

A Review of Therapeutic Drug Monitoring in Patients with Inflammatory Bowel Disease Receiving Combination Therapy


Abstract
:1. Introduction
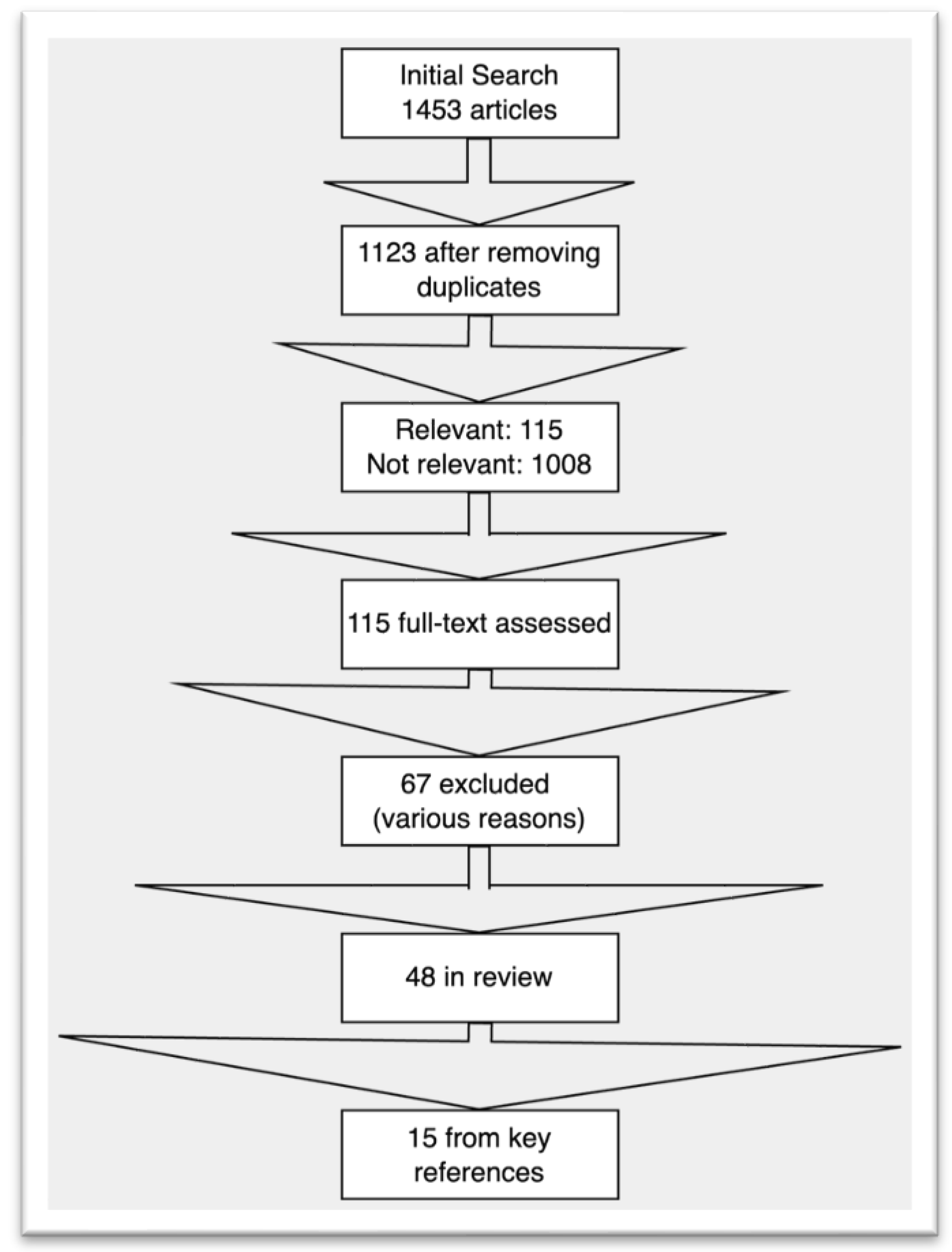
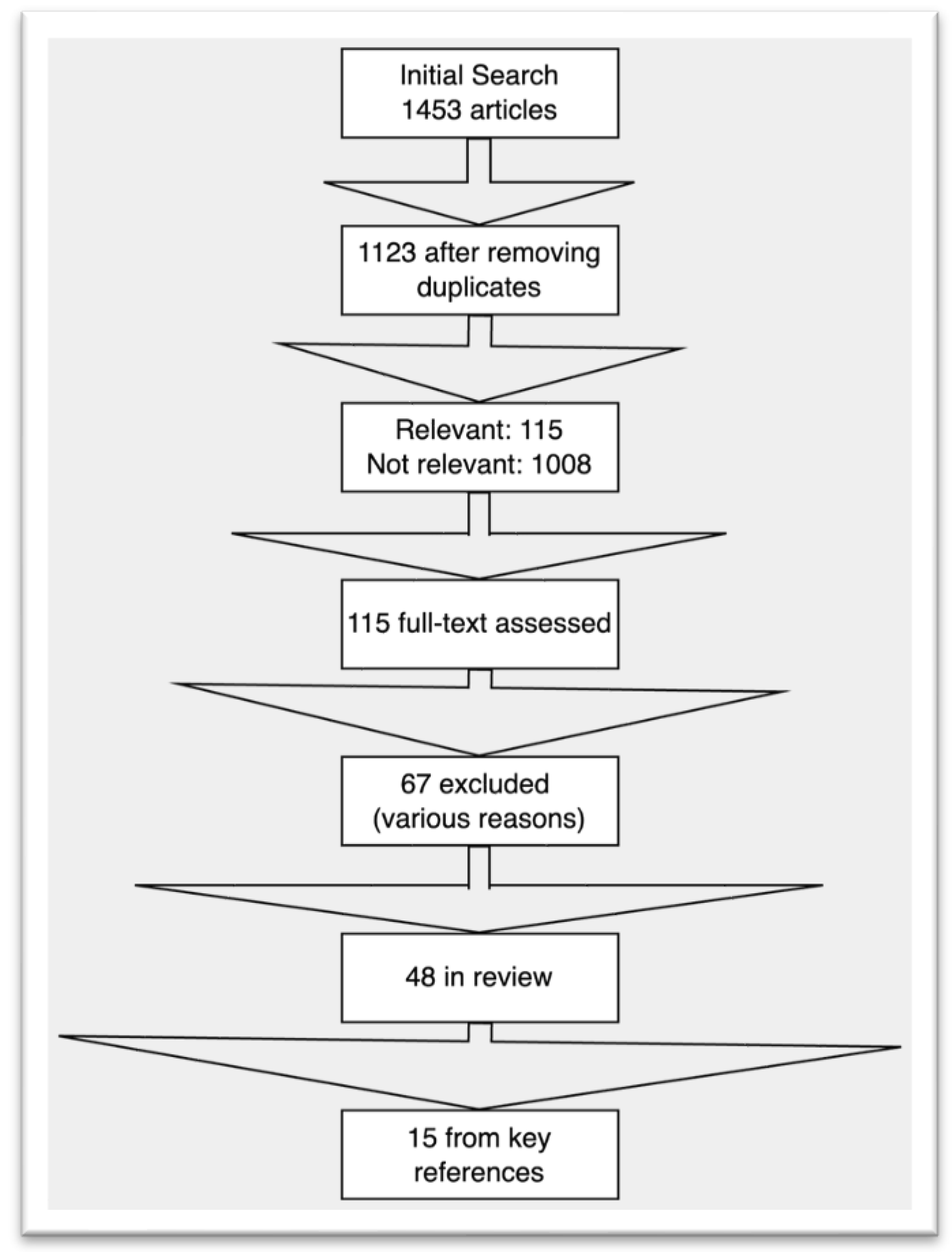
2. Methodology
3. Therapeutic Drug Monitoring Strategies in Inflammatory Bowel Disease
4. Evidence for TDM in Combination Therapy
5. Role of TDM When Restarting Anti-TNFs after a Drug Holiday
TDM and De-Escalation of Combination Therapy
6. Discussion
7. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Targan, S.R.; Hanauer, S.B.; van Deventer, S.J.H.; Mayer, L.; Present, D.H.; Braakman, T.; DeWoody, K.L.; Schaible, T.F.; Rutgeerts, P.J. A Short-Term Study of Chimeric Monoclonal Antibody CA2 to Tumor Necrosis Factor α for Crohn’s Disease. N. Engl. J. Med. 1997, 337, 1029–1036. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Rutgeerts, P.; Enns, R.; Hanauer, S.B.; Colombel, J.-F.; Panaccione, R.; D’Haens, G.; Li, J.; Rosenfeld, M.R.; Kent, J.D.; et al. Adalimumab Induction Therapy for Crohn Disease Previously Treated with Infliximab. Ann. Intern. Med. 2007, 146, 829. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Sandborn, W.J.; Rutgeerts, P.; Fedorak, R.N.; Lukas, M.; MacIntosh, D.; Panaccione, R.; Wolf, D.; Pollack, P. Human Anti–Tumor Necrosis Factor Monoclonal Antibody (Adalimumab) in Crohn’s Disease: The CLASSIC-I Trial. Gastroenterology 2006, 130, 323–333. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Feagan, B.G.; Lichtenstein, G.R.; Mayer, L.F.; Schreiber, S.; Colombel, J.F.; Rachmilewitz, D.; Wolf, D.C.; Olson, A.; Bao, W.; et al. Maintenance Infliximab for Crohn’s Disease: The ACCENT I Randomised Trial. Lancet 2002, 359, 1541–1549. [Google Scholar] [CrossRef]
- Colombel, J.; Sandborn, W.J.; Rutgeerts, P.; Enns, R.; Hanauer, S.B.; Panaccione, R.; Schreiber, S.; Byczkowski, D.; Li, J.; Kent, J.D.; et al. Adalimumab for Maintenance of Clinical Response and Remission in Patients with Crohn’s Disease: The CHARM Trial. Gastroenterology 2007, 132, 52–65. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Stoinov, S.; Honiball, P.J.; Rutgeerts, P.; Mason, D.; Bloomfield, R.; Schreiber, S. Certolizumab Pegol for the Treatment of Crohn’s Disease. N. Engl. J. Med. 2007, 357, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Khaliq-Kareemi, M.; Lawrance, I.C.; Thomsen, O.Ø.; Hanauer, S.B.; McColm, J.; Bloomfield, R.; Sandborn, W.J. Maintenance Therapy with Certolizumab Pegol for Crohn’s Disease. N. Engl. J. Med. 2007, 357, 239–250. [Google Scholar] [CrossRef]
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.-F.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.-J.; Danese, S.; et al. Vedolizumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.-F.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2013, 369, 711–721. [Google Scholar] [CrossRef]
- Sands, B.E.; Sandborn, W.J.; Panaccione, R.; O’Brien, C.D.; Zhang, H.; Johanns, J.; Adedokun, O.J.; Li, K.; Peyrin-Biroulet, L.; Van Assche, G.; et al. Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2019, 381, 1201–1214. [Google Scholar] [CrossRef]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.-L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, N.A.; Heap, G.A.; Green, H.D.; Hamilton, B.; Bewshea, C.; Walker, G.J.; Thomas, A.; Nice, R.; Perry, M.H.; Bouri, S.; et al. Predictors of Anti-TNF Treatment Failure in Anti-TNF-Naive Patients with Active Luminal Crohn’s Disease: A Prospective, Multicentre, Cohort Study. Lancet Gastroenterol. Hepatol. 2019, 4, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.-F.; Adedokun, O.J.; Gasink, C.; Gao, L.-L.; Cornillie, F.J.; D’Haens, G.R.; Rutgeerts, P.J.; Reinisch, W.; Sandborn, W.J.; Hanauer, S.B. Combination Therapy with Infliximab and Azathioprine Improves Infliximab Pharmacokinetic Features and Efficacy: A Post Hoc Analysis. Clin. Gastroenterol. Hepatol. 2019, 17, 1525–1532.e1. [Google Scholar] [CrossRef]
- Marquez-Megias, S.; Nalda-Molina, R.; Sanz-Valero, J.; Más-Serrano, P.; Diaz-Gonzalez, M.; Candela-Boix, M.R.; Ramon-Lopez, A. Cost-Effectiveness of Therapeutic Drug Monitoring of Anti-TNF Therapy in Inflammatory Bowel Disease: A Systematic Review. Pharmaceutics 2022, 14, 1009. [Google Scholar] [CrossRef]
- Dubinsky, M.C.; Lamothe, S.; Yang, H.Y.; Targan, S.R.; Sinnett, D.; Théorêt, Y.; Seidman, E.G. Pharmacogenomics and Metabolite Measurement for 6-Mercaptopurine Therapy in Inflammatory Bowel Disease. Gastroenterology 2000, 118, 705–713. [Google Scholar] [CrossRef]
- Dart, R.J.; Irving, P.M. Optimising Use of Thiopurines in Inflammatory Bowel Disease. Expert Rev. Clin. Immunol. 2017, 13, 877–888. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Z.; Chua, E.W. Revisiting the Role of Thiopurines in Inflammatory Bowel Disease Through Pharmacogenomics and Use of Novel Methods for Therapeutic Drug Monitoring. Front. Pharmacol. 2018, 9, 1107. [Google Scholar] [CrossRef]
- Mao, R.; Guo, J.; Luber, R.; Chen, B.-L.; He, Y.; Zeng, Z.-R.; Ben-Horin, S.; Sparrow, M.P.; Roblin, X.; Chen, M.-H. 6-Thioguanine Nucleotide Levels Are Associated with Mucosal Healing in Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 2621–2627. [Google Scholar] [CrossRef]
- Colombel, J.F.; Sandborn, W.J.; Reinisch, W.; Mantzaris, G.J.; Kornbluth, A.; Rachmilewitz, D.; Lichtiger, S.; d’Haens, G.; Diamond, R.H.; Broussard, D.L.; et al. Infliximab, Azathioprine, or Combination Therapy for Crohn’s Disease. N. Engl. J. Med. 2010, 362, 1383–1395. [Google Scholar] [CrossRef] [PubMed]
- Yarur, A.J.; Kubiliun, M.J.; Czul, F.; Sussman, D.A.; Quintero, M.A.; Jain, A.; Drake, K.A.; Hauenstein, S.I.; Lockton, S.; Deshpande, A.R.; et al. Concentrations of 6-Thioguanine Nucleotide Correlate with Trough Levels of Infliximab in Patients with Inflammatory Bowel Disease on Combination Therapy. Clin. Gastroenterol. Hepatol. 2015, 13, 1118–1124.e3. [Google Scholar] [CrossRef] [PubMed]
- Maser, E.A.; Villela, R.; Silverberg, M.S.; Greenberg, G.R. Association of Trough Serum Infliximab to Clinical Outcome After Scheduled Maintenance Treatment for Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2006, 4, 1248–1254. [Google Scholar] [CrossRef] [PubMed]
- Yarur, A.J.; Jain, A.; Hauenstein, S.I.; Quintero, M.A.; Barkin, J.S.; Deshpande, A.R.; Sussman, D.A.; Singh, S.; Abreu, M.T. Higher Adalimumab Levels Are Associated with Histologic and Endoscopic Remission in Patients with Crohns Disease and Ulcerative Colitis. Inflamm. Bowel Dis. 2016, 22, 409–415. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Feagan, B.G.; Vermeire, S.; Yassine, M.; Coarse, J.; Kosutic, G.; Sandborn, W.J. Exposure-Response Relationship of Certolizumab Pegol Induction and Maintenance Therapy in Patients with Crohn’s Disease. Aliment. Pharmacol. Ther. 2017, 47, 229–237. [Google Scholar] [CrossRef]
- Papamichael, K.; Cheifetz, A.S.; Melmed, G.Y.; Irving, P.M.; Vande Casteele, N.; Kozuch, P.L.; Raffals, L.E.; Baidoo, L.; Bressler, B.; Devlin, S.M.; et al. Appropriate Therapeutic Drug Monitoring of Biologic Agents for Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2019, 17, 1655–1668.e3. [Google Scholar] [CrossRef] [PubMed]
- Battat, R.; Lukin, D.; Scherl, E.J.; Pola, S.; Kumar, A.; Okada, L.; Yang, L.; Jain, A.; Siegel, C.A. Immunogenicity of Tumor Necrosis Factor Antagonists and Effect of Dose Escalation on Anti-Drug Antibodies and Serum Drug Concentrations in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2020, 27, 1443–1451. [Google Scholar] [CrossRef]
- Afif, W.; Loftus, E.V.; Faubion, W.A.; Kane, S.V.; Bruining, D.H.; Hanson, K.A.; Sandborn, W.J. Clinical Utility of Measuring Infliximab and Human Anti-Chimeric Antibody Concentrations in Patients with Inflammatory Bowel Disease. Am. J. Gastroenterol. 2010, 105, 1133–1139. [Google Scholar] [CrossRef]
- Vermeire, S.; Dreesen, E.; Papamichael, K.; Dubinsky, M.C. How, When, and for Whom Should We Perform Therapeutic Drug Monitoring? Clin. Gastroenterol. Hepatol. 2020, 18, 1291–1299. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Ferrante, M.; Van Assche, G.; Ballet, V.; Compernolle, G.; Van Steen, K.; Simoens, S.; Rutgeerts, P.; Gils, A.; Vermeire, S. everine Trough Concentrations of Infliximab Guide Dosing for Patients with Inflammatory Bowel Disease. Gastroenterology 2015, 148, 1320–1329.e3. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Vermeire, S.; Lambrecht, G.; Baert, F.; Bossuyt, P.; Pariente, B.; Buisson, A.; Bouhnik, Y.; Filippi, J.; vander Woude, J.; et al. Increasing Infliximab Dose Based on Symptoms, Biomarkers, and Serum Drug Concentrations Does Not Increase Clinical, Endoscopic, and Corticosteroid-Free Remission in Patients with Active Luminal Crohn’s Disease. Gastroenterology 2018, 154, 1343–1351.e1. [Google Scholar] [CrossRef]
- Laharie, D.; D’Haens, G.; Nachury, M.; Lambrecht, G.; Bossuyt, P.; Bouhnik, Y.; Louis, E.; Janneke van der Woude, C.; Buisson, A.; Van Hootegem, P.; et al. Steroid-Free Deep Remission at One Year Does Not Prevent Crohn’s Disease Progression: Long-Term Data From the TAILORIX Trial. Clin. Gastroenterol. Hepatol. 2022, 20, 2074–2082. [Google Scholar] [CrossRef] [PubMed]
- Assa, A.; Matar, M.; Turner, D.; Broide, E.; Weiss, B.; Ledder, O.; Guz-Mark, A.; Rinawi, F.; Cohen, S.; Topf-Olivestone, C.; et al. Proactive Monitoring of Adalimumab Trough Concentration Associated with Increased Clinical Remission in Children with Crohn’s Disease Compared with Reactive Monitoring. Gastroenterology 2019, 157, 985–996.e2. [Google Scholar] [CrossRef]
- Syversen, S.W. Effect of Therapeutic Drug Monitoring vs Standard Therapy During Infliximab Induction on Disease Remission In. JAMA 2021, 325, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Syversen, S.W. Effect of Therapeutic Drug Monitoring vs Standard Therapy During Maintenance Infliximab Therapy on Disease. JAMA 2021, 326, 2375–2384. [Google Scholar] [CrossRef] [PubMed]
- Yarur, A.J.; Abreu, M.T.; Deepak, P.; Beniwal-Patel, P.; Papamichail, K.; Vaughn, B.; Bruss, A.; Sekhri, S.; Moosreiner, A.; Gu, P.; et al. Patients with Inflammatory Bowel Diseases and Higher Visceral Adipose Tissue Burden May Benefit from Higher Infliximab Concentrations to Achieve Remission. Am. J. Gastroenterol. 2023, 10-14309, in press. [Google Scholar] [CrossRef]
- Magro, F.; Rodrigues-Pinto, E.; Santos-Antunes, J.; Vilas-Boas, F.; Lopes, S.; Nunes, A.; Camila-Dias, C.; Macedo, G. High C-Reactive Protein in Crohn’s Disease Patients Predicts Nonresponse to Infliximab Treatment. J. Crohn’s Colitis 2014, 8, 129–136. [Google Scholar] [CrossRef]
- Hibi, T.; Sakuraba, A.; Watanabe, M.; Motoya, S.; Ito, H.; Sato, N.; Yoshinari, T.; Motegi, K.; Kinouchi, Y.; Takazoe, M.; et al. C-Reactive Protein Is an Indicator of Serum Infliximab Level in Predicting Loss of Response in Patients with Crohn’s Disease. J. Gastroenterol. 2013, 49, 254–262. [Google Scholar] [CrossRef]
- Velayos, F.S.; Kahn, J.G.; Sandborn, W.J.; Feagan, B.G. A Test-Based Strategy Is More Cost Effective Than Empiric Dose Escalation for Patients with Crohn’s Disease Who Lose Responsiveness to Infliximab. Clin. Gastroenterol. Hepatol. 2013, 11, 654–666. [Google Scholar] [CrossRef] [PubMed]
- Steenholdt, C.; Brynskov, J.; Thomsen, O.Ø.; Munck, L.K.; Fallingborg, J.; Christensen, L.A.; Pedersen, G.; Kjeldsen, J.; Jacobsen, B.A.; Oxholm, A.S.; et al. Individualised Therapy Is More Cost-Effective than Dose Intensification in Patients with Crohn’s Disease Who Lose Response to Anti-TNF Treatment: A Randomised, Controlled Trial. Gut 2014, 63, 919–927. [Google Scholar] [CrossRef]
- Negoescu, D.M.; Enns, E.A.; Swanhorst, B.; Baumgartner, B.; Campbell, J.P.; Osterman, M.T.; Papamichael, K.; Cheifetz, A.S.; Vaughn, B.P. Proactive Vs Reactive Therapeutic Drug Monitoring of Infliximab in Crohn’s Disease: A Cost-Effectiveness Analysis in a Simulated Cohort. Inflamm. Bowel Dis. 2020, 26, 103–111. [Google Scholar] [CrossRef]
- McNeill, R.P.; Barclay, M.L. Cost-Effectiveness of Therapeutic Drug Monitoring in Inflammatory Bowel Disease. Curr. Opin. Pharmacol. 2020, 55, 41–46. [Google Scholar] [CrossRef]
- Strik, A.S.; Löwenberg, M.; Mould, D.R.; Berends, S.E.; Ponsioen, C.I.; van den Brande, J.M.H.; Jansen, J.M.; Hoekman, D.R.; Brandse, J.F.; Duijvestein, M.; et al. Efficacy of Dashboard Driven Dosing of Infliximab in Inflammatory Bowel Disease Patients; a Randomized Controlled Trial. Scand. J. Gastroenterol. 2020, 56, 145–154. [Google Scholar] [CrossRef]
- Cheifetz, A.S.; Abreu, M.T.; Afif, W.; Cross, R.K.; Dubinsky, M.C.; Loftus, E.V.; Osterman, M.T.; Saroufim, A.; Siegel, C.A.; Yarur, A.J.; et al. A Comprehensive Literature Review and Expert Consensus Statement on Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2021, 116, 2014–2025. [Google Scholar] [CrossRef]
- Sethi, S.; Dias, S.; Kumar, A.; Blackwell, J.; Brookes, M.J.; Segal, J.P. Metaanalysis: The Efficacy of Therapeutic Drug Monitoring of Anti TNF Therapy in Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2022, 57, 1362–1374. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Dulai, P.S.; Vande Casteele, N.; Battat, R.; Fumery, M.; Boland, B.S.; Sandborn, W.J. Systematic Review with Meta-Analysis: Association between Vedolizumab Trough Concentration and Clinical Outcomes in Patients with Inflammatory Bowel Diseases. Aliment. Pharmacol. Ther. 2019, 50, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Dreesen, E.; Verstockt, B.; Bian, S.; de Bruyn, M.; Compernolle, G.; Tops, S.; Noman, M.; Van Assche, G.; Ferrante, M.; Gils, A.; et al. Evidence to Support Monitoring of Vedolizumab Trough Concentrations in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1937–1946.e8. [Google Scholar] [CrossRef] [PubMed]
- Adedokun, O.J.; Xu, Z.; Gasink, C.; Jacobstein, D.; Szapary, P.; Johanns, J.; Gao, L.-L.; Davis, H.M.; Hanauer, S.B.; Feagan, B.G.; et al. Pharmacokinetics and Exposure Response Relationships of Ustekinumab in Patients with Crohn’s Disease. Gastroenterology 2018, 154, 1660–1671. [Google Scholar] [CrossRef] [PubMed]
- Battat, R.; Kopylov, U.; Bessissow, T.; Bitton, A.; Cohen, A.; Jain, A.; Martel, M.; Seidman, E.; Afif, W. Association Between Ustekinumab Trough Concentrations and Clinical, Biomarker, and Endoscopic Outcomes in Patients with Crohn’s Disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2017, 15, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Yarur, A.J.; Bruss, A.; Naik, S.; Beniwal-Patel, P.; Fox, C.; Jain, A.; Berens, B.; Patel, A.; Ungaro, R.; Bahur, B.; et al. Vedolizumab Concentrations Are Associated with Long-Term Endoscopic Remission in Patients with Inflammatory Bowel Diseases. Dig. Dis. Sci. 2019, 64, 1651–1659. [Google Scholar] [CrossRef]
- Yarur, A.J.; Digestive Disease Week ePoster Library 2022. Higher Serum Ustekinumab Levels Correlate with Higher Rates of Steroid-Free Deep Remission and Endoscopic Healing in Patients with IBD. Available online: https://eposters.ddw.org/ddw/2022/ddw-2022/353592/ (accessed on 29 April 2023).
- Osterman, M.T.; Jairath, V.; Rana-Khan, Q.; James, A.; Balma, D.; Mehrotra, S.; Yang, L.; Lasch, K.; Yarur, A.J. 791: A randomized trial of vedolizumab dose optimization in patients with moderate to severe ulcerative colitis who have early nonresponse and high drug clearance: The enterpret trial. Gastroenterology 2022, 162, S-190–S-191. [Google Scholar] [CrossRef]
- Admin, S. European Crohn’s and Colitis Organisation-ECCO-P436 Efficacy and Safety of Intravenous Ustekinumab Re-Induction Therapy in Crohn’s Disease Patients with Secondary Loss of Response to Ustekinumab Maintenance Therapy: Week 16 Results from the POWER Trial. Available online: https://www.ecco-ibd.eu/publications/congress-abstracts/item/p436-efficacy-and-safety-of-intravenous-ustekinumab-re-induction-therapy-in-crohn-s-disease-patients-with-secondary-loss-of-response-to-ustekinumab-maintenance-therapy-week-16-results-from-the-power-trial.html (accessed on 21 May 2023).
- Yarur, A.J.; Deepak, P.; Vande Casteele, N.; Battat, R.; Jain, A.; Okada, L.; Osterman, M.; Regueiro, M. Between Vedolizumab Levels, Anti-Vedolizumab Antibodies, and Endoscopic Healing Index in a Large Population of Patients with Inflammatory Bowel Diseases. Dig. Dis. Sci. 2020, 66, 3563–3569. [Google Scholar] [CrossRef]
- Vande Casteele, N.; Khanna, R.; Levesque, B.G.; Stitt, L.; Zou, G.Y.; Singh, S.; Lockton, S.; Hauenstein, S.; Ohrmund, L.; Greenberg, G.R.; et al. The Relationship between Infliximab Concentrations, Antibodies to Infliximab and Disease Activity in Crohn’s Disease. Gut 2014, 64, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, S.; Gils, A.; Accossato, P.; Lula, S.; Marren, A. Immunogenicity of Biologics in Inflammatory Bowel Disease. Ther. Adv. Gastroenterol. 2018, 11, 1756283X1775035. [Google Scholar] [CrossRef]
- Stallhofer, J.; Guse, J.; Kesselmeier, M.; Grunert, P.C.; Lange, K.; Stalmann, R.; Eckardt, V.; Stallmach, A. Immunomodulator Comedication Promotes the Reversal of Anti-Drug Antibody-Mediated Loss of Response to Anti-TNF Therapy in Inflammatory Bowel Disease. Int. J. Color. Dis. 2023, 38, 54. [Google Scholar] [CrossRef] [PubMed]
- Ungar, B.; Kopylov, U.; Engel, T.; Yavzori, M.; Fudim, E.; Picard, O.; Lang, A.; Williet, N.; Paul, S.; Chowers, Y.; et al. Addition of an Immunomodulator Can Reverse Antibody Formation and Loss of Response in Patients Treated with Adalimumab. Aliment. Pharmacol. Ther. 2017, 45, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Panaccione, R.; Ghosh, S.; Middleton, S.; Márquez, J.R.; Scott, B.B.; Flint, L.; van Hoogstraten, H.J.F.; Chen, A.C.; Zheng, H.; Danese, S.; et al. Combination Therapy with Infliximab and Azathioprine Is Superior to Monotherapy with Either Agent in Ulcerative Colitis. Gastroenterology 2014, 146, 392–400.e3. [Google Scholar] [CrossRef]
- Feagan, B.G.; McDonald, J.W.D.; Panaccione, R.; Enns, R.A.; Bernstein, C.N.; Ponich, T.P.; Bourdages, R.; MacIntosh, D.G.; Dallaire, C.; Cohen, A.; et al. Methotrexate in Combination with Infliximab Is No More Effective Than Infliximab Alone in Patients with Crohn’s Disease. Gastroenterology 2014, 146, 681–688.e1. [Google Scholar] [CrossRef] [PubMed]
- Vande Casteele, N.; Abreu, M.T.; Flier, S.; Papamichael, K.; Rieder, F.; Silverberg, M.S.; Khanna, R.; Okada, L.; Yang, L.; Jain, A.; et al. Patients with Low Drug Levels or Antibodies to a Prior Anti-Tumor Necrosis Factor Are More Likely to Develop Antibodies to a Subsequent Anti-Tumor Necrosis Factor. Clin. Gastroenterol. Hepatol. 2022, 20, 465–467.e2. [Google Scholar] [CrossRef]
- Vermeire, S.; Noman, M.; Assche, G.V.; Baert, F.; D’Haens, G.; Rutgeerts, P. Effectiveness of Concomitant Immunosuppressive Therapy in Suppressing the Formation of Antibodies to Infliximab in Crohn’s Disease. Gut 2007, 56, 1226–1231. [Google Scholar] [CrossRef]
- Privitera, G.; Pugliese, D.; Onali, S.; Petito, V.; Scaldaferri, F.; Gasbarrini, A.; Danese, S.; Armuzzi, A. Combination Therapy in Inflammatory Bowel Disease–from Traditional Immunosuppressors towards the New Paradigm of Dual Targeted Therapy. Autoimmun. Rev. 2021, 20, 102832. [Google Scholar] [CrossRef] [PubMed]
- Roblin, X.; Williet, N.; Boschetti, G.; Phelip, J.-M.; Del Tedesco, E.; Berger, A.-E.; Vedrines, P.; Duru, G.; Peyrin-Biroulet, L.; Nancey, S.; et al. Addition of Azathioprine to the Switch of Anti-TNF in Patients with IBD in Clinical Relapse with Undetectable Anti-TNF Trough Levels and Antidrug Antibodies: A Prospective Randomised Trial. Gut 2020, 69, 1206–1212. [Google Scholar] [CrossRef]
- Yarur, A.J.; McGovern, D.; Abreu, M.T.; Cheifetz, A.; Papamichail, K.; Deepak, P.; Bruss, A.; Beniwal-Patel, P.; Dubinsky, M.; Targan, S.R.; et al. Combination Therapy with Immunomodulators Improves the Pharmacokinetics of Infliximab But Not Vedolizumab or Ustekinumab. Clin. Gastroenterol. Hepatol. 2022, 21, 2908–2917. [Google Scholar] [CrossRef] [PubMed]
- Baert, F.; Drobne, D.; Gils, A.; Vande Casteele, N.; Hauenstein, S.; Singh, S.; Lockton, S.; Rutgeerts, P.; Vermeire, S. Early Trough Levels and Antibodies to Infliximab Predict Safety and Success of Reinitiation of Infliximab Therapy. Clin. Gastroenterol. Hepatol. 2014, 12, 1474–1481.e2. [Google Scholar] [CrossRef] [PubMed]
- Normatov, I. Mo1890–Using Therapeutic Drug Monitoring to Predict Success of Restarting Infliximab Therapy After a Drug Holiday in Inflammatory Bowel Disease. Gastroenterology 2019, 156, S-876. [Google Scholar] [CrossRef]
- Louis, E.; Mary, J.-Y.; Vernier-Massouille, G.; Grimaud, J.-C.; Bouhnik, Y.; Laharie, D.; Dupas, J.-L.; Pillant, H.; Picon, L.; Veyrac, M.; et al. Maintenance of Remission among Patients with Crohn’s Disease on Antimetabolite Therapy after Infliximab Therapy Is Stopped. Gastroenterology 2012, 142, 63–70.e5, quiz e31. [Google Scholar] [CrossRef]
- Sazonovs, A.; Kennedy, N.A.; Moutsianas, L.; Heap, G.A.; Rice, D.L.; Reppell, M.; Bewshea, C.M.; Chanchlani, N.; Walker, G.J.; Perry, M.H.; et al. HLA-DQA1*05 Carriage Associated with Development of Anti-Drug Antibodies to Infliximab and Adalimumab in Patients with Crohn’s Disease. Gastroenterology 2020, 158, 189–199. [Google Scholar] [CrossRef]
- Spencer, E.A.; Stachelski, J.; Dervieux, T.; Dubinsky, M.C. Failure to Achieve Target Drug Concentrations During Induction and Not HLA-DQA1∗05 Carriage Is Associated with Antidrug Antibody Formation in Patients with Inflammatory Bowel Disease. Gastroenterology 2022, 162, 1746–1748.e3. [Google Scholar] [CrossRef]
- Fuentes-Valenzuela, E.; García-Alonso, F.J.; Maroto-Martín, C.; Juan Casamayor, L.; Garrote, J.A.; Almendros Muñoz, R.; De Prado, Á.; Vara Castrodeza, A.; Marinero, M.Á.; Calleja Carbajosa, R.; et al. Influence of HLADQA1*05 Genotype in Adults with Inflammatory Bowel Disease and Anti-TNF Treatment with Proactive Therapeutic Drug Monitoring: A Retrospective Cohort Study. Inflamm. Bowel Dis. 2023, 29, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, G.; Magdelaine–Beuzelin, C.; D’Haens, G.; Baert, F.; Noman, M.; Vermeire, S.; Ternant, D.; Watier, H.; Paintaud, G.; Rutgeerts, P. Withdrawal of Immunosuppression in Crohn’s Disease Treated with Scheduled Infliximab Maintenance: A Randomized Trial. Gastroenterology 2008, 134, 1861–1868. [Google Scholar] [CrossRef]
- Drobne, D.; Bossuyt, P.; Breynaert, C.; Cattaert, T.; Vande Casteele, N.; Compernolle, G.; Jürgens, M.; Ferrante, M.; Ballet, V.; Wollants, W.-J.; et al. Withdrawal of Immunomodulators After Co-Treatment Does Not Reduce Trough Level of Infliximab in Patients with Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2015, 13, 514–521.e4. [Google Scholar] [CrossRef]
- Sokol, H.; Seksik, P.; Carrat, F.; Nion-Larmurier, I.; Vienne, A.; Beaugerie, L.; Cosnes, J. Usefulness of Co-Treatment with Immunomodulators in Patients with Inflammatory Bowel Disease Treated with Scheduled Infliximab Maintenance Therapy. Gut 2010, 59, 1363–1368. [Google Scholar] [CrossRef]
- Roblin, X.; Boschetti, G.; Williet, N.; Nancey, S.; Marotte, H.; Berger, A.; Phelip, J.M.; Peyrin-Biroulet, L.; Colombel, J.F.; Del Tedesco, E.; et al. Azathioprine Dose Reduction in Inflammatory Bowel Disease Patients on Combination Therapy: An Open-Label, Prospective and Randomised Clinical Trial. Aliment. Pharmacol. Ther. 2017, 46, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Dulai, P.S.; Siegel, C.A.; Colombel, J.-F.; Sandborn, W.J.; Peyrin-Biroulet, L. Systematic Review: Monotherapy with Antitumour Necrosis Factor α Agents versus Combination Therapy with an Immunosuppressive for IBD. Gut 2014, 63, 1843–1853. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Huang, Y.-H.; Jiang, M. Combination Therapy in Inflammatory Bowel Disease: Current Evidence and Perspectives. Int. Immunopharmacol. 2023, 114, 109545. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Afif, W.; Drobne, D.; Dubinsky, M.C.; Ferrante, M.; Irving, P.M.; Kamperidis, N.; Kobayashi, T.; Kotze, P.G.; Lambert, J.; et al. Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease: Unmet Needs and Future Perspectives. Lancet Gastroenterol. Hepatol. 2022, 7, 171–185. [Google Scholar] [CrossRef] [PubMed]
- Laserna-Mendieta, E.J.; Salvador-Martín, S.; Arias-González, L.; Ruiz-Ponce, M.; Menchén, L.A.; Sánchez, C.; López-Fernández, L.A.; Lucendo, A.J. Comparison of a New Rapid Method for the Determination of Adalimumab Serum Levels with Two Established ELISA Kits. Clin. Chem. Lab. Med. 2019, 57, 1906–1914. [Google Scholar] [CrossRef]
- Nasser, Y.; Labetoulle, R.; Harzallah, I.; Berger, A.-E.; Roblin, X.; Paul, S. Comparison of Point-of-Care and Classical Immunoassays for the Monitoring Infliximab and Antibodies Against Infliximab in IBD. Dig. Dis. Sci. 2018, 63, 2714–2721. [Google Scholar] [CrossRef]
- Irving, P.M.; Gecse, K.B. Optimizing Therapies Using Therapeutic Drug Monitoring: Current Strategies and Future Perspectives. Gastroenterology 2022, 162, 1512–1524. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study Name/Reference | Study Design | Population | Intervention | Key Findings |
|---|---|---|---|---|
| TAXIT [28] | Randomized trial | IBD patients on infliximab | Proactive TDM vs. as-needed dose adjustment | Proactive TDM was not superior |
| TAILORIX [29,30] | Randomized trial | IBD patients on infliximab | Proactive TDM | Results similar to TAXIT |
| PAILOT [31] | Non-blinded RCT | Pediatric CD patients on adalimumab | Proactive dose adjustment | More efficacious than reactive approach |
| NOR-DRUM A and B [32,33] | Randomized study | IBD patients on various treatments | Proactive TDM | No benefit during induction but beneficial during maintenance |
| Study Name/Reference | Study Design | Population | Intervention | Key Findings |
|---|---|---|---|---|
| SONIC [19] | Randomized trial | CD patients on infliximab and azathioprine | Monotherapy vs. combination | Lower immunogenicity, and combination therapy superior |
| UC-SUCCESS [57] | Randomized trial | UC patients on infliximab and azathioprine | Monotherapy vs. combination | Results similar to SONIC |
| COMMIT [58] | Randomized trial | CD patients on infliximab and methotrexate | Monotherapy vs. combination | Lower immunogenicity but no significant difference in clinical outcomes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, S.; Yarur, A.J. A Review of Therapeutic Drug Monitoring in Patients with Inflammatory Bowel Disease Receiving Combination Therapy. J. Clin. Med. 2023, 12, 6577. https://doi.org/10.3390/jcm12206577
Patel S, Yarur AJ. A Review of Therapeutic Drug Monitoring in Patients with Inflammatory Bowel Disease Receiving Combination Therapy. Journal of Clinical Medicine. 2023; 12(20):6577. https://doi.org/10.3390/jcm12206577
Chicago/Turabian StylePatel, Sanket, and Andres J. Yarur. 2023. "A Review of Therapeutic Drug Monitoring in Patients with Inflammatory Bowel Disease Receiving Combination Therapy" Journal of Clinical Medicine 12, no. 20: 6577. https://doi.org/10.3390/jcm12206577
APA StylePatel, S., & Yarur, A. J. (2023). A Review of Therapeutic Drug Monitoring in Patients with Inflammatory Bowel Disease Receiving Combination Therapy. Journal of Clinical Medicine, 12(20), 6577. https://doi.org/10.3390/jcm12206577