

Distinct Food Triggers for Migraine, Medication Overuse Headache and Irritable Bowel Syndrome
 , , and
, , and
Abstract
:1. Introduction
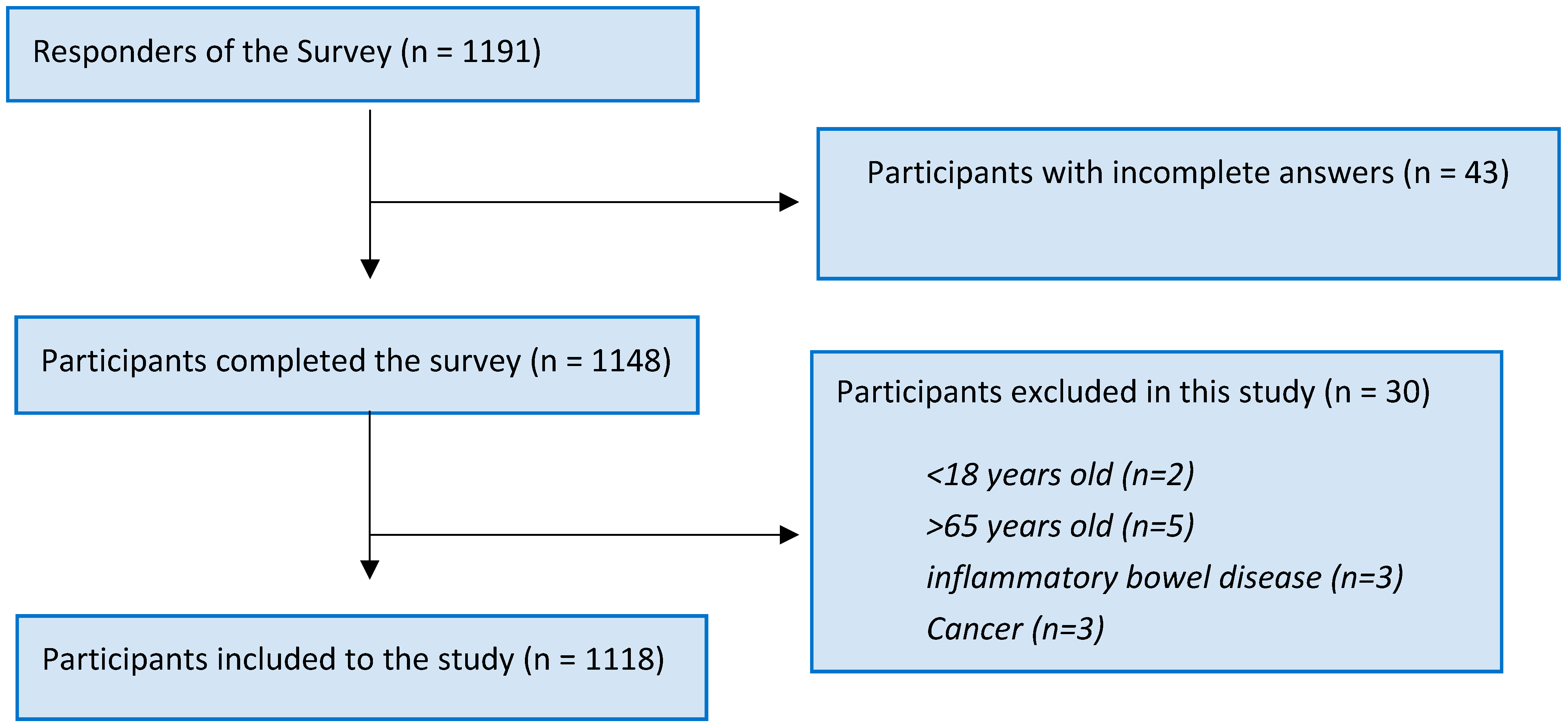
2. Methods
2.1. Study Design and Data Collection
2.2. Statistical Analysis
3. Results
Characteristics of the Study Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ertas, M.; Baykan, B.; Orhan, E.K.; Zarifoglu, M.; Karli, N.; Saip, S.; Onal, A.E.; Siva, A. One-year prevalence and the impact of migraine and tension-type headache in Turkey: A nationwide home-based study in adults. J. Headache Pain 2012, 13, 147–157. [Google Scholar] [CrossRef]
- Kelman, L. The triggers or precipitants of the acute migraine attack. Cephalalgia 2007, 27, 394–402. [Google Scholar] [CrossRef]
- Cole, J.A.; Rothman, K.J.; Cabral, H.J.; Zhang, Y.; Farraye, F.A. Migraine, fibromyalgia, and depression among people with IBS: A prevalence study. BMC Gastroenterol. 2006, 6, 26. [Google Scholar] [CrossRef]
- Sayuk, G.S.; Wolf, R.; Chang, L. Comparison of Symptoms, Healthcare Utilization, and Treatment in Diagnosed and Undiagnosed Individuals With Diarrhea-Predominant Irritable Bowel Syndrome. Am. J. Gastroenterol. 2017, 112, 892–899. [Google Scholar] [CrossRef]
- Chang, F.Y.; Lu, C.L. Irritable bowel syndrome and migraine: Bystanders or partners? J. Neurogastroenterol. Motil. 2013, 19, 301–311. [Google Scholar] [CrossRef]
- Sandler, R.S.; Everhart, J.E.; Donowitz, M.; Adams, E.; Cronin, K.; Goodman, C.; Gemmen, E.; Shah, S.; Avdic, A.; Rubin, R. The burden of selected digestive diseases in the United States. Gastroenterology 2002, 122, 1500–1511. [Google Scholar] [CrossRef]
- Kim, B.K.; Cho, S.; Kim, H.Y.; Chu, M.K. Validity and reliability of the self-administered Visual Aura Rating Scale questionnaire for migraine with aura diagnosis: A prospective clinic-based study. Headache 2021, 61, 863–871. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef]
- Schmulson, M.J.; Drossman, D.A. What Is New in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151–163. [Google Scholar] [CrossRef]
- Arici DÜZ, Ö.; Sari, S.; KiliÇ, Ş.; Helvaci Yilmaz, N.; ÖZge, A.; Polat, B.; TaŞDelen, B. Validity and Reliability of the Turkish Version of the Mig-Scog Scale in Migraine Patients. Neurol. Sci. Neurophysiol. 2020, 37, 29–35. [Google Scholar]
- Agrawal, R.; Srikant, R. Fast Algorithms for Mining Association Rules in Large Databases. In Proceedings of the Very Large Data Bases Conference, San Jose, CA, USA, 12–15 September 1994. [Google Scholar]
- Eagle, K. Toxicological effects of red wine, orange juice, and other dietary SULT1A inhibitors via excess catecholamines. Food Chem. Toxicol. 2012, 50, 2243–2249. [Google Scholar] [CrossRef]
- Rahul; Siddique, Y.H. Neurodegenerative Diseases and Flavonoids: Special Reference to Kaempferol. CNS Neurol. Disord. Drug Targets 2021, 20, 327–342. [Google Scholar] [CrossRef]
- Arai, Y.; Watanabe, S.; Kimira, M.; Shimoi, K.; Mochizuki, R.; Kinae, N. Dietary intakes of flavonols, flavones and isoflavones by Japanese women and the inverse correlation between quercetin intake and plasma LDL cholesterol concentration. J. Nutr. 2000, 130, 2243–2250. [Google Scholar] [CrossRef]
- Calis, Z.; Mogulkoc, R.; Baltaci, A.K. The Roles of Flavonols/Flavonoids in Neurodegeneration and Neuroinflammation. Mini Rev. Med. Chem. 2020, 20, 1475–1488. [Google Scholar] [CrossRef]
- Zeng, Y.; Pu, X.; Yang, J.; Du, J.; Yang, X.; Li, X.; Li, L.; Zhou, Y.; Yang, T. Preventive and Therapeutic Role of Functional Ingredients of Barley Grass for Chronic Diseases in Human Beings. Oxidative Med. Cell. Longev. 2018, 2018, 3232080. [Google Scholar] [CrossRef]
- Braidot, E.; Zancani, M.; Petrussa, E.; Peresson, C.; Bertolini, A.; Patui, S.; Macrì, F.; Vianello, A. Transport and accumulation of flavonoids in grapevine (Vitis vinifera L.). Plant Signal. Behav. 2008, 3, 626–632. [Google Scholar] [CrossRef]
- Soussi, M.; El Yaagoubi, W.; Nekhla, H.; El Hanafi, L.; Squalli, W.; Benjelloun, M.; El Ghadraoui, L. A Multidimensional Review of Pimpinella anisum and Recommendation for Future Research to Face Adverse Climatic Conditions. Chem. Afr. 2023, 6, 1727–1746. [Google Scholar] [CrossRef]
- Black, C.J.; Ford, A.C. Global burden of irritable bowel syndrome: Trends, predictions and risk factors. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 473–486. [Google Scholar] [CrossRef]
- Canavan, C.; West, J.; Card, T. The epidemiology of irritable bowel syndrome. Clin. Epidemiol. 2014, 6, 71–80. [Google Scholar] [CrossRef]
- Locke, G.R., 3rd; Zinsmeister, A.R.; Talley, N.J.; Fett, S.L.; Melton, L.J. Risk factors for irritable bowel syndrome: Role of analgesics and food sensitivities. Am. J. Gastroenterol. 2000, 95, 157–165. [Google Scholar] [CrossRef]
- Sigthorsson, G.; Tibble, J.; Hayllar, J.; Menzies, I.; Macpherson, A.; Moots, R.; Scott, D.; Gumpel, M.J.; Bjarnason, I. Intestinal permeability and inflammation in patients on NSAIDs. Gut 1998, 43, 506–511. [Google Scholar] [CrossRef]
- Bhatt, A.P.; Gunasekara, D.B.; Speer, J.; Reed, M.I.; Peña, A.N.; Midkiff, B.R.; Magness, S.T.; Bultman, S.J.; Allbritton, N.L.; Redinbo, M.R. Nonsteroidal Anti-Inflammatory Drug-Induced Leaky Gut Modeled Using Polarized Monolayers of Primary Human Intestinal Epithelial Cells. ACS Infect. Dis. 2018, 4, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Dağıdır, H.; Topa, E.; Vuralli, D.; Bolay, H. Medication Overuse Headache is Associated with Elevated Lipopolysaccharide Binding Protein and Pro-inflammatory Molecules in the Bloodstream. J. Headache Pain, 2023; in press. [Google Scholar] [CrossRef]
- Vuralli, D.; Arslan, B.; Topa, E.; de Morais, A.L.; Gulbahar, O.; Ayata, C.; Bolay, H. Migraine susceptibility is modulated by food triggers and analgesic overuse via sulfotransferase inhibition. J. Headache Pain 2022, 23, 36. [Google Scholar] [CrossRef] [PubMed]
- Błaszczyk, B.; Straburzyński, M.; Więckiewicz, M.; Budrewicz, S.; Niemiec, P.; Staszkiewicz, M.; Waliszewska-Prosół, M. Relationship between alcohol and primary headaches: A systematic review and meta-analysis. J. Headache Pain. 2023, 24, 116. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.J.; Stovner, L.J.; Vos, T.; Jensen, R.; Katsarava, Z. Migraine is first cause of disability in under 50s: Will health politicians now take notice? J. Headache Pain 2018, 19, 17. [Google Scholar] [CrossRef]
- Vuralli, D.; Ayata, C.; Bolay, H. Cognitive dysfunction and migraine. J. Headache Pain 2018, 19, 109. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Migraine | MOH | IBS | Participants without Headache | |
|---|---|---|---|---|
| n (%) | 984 (88.0%) | 344 (30.7%) | 560 (50.2%) | 134 (12.0%) |
| Age (years), mean ± SD | 33.96 ± 11.1 | 35.01 ± 11.1 | 32.92 ± 11.1 | 33.20 ± 12.5 |
| Woman, n (%) | 731 (75.0%) | 293 (80.7%) | 436 (77.9%) | 62 (51.7%) |
| Education/University graduate, n (%) | 267 (73.6%) | 757 (76.9%) | 407 (72.7%) | 86 (71.7%) |
| Body Mass Index, mean ± SD | 24.38 ± 5.8 | 24.15 ± 4.1 | 24.47 ± 6.8 | 24.28 ± 7.6 |
| Foods | Food Content | Main Related Neurotransmitter | Flavonoids | SULT Inhibition | Additives ** |
|---|---|---|---|---|---|
| Bakery (bread, simit, etc.) | Wheat Yeast Egg Gluten | Dopamine Histamine | Apigenin | SULT1A1 | In packaged breads (Caramels, sorbic acid, propionic acid, phosphoric acid, acetic acid, stearol -2-lactylates, tartaric acid of mono and diglycerides of fatty acids esters, lactic acid) |
| Milk and milk products (Cheese, yoghurt, heavy cream, etc.) | Casein, whey Tyrosine Lactose Vitamins (A, B, D) Minerals (Ca, Mg, P…) | Dopamine Histamine | - | - | Carrageenan, Polyphosphates, Potassium sorbate, trisodium sorbate, calcium gluconate, sodium citrates, succinic acid, sucrose esters of fatty acids |
| Olives [12] | Fatty acid Oleic acid Linoleic acid Synapic acid Vanillic acid Cyanidin-3 rutinosid | Dopamine | Apigenin Luteolin Olueropein | SULT1A1 SULT1A3 | - |
| Apple | Chlorogenic acid Pectin Ursolic acid Anthocyanin | Dopamine | Quercetin Kaempferol | SULT1A1 | - |
| Apricot | Beta- carotene Carotenoids Ferulic acid Beta-sitosterol | Dopamine | Quercetin Kaempferol | SULT1A1 | - |
| Banana | Caffeic acid Chlorogenic acid Carotenoids | Dopamine | Quercetin Kaempferol | SULT1A1 SULT1A3 | - |
| Watermelon | Lycopene Cucurbitacin Citrulline Carotenoids Lutein | Dopamine | Luteolin Kaempferol | SULT1A1 | - |
| Citrus | Ascorbic acid Limonoids Carotenoids Lutein Tangerine | Dopamine | Hesperidin Naringin | SULT1A1 SULT1A3 | - |
| Cherry | Caffeic acid Chlorogenic acid Anthocyanin Melatonin Ascorbic acid | Dopamine | Quercetin | SULT1A1 | - |
| Strawberry [13] | Ellagitannins Anthocyanin | Dopamine Histamine | Quercetin Kaempferol Catechin Ficetin | SULT1A1 | - |
| Grapefruit | Limonen Naringenin Lycopene Vitamins (A, B9, C…) | Dopamine | Hesperidin Quercetin Apigenin | SULT1A1 SULT1A3 | - |
| Red grapes | Ellagic acid Vitamins (C, K, B6, B9…) Minerals (Magnesium, Potassium…) | Dopamine | Quercetin Kaempferol Catechin Resveratrol Apigenin | SULT1A1 SULT1A3 | - |
| Pomegranate | Punicalagin Ellagic acid Anthocyanin Flavonoids Vitamins (C, K…) Minerals( Potassium, Calcium, Iron…) | Dopamine | Quercetin Kaempferol Myricetin | SULT1A1 | - |
| Tomatoes | Lycopene Carotenoids Malic acid Citric acid | Dopamine Histamine | Quercetin Kaempferol | SULT1A1 | - |
| Onion/Garlic | Sulfur, organosulfur compounds Saponins Allicin | Dopamine | Quercetin Kaempferol | SULT1A1 SULT1A3 | - |
| Cabbage | Glucosinolates Sulphoraphane Indol- 3 carbinol Vitamins (vitamin C, B9…) Minerals (Calcium, Iron, Magnesium…) | Dopamine | Quercetin Kaempferol Apigenin | SULT1A1 | - |
| Spinach | Zeaxantine Carotenoids Vitamins (K, C, B9…) | Histamine Dopamine | Luteolin | SULT1A1 | - |
| Eggplant | Anthocyanin Chlorogenic acid Nicotine | Histamine Dopamine | Nasunin Quercetin Lutein Rutin | SULT1A1 | - |
| Lentils | Phytoesterols Lignans | Dopamine Histamine | Quercetin Kaempferol Myricetin | SULT1A1 | - |
| Nuts | Eflvanoids Proanthocyanidins Phytosterols Omega-3 fatty acids Alfa tocopherol | Histamine Dopamine | Quercetin Kaempferol | SULT1A1 | - |
| Canned foods | Acetic acid salts | It varies according to the type of food | Benzoic acid Sulfur dioxide Bisphenol A (BPA)- in tin cans | ||
| French fries [14] | Carotenoids Chlorogenic acid Caffeic acid | Quercetin Kaempferol | SULT1A1 | May contain sodium bisulfite, nitrite, nitrate if it is frozen | |
| Ketchup | Lycopene Carotenoids Malic acid Citric acid Lactic acid | Dopamine Histamine | Benzoic acid, tartrazine, modified cornstarch Xanthan gum Guar gum | ||
| Mayonnaise | Egg Yoghurt Garlic Olive oil | Dopamine Histamine | Sodium benzoate, benzoic acid Potassium sorbate Ethylene diamine tetra acetates (EDTA) Sulfur dioxide Carrageenan Colorants Modified cornstarch Sorbic acid Xanthan gum | ||
| Soy sauce | Soybean (Phytosterol, flavonoids, saponin) Wheat Salt Vinegar | Dopamine Histamine | Apigenin Luteolin | SULT1A1 | Monosodium glutamate (MSG) Citric acid |
| Mustard [15] | Mustard seed (glucosinolate, sinigrin, Sulphoraphane, isothiocyanates, phenolic acids, flavonoids) Salt Vinegar High fructose syrup | Dopamine Histamine | Quercetin Kaempferol Catechin Myricetin | Sodium benzoate, sodium metabisulfite Carrageenan Colorants Modified cornstarch Sorbic acid Xanthan gum | |
| Beer [16] | Barley (Flavonoids, Polyphenols, Saponarin, Kutonarin, Superoxide dismutase (SOD), GABA, Tryptophan) Malt Gluten Yeast Ethanol | Dopamine | Quercetin Kaempferol Myricetin | SULT1A1 | Carbon dioxide Congener Benzoic acid, benzoates Sorbic acid, sorbates Sulfur dioxide Lactic acid Caramels Propane-1-2- diol alginate |
| Red wine [12] | Red grape Ethanol Yeast Tannin | Dopamine Histamine | Epicatechin gallate Resveratrol | SULT1A1 SULT1A3 | Carbon dioxide Congener Benzoic acid, benzoates Sorbic acid, sorbates Phosphoric acid Sucrose esters of fatty acids Synthetic colorants |
| White wine | White grape [17] Ethanol Yeast Tannin | Dopamine Histamine | Naringenin Anthocyanin | SULT1A1 | Carbon dioxide Benzoic acid, benzoates Sorbic acid, sorbates Phosphoric acid Sucrose esters of fatty acids Synthetic colorants |
| Rakı [18] | Pimpinella anisum Ethanol Tannin | Dopamine | Quercetin Luteolin Izoretientin Izovitexin | SULT1A1 | Sulphite |
| Chocolate/Cocoa | Cocoa mass Egg products Gluten Sugar Butter oil (from milk) Palm oil | Dopamine | Quercetin Vanillin | SULT1A1 | Soy lecithin Polyglycerol polyricinoleate |
| Coffee | Caffeic acid Quinic acid Chlorogenic acid | Dopamine | Trigonelline (coffee beans) | SULT1A1 SULT1A3 | Dipotassium phosphate Sodium polyphosphate Silicon dioxide Pentasodiumtriphosphate Acacia gum Sodium aluminum silicate |
| Carmosine [12] (Red food dye) | Dopamine | SULT1A1 | Synthetic colorant, E122 | ||
| Artificially sweetened snacks | It may contain palm oil, gluten, cocoa, cream, sugar depending on the product. | Tartrazine, Brilliant blue FCF, carmosine, Green S Aspartame Sucralose Neohesperidin C | |||
| Meat/Chicken Bouillon | Salt, sugar, beef fat, dried chicken meat, chicken fat, parsley, soybean oil, whey, sodium caseinate | Monosodium glutamate (MSG), Corn starch, hydrolyzed corn protein, autolyzed yeast extract, disodium inosinate, disodium guanylate, citric acid, onion powder, yellow 5, yellow 6, Anotta | |||
| Packaged juice | Apple, apricot, cherry, watermelon, etc. Sodium salt Potassium salt High fructose syrup | Dopamine Histamine | Hesperidin Quercetin Kaempferol | SULT1A1 SULT1A3 | Acesulfame KA Acesulfame K Aspartame Saccharin Sucralose Carboxy methyl cellulose Sorbic acid, sorbates |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceren Akgor, M.; Vuralli, D.; Sucu, D.H.; Gokce, S.; Tasdelen, B.; Gultekin, F.; Bolay, H. Distinct Food Triggers for Migraine, Medication Overuse Headache and Irritable Bowel Syndrome. J. Clin. Med. 2023, 12, 6488. https://doi.org/10.3390/jcm12206488
Ceren Akgor M, Vuralli D, Sucu DH, Gokce S, Tasdelen B, Gultekin F, Bolay H. Distinct Food Triggers for Migraine, Medication Overuse Headache and Irritable Bowel Syndrome. Journal of Clinical Medicine. 2023; 12(20):6488. https://doi.org/10.3390/jcm12206488
Chicago/Turabian StyleCeren Akgor, Merve, Doga Vuralli, Damla Hazal Sucu, Saliha Gokce, Bahar Tasdelen, Fatih Gultekin, and Hayrunnisa Bolay. 2023. "Distinct Food Triggers for Migraine, Medication Overuse Headache and Irritable Bowel Syndrome" Journal of Clinical Medicine 12, no. 20: 6488. https://doi.org/10.3390/jcm12206488
APA StyleCeren Akgor, M., Vuralli, D., Sucu, D. H., Gokce, S., Tasdelen, B., Gultekin, F., & Bolay, H. (2023). Distinct Food Triggers for Migraine, Medication Overuse Headache and Irritable Bowel Syndrome. Journal of Clinical Medicine, 12(20), 6488. https://doi.org/10.3390/jcm12206488