
The Greifswald Post COVID Rehabilitation Study and Research (PoCoRe)–Study Design, Characteristics and Evaluation Tools

 , , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , , and add
Show full author list
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
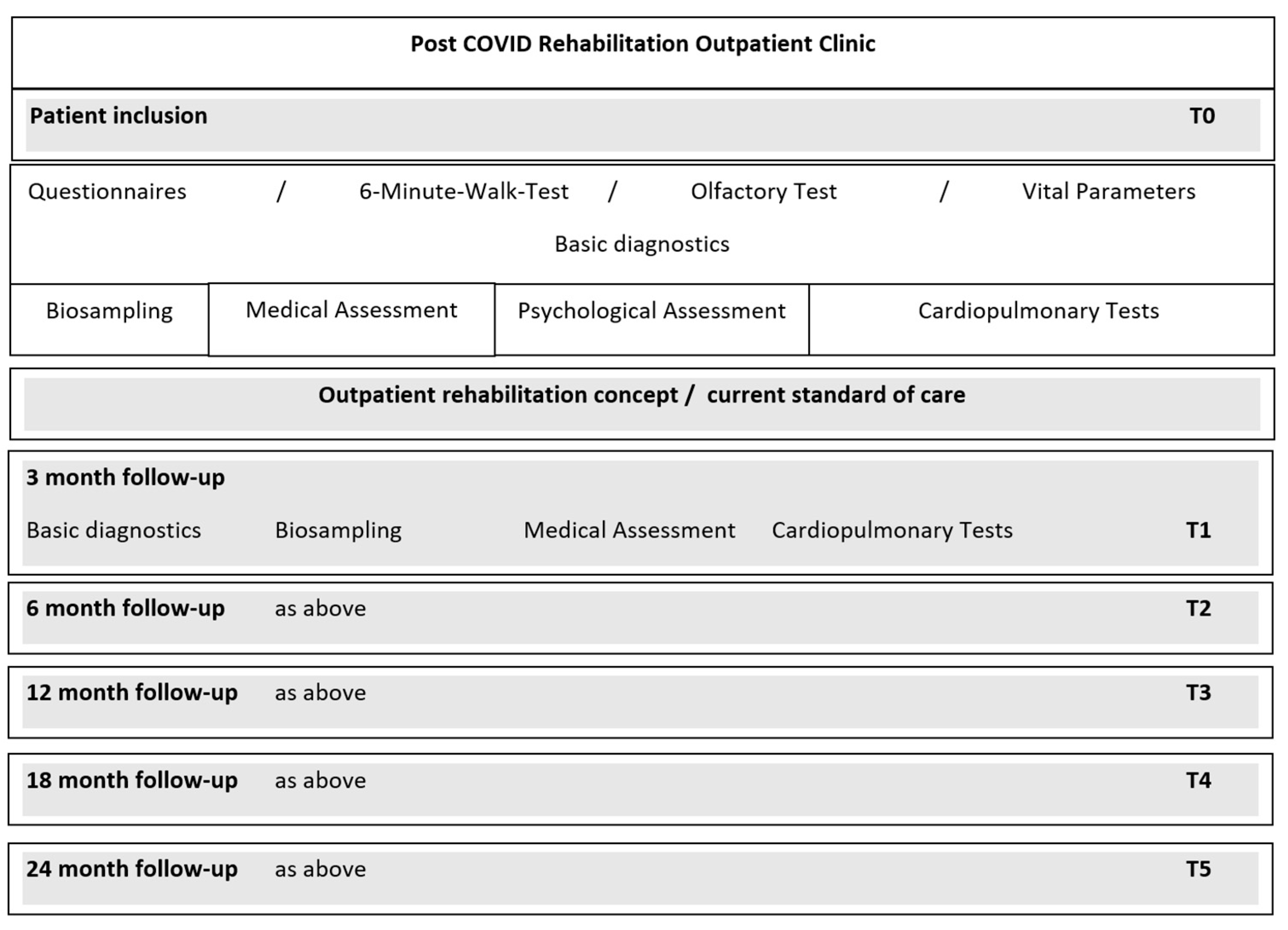
2.1. Study Design
2.2. Eligibility Criteria
2.3. Ethics
2.4. Study Population
2.5. Study Procedures
2.5.1. Standardized Medical History Assessment and Medical Examination (PoCoRe Outpatient Clinic)
2.5.2. Vital Parameters and Physical Function Diagnostics
Vital Parameters
Six-Minute Walk Test
Ethyl Alcohol Threshold Test
Laboratory Measures and Biobanking
2.5.3. Questionnaires
- -
- MEDIAN Corona Recovery Score (GAD-7; PHQ-9, ITQ Part 1, critical life events),
- -
- Fatigue Assessment Scale
- -
- Veterans Rand 12-item Health SurveyThe COPD Assessment Test, the Post-COVID-19 Functional Status Scale as the well as the Montreal Cognitive Assessment are carried out by the medical staff during the consultation.
- -
- Twenty-Item Toronto Alexithymia Scale
- -
- Childhood Trauma Screener
- -
- Generalized Resistance Resources (self-efficacy beliefs, stress experiences, self-esteem-short-scale, optimism-short-scale, social support-short scale, sense of coherence)
Median Corona Recovery Score
Generalized Anxiety Disorder (GAD-7)
Patient Health Questionnaire–Depression Module (PHQ-9)
International Trauma Questionnaire-Part I (Posttraumatic Stress Disorder)
COPD Assessment Test
Post-COVID-19 Functional Status Scale
Fatigue Assessment Scale (FAS)
Montreal Cognitive Assessment (MoCA)
Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE)
Veterans Rand 12-Item Health Survey/Health-Related Quality of Life (HrQol)
Twenty-ITEM Toronto Alexithymia Scale (TAS-20)
Childhood Trauma Screener (CTS)
Generalized Resistance Resources (GRRs)
- Self-Efficacy Beliefs
- Stress Experiences
- Self-Esteem-Short-Scale
- Optimism-Short-Scale
- Social Support-Short Scale
- Sense of Coherence
2.5.4. Cardiopulmonary Examination Modules
Anthropometric Parameters
Arm, Thigh and Lower Leg Measurement
Ultrasound Measurement of Mid and Two Third of Upper Thigh
Bioelectrical Impedance Analysis (BIA)
Handgrip Strength
Pulmonary Function
Echocardiography
Pulse Wave Analysis and of Vascular Stiffness
2.5.5. Data Collection, Management and Analysis
3. Discussion
3.1. Limitations and Biases
3.2. Perspective
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Post COVID-19 Condition (Long COVID). Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on 5 October 2022).
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Giurgi-Oncu, C.; Tudoran, C.; Pop, G.N.; Bredicean, C.; Pescariu, S.A.; Giurgiuca, A.; Tudoran, M. Cardiovascular Abnormalities and Mental Health Difficulties Result in a Reduced Quality of Life in the Post-Acute COVID-19 Syndrome. Brain Sci. 2021, 11, 1456. [Google Scholar] [CrossRef] [PubMed]
- Petersen, E.L.; Goßling, A.; Adam, G.; Aepfelbacher, M.; Behrendt, C.-A.; Cavus, E.; Cheng, B.; Fischer, N.; Gallinat, J.; Kühn, S.; et al. Multi-organ assessment in mainly non-hospitalized individuals after SARS-CoV-2 infection: The Hamburg City Health Study COVID programme. Eur. Heart J. 2022, 43, 1124–1137. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.D.; Lavelle, M.; Boursiquot, B.C.; Wan, E.Y. Long-term complications of COVID-19. Am. J. Physiol. Cell Physiol. 2022, 322, C1–C11. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef]
- Nittas, V.; Gao, M.; West, E.A.; Ballouz, T.; Menges, D.; Wulf Hanson, S.; Puhan, M.A. Long COVID through a Public Health Lens: An Umbrella Review. Public Health Rev. 2022, 43, 1604501. [Google Scholar] [CrossRef]
- WMA. Deklaration von Helsinki. Available online: http://www.bundesaerztekammer.de/fileadmin/user_upload/Deklaration_von_Helsinki_2013_DE.pdf (accessed on 10 October 2022).
- Calvo-Henriquez, C.; Maldonado-Alvarado, B.; Chiesa-Estomba, C.; Rivero-Fernández, I.; Sanz-Rodriguez, M.; Villarreal, I.M.; Rodriguez-Iglesias, M.; Mariño-Sánchez, F.; Rivero-de-Aguilar, A.; Lechien, J.R.; et al. Ethyl alcohol threshold test: A fast, reliable and affordable olfactory Assessment tool for COVID-19 patients. Eur. Arch. Otorhinolaryngol. 2020, 277, 2783–2792. [Google Scholar] [CrossRef]
- Winter, T.; Friedrich, N.; Lamp, S.; Schäfer, C.; Schattschneider, M.; Bollmann, S.; Brümmer, D.; Riemann, K.; Petersmann, A.; Nauck, M. The Integrated Research Biobank of the University Medicine Greifswald. Open J. Bioresour. 2020, 7, Art. 2. [Google Scholar] [CrossRef]
- Altmann, C.; Schröter, J.; Nagel, S.; Schueth, S. MEDIAN Corona Recovery Score (MCRS). Available online: https://www.median-kliniken.de/fileadmin/user_upload/median-global/pdf-median-global/MEDIAN_Corona_Recovery_Score_Manual_EN.pdf (accessed on 5 October 2022).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Hinz, A.; Klein, A.M.; Brähler, E.; Glaesmer, H.; Luck, T.; Riedel-Heller, S.G.; Wirkner, K.; Hilbert, A. Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J. Affect. Disord. 2017, 210, 338–344. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A New Depression Diagnostic and Severity Measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.J.; Richards, J.S. Factor structure of the PHQ-9 screen for depression across time since injury among persons with spinal cord injury. Rehabil. Psychol. 2008, 53, 243–249. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Cloitre, M.; Hyland, P.; Prins, A.; Shevlin, M. The international trauma questionnaire (ITQ) measures reliable and clinically significant treatment-related change in PTSD and complex PTSD. Eur. J. Psychotraumatol. 2021, 12, 1930961. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.-H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Daynes, E.; Gerlis, C.; Briggs-Price, S.; Jones, P.; Singh, S.J. COPD assessment test for the evaluation of COVID-19 symptoms. Thorax 2021, 76, 185–187. [Google Scholar] [CrossRef]
- Boon, G.J.A.M.; Barco, S.; Bertoletti, L.; Ghanima, W.; Huisman, M.V.; Kahn, S.R.; Noble, S.; Prandoni, P.; Rosovsky, R.P.; Sista, A.K.; et al. Measuring functional limitations after venous thromboembolism: Optimization of the Post-VTE Functional Status (PVFS) Scale. Thromb. Res. 2020, 190, 45–51. [Google Scholar] [CrossRef]
- Bayat, M.; Raeissadat, S.A.; Lashgari, S.; Bolandnazar, N.S.; Taheri, S.N.; Soleimani, M. Post-COVID-19 functional limitations in hospitalized patients and associated risk factors: A 3-month follow-up study. Physiother. Res. Int. 2022, 27, e1965. [Google Scholar] [CrossRef]
- Benkalfate, N.; Eschapasse, E.; Georges, T.; Leblanc, C.; Dirou, S.; Melscoet, L.; Chéné, A.-L.; Horeau-Langlard, D.; Bry, C.; Chambellan, A.; et al. Evaluation of the Post-COVID-19 Functional Status (PCFS) Scale in a cohort of patients recovering from hypoxemic SARS-CoV-2 pneumonia. BMJ Open Respir. Res. 2022, 9, e001136. [Google Scholar] [CrossRef] [PubMed]
- Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Vaes, A.W.; Goërtz, Y.M.J.; van Herck, M.; Houben-Wilke, S.; Boon, G.J.A.M.; Barco, S.; Burtin, C.; et al. Construct validity of the Post-COVID-19 Functional Status Scale in adult subjects with COVID-19. Health Qual. Life Outcomes 2021, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Torres, L.A.; Ventura-Alfaro, C.E. Validation of the Post-COVID-19 Functional Status Scale into Mexican-Spanish. J. Rehabil. Med. Clin. Commun. 2021, 4, 1000070. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Boon, G.J.A.M.; Barco, S.; Endres, M.; Geelhoed, J.J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status scale: A tool to measure functional status over time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef] [PubMed]
- Michielsen, H.J.; de Vries, J.; van Heck, G.L. Psychometric qualities of a brief self-rated fatigue measure. J. Psychosom. Res. 2003, 54, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Thams, F.; Antonenko, D.; Fleischmann, R.; Meinzer, M.; Grittner, U.; Schmidt, S.; Brakemeier, E.-L.; Steinmetz, A.; Flöel, A. Neuromodulation through brain stimulation-assisted cognitive training in patients with post-COVID-19 cognitive impairment (Neuromod-COV): Study protocol for a PROBE phase IIb trial. BMJ Open 2022, 12, e055038. [Google Scholar] [CrossRef]
- Jorm, A.F. The Informant Questionnaire on cognitive decline in the elderly (IQCODE): A review. Int. Psychogeriatr. 2004, 16, 275–293. [Google Scholar] [CrossRef]
- Lim, H.J.; Lim, J.P.P.; Anthony, P.; Yeo, D.H.H.; Sahadevan, S. Prevalence of cognitive impairment amongst Singapore’s elderly Chinese: A community-based study using the ECAQ and the IQCODE. Int. J. Geriatr. Psychiatry 2003, 18, 142–148. [Google Scholar] [CrossRef]
- Buchholz, I.; Feng, Y.-S.; Buchholz, M.; Kazis, L.E.; Kohlmann, T. Translation and adaptation of the German version of the Veterans Rand-36/12 Item Health Survey. Health Qual. Life Outcomes 2021, 19, 137. [Google Scholar] [CrossRef]
- Oak, S.R.; Strnad, G.J.; Bena, J.; Farrow, L.D.; Parker, R.D.; Jones, M.H.; Spindler, K.P. Responsiveness Comparison of the EQ-5D, PROMIS Global Health, and VR-12 Questionnaires in Knee Arthroscopy. Orthop. J. Sport. Med. 2016, 4, 2325967116674714. [Google Scholar] [CrossRef] [PubMed]
- Bagby, R.; Parker, J.D.; Taylor, G.J. The twenty-item Toronto Alexithymia scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.; Popp, K.; Schaefer, R.; Sitte, W.; Schneider, C.; Hardt, J.; Decker, O.; Braehler, E. Alexithymia in the German general population. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.J.; Bagby, R.; Parker, J.D. The 20-Item Toronto Alexithymia Scale. J. Psychosom. Res. 2003, 55, 277–283. [Google Scholar] [CrossRef]
- Grabe, H.J.; Schulz, A.; Schmidt, C.O.; Appel, K.; Driessen, M.; Wingenfeld, K.; Barnow, S.; Spitzer, C.; John, U.; Berger, K.; et al. Ein Screeninginstrument für Missbrauch und Vernachlässigung in der Kindheit: Der Childhood Trauma Screener (CTS). Psychiatr. Prax. 2012, 39, 109–115. [Google Scholar] [CrossRef]
- Glaesmer, H.; Schulz, A.; Häuser, W.; Freyberger, H.J.; Brähler, E.; Grabe, H.-J. Der Childhood Trauma Screener (CTS)—Entwicklung und Validierung von Schwellenwerten zur Klassifikation. Psychiatr. Prax. 2013, 40, 220–226. [Google Scholar] [CrossRef]
- Klinger-König, J.; Streit, F.; Erhardt, A.; Kleineidam, L.; Schmiedek, F.; Schmidt, B.; Investigators, N.; Wagner, M.; Deckert, J.; Rietschel, M.; et al. The assessment of childhood maltreatment and its associations with affective symptoms in adulthood: Results of the German National Cohort (NAKO). World J. Biol. Psychiatry 2022, 1–12, online ahead of print. [Google Scholar] [CrossRef]
- Beierlein, C.; Kemper, C.J.; Kovaleva, A.; Rammstedt, B. Short Scale for Measuring General Self-efficacy Beliefs (ASKU). Methods Data Anal. 2017, 7, 1–28. [Google Scholar]
- Satow, L. Stress- und Coping-Inventar (SCI): Vollständige Test- und Skalendokumentation: [Stress and Coping-Inventory (SCI): Complete Test and Scale Documentation]. Available online: http://www.drsatow.de/tests/stress-und-coping-inventar/ (accessed on 10 October 2022).
- Robins, R.W.; Hendin, H.M.; Trzesniewski, K.H. Measuring Global Self-Esteem: Construct Validation of a Single-Item Measure and the Rosenberg Self-Esteem Scale. Pers. Soc. Psychol. Bull. 2001, 27, 151–161. [Google Scholar] [CrossRef]
- Glaesmer, H.; Hoyer, J.; Klotsche, J.; Herzberg, P.Y. Die deutsche Version des Life-Orientation-Tests (LOT-R) zum dispositionellen Optimismus und Pessimismus. Z. Für Gesundh. 2008, 16, 26–31. [Google Scholar] [CrossRef]
- Fydrich, T.; Geyer, M.; Hessel, A.; Sommer, G.; Brähler, E. Fragebogen zur Sozialen Unterstützung (F-SozU): Normierung an einer repräsentativen Stichprobe. Diagnostica 1999, 45, 212–216. [Google Scholar] [CrossRef]
- Fydrich, T.; Sommer, G.; Tydecks, S.; Brähler, E. Fragebogen zur sozialen Unterstützung (F-SozU): Normierung der Kurzform (K-14)Social Support Questionnaire (F-SozU): Standardization of short form (K-14). Z. Für Med. Psychol. 2009, 18, 43–48. [Google Scholar]
- Schumacher, J.; Wilz, G.; Gunzelmann, T.; Brähler, E. Die Sense of Coherence Scale von Antonovsky. Teststatistische Uberprüfung in einer repräsentativen Bevölkerungsstichprobe und Konstruktion einer Kurzskala. Psychother. Psychosom. Med. Psychol. 2000, 50, 472–482. [Google Scholar] [CrossRef] [PubMed]
- DZHK. Echocardiography Standard Operating Procedure: German Centre for Cardiovascular Research (DZHK) e.V., Partner Site Greifswald. Available online: https://dzhk.de/forschung/klinische-forschung/sops/ (accessed on 10 October 2022).
- Bull-Otterson, L.; Baca, S.; Saydah, S.; Boehmer, T.K.; Adjei, S.; Gray, S.; Harris, A.M. Post–COVID Conditions Among Adult COVID-19 Survivors Aged 18–64 and ≥65 Years—United States, March 2020–November 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 713–717. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent COVID-19 symptoms in a community study of 606,434 people in England. Nat. Commun. 2022, 13, 1957. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; Olde Hartman, T.C.; Rosmalen, J.G.M. Persistence of somatic symptoms after COVID-19 in the Netherlands: An observational cohort study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef]
- Roessler, M.; Tesch, F.; Batram, M.; Jacob, J.; Loser, F.; Weidinger, O.; Wende, D.; Vivirito, A.; Toepfner, N.; Ehm, F.; et al. Post-COVID-19-associated morbidity in children, adolescents, and adults: A matched cohort study including more than 157,000 individuals with COVID-19 in Germany. PLoS Med. 2022, 19, e1004122. [Google Scholar] [CrossRef]
- Peter, R.S.; Nieters, A.; Kräusslich, H.-G.; Brockmann, S.O.; Göpel, S.; Kindle, G.; Merle, U.; Steinacker, J.M.; Rothenbacher, D.; Kern, W.V. Post-acute sequelae of COVID-19 six to 12 months after infection: Population based study. BMJ 2022, 379, e071050. [Google Scholar] [CrossRef]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent Symptoms in Adult Patients 1 Year After Coronavirus Disease 2019 (COVID-19): A Prospective Cohort Study. Clin. Infect. Dis. 2022, 74, 1191–1198. [Google Scholar] [CrossRef]
- Saunders, C.; Sperling, S.; Bendstrup, E. A new paradigm is needed to explain long COVID. Lancet Respir. Med. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinmetz, A.; Bahlmann, S.; Bergelt, C.; Bröker, B.M.; Ewert, R.; Felix, S.B.; Flöel, A.; Fleischmann, R.; Hoffmann, W.; Holtfreter, S.; et al. The Greifswald Post COVID Rehabilitation Study and Research (PoCoRe)–Study Design, Characteristics and Evaluation Tools. J. Clin. Med. 2023, 12, 624. https://doi.org/10.3390/jcm12020624
Steinmetz A, Bahlmann S, Bergelt C, Bröker BM, Ewert R, Felix SB, Flöel A, Fleischmann R, Hoffmann W, Holtfreter S, et al. The Greifswald Post COVID Rehabilitation Study and Research (PoCoRe)–Study Design, Characteristics and Evaluation Tools. Journal of Clinical Medicine. 2023; 12(2):624. https://doi.org/10.3390/jcm12020624
Chicago/Turabian StyleSteinmetz, Anke, Susanne Bahlmann, Corinna Bergelt, Barbara M. Bröker, Ralf Ewert, Stephan B. Felix, Agnes Flöel, Robert Fleischmann, Wolfgang Hoffmann, Silva Holtfreter, and et al. 2023. "The Greifswald Post COVID Rehabilitation Study and Research (PoCoRe)–Study Design, Characteristics and Evaluation Tools" Journal of Clinical Medicine 12, no. 2: 624. https://doi.org/10.3390/jcm12020624
APA StyleSteinmetz, A., Bahlmann, S., Bergelt, C., Bröker, B. M., Ewert, R., Felix, S. B., Flöel, A., Fleischmann, R., Hoffmann, W., Holtfreter, S., Nauck, M., Riemann, K., Scheer, C., Stahl, D., Vogelgesang, A., Völker, U., Wiesmann, U., Klinger-König, J., Walk, R., ... Dörr, M. (2023). The Greifswald Post COVID Rehabilitation Study and Research (PoCoRe)–Study Design, Characteristics and Evaluation Tools. Journal of Clinical Medicine, 12(2), 624. https://doi.org/10.3390/jcm12020624