
Increased General, Eating, and Body-Related Psychopathology in Inpatients in a Specialized Eating Disorders Unit after the Beginning of the COVID-19 Pandemic: A Retrospective Comparison with the Pre-Pandemic Period


Abstract
1. Introduction
Aims
2. Materials and Methods
2.1. Procedure
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Clinical and Psychopathological Measures at Admission and Discharge
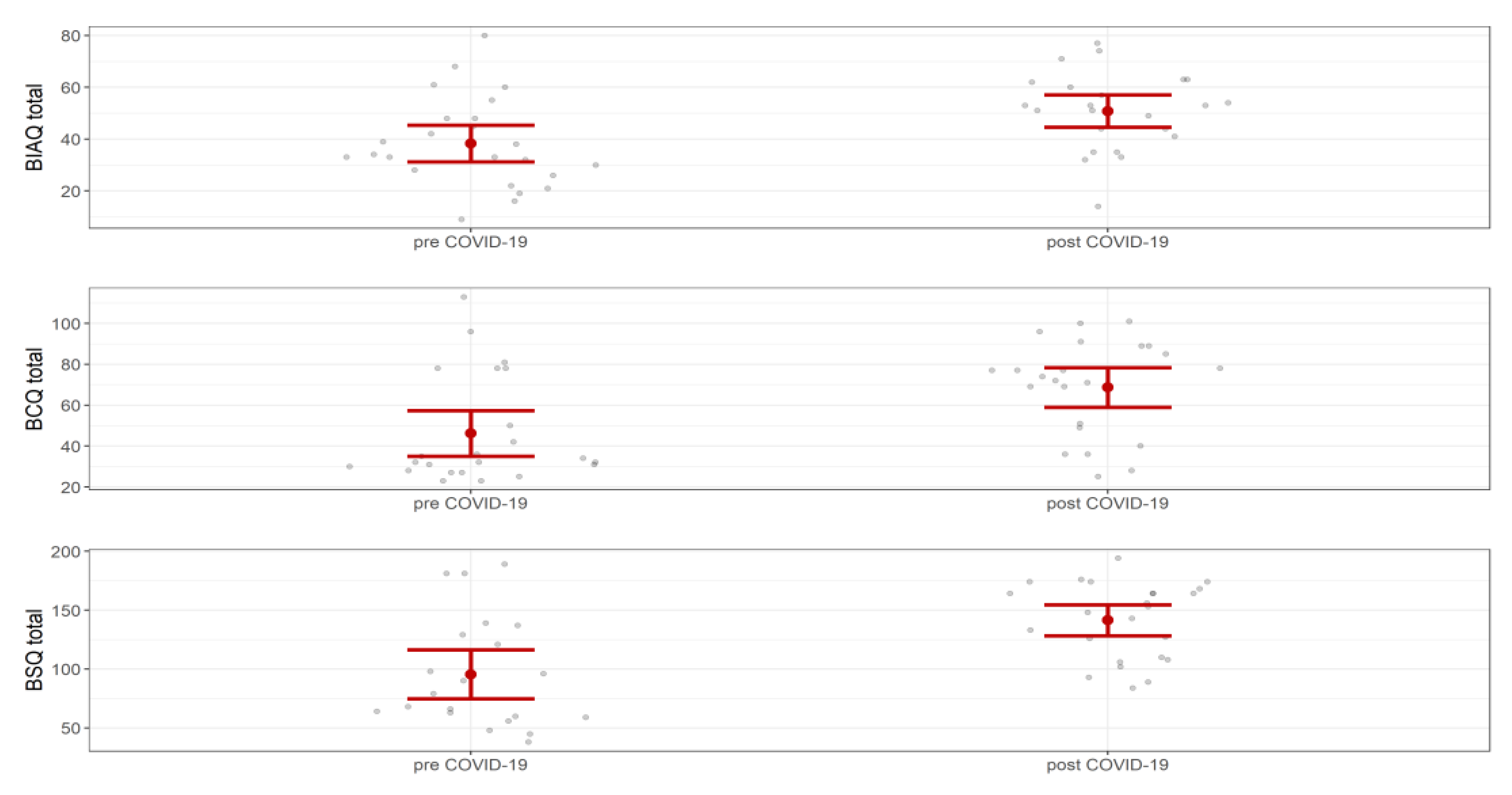
3.2. Body Checking, Avoidance, and Shape Concerns
3.3. Lockdown and Re-Opening Comparison
3.4. Extreme-AN
3.5. Logistic Regression
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary Research Priorities for the COVID-19 Pandemic: A Call for Action for Mental Health Science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Neelam, K.; Duddu, V.; Anyim, N.; Neelam, J.; Lewis, S. Pandemics and Pre-Existing Mental Illness: A Systematic Review and Meta-Analysis. Brain Behav. Immun. Health 2021, 10, 100177. [Google Scholar] [CrossRef] [PubMed]
- Baenas, I.; Etxandi, M.; Munguía, L.; Granero, R.; Mestre-Bach, G.; Sánchez, I.; Ortega, E.; Andreu, A.; Moize, V.L.; Fernández-Real, J.-M.; et al. Impact of COVID-19 Lockdown in Eating Disorders: A Multicentre Collaborative International Study. Nutrients 2021, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Favreau, M.; Hillert, A.; Osen, B.; Gärtner, T.; Hunatschek, S.; Riese, M.; Hewera, K.; Voderholzer, U. Psychological Consequences and Differential Impact of the COVID-19 Pandemic in Patients with Mental Disorders. Psychiatry Res. 2021, 302, 114045. [Google Scholar] [CrossRef] [PubMed]
- Baenas, I.; Caravaca-Sanz, E.; Granero, R.; Sánchez, I.; Riesco, N.; Testa, G.; Vintró-Alcaraz, C.; Treasure, J.; Jiménez-Murcia, S.; Fernández-Aranda, F. COVID-19 and Eating Disorders during Confinement: Analysis of Factors Associated with Resilience and Aggravation of Symptoms. Eur. Eat. Disord. Rev. 2020, 28, 855–863. [Google Scholar] [CrossRef]
- Branley-Bell, D.; Talbot, C.V. Exploring the Impact of the COVID-19 Pandemic and UK Lockdown on Individuals with Experience of Eating Disorders. J. Eat. Disord. 2020, 8, 44. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Munguía, L.; Mestre-Bach, G.; Steward, T.; Etxandi, M.; Baenas, I.; Granero, R.; Sánchez, I.; Ortega, E.; Andreu, A.; et al. COVID Isolation Eating Scale (CIES): Analysis of the Impact of Confinement in Eating Disorders and Obesity—A Collaborative International Study. Eur. Eat. Disord. Rev. 2020, 28, 871–883. [Google Scholar] [CrossRef]
- Giel, K.E.; Schurr, M.; Zipfel, S.; Junne, F.; Schag, K. Eating Behaviour and Symptom Trajectories in Patients with a History of Binge Eating Disorder during COVID-19 Pandemic. Eur. Eat. Disord. Rev. 2021, 29, 657–662. [Google Scholar] [CrossRef]
- Monteleone, A.M.; Cascino, G.; Marciello, F.; Abbate-Daga, G.; Baiano, M.; Balestrieri, M.; Barone, E.; Bertelli, S.; Carpiniello, B.; Castellini, G.; et al. Risk and Resilience Factors for Specific and General Psychopathology Worsening in People with Eating Disorders during COVID-19 Pandemic: A Retrospective Italian Multicentre Study. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 2443–2452. [Google Scholar] [CrossRef]
- Schlegl, S.; Maier, J.; Meule, A.; Voderholzer, U. Eating Disorders in Times of the COVID-19 Pandemic—Results from an Online Survey of Patients with Anorexia Nervosa. Int. J. Eat. Disord. 2020, 53, 1791–1800. [Google Scholar] [CrossRef]
- Termorshuizen, J.D.; Watson, H.J.; Thornton, L.M.; Borg, S.; Flatt, R.E.; MacDermod, C.M.; Harper, L.E.; van Furth, E.F.; Peat, C.M.; Bulik, C.M. Early Impact of COVID-19 on Individuals with Self-Reported Eating Disorders: A Survey of ~1000 Individuals in the United States and the Netherlands. Int. J. Eat. Disord. 2020, 53, 1780–1790. [Google Scholar] [CrossRef]
- Carmassi, C.; Tosato, S.; Bertelloni, C.A.; Pedrinelli, V.; Cappelli, A.; Abbate-Daga, G.; Albert, U.; Castellini, G.; Luciano, M.; Menchetti, M.; et al. PTSD Trajectories across Different Mental Disorders in the Second Year of the COVID-19 Pandemic in Italy: A Naturalistic, Longitudinal, Multicenter Study. Int. Rev. Psychiatry 2022, 1–12. [Google Scholar] [CrossRef]
- Castellini, G.; Cassioli, E.; Rossi, E.; Innocenti, M.; Gironi, V.; Sanfilippo, G.; Felciai, F.; Monteleone, A.M.; Ricca, V. The Impact of COVID-19 Epidemic on Eating Disorders: A Longitudinal Observation of Pre Versus Post Psychopathological Features in a Sample of Patients with Eating Disorders and a Group of Healthy Controls. Int. J. Eat. Disord. 2020, 53, 1855–1862. [Google Scholar] [CrossRef]
- Monteleone, A.M.; Marciello, F.; Cascino, G.; Abbate-Daga, G.; Anselmetti, S.; Baiano, M.; Balestrieri, M.; Barone, E.; Bertelli, S.; Carpiniello, B.; et al. The Impact of COVID-19 Lockdown and of the Following “Re-Opening” Period on Specific and General Psychopathology in People with Eating Disorders: The Emergent Role of Internalizing Symptoms. J. Affect. Disord. 2021, 285, 77–83. [Google Scholar] [CrossRef]
- Marzola, E.; Porliod, A.; Panero, M.; De-Bacco, C.; Abbate-Daga, G. Affective Temperaments and Eating Psychopathology in Anorexia Nervosa: Which Role for Anxious and Depressive Traits? J. Affect. Disord. 2020, 266, 374–380. [Google Scholar] [CrossRef]
- Sideli, L.; Lo Coco, G.; Bonfanti, R.C.; Borsarini, B.; Fortunato, L.; Sechi, C.; Micali, N. Effects of COVID-19 Lockdown on Eating Disorders and Obesity: A Systematic Review and Meta-Analysis. Eur. Eat. Disord. Rev. 2021, 29, 826–841. [Google Scholar] [CrossRef]
- Carr, A.; Toloza, C.; Li, Z.; Nazar, B.P.; Himmerich, H. Therapy Outcome of Day Treatment for People with Anorexia Nervosa before and during the COVID-19 Pandemic. Brain Behav. 2022, 12, e2604. [Google Scholar] [CrossRef]
- Haripersad, Y.V.; Kannegiesser-Bailey, M.; Morton, K.; Skeldon, S.; Shipton, N.; Edwards, K.; Newton, R.; Newell, A.; Stevenson, P.G.; Martin, A.C. Outbreak of Anorexia Nervosa Admissions during the COVID-19 Pandemic. Arch. Dis. Child. 2021, 106, e15. [Google Scholar] [CrossRef]
- Spettigue, W.; Obeid, N.; Erbach, M.; Feder, S.; Finner, N.; Harrison, M.E.; Isserlin, L.; Robinson, A.; Norris, M.L. The Impact of COVID-19 on Adolescents with Eating Disorders: A Cohort Study. J. Eat. Disord. 2021, 9, 65. [Google Scholar] [CrossRef]
- Agostino, H.; Burstein, B.; Moubayed, D.; Taddeo, D.; Grady, R.; Vyver, E.; Dimitropoulos, G.; Dominic, A.; Coelho, J.S. Trends in the Incidence of New-Onset Anorexia Nervosa and Atypical Anorexia Nervosa Among Youth during the COVID-19 Pandemic in Canada. JAMA Netw. Open 2021, 4, e2137395. [Google Scholar] [CrossRef]
- Devoe, D.J.; Han, A.; Anderson, A.; Katzman, D.K.; Patten, S.B.; Soumbasis, A.; Flanagan, J.; Paslakis, G.; Vyver, E.; Marcoux, G.; et al. The Impact of the COVID-19 Pandemic on Eating Disorders: A Systematic Review. Int. J. Eat. Disord. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ayton, A.; Viljoen, D.; Ryan, S.; Ibrahim, A.; Ford, D. Risk, Demand, Capacity and Outcomes in Adult Specialist Eating Disorder Services in South-East of England before and Since COVID-19. BJPsych Bull. 2022, 46, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.; Ziv, A.; Vardi, Y.; Hadas, S.; Zuabi, T.; Yeshareem, L.; Gur, T.; Steinling, S.; Scheuerman, O.; Levinsky, Y. The Effect of COVID-19 Pandemic on Hospitalizations and Disease Characteristics of Adolescents with Anorexia Nervosa. Eur. J. Pediatr. 2022, 181, 1767–1771. [Google Scholar] [CrossRef] [PubMed]
- Graell, M.; Morón-Nozaleda, M.G.; Camarneiro, R.; Villaseñor, Á.; Yáñez, S.; Muñoz, R.; Martínez-Núñez, B.; Miguélez-Fernández, C.; Muñoz, M.; Faya, M. Children and Adolescents with Eating Disorders during COVID-19 Confinement: Difficulties and Future Challenges. Eur. Eat. Disord. Rev. 2020, 28, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Schreyer, C.C.; Vanzhula, I.A.; Guarda, A.S. Evaluating the Impact of COVID-19 on Severity at Admission and Response to Inpatient Treatment for Adult and Adolescent Patients with Eating Disorders. Int. J. Eat. Disord. 2022. [Google Scholar] [CrossRef]
- Marzola, E.; Panero, M.; Cavallo, F.; Delsedime, N.; Abbate-Daga, G. Body Shape in Inpatients with Severe Anorexia Nervosa. Eur. Psychiatry 2020, 63, e2. [Google Scholar] [CrossRef]
- Marzola, E.; Martini, M.; Brustolin, A.; Abbate-Daga, G. Inpatients with Severe-Enduring Anorexia Nervosa: Understanding the “Enduringness” Specifier. Eur. Psychiatry 2021, 64, e44. [Google Scholar] [CrossRef]
- Toppino, F.; Longo, P.; Martini, M.; Abbate-Daga, G.; Marzola, E. Body Mass Index Specifiers in Anorexia Nervosa: Anything Below the “Extreme”? J. Clin. Med. 2022, 11, 542. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.; Karg, R.S.; Spitzer, R.L. User’s Guide for the SCID-5-CV Structured Clinical Interview for DSM-5 Disorders: Clinical Version; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2016. [Google Scholar]
- Davidson, J.R.; Miner, C.M.; De Veaugh-Geiss, J.; Tupler, L.A.; Colket, J.T.; Potts, N.L.S. The Brief Social Phobia Scale: A Psychometric Evaluation. Psychol. Med. 1997, 27, 161–166. [Google Scholar] [CrossRef]
- Calugi, S.; Milanese, C.; Sartirana, M.; El Ghoch, M.; Sartori, F.; Geccherle, E.; Coppini, A.; Franchini, C.; Dalle Grave, R. The Eating Disorder Examination Questionnaire: Reliability and Validity of the Italian Version. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2017, 22, 509–514. [Google Scholar] [CrossRef]
- Lazzari, R.; Pancheri, P. Questionario di Valutazione Dell’ansia di Stato e di Tratto [State-Trait Anxiety Inventory]; Organizzazioni Speciali: Firenze, Italy, 1980. [Google Scholar]
- Baggio, A.; Ferrari, R.; Partinico, M.; Vidotto, G.; Visentin, M. Il Beck Depression Inventory Per La Valutazione Della Depressione Nel Dolore Cronico. Il Contributo Degli “Item” Somatici. Int. J. Pain. Ther. 1997, 7, 4–11. [Google Scholar]
- Riva, G.; Molinari, E. Replicated Factor Analysis of the Italian Version of the Body Image Avoidance Questionnaire. Percept. Mot. Ski. 1998, 86, 1071–1074. [Google Scholar] [CrossRef]
- Calugi, S.; Dalle Grave, R.; Ghisi, M.; Sanavio, E. Validation of the Body Checking Questionnaire (BCQ) in an Eating Disorders Population. Behav. Cogn. Psychother. 2006, 34, 233–242. [Google Scholar] [CrossRef]
- Marzola, E.; Martini, M.; Longo, P.; Toppino, F.; Bevione, F.; Delsedime, N.; Abbate-Daga, G.; Preti, A. Psychometric Properties of the Italian Body Shape Questionnaire: An Investigation of Its Reliability, Factorial, Concurrent, and Criterion Validity. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2022, 27, 3637–3648. [Google Scholar] [CrossRef]
- Tjur, T. Coefficients of Determination in Logistic Regression Models—A New Proposal: The Coefficient of Discrimination. Am. Stat. 2009, 63, 366–372. [Google Scholar] [CrossRef]
- Martini, M.; Marzola, E.; Musso, M.; Brustolin, A.; Abbate-Daga, G. Association of Emotion Recognition Ability and Interpersonal Emotional Competence in Anorexia Nervosa: A Study with a Multimodal Dynamic Task. Int. J. Eat. Disord. 2022. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Admission | Discharge | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Pre-COVID, N = 80 1 | Post-COVID, N = 79 1 | p-Value 2 | q-Value 3 | ES (95% CI) 4 | Pre-COVID, N = 80 1 | Post-COVID, N = 79 1 | p-Value 5 | q-Value 3 | ES (95% CI) 4 |
| Age, years | 24.88 (8.48) | 24.73 (7.80) | >0.9 | >0.9 | −0.02 (−0.34, 0.30) | |||||
| Sex: female | 78 (98%) | 78 (99%) | >0.9 | >0.9 | ||||||
| Diagnosis | 0.4 | >0.9 | ||||||||
| AN-BP | 14 (18%) | 21 (27%) | ||||||||
| AN-R | 47 (59%) | 45 (57%) | ||||||||
| ARFID | 3 (3.8%) | 2 (2.5%) | ||||||||
| BN | 6 (7.5%) | 7 (8.9%) | ||||||||
| OSFED | 10 (12%) | 4 (5.1%) | ||||||||
| Duration of Illness, years | 6.43 (6.92) | 7.30 (7.62) | 0.5 | >0.9 | 0.12 (−0.21, 0.44) | |||||
| Length of stay, days | 34.55 (19.54) | 29.08 (18.35) | 0.088 | 0.7 | −0.29 (−0.62, 0.05) | |||||
| Admission from emergency room | 13 (16%) | 22 (28%) | 0.078 | 0.7 | ||||||
| BMI (underweight individuals) | 14.39 (2.21) | 14.30 (1.93) | 0.8 | >0.9 | −0.04 (−0.39, 0.30) | 15.08 (2.13) | 14.75 (1.82) | 0.4 | >0.9 | −0.17 (−0.53, 0.20) |
| Caloric intake (underweight), kcal | 769.64 (499.88) | 786.32 (371.96) | 0.8 | >0.9 | 0.04 (−0.33, 0.41) | 1457.46 (378.48) | 1376.51 (247.12) | 0.2 | >0.9 | −0.25 (−0.62, 0.12) |
| Physical hyperactivity | 24 (30%) | 41 (52%) | 0.005 | 0.050 | 8 (10%) | 17 (22%) | 0.046 | 0.4 | ||
| Binge-purging symptoms | 18 (22%) | 25 (32%) | 0.2 | >0.9 | 2 (2.5%) | 2 (2.5%) | >0.9 | >0.9 | ||
| BSPS fear | 9.68 (5.05) | 9.61 (6.74) | >0.9 | >0.9 | −0.01 (−0.34, 0.32) | 7.79 (5.01) | 8.18 (6.21) | 0.7 | >0.9 | 0.07 (−0.27, 0.41) |
| BSPS avoidance | 8.95 (5.23) | 9.03 (6.54) | >0.9 | >0.9 | 0.01 (−0.31, 0.34) | 7.23 (4.83) | 7.85 (6.22) | 0.5 | >0.9 | 0.11 (−0.23, 0.46) |
| BSPS physiologic | 3.73 (2.70) | 5.53 (5.58) | 0.016 | 0.073 | 0.41 (0.08, 0.74) | 3.06 (2.91) | 4.21 (3.62) | 0.048 | 0.4 | 0.35 (0.01, 0.70) |
| BSPS total score | 22.41 (12.04) | 23.49 (16.50) | 0.7 | >0.9 | 0.07 (−0.25, 0.40) | 17.99 (11.25) | 20.21 (14.62) | 0.3 | >0.9 | 0.17 (−0.17, 0.52) |
| EDE-Q restraint | 3.14 (2.07) | 4.01 (1.86) | 0.007 | 0.046 | 0.44 (0.12, 0.76) | 1.75 (1.67) | 2.65 (1.57) | 0.008 | 0.015 | 0.56 (0.14, 1.0) |
| Unknown | 29 | 35 | ||||||||
| EDE-Q eating concern | 3.01 (1.58) | 3.64 (1.35) | 0.009 | 0.054 | 0.42 (0.10, 0.74) | 2.05 (1.39) | 2.73 (1.17) | 0.011 | 0.015 | 0.52 (0.11, 0.93) |
| Unknown | 29 | 35 | ||||||||
| EDE-Q shape concern | 3.98 (1.58) | 4.98 (1.37) | <0.001 | <0.001 | 0.67 (0.35, 1.0) | 3.01 (1.93) | 4.60 (1.40) | <0.001 | <0.001 | 0.92 (0.49, 1.3) |
| Unknown | 29 | 35 | ||||||||
| EDE-Q weight concern | 3.50 (1.69) | 4.49 (1.61) | <0.001 | 0.003 | 0.60 (0.27, 0.92) | 2.46 (1.71) | 3.94 (1.58) | <0.001 | <0.001 | 0.89 (0.46, 1.3) |
| Unknown | 29 | 35 | ||||||||
| EDE-Q global score | 3.41 (1.61) | 4.28 (1.38) | <0.001 | 0.004 | 0.58 (0.26, 0.90) | 2.32 (1.52) | 3.48 (1.26) | <0.001 | <0.001 | 0.82 (0.40, 1.2) |
| Unknown | 29 | 35 | ||||||||
| STAI state anxiety | 54.32 (13.05) | 60.34 (11.73) | 0.004 | 0.035 | 0.48 (0.15, 0.82) | |||||
| STAI trait anxiety | 56.90 (15.92) | 64.12 (10.01) | 0.001 | 0.013 | 0.54 (0.21, 0.87) | |||||
| BDI total score | 15.97 (8.73) | 19.64 (7.53) | 0.015 | 0.073 | 0.44 (0.08, 0.81) | |||||
| Characteristic | Pre-COVID, N = 53 1 | Post-COVID, N = 46 1 | p-Value 2 | q-Value 3 | ES (95% CI) 4 |
|---|---|---|---|---|---|
| BCQ specific body parts | 20.52 (10.67) | 28.89 (10.83) | <0.001 | 0.002 | 0.77 (0.36, 1.2) |
| BCQ idiosyncratic checking | 9.15 (5.63) | 14.83 (6.50) | <0.001 | <0.001 | 0.93 (0.51, 1.3) |
| BCQ total score | 56.00 (25.62) | 75.76 (25.53) | <0.001 | 0.002 | 0.77 (0.35, 1.2) |
| BIAQ clothing | 19.13 (9.20) | 23.65 (9.43) | 0.018 | 0.041 | 0.48 (0.08, 0.88) |
| BIAQ social activities | 7.58 (5.96) | 10.83 (5.43) | 0.006 | 0.028 | 0.56 (0.16, 1.0) |
| BIAQ eating-related control behavior | 5.98 (4.85) | 8.33 (4.43) | 0.014 | 0.041 | 0.50 (0.10, 0.90) |
| BIAQ grooming/weighing | 8.72 (3.66) | 8.76 (3.40) | >0.9 | >0.9 | 0.01 (−0.38, 0.41) |
| BIAQ total score | 41.42 (18.04) | 51.57 (17.47) | 0.006 | 0.028 | 0.57 (0.16, 1.0) |
| BSQ | 114.04 (47.11) | 149.35 (40.08) | <0.001 | 0.001 | 0.80 (0.38, 1.2) |
| Characteristic | OR 1 | 95% CI 1 | p-Value |
|---|---|---|---|
| Physical hyperactivity | 1.95 | 0.92, 4.19 | 0.085 |
| EDE-Q restraint | 0.76 | 0.56, 1.03 | 0.084 |
| EDE-Q shape concern | 1.86 | 1.22, 2.94 | 0.006 |
| STAI state anxiety | 1.00 | 0.96, 1.04 | >0.9 |
| STAI trait anxiety | 1.03 | 0.99, 1.07 | 0.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, M.; Longo, P.; Delsedime, N.; Abbate-Daga, G.; Panero, M. Increased General, Eating, and Body-Related Psychopathology in Inpatients in a Specialized Eating Disorders Unit after the Beginning of the COVID-19 Pandemic: A Retrospective Comparison with the Pre-Pandemic Period. J. Clin. Med. 2023, 12, 573. https://doi.org/10.3390/jcm12020573
Martini M, Longo P, Delsedime N, Abbate-Daga G, Panero M. Increased General, Eating, and Body-Related Psychopathology in Inpatients in a Specialized Eating Disorders Unit after the Beginning of the COVID-19 Pandemic: A Retrospective Comparison with the Pre-Pandemic Period. Journal of Clinical Medicine. 2023; 12(2):573. https://doi.org/10.3390/jcm12020573
Chicago/Turabian StyleMartini, Matteo, Paola Longo, Nadia Delsedime, Giovanni Abbate-Daga, and Matteo Panero. 2023. "Increased General, Eating, and Body-Related Psychopathology in Inpatients in a Specialized Eating Disorders Unit after the Beginning of the COVID-19 Pandemic: A Retrospective Comparison with the Pre-Pandemic Period" Journal of Clinical Medicine 12, no. 2: 573. https://doi.org/10.3390/jcm12020573
APA StyleMartini, M., Longo, P., Delsedime, N., Abbate-Daga, G., & Panero, M. (2023). Increased General, Eating, and Body-Related Psychopathology in Inpatients in a Specialized Eating Disorders Unit after the Beginning of the COVID-19 Pandemic: A Retrospective Comparison with the Pre-Pandemic Period. Journal of Clinical Medicine, 12(2), 573. https://doi.org/10.3390/jcm12020573