
| Scaramuzzi et al., 2001 [28] | 83.3 | 33.3 |
| Klotz et al., 2002 [29] | 75 | 25 |
| Scroop et al., 2003 [30] | 100 | 0 |
| Vokes et al., 2004 [10] | 85.7 | 14.3 |
| Ricci et al., 2004 [31] | 81.8 | 18.2 |
| Duncan et al., 2004 [32] | 86.3 | 13.7 |
| Gurney et al., 2004 [33] | 100 | 12 |
| Anderson et al., 2005 [34] | 45.5 | 54.5 |
| Christensen et al., 2005 [35] | 81.4 | 32.9 |
| Sadri et al., 2006 [36] | 100 | 14.3 |
| Fukutsuji et al., 2008 [6] | 100 | 27.3 |
| Kordecki et al., 2008 [37] | 100 | 15.5 |
| Santaolalla et al., 2009 [38] | 100 | 25 |
| Lesley et al., 2010 [39] | 100 | 5 |
| Strach et al., 2011 [8] | 95.8 | 6.3 |
| Baloch et al., 2012 [40] | 100 | 12.5 |
| Cohen et al., 2012 [41] | 100 | 5.3 |
| Gottumukkala et al., 2013 [42] | 89.3 | 10.7 |
| Seidel et al., 2015 [15] | 66.7 | 41.7 |
| Wang et al., 2016 [43] | 90.7 | 20.9 |
| Robinson et al., 2017 [3] | 94.9 | 16.9 |
| de Bonnecaze et al., 2018 [44] | 75.6 | 24.4 |
| Huyett et al., 2019 [45] | 92.6 | 35.2 |
| Franke et al., 2020 [46] | 95.1 | 17.9 |
| Lelegren et al., 2021 [47] | 92.6 | 22.2 |
| Pooled Estimate (CI) | 90.9 (90.4–91.4) | 17 (16.5–17.5) |
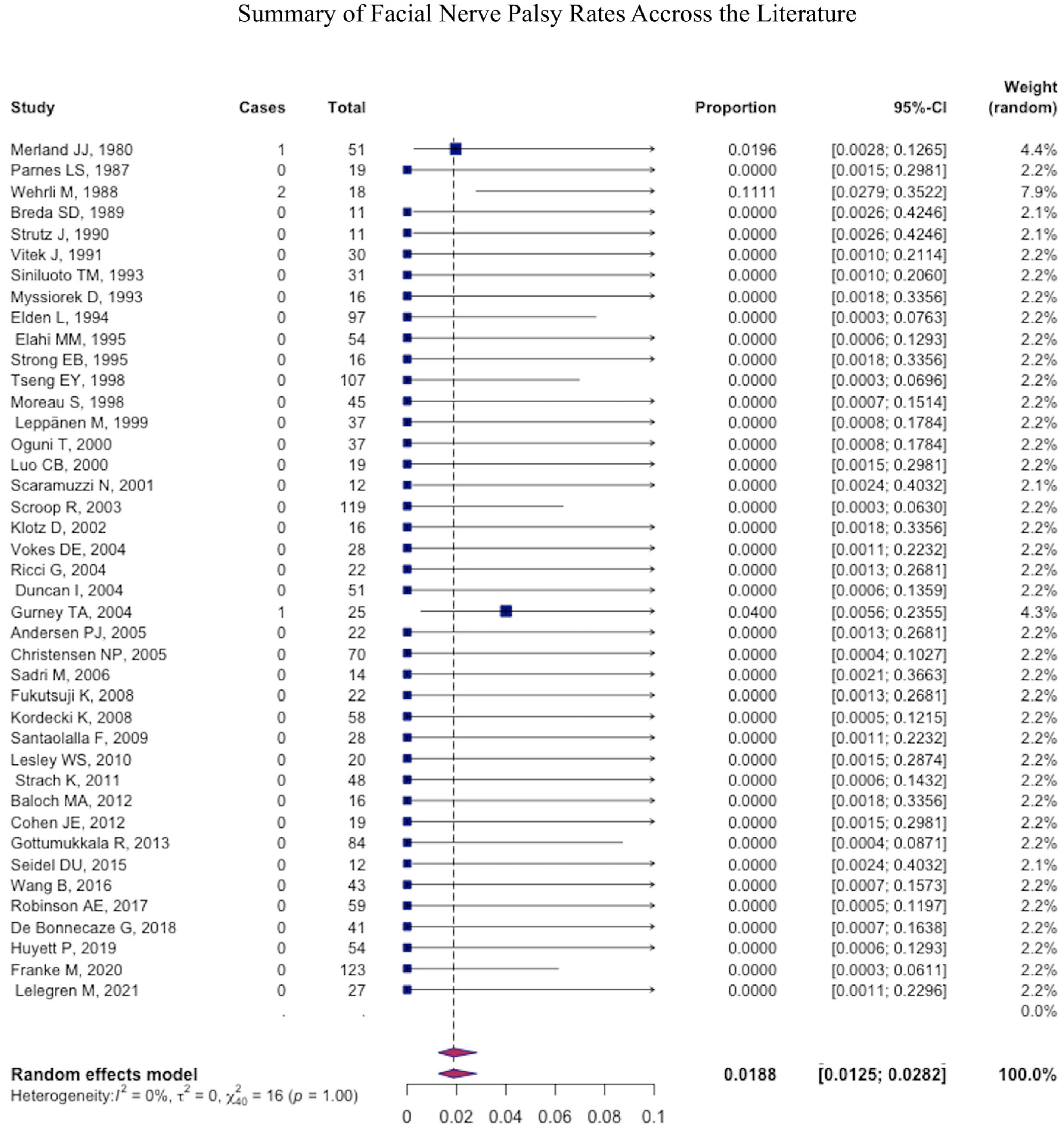
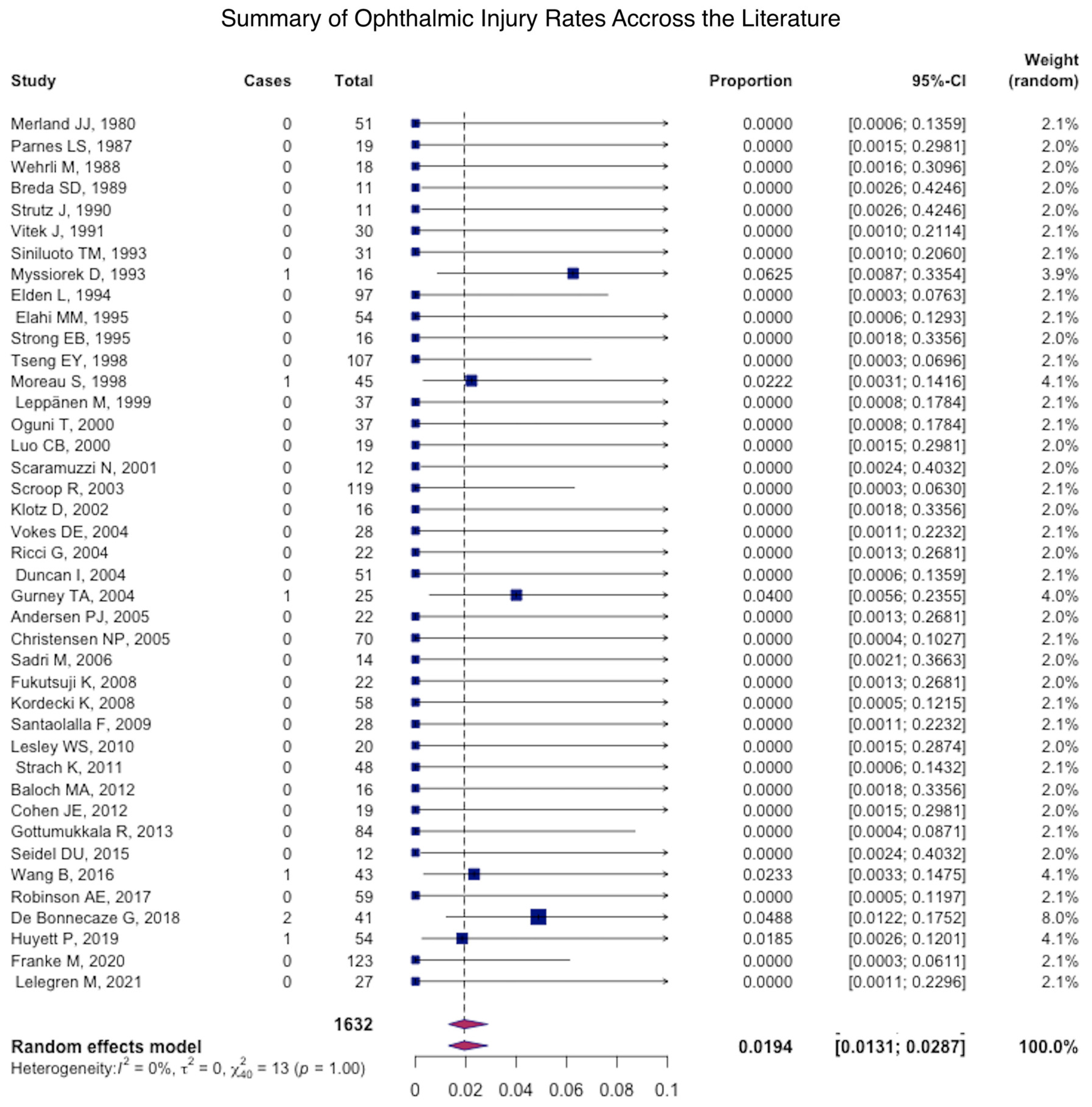
| Study/Year | Stroke (%) | Ophthalmic Injury (%) | Facial Nerve Palsy (%) | Necrosis (%) |
|---|---|---|---|---|
| Merland et al., 1980 [16] | 2 | 0 | 2 | 0 |
| Parnes et al., 1987 [17] | 5.3 | 0 | 0 | 0 |
| Wehrli et al., 1988 [18] | 0 | 0 | 11.1 | 11.1 |
| Breda et al., 1989 [19] | 0 | 0 | 0 | 9.1 |
| Strutz et al., 1990 [20] | 0 | 0 | 0 | 0 |
| Vitek et al., 1991 [9] | 3.3 | 0 | 0 | 0 |
| Siniluoto et al., 1993 [21] | 0 | 0 | 0 | 0 |
| Myssoirek et al., 1993 [22] | 0 | 6.3 | 0 | 0 |
| Elden et al., 1994 [7] | 1 | 0 | 0 | 2.1 |
| Elahi et al., 1995 [23] | 3.7 | 0 | 0 | 0 |
| Strong et al., 1995 [14] | 0 | 0 | 0 | 0 |
| Tseng et al., 1998 [24] | 1.9 | 0 | 0 | 0 |
| Moreau et al., 1998 [25] | 2.2 | 2.2 | 0 | 0 |
| Leppänen et al., 1999 [11] | 2.7 | 0 | 0 | 0 |
| Oguni et al., 2000 [26] | 0 | 0 | 0 | 0 |
| Luo et al., 2000 [27] | 0 | 0 | 0 | 0 |
| Scaramuzzi et al., 2001 [28] | 0 | 0 | 0 | 0 |
| Klotz et al., 2002 [29] | 0 | 0 | 0 | 6.3 |
| Scroop et al., 2003 [30] | 0 | 0 | 0 | 0 |
| Vokes et al., 2004 [10] | 0 | 0 | 0 | 0 |
| Ricci et al., 2004 [31] | 0 | 0 | 0 | 0 |
| Duncan et al., 2004 [32] | 2 | 0 | 0 | 0 |
| Gurney et al., 2004 [33] | 0 | 4 | 4 | 0 |
| Anderson et al., 2005 [34] | 0 | 0 | 0 | 4.5 |
| Christensen et al., 2005 [35] | 1.4 | 0 | 0 | 0 |
| Sadri et al., 2006 [36] | 0 | 0 | 0 | 14.3 |
| Fukutsuji et al., 2008 [6] | 0 | 0 | 0 | 0 |
| Kordecki et al., 2008 [37] | 0 | 0 | 0 | 0 |
| Santaolalla et al., 2009 [38] | 10.7 | 0 | 0 | 0 |
| Lesley et al., 2010 [39] | 0 | 0 | 0 | 0 |
| Strach et al., 2011 [8] | 2.1 | 0 | 0 | 2.1 |
| Baloch et al., 2012 [40] | 0 | 0 | 0 | 0 |
| Cohen et al., 2012 [41] | 0 | 0 | 0 | 0 |
| Gottumukkala et al., 2013 [42] | 0 | 0 | 0 | 1.2 |
| Seidel et al., 2015 [15] | 0 | 0 | 0 | 0 |
| Wang et al., 2016 [43] | 0 | 0 | 0 | 2.3 |
| Robinson et al., 2017 [3] | 0 | 0 | 0 | 0 |
| de Bonnecaze et al., 2018 [44] | 0 | 0 | 0 | 12.2 |
| Huyett et al., 2019 [45] | 1.9 | 0 | 0 | 7.4 |
| Franke et al., 2020 [46] | 0 | 0 | 0 | 0 |
| Lelegren et al., 2021 [47] | 3.7 | 0 | 0 | 0 |
| Pooled Estimate | 1.1 (1.0–1.2) | 0.4 (0.4–0.5) | 0.2 (0.2–0.3) | 1.2 (1.1–1.4) |
| Study/Year | Facial Pain (%) | Headache (%) | Mental Status Change (%) | Facial Numbness (%) | Facial Edema (%) |
|---|---|---|---|---|---|
| Merland et al., 1980 [16] | - | - | - | - | - |
| Parnes et al., 1987 [17] | 31.6 | 0 | 0 | 0 | 0 |
| Wehrli et al., 1988 [18] | 33.3 | 0 | 0 | 16.7 | 0 |
| Breda et al., 1989 [19] | 0 | 0 | 0 | 0 | 0 |
| Strutz et al., 1990 [20] | 0 | 0 | 0 | 0 | 0 |
| Vitek et al., 1991 [9] | 0 | 0 | 0 | 0 | 0 |
| Siniluoto et al., 1993 [21] | 96.8 | 0 | 0 | 0 | 0 |
| Myssoirek et al., 1993 [22] | 68.8 | 0 | 0 | 6.3 | 0 |
| Elden et al., 1994 [7] | 20.6 | 0 | 0 | 0 | 0 |
| Elahi et al., 1995 [23] | 3.7 | 0 | 0 | 1.9 | 0 |
| Strong et al., 1995 [14] | 0 | 0 | 0 | 0 | 0 |
| Tseng et al., 1998 [24] | 5.6 | 2.8 | 4.7 | 0.9 | 0.9 |
| Moreau et al., 1998 [25] | 2.2 | 0 | 0 | 0 | 0 |
| Leppänen et al., 1999 [11] | 0 | 0 | 0 | 8.1 | 0 |
| Oguni et al., 2000 [26] | 24.3 | 18.9 | 0 | 0 | 0 |
| Luo et al., 2000 [27] | 10.5 | 0 | 0 | 0 | 0 |
| Scaramuzzi et al., 2001 [28] | 16.7 | 0 | 0 | 0 | 0 |
| Klotz et al., 2002 [29] | - | - | - | - | - |
| Scroop et al., 2003 [30] | 0 | 0 | 0 | 0 | 0 |
| Vokes et al., 2004 [10] | 3.6 | 3.6 | 0 | 3.6 | 0 |
| Ricci et al., 2004 [31] | 0 | 0 | 0 | 0 | 0 |
| Duncan et al., 2004 [32] | 3.9 | 5.9 | 0 | 0 | 0 |
| Gurney et al., 2004 [33] | 0 | 0 | 0 | 4 | 0 |
| Anderson et al., 2005 [34] | 68.1 | 0 | 0 | 9.1 | 0 |
| Christensen et al., 2005 [35] | - | - | - | - | - |
| Sadri et al., 2006 [36] | 0 | 0 | 0 | 0 | 0 |
| Fukutsuji et al., 2008 [6] | 27.3 | 9.1 | 0 | 13.6 | 4.5 |
| Kordecki et al., 2008 [37] | 0 | 15.5 | 0 | 0 | 5.2 |
| Santaolalla et al., 2009 [38] | 17.9 | 25 | 0 | 0 | 0 |
| Lesley et al., 2010 [39] | 5 | 0 | 0 | 0 | 0 |
| Strach et al., 2011 [8] | - | - | - | - | - |
| Baloch et al., 2012 [40] | 6.3 | 0 | 0 | 0 | 0 |
| Cohen et al., 2012 [41] | 0 | 0 | 0 | 0 | 0 |
| Gottumukkala et al., 2013 [42] | 20.2 | 3.6 | 0 | 0 | 1.2 |
| Seidel et al., 2015 [15] | 0 | 0 | 0 | 0 | 0 |
| Wang et al., 2016 [43] | 30.2 | 0 | 0 | 0 | 0 |
| Robinson et al., 2017 [3] | - | - | 0 | 0 | 0 |
| de Bonnecaze et al., 2018 [44] | 12.2 | 0 | 0 | 0 | 0 |
| Huyett et al., 2019 [45] | 7.4 | 0 | 0 | 3.7 | 0 |
| Franke et al., 2020 [46] | - | - | - | - | - |
| Lelegren et al., 2021 [47] | 0 | 0 | 0 | 0 | 0 |
| Pooled Estimate | 13.1 (12–14.2) | 2.8 (2.5–3.2) | 0.4 (−0.3–0.5) | 1.4 (1.2–1.6) | 0.4 (−0.4–0.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Naamani, K.; Morse, C.; Ghanem, M.; Barbera, J.; Amllay, A.; Severance, G.; Ruiz, R.; Sweid, A.; Gooch, M.R.; Herial, N.A.; et al. Endovascular Embolization for Epistaxis: A Single Center Experience and Meta-Analysis. J. Clin. Med. 2023, 12, 6958. https://doi.org/10.3390/jcm12226958
El Naamani K, Morse C, Ghanem M, Barbera J, Amllay A, Severance G, Ruiz R, Sweid A, Gooch MR, Herial NA, et al. Endovascular Embolization for Epistaxis: A Single Center Experience and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(22):6958. https://doi.org/10.3390/jcm12226958
Chicago/Turabian StyleEl Naamani, Kareem, Charles Morse, Marc Ghanem, Julie Barbera, Abdelaziz Amllay, Grace Severance, Ramon Ruiz, Ahmad Sweid, Michael R. Gooch, Nabeel A. Herial, and et al. 2023. "Endovascular Embolization for Epistaxis: A Single Center Experience and Meta-Analysis" Journal of Clinical Medicine 12, no. 22: 6958. https://doi.org/10.3390/jcm12226958
APA StyleEl Naamani, K., Morse, C., Ghanem, M., Barbera, J., Amllay, A., Severance, G., Ruiz, R., Sweid, A., Gooch, M. R., Herial, N. A., Jabbour, P., Rosenwasser, R. H., Nyquist, G. G., & Tjoumakaris, S. (2023). Endovascular Embolization for Epistaxis: A Single Center Experience and Meta-Analysis. Journal of Clinical Medicine, 12(22), 6958. https://doi.org/10.3390/jcm12226958