
Severe Intrahepatic Cholestasis of Pregnancy—Potential Mechanism by Which Fetuses Are Protected from the Hazardous Effect of Bile Acids



 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
Diagnosis and Management of Women with ICP
2.2. Study Population
2.3. Specimen Collection and Handling
2.4. TBA Assay
2.5. Data
2.6. Statistical Analysis
2.7. Ethical Approval
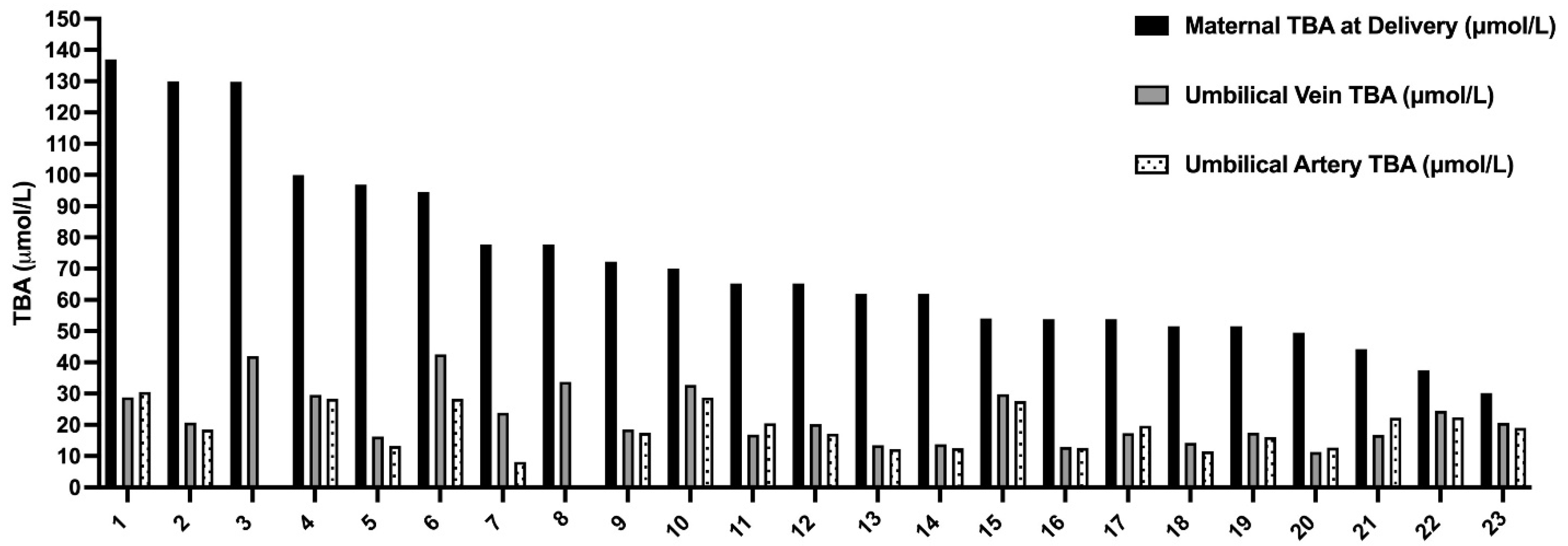
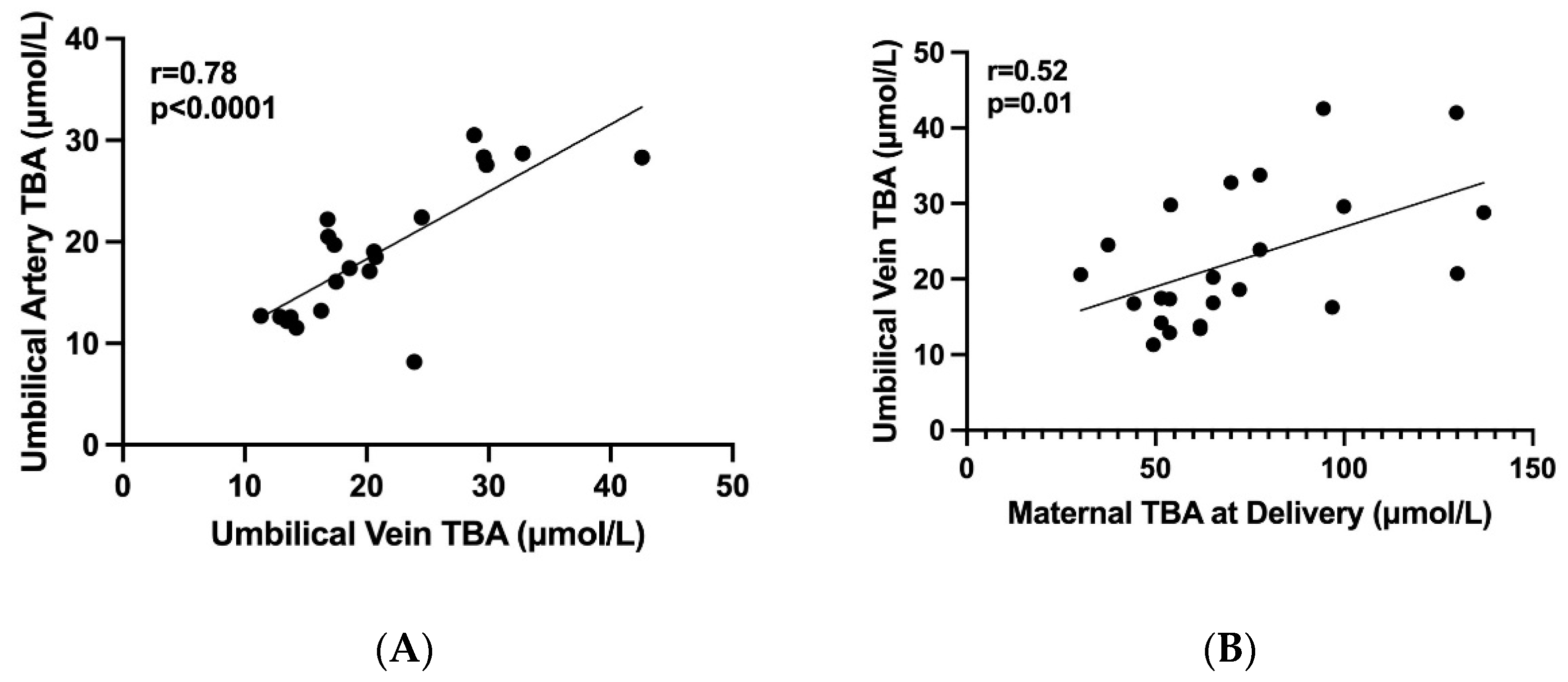
3. Results
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Smith, D.D.; Rood, K.M. Intrahepatic cholestasis of pregnancy. Clin. Obs. Gynecol. 2020, 63, 134–151. [Google Scholar] [CrossRef]
- Geenes, V.; Williamson, C. Intrahepatic cholestasis of pregnancy. WJG 2009, 15, 2049. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Li, Z.; Song, Y.; Sun, Y.; Shi, H.; Chen, D.; Zhang, Y. Pathogenesis of Intrahepatic Cholestasis of Pregnancy. Can. J. Gastroenterol. Hepatol. 2021, 30, 6679322. [Google Scholar]
- Piechota, J.; Jelski, W. Intrahepatic Cholestasis in Pregnancy: Review of the Literature. J. Clin. Med. 2020, 9, 1361. [Google Scholar] [CrossRef]
- Glantz, A.; Marschall, H.-U.; Mattsson, L.-A. Intrahepatic cholestasis of pregnancy: Relationships between bile acid levels and fetal complication rates. Hepatology 2004, 40, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Geenes, V.; Chappell, L.C.; Seed, P.T.; Steer, P.J.; Knight, M.; Williamson, C. Association of severe intrahepatic cholestasis of pregnancy with adverse pregnancy outcomes: A prospective population-based case-control study. Hepatology 2014, 59, 1482–1491. [Google Scholar] [CrossRef]
- Brouwers, L.; Koster, M.P.H.; Page-Christiaens, G.C.M.L.; Kemperman, H.; Boon, J.; Evers, I.M.; Bogte, A.; Oudijk, M.A. Intrahepatic cholestasis of pregnancy: Maternal and fetal outcomes associated with elevated bile acid levels. Am. J. Obstet. Gynecol. 2015, 212, 100.e1–100.e7. [Google Scholar] [CrossRef]
- Di Mascio, D.; Quist-Nelson, J.; Riegel, M.; George, B.; Saccone, G.; Brun, R.; Haslinger, C.; Herrera, C.; Kawakita, T.; Lee, R.H.; et al. Perinatal death by bile acid levels in intrahepatic cholestasis of pregnancy: A systematic review. J. Matern. Fetal. Neonatal. Med. 2021, 34, 3614–3622. [Google Scholar] [CrossRef]
- Ovadia, C.; Seed, P.T.; Sklavounos, A.; Geenes, V.; Di Ilio, C.; Chambers, J.; Kohari, K.; Bacq, Y.; Bozkurt, N.; Brun-Furrer, R.; et al. Association of adverse perinatal outcomes of intrahepatic cholestasis of pregnancy with biochemical markers: Results of aggregate and individual patient data meta-analyses. Lancet 2019, 393, 899–909. [Google Scholar] [CrossRef]
- Macias, R.I.R.; Marin, J.J.G.; Serrano, M.A. Excretion of biliary compounds during intrauterine life. World J. Gastroenterol. 2009, 15, 817–828. [Google Scholar] [CrossRef]
- Geenes, V.; Lövgren-Sandblom, A.; Benthin, L.; Lawrance, D.; Chambers, J.; Gurung, V.; Thornton, J.; Chappell, L.; Khan, E.; Dixon, P.; et al. The reversed feto-maternal bile acid gradient in intrahepatic cholestasis of pregnancy is corrected by ursodeoxycholic acid. PLoS ONE 2014, 9, e83828. [Google Scholar] [CrossRef]
- Mazzella, G.; Rizzo, N.; Azzaroli, F.; Simoni, P.; Bovicelli, L.; Miracolo, A.; Giuliana, S.; Antonio, C.; Giovanni, N.; Constance, M.; et al. Ursodeoxycholic acid administration in patients with cholestasis of pregnancy: Effects on primary bile acids in babies and mothers. Hepatology 2001, 33, 504–508. [Google Scholar] [CrossRef]
- Raz, Y.; Lavie, A.; Vered, Y.; Goldiner, I.; Skornick-Rapaport, A.; Asher, Y.L.; Maslovitz, S.; Levin, I.; Lessing, J.B.; Kuperminc, M.J.; et al. Severe intrahepatic cholestasis of pregnancy is a risk factor for preeclampsia in singleton and twin pregnancies. Am. J. Obstet. Gynecol. 2015, 213, 395.e1–395.e8. [Google Scholar] [CrossRef]
- Society for Maternal-Fetal Medicine (SMFM); Lee, R.H.; Mara Greenberg Metz, T.D.; Pettker, C.M. Society for Maternal-Fetal Medicine Consult Series #53: Intrahepatic cholestasis of pregnancy: Replaces Consult #13, April 2011. Am. J. Obs. Gynecol. 2021, 224, B2–B9. [Google Scholar]
- Girling, J.; Knight, C.L.; Chappell, L.; Royal College of Obstetricians and Gynaecologists. Intrahepatic cholestasis of pregnancy: Green-top Guideline No. 43 June 2022. BJOG 2022, 129, e95–e114. [Google Scholar] [CrossRef]
- Dollberg, S.; Haklai, Z.; Mimouni, F.B.; Gorfein, I.; Gordon, E.-S. Birth weight standards in the live-born population in Israel. Isr. Med. Assoc. J. 2005, 7, 311–314. [Google Scholar]
- St-Pierre, M.V.; Serrano, M.A.; Macias, R.I.; Dubs, U.; Hoechli, M.; Lauper, U.; Meier, P.J.; Marin, J.J.G. Expression of members of the multidrug resistance protein family in human term placenta. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R1495–R1503. [Google Scholar] [CrossRef]
- Marin, J.J.; Bravo, P.; el-Mir, M.Y.; Serrano, M.A. ATP-dependent bile acid transport across microvillous membrane of human term trophoblast. Am. J. Physiol. 1995, 268, G685–G694. [Google Scholar] [CrossRef]
- Fan, H.M.; Mitchell, A.L.; Williamson, C. Endocrinology in Pregnancy: Metabolic impact of bile acids in gestation. Eur. J. Endocrinol. 2021, 184, R69–R83. [Google Scholar] [CrossRef]
- Bacq, Y.; le Besco, M.; Lecuyer, A.-I.; Gendrot, C.; Potin, J.; Andres, C.R.; Aubourg, A. Ursodeoxycholic acid therapy in intrahepatic cholestasis of pregnancy: Results in real-world conditions and factors predictive of response to treatment. Dig. Liver Dis. 2017, 49, 63–69. [Google Scholar] [CrossRef]
- Serrano, M.A.; Macias, R.I.R.; Vallejo, M.; Briz, O.; Bravo, A.; Pascual, M.J.; St-Pierre, M.V.; Stieger, B.; Meier, P.J.; Marin, J.J.G. Effect of ursodeoxycholic acid on the impairment induced by maternal cholestasis in the rat placenta-maternal liver tandem excretory pathway. J. Pharm. Exp. Ther. 2003, 305, 515–524. [Google Scholar] [CrossRef]
- Brites, D. Intrahepatic cholestasis of pregnancy: Changes in maternal-fetal bile acid balance and improvement by ursodeoxycholic acid. Ann. Hepatol. 2002, 1, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhu, L.; Xu, D.; Gao, L.; Li, Y.; Liang, B.; Zhang, X.; Yue, Y. Intrahepatic Cholestasis of Pregnancy Is Associated with Reduced Nitric Oxide Synthase (iNOS) in Plasma and Placentas: A Pilot Study. Med. Sci. Monit. 2021, 27, e930176. [Google Scholar] [CrossRef] [PubMed]
- Manzotti, C.; Casazza, G.; Stimac, T.; Nikolova, D.; Gluud, C. Total serum bile acids or serum bile acid profile, or both, for the diagnosis of intrahepatic cholestasis of pregnancy. Cochrane Database Syst. Rev. 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age (years) at Time of Delivery a | 5.2 ± 36.5 |
| Parity a | 0.9 ± 1 |
| Pregestational BMI a | 3 ± 23 |
| Multiple gestation b | (27) 18/5 |
| ICP in previous pregnancy b | (44) 18/8 |
| IUFD in previous pregnancy due to ICP b | (5.5) 18/1 |
| Gestational diabetes b | 6/18 (33) |
| Gestational age at diagnosis (wks.) a | 5 ± 32 |
| TBA at diagnosis a (µmol/L) (range) | (94−12) 3 ± 33.4 |
| Gestational age at UDCA administration | 33 ± 5.7 |
| Length of treatment (days) a | 29 ± 44 (2−133) |
| Maximal TBA a (µmol/L) (range) | 99.6 ± 46 (51−247) |
| Second line therapy | 6/18(33) |
| Maternal TBA at delivery a (µmol/L) (range) | 76.4 ± 30.3 (40−129) |
| Maternal TBA at delivery >90 µmol/L. b | 4/18(22) |
| Gestational age at delivery (wks.) a | 35.6 ± 1.6 |
| Delivery < 37 wks. b | 16/18 (88) |
| Delivery < 34 wks. b | 3/18 (17) |
| Spontaneous delivery b | 1/18 (5.5) |
| Cesarean section b | 5/18 (27) |
| Umbilical Vein TBA a (µmol/L), (range) | 22.5 ± 8.8.(12−42) |
| Umbilical artery TBA a (µmol/L), (range) | 19.6 ± 6.5 (11−30) |
| Birthweight singleton (gr) a | 2614 ± 380 |
| Birthweight percentile singleton a | 51 ± 22 |
| Birthweight twins (gr) a | 2440 ± 466 |
| Birthweight percentile twins a | 57 ± 26 |
| SGA b | 0/23 |
| Umbilical cord pH <7.1 b | 0/23 |
| MSAF | 7/23 (30) |
| Fetal asphyxia b | 0/23 |
| NICU admission b | 6/23 (26) |
| NICU hospitalization (days) a, (range) | 24 ± 11 (3−36) |
| RDS b (gestational age at delivery, wks.) | 3/23 (13) (32−33) |
| Jaundice b | 5/23 (21) |
| Perinatal death b | 0/23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hershkovitz, G.; Raz, Y.; Goldinger, I.; Many, A.; Hiersch, L.; Eli, R. Severe Intrahepatic Cholestasis of Pregnancy—Potential Mechanism by Which Fetuses Are Protected from the Hazardous Effect of Bile Acids. J. Clin. Med. 2023, 12, 616. https://doi.org/10.3390/jcm12020616
Hershkovitz G, Raz Y, Goldinger I, Many A, Hiersch L, Eli R. Severe Intrahepatic Cholestasis of Pregnancy—Potential Mechanism by Which Fetuses Are Protected from the Hazardous Effect of Bile Acids. Journal of Clinical Medicine. 2023; 12(2):616. https://doi.org/10.3390/jcm12020616
Chicago/Turabian StyleHershkovitz, Gal, Yael Raz, Ilana Goldinger, Ariel Many, Liran Hiersch, and Rimon Eli. 2023. "Severe Intrahepatic Cholestasis of Pregnancy—Potential Mechanism by Which Fetuses Are Protected from the Hazardous Effect of Bile Acids" Journal of Clinical Medicine 12, no. 2: 616. https://doi.org/10.3390/jcm12020616
APA StyleHershkovitz, G., Raz, Y., Goldinger, I., Many, A., Hiersch, L., & Eli, R. (2023). Severe Intrahepatic Cholestasis of Pregnancy—Potential Mechanism by Which Fetuses Are Protected from the Hazardous Effect of Bile Acids. Journal of Clinical Medicine, 12(2), 616. https://doi.org/10.3390/jcm12020616