
ROCK Inhibitors in Corneal Diseases and Glaucoma—A Comprehensive Review of These Emerging Drugs

 , ,
, ,  ,
,
Abstract
1. Introduction
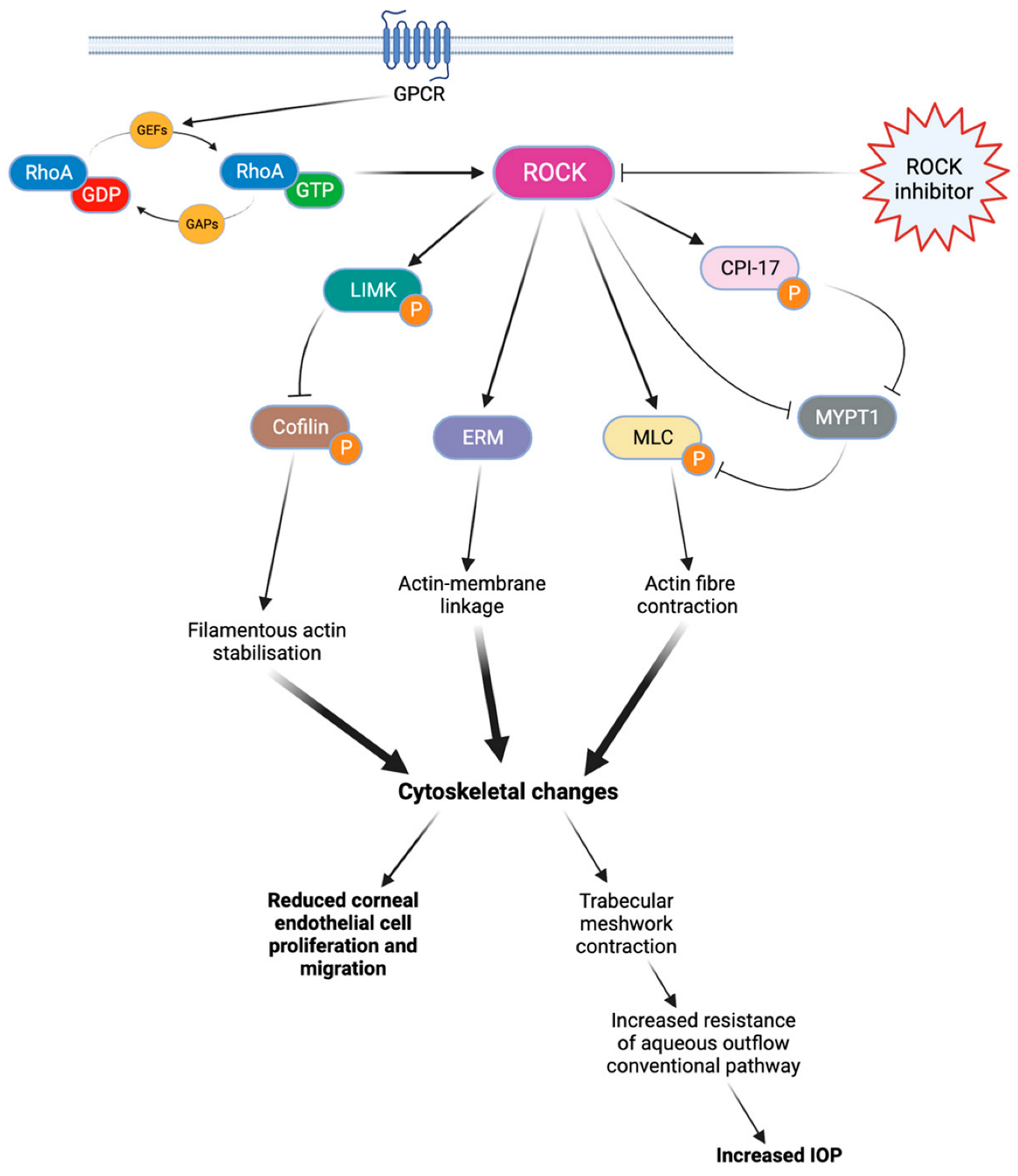
2. The Rho Kinase Pathway
3. Evidence for Clinical Efficacy and Safety of Ripasudi
3.1. Ripasudil in Glaucoma
3.2. Ripasudil in Corneal Diseases
3.3. Safety Profile of Ripasudil
4. Evidence for Clinical Efficacy and Safety of Netarsudil
4.1. Netarsudil in Glaucoma
4.2. Netarsudil in Corneal Diseases
4.3. Safety Profile of Netarsudil
5. Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, K.; Singh, A. Rho-kinase Inhibitors in Ocular Diseases: A Translational Research Journey. J. Curr. Glaucoma Pract. 2023, 17, 44–48. [Google Scholar] [CrossRef]
- Patel, A.R.; Schwartz, G.F.; Campbell, J.H.; Chen, C.C.; McGuiness, C.B.; Multani, J.K.; Shih, V.; Smith, O.U. Economic and Clinical Burden Associated With Intensification of Glaucoma Topical Therapy: A US Claims-based Analysis. J. Glaucoma 2021, 30, 242–250. [Google Scholar] [CrossRef]
- Rikitake, Y.; Liao, J.K. Rho GTPases, statins, and nitric oxide. Circ. Res. 2005, 97, 1232–1235. [Google Scholar] [CrossRef]
- Okumura, N.; Koizumi, N.; Kay, E.P.; Ueno, M.; Sakamoto, Y.; Nakamura, S.; Hamuro, J.; Kinoshita, S. The ROCK inhibitor eye drop accelerates corneal endothelium wound healing. Invest. Ophthalmol. Vis. Sci. 2013, 54, 2493–2502. [Google Scholar] [CrossRef]
- Peh, G.S.L.; Bandeira, F.; Neo, D.; Adnan, K.; Hartono, Y.; Ong, H.S.; Naso, S.; Venkatraman, A.; Gomes, J.A.P.; Kocaba, V.; et al. Effects of Rho-Associated Kinase (Rock) Inhibitors (Alternative to Y-27632) on Primary Human Corneal Endothelial Cells. Cells 2023, 12, 1307. [Google Scholar] [CrossRef]
- Okumura, N.; Nakano, S.; Kay, E.P.; Numata, R.; Ota, A.; Sowa, Y.; Sakai, T.; Ueno, M.; Kinoshita, S.; Koizumi, N. Involvement of cyclin D and p27 in cell proliferation mediated by ROCK inhibitors Y-27632 and Y-39983 during corneal endothelium wound healing. Invest. Ophthalmol. Vis. Sci. 2014, 55, 318–329. [Google Scholar] [CrossRef]
- Franceschino, A.; Dutheil, F.; Pereira, B.; Watson, S.L.; Chiambaretta, F.; Navel, V. Descemetorhexis Without Endothelial Keratoplasty in Fuchs Endothelial Corneal Dystrophy: A Systematic Review and Meta-Analysis. Cornea 2022, 41, 815–825. [Google Scholar] [CrossRef]
- Sugiyama, T.; Shibata, M.; Kajiura, S.; Okuno, T.; Tonari, M.; Oku, H.; Ikeda, T. Effects of fasudil, a Rho-associated protein kinase inhibitor, on optic nerve head blood flow in rabbits. Invest. Ophthalmol. Vis. Sci. 2011, 52, 64–69. [Google Scholar] [CrossRef]
- Tanihara, H.; Yamamoto, T.; Aihara, M.; Kawakita, K.; Kojima, S.; Kanazawa, M.; Nojima, T.; Suganami, H. Ripasudil-Brimonidine Fixed-Dose Combination vs. Ripasudil or Brimonidine: Two Phase 3 Randomized Clinical Trials. Am. J. Ophthalmol. 2023, 248, 35–44. [Google Scholar] [CrossRef]
- Inoue, T.; Tanihara, H.; Tokushige, H.; Araie, M. Efficacy and safety of SNJ-1656 in primary open-angle glaucoma or ocular hypertension. Acta Ophthalmol. 2015, 93, e393–e395. [Google Scholar] [CrossRef]
- Rao, P.V.; Pattabiraman, P.P.; Kopczynski, C. Role of the Rho GTPase/Rho kinase signaling pathway in pathogenesis and treatment of glaucoma: Bench to bedside research. Exp. Eye Res. 2017, 158, 23–32. [Google Scholar] [PubMed]
- Moshirfar, M.; Parker, L.; Birdsong, O.C.; Ronquillo, Y.C.; Hofstedt, D.; Shah, T.J.; Gomez, A.T.; Hoopes, P.C.S. Use of Rho kinase Inhibitors in Ophthalmology: A Review of the Literature. Med. Hypothesis Discov. Innov. Ophthalmol. 2018, 7, 101–111. [Google Scholar] [PubMed]
- Moura-Coelho, N.; Tavares Ferreira, J.; Bruxelas, C.P.; Dutra-Medeiros, M.; Cunha, J.P.; Pinto Proenca, R. Rho kinase inhibitors-a review on the physiology and clinical use in Ophthalmology. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 1101–1117. [Google Scholar]
- Hein, T.W.; Rosa, R.H., Jr.; Yuan, Z.; Roberts, E.; Kuo, L. Divergent roles of nitric oxide and rho kinase in vasomotor regulation of human retinal arterioles. Invest. Ophthalmol. Vis. Sci. 2010, 51, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Higashide, T.; Nagata, A.; Sugiyama, K. Effects of ripasudil, a rho kinase inhibitor, on blood flow in the optic nerve head of normal rats. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.T.; Chang, J.S.; Chen, T.C.; Wang, J.K.; Chang, S.W.; Yang, M.H.; Jou, T.; Wang, I. Inhibition of Rho-associated protein kinase activity enhances oxidative phosphorylation to support corneal endothelial cell migration. FASEB J. 2022, 36, e22397. [Google Scholar] [CrossRef]
- Arita, R.; Hata, Y.; Ishibashi, T. ROCK as a Therapeutic Target of Diabetic Retinopathy. J. Ophthalmol. 2010, 2010, 175163. [Google Scholar] [CrossRef]
- Mateos-Olivares, M.; Garcia-Onrubia, L.; Valentin-Bravo, F.J.; Gonzalez-Sarmiento, R.; Lopez-Galvez, M.; Pastor, J.C.; Usategui-Martín, R.; Pastor-Idoate, S. Rho-Kinase Inhibitors for the Treatment of Refractory Diabetic Macular Oedema. Cells 2021, 10, 1683. [Google Scholar] [CrossRef]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Araie, M.; K-115 Clinical Study Group. Phase 1 clinical trials of a selective Rho kinase inhibitor, K-115. JAMA Ophthalmol. 2013, 131, 1288–1295. [Google Scholar] [CrossRef]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Araie, M.; K-115 Clinical Study Group. Phase 2 randomized clinical study of a Rho kinase inhibitor, K-115, in primary open-angle glaucoma and ocular hypertension. Am. J. Ophthalmol. 2013, 156, 731–736. [Google Scholar] [CrossRef]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Suganami, H.; Araie, M.; K-115 Clinical Study Group. Additive Intraocular Pressure-Lowering Effects of the Rho Kinase Inhibitor Ripasudil (K-115) Combined With Timolol or Latanoprost: A Report of 2 Randomized Clinical Trials. JAMA Ophthalmol. 2015, 133, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Fukushima, A.; Suganami, H.; Araie, M.; K-115 Clinical Study Group. One-year clinical evaluation of 0.4% ripasudil (K-115) in patients with open-angle glaucoma and ocular hypertension. Acta Ophthalmol. 2016, 94, e26–e34. [Google Scholar] [PubMed]
- Tanihara, H.; Kakuda, T.; Sano, T.; Kanno, T.; Imada, R.; Shingaki, W.; Gunji, R. Safety and Efficacy of Ripasudil in Japanese Patients with Glaucoma or Ocular Hypertension: 3-month Interim Analysis of ROCK-J, a Post-Marketing Surveillance Study. Adv. Ther. 2019, 36, 333–343. [Google Scholar] [PubMed]
- Matsumura, R.; Inoue, T.; Matsumura, A.; Tanihara, H. Efficacy of Ripasudil as a Second-line Medication in Addition to a Prostaglandin Analog in Patients with Exfoliation Glaucoma: A Pilot Study. Clin. Drug Investig. 2017, 37, 535–539. [Google Scholar]
- Kusuhara, S.; Katsuyama, A.; Matsumiya, W.; Nakamura, M. Efficacy and safety of ripasudil, a Rho-associated kinase inhibitor, in eyes with uveitic glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 809–814. [Google Scholar]
- Futakuchi, A.; Morimoto, T.; Ikeda, Y.; Tanihara, H.; Inoue, T.; Collaborators R-Ssg. Intraocular pressure-lowering effects of ripasudil in uveitic glaucoma, exfoliation glaucoma, and steroid-induced glaucoma patients: ROCK-S, a multicentre historical cohort study. Sci. Rep. 2020, 10, 10308. [Google Scholar]
- Inazaki, H.; Kobayashi, S.; Anzai, Y.; Satoh, H.; Sato, S.; Inoue, M.; Yamane, S.; Kadonosono, K. Efficacy of the Additional Use of Ripasudil, a Rho-Kinase Inhibitor, in Patients With Glaucoma Inadequately Controlled Under Maximum Medical Therapy. J. Glaucoma 2017, 26, 96–100. [Google Scholar]
- Sakata, R.; Fujishiro, T.; Saito, H.; Honjo, M.; Shirato, S.; Aihara, M. The Additive Effect of ROCK Inhibitor on Prostaglandin-Treated Japanese Patients with Glaucoma Indicating 15 mmHg and Under: ROCK U-15. Adv Ther. 2021, 38, 3760–3770. [Google Scholar]
- Jethva, J.; Bhagat, P.; Prajapati, K.; Tank, G. Safety, efficacy, and patient selection of ripasudil in patients with uncontrolled glaucoma with maximum conventional medical therapy. Indian J. Ophthalmol. 2022, 70, 2020–2023. [Google Scholar]
- Mimura, T.; Noma, H.; Inoue, Y.; Kawashima, M.; Kitsu, K.; Mizota, A. Early Postoperative Effect of Ripasudil Hydrochloride After Trabeculectomy on Secondary Glaucoma: A Randomized Controlled Trial. Open Ophthalmol. J. 2022, 16. [Google Scholar] [CrossRef]
- Mizuno, Y.; Komatsu, K.; Tokumo, K.; Okada, N.; Onoe, H.; Okumichi, H.; Hirooka, K.; Miura, Y.; Kiuchi, Y. A multicenter phase II study on the safety of rho-kinase inhibitor (ripasudil) with needling for the patients after trabeculectomy. Contemp. Clin. Trials Commun. 2023, 33, 101160. [Google Scholar] [PubMed]
- Moloney, G.; Petsoglou, C.; Ball, M.; Kerdraon, Y.; Höllhumer, R.; Spiteri, N.; Beheregaray, S.; Hampson, J.; D’Souza, M.; Devasahayam, R.N. Descemetorhexis Without Grafting for Fuchs Endothelial Dystrophy-Supplementation With Topical Ripasudil. Cornea 2017, 36, 642–648. [Google Scholar] [PubMed]
- Huang, M.J.; Kane, S.; Dhaliwal, D.K. Descemetorhexis Without Endothelial Keratoplasty Versus DMEK for Treatment of Fuchs Endothelial Corneal Dystrophy. Cornea 2018, 37, 1479–1483. [Google Scholar] [PubMed]
- Din, N.; Cohen, E.; Popovic, M.; Mimouni, M.; Trinh, T.; Gouvea, L.; Alshaker, S.M.; Tone, S.M.O.; Chan, C.C.M.; Slomovic, A.R.M. Surgical Management of Fuchs Endothelial Corneal Dystrophy: A Treatment Algorithm and Individual Patient Meta-Analysis of Descemet Stripping Only. Cornea 2022, 41, 1188–1195. [Google Scholar] [PubMed]
- Moloney, G.; Congote, D.G.; Hirnschall, N.; Arsiwalla, T.; Boso, A.L.; Toalster, N.; D’Souza, M.; Devasahayam, R.N. Descemet Stripping Only Supplemented With Topical Ripasudil for Fuchs Endothelial Dystrophy 12-Month Outcomes of the Sydney Eye Hospital Study. Cornea 2021, 40, 320–326. [Google Scholar]
- Macsai, M.S.; Shiloach, M. Use of Topical Rho Kinase Inhibitors in the Treatment of Fuchs Dystrophy After Descemet Stripping Only. Cornea 2019, 38, 529–534. [Google Scholar]
- Parekh, M.; Wongvisavavit, R.; Cubero Cortes, Z.M.; Wojcik, G.; Romano, V.; Tabernero, S.S.; Ferrari, S.; Ahmad, S. Alternatives to endokeratoplasty: An attempt towards reducing global demand of human donor corneas. Regen. Med. 2022, 17, 461–475. [Google Scholar]
- Fujimoto, H.; Setoguchi, Y.; Kiryu, J. The ROCK Inhibitor Ripasudil Shows an Endothelial Protective Effect in Patients With Low Corneal Endothelial Cell Density After Cataract Surgery. Transl. Vis. Sci. Technol. 2021, 10, 18. [Google Scholar]
- Azhari, J.; Patel, U.; Vakharia, M. Corneal endothelial wound healing after Descemet tear with a rho kinase inhibitor. J. Cataract. Refract. Surg. Online Case Rep. 2022, 10, e00075. [Google Scholar]
- Fernandez Lopez, E.; Montolio-Marzo, S.; Ortega Perez, C.; Catalan Gomez, M.; Peris Martinez, C.; Pia Ludena, J.V.; Chan, E. Descemet stripping only and ripasudil for the treatment of traumatic Descemet’s membrane ruptures. Eur. J. Ophthalmol. 2023, 33, NP13-8. [Google Scholar]
- Tseng, M.; Feder, R. Topical Ripasudil for the Treatment of Segmental Corneal Edema: A Case Series. Cornea 2023, 42, 903–907. [Google Scholar] [CrossRef] [PubMed]
- Eslami, M.; Arsiwalla, T.; Boso, A.L.M.; Moloney, G. Use of ripasudil for rapid resolution of acute hydrops in keratoconus. Can. J. Ophthalmol. 2022, 57, e126–e128. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, E.; Ishida, W.; Sumi, T.; Kishimoto, T.; Tada, K.; Fukuda, K.; Yoneda, T.; Kuroiwa, H.; Terao, E.; Fujisawa, Y. Evaluation of offset of conjunctival hyperemia induced by a Rho-kinase inhibitor; 0.4% Ripasudil ophthalmic solution clinical trial. Sci. Rep. 2019, 9, 3755. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Kagami, S.; Mishima, K.; Mataki, N.; Fukushima, A.; Araie, M. Long-term Side Effects Including Blepharitis Leading to Discontinuation of Ripasudil. J. Glaucoma 2019, 28, 289–293. [Google Scholar] [CrossRef]
- Jain, N.; Singh, A.; Mishra, D.K.; Murthy, S.I. Honeycomb epithelial oedema due to ripasudil: Clinical, optical coherence tomography and histopathological correlation. BMJ Case Rep. 2022, 15, e251074. [Google Scholar] [CrossRef]
- Bhargava, M.; Sen, S.; Bhambhani, V.; Paul, R.S.; Dutta, C. Reticular epithelial corneal edema as a novel side-effect of Rho Kinase Inhibitors: An Indian scenario. Indian. J. Ophthalmol. 2022, 70, 1163–1170. [Google Scholar] [CrossRef]
- Tanihara, H.; Kakuda, T.; Sano, T.; Kanno, T.; Gunji, R. Safety and efficacy of ripasudil in Japanese patients with glaucoma or ocular hypertension: 12-month interim analysis of ROCK-J, a post-marketing surveillance study. BMC Ophthalmol. 2020, 20, 275. [Google Scholar]
- Tanihara, H.; Kakuda, T.; Sano, T.; Kanno, T.; Kurihara, Y. Long-Term Intraocular Pressure-Lowering Effects and Adverse Events of Ripasudil in Patients with Glaucoma or Ocular Hypertension over 24 Months. Adv. Ther. 2022, 39, 1659–1677. [Google Scholar] [CrossRef]
- Giles, A.; Foushee, J.; Lantz, E.; Gumina, G. Sulfonamide Allergies. Pharmacy 2019, 7, 132. [Google Scholar] [CrossRef]
- Sit, A.J.; Gupta, D.; Kazemi, A.; McKee, H.; Challa, P.; Liu, K.C.; Lopez, J.; Kopczynski, C.; Heah, T. Netarsudil Improves Trabecular Outflow Facility in Patients with Primary Open Angle Glaucoma or Ocular Hypertension: A Phase 2 Study. Am. J. Ophthalmol. 2021, 226, 262–269. [Google Scholar] [CrossRef]
- Bacharach, J.; Dubiner, H.B.; Levy, B.; Kopczynski, C.C.; Novack, G.D.; AR-13324-CS202 Study Group. Double-masked, randomized, dose-response study of AR-13324 versus latanoprost in patients with elevated intraocular pressure. Ophthalmology 2015, 122, 302–307. [Google Scholar] [CrossRef]
- Asrani, S.; Robin, A.L.; Serle, J.B.; Lewis, R.A.; Usner, D.W.; Kopczynski, C.C.; Heah, T.; Ackerman, S.L.; Alpern, L.M.; Bashford, K.; et al. Netarsudil/Latanoprost Fixed-Dose Combination for Elevated Intraocular Pressure: Three-Month Data from a Randomized Phase 3 Trial. Am. J. Ophthalmol. 2019, 207, 248–257. [Google Scholar] [CrossRef]
- Walters, T.R.; Ahmed, I.I.K.; Lewis, R.A.; Usner, D.W.; Lopez, J.; Kopczynski, C.C.; Heah, T. Once-Daily Netarsudil/Latanoprost Fixed-Dose Combination for Elevated Intraocular Pressure in the Randomized Phase 3 MERCURY-2 Study. Ophthalmol. Glaucoma 2019, 2, 280–289. [Google Scholar] [CrossRef]
- Stalmans, I.; Lim, K.S.; Oddone, F.; Fichtl, M.; Belda, J.I.; Hommer, A.; Laganovska, G.; Schweitzer, C.; Voykov, B.; Zarnowski, T. MERCURY-3: A randomized comparison of netarsudil/latanoprost and bimatoprost/timolol in open-angle glaucoma and ocular hypertension. Graefes Arch. Clin. Exp. Ophthalmol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Singh, I.P.; Fechtner, R.D.; Myers, J.S.; Kim, T.; Usner, D.W.; McKee, H.; Sheng, H.; Lewis, R.A.; Heah, T.; Kopczynski, C.C. Pooled Efficacy and Safety Profile of Netarsudil Ophthalmic Solution 0.02% in Patients With Open-angle Glaucoma or Ocular Hypertension. J. Glaucoma 2020, 29, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Serle, J.B.; Katz, L.J.; McLaurin, E.; Heah, T.; Ramirez-Davis, N.; Usner, D.W.; Novack, G.D.; Kopczynski, C.C. Two Phase 3 Clinical Trials Comparing the Safety and Efficacy of Netarsudil to Timolol in Patients With Elevated Intraocular Pressure: Rho Kinase Elevated IOP Treatment Trial 1 and 2 (ROCKET-1 and ROCKET-2). Am. J. Ophthalmol. 2018, 186, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Khouri, A.S.; Serle, J.B.; Bacharach, J.; Usner, D.W.; Lewis, R.A.; Braswell, P.; Kopczynski, C.C.; Heah, T.; Benza, R.; Boyle, J.W. Once-Daily Netarsudil Versus Twice-Daily Timolol in Patients With Elevated Intraocular Pressure: The Randomized Phase 3 ROCKET-4 Study. Am. J. Ophthalmol. 2019, 204, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.C.; Ratnam, P.V.; Saikumar, S.J.; John, M.; Ravishankar, S.; Dinesh, M.B.; Chandil, P.; Pahuja, K.; Cherlikar, V.; Wadhwani, S.; et al. Netarsudil monotherapy as the initial treatment for open-angle glaucoma and ocular hypertension in Indian patients: A real-world evaluation of efficacy and safety. Indian J. Ophthalmol. 2023, 71, 2500–2503. [Google Scholar] [CrossRef]
- Oydanich, M.; Roll, E.H.; Uppuluri, S.; Khouri, A.S. Effectiveness of netarsudil 0.02% in lowering intraocular pressure in patients with secondary glaucoma. Can. J. Ophthalmol. 2023. [Google Scholar] [CrossRef]
- Kaufman, A.R.; Elhusseiny, A.M.; Edward, D.P.; Vajaranant, T.S.; Aref, A.A.; Abbasian, J. Topical netarsudil for treatment of glaucoma with elevated episcleral venous pressure: A pilot investigation in sturge-weber syndrome. Eur. J. Ophthalmol. 2023, 33, 1969–1976. [Google Scholar] [CrossRef]
- Mehta, A.A.; Kanu, L.N.; Sood-Mendiratta, S.; Quinones, R.; Hawkins, A.; Lehrer, R.A.; Malhotra, K.; Papas, R.; Hillman, D.; Wilensky, J.T.; et al. Experience with netarsudil 0.02% and latanoprostene bunod 0.024% as adjunctive therapy for glaucoma. Eur. J. Ophthalmol. 2022, 32, 322–326. [Google Scholar]
- Araie, M.; Sugiyama, K.; Aso, K.; Kanemoto, K.; Iwata, R.; Hollander, D.A.; Senchyna, M.; Kopczynski, C.C. Phase 3 Clinical Trial Comparing the Safety and Efficacy of Netarsudil to Ripasudil in Patients with Primary Open-Angle Glaucoma or Ocular Hypertension: Japan Rho Kinase Elevated Intraocular Pressure Treatment Trial (J-ROCKET). Adv. Ther. 2023, 40, 4639–4656. [Google Scholar] [PubMed]
- Xu, H.; Thomas, M.T.; Lee, D.; Hirabayashi, M.T.; An, J.A. Response to netarsudil in goniotomy-treated eyes and goniotomy-naive eyes: A pilot study. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3001–3007. [Google Scholar] [CrossRef] [PubMed]
- Price, M.O.; Price, F.W., Jr. Randomized, Double-Masked, Pilot Study of Netarsudil 0.02% Ophthalmic Solution for Treatment of Corneal Edema in Fuchs Dystrophy. Am. J. Ophthalmol. 2021, 227, 100–105. [Google Scholar] [PubMed]
- Lindstrom, R.L.; Lewis, A.E.; Holland, E.J.; Sheppard, J.D.; Hovanesian, J.A.; Senchyna, M.; Holander, D.A. Phase 2, Randomized, Open-Label Parallel-Group Study of Two Dosing Regimens of Netarsudil for the Treatment of Corneal Edema Due to Fuchs Corneal Dystrophy. J. Ocul. Pharmacol. Ther. 2022, 38, 657–663. [Google Scholar]
- Ploysangam, P.; Patel, S.P. A Case Report Illustrating the Postoperative Course of Descemetorhexis without Endothelial Keratoplasty with Topical Netarsudil Therapy. Case Rep. Ophthalmol. Med. 2019, 2019, 6139026. [Google Scholar] [CrossRef]
- Hirabayashi, K.E.; Mark, D.; Lau, J.; Lin, C.C. Descemet Stripping Only for a Chronic Descemet Detachment After Cataract Surgery. Cornea 2020, 39, 379–381. [Google Scholar]
- Chen, S.L.; LoBue, S.A.; Goyal, H. Case report: The use of netarsudil to improve corneal edema after laser peripheral iridotomy and Descemet’s membrane endothelial keratoplasty. Am. J. Ophthalmol. Case Rep. 2021, 22, 101087. [Google Scholar]
- Asrani, S.; Bacharach, J.; Holland, E.; McKee, H.; Sheng, H.; Lewis, R.A.; Kopczynski, C.C.; Heah, T. Fixed-Dose Combination of Netarsudil and Latanoprost in Ocular Hypertension and Open-Angle Glaucoma: Pooled Efficacy/Safety Analysis of Phase 3 MERCURY-1 and -2. Adv. Ther. 2020, 37, 1620–1631. [Google Scholar]
- Lyons, L.J.; Wu, K.Y.; Baratz, K.H.; Sit, A.J. Honeycomb Epithelial Edema Associated with Rho Kinase Inhibition: A Case Series and Review of the Literature. Cornea 2022, 41, 243–248. [Google Scholar]
- Jeang, L.J.; Shah, A.S.; Hammer, J.D.; Tuli, S.S. Reticular epithelial edema after penetrating keratoplasty in a patient taking netarsudil. Digit. J. Ophthalmol. 2022, 28, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Parmar, D.P.; Bhole, P.K.; Garde, P.V. Reticular corneal epithelial edema with topical netarsudil. Oman J. Ophthalmol. 2023, 16, 94–97. [Google Scholar] [PubMed]
- Guzman Aparicio, M.A.; Liebman, D.L.; Chodosh, J.; Freitag, S.K.; Kazlas, M.; Mai, D.D.; Marando, C.M.; Mukai, S.; Wu, A.M.; Chen, T.C. Two pediatric cases of reticular corneal epithelial edema associated with netarsudil. Am. J. Ophthalmol. Case Rep. 2022, 27, 101638. [Google Scholar] [CrossRef]
- Ganesh, D.; Coleman, A.L.; Shibayama, V.P.; Tseng, V.L. Netarsudil-Induced Corneal Flattening in a Child with Secondary Open-Angle Glaucoma. Case Rep. Ophthalmol. 2022, 13, 330–335. [Google Scholar] [PubMed]
- Inoue, T.; Tanihara, H. Rho-associated kinase inhibitors: A novel glaucoma therapy. Prog. Retin. Eye Res. 2013, 37, 1–12. [Google Scholar]
- Okumura, N.; Kinoshita, S.; Koizumi, N. Application of Rho Kinase Inhibitors for the Treatment of Corneal Endothelial Diseases. J. Ophthalmol. 2017, 2017, 2646904. [Google Scholar]
- Honjo, M.; Tanihara, H.; Kameda, T.; Kawaji, T.; Yoshimura, N.; Araie, M. Potential role of Rho-associated protein kinase inhibitor Y-27632 in glaucoma filtration surgery. Invest. Ophthalmol. Vis. Sci. 2007, 48, 5549–5557. [Google Scholar]
- Tura, A.; Grisanti, S.; Petermeier, K.; Henke-Fahle, S. The Rho-kinase inhibitor H-1152P suppresses the wound-healing activities of human Tenon’s capsule fibroblasts in vitro. Invest. Ophthalmol. Vis. Sci. 2007, 48, 2152–2161. [Google Scholar] [CrossRef][Green Version]
- Van de Velde, S.; Van Bergen, T.; Vandewalle, E.; Kindt, N.; Castermans, K.; Moons, L.; Stalmans, I. Rho kinase inhibitor AMA0526 improves surgical outcome in a rabbit model of glaucoma filtration surgery. Prog. Brain Res. 2015, 220, 283–297. [Google Scholar]
- Doe, C.; Bentley, R.; Behm, D.J.; Lafferty, R.; Stavenger, R.; Jung, D.; Bamford, M.; Panchal, T.; Grygielko, E.; Wright, L.L.; et al. Novel Rho kinase inhibitors with anti-inflammatory and vasodilatory activities. J. Pharmacol. Exp. Ther. 2007, 320, 89–98. [Google Scholar]
- He, Y.; Xu, H.; Liang, L.; Zhan, Z.; Yang, X.; Yu, X.; Ye, Y.; Sun, L. Antiinflammatory effect of Rho kinase blockade via inhibition of NF-kappaB activation in rheumatoid arthritis. Arthritis Rheum. 2008, 58, 3366–3376. [Google Scholar] [CrossRef] [PubMed]
- Segain, J.P.; Raingeard de la Bletiere, D.; Sauzeau, V.; Bourreille, A.; Hilaret, G.; Cario-Toumaniantz, C.; Pacaud, P.; Galmiche, J.P.; Loirand, G. Rho kinase blockade prevents inflammation via nuclear factor kappa B inhibition: Evidence in Crohn’s disease and experimental colitis. Gastroenterology 2003, 124, 1180–1187. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Similarities | Differences |
|---|---|
| Overall safety profiles acceptable for clinical use. | The adverse drug reaction (ADR) rate for netarsudil was 3.3% (RCT) versus 18.7% for ripasudil (post-marketing surveillance). |
| Conjunctival hyperemia is the most frequent adverse event. | Blepharitis is the most common reason for discontinuation of ripasudil treatment but is not a prominent side effect of netarsudil. |
| The incidence of severe conjunctival hyperemia is greater in ripasudil compared to netarsudil. | |
| Netarsudil is associated with cornea verticillata as an adverse drug reaction, whereas this has not been observed with ripasudil. | |
| Reticular honeycomb epithelial edema has been observed with both drugs. | Reticular honeycomb epithelial oedema seems to be more frequent with netarsudil, and it has not been observed in the randomized controlled trials for ripasudil. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagano, L.; Lee, J.W.; Posarelli, M.; Giannaccare, G.; Kaye, S.; Borgia, A. ROCK Inhibitors in Corneal Diseases and Glaucoma—A Comprehensive Review of These Emerging Drugs. J. Clin. Med. 2023, 12, 6736. https://doi.org/10.3390/jcm12216736
Pagano L, Lee JW, Posarelli M, Giannaccare G, Kaye S, Borgia A. ROCK Inhibitors in Corneal Diseases and Glaucoma—A Comprehensive Review of These Emerging Drugs. Journal of Clinical Medicine. 2023; 12(21):6736. https://doi.org/10.3390/jcm12216736
Chicago/Turabian StylePagano, Luca, Jason William Lee, Matteo Posarelli, Giuseppe Giannaccare, Stephen Kaye, and Alfredo Borgia. 2023. "ROCK Inhibitors in Corneal Diseases and Glaucoma—A Comprehensive Review of These Emerging Drugs" Journal of Clinical Medicine 12, no. 21: 6736. https://doi.org/10.3390/jcm12216736
APA StylePagano, L., Lee, J. W., Posarelli, M., Giannaccare, G., Kaye, S., & Borgia, A. (2023). ROCK Inhibitors in Corneal Diseases and Glaucoma—A Comprehensive Review of These Emerging Drugs. Journal of Clinical Medicine, 12(21), 6736. https://doi.org/10.3390/jcm12216736