
Sex Differences in Falls: The Mediating Role of Gait Stability Ratio and Body Balance in Vulnerable Older Adults

 ,
,  ,
, 
 ,
,  , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Design and Participants
2.2. Data Collection
2.2.1. Demographic and Health Characteristics
2.2.2. Falls
2.2.3. Anthropometry
2.2.4. Gait Parameters
2.2.5. Balance
2.2.6. Covariates
2.2.7. Statistics
3. Results
3.1. Main Characteristics of Participants
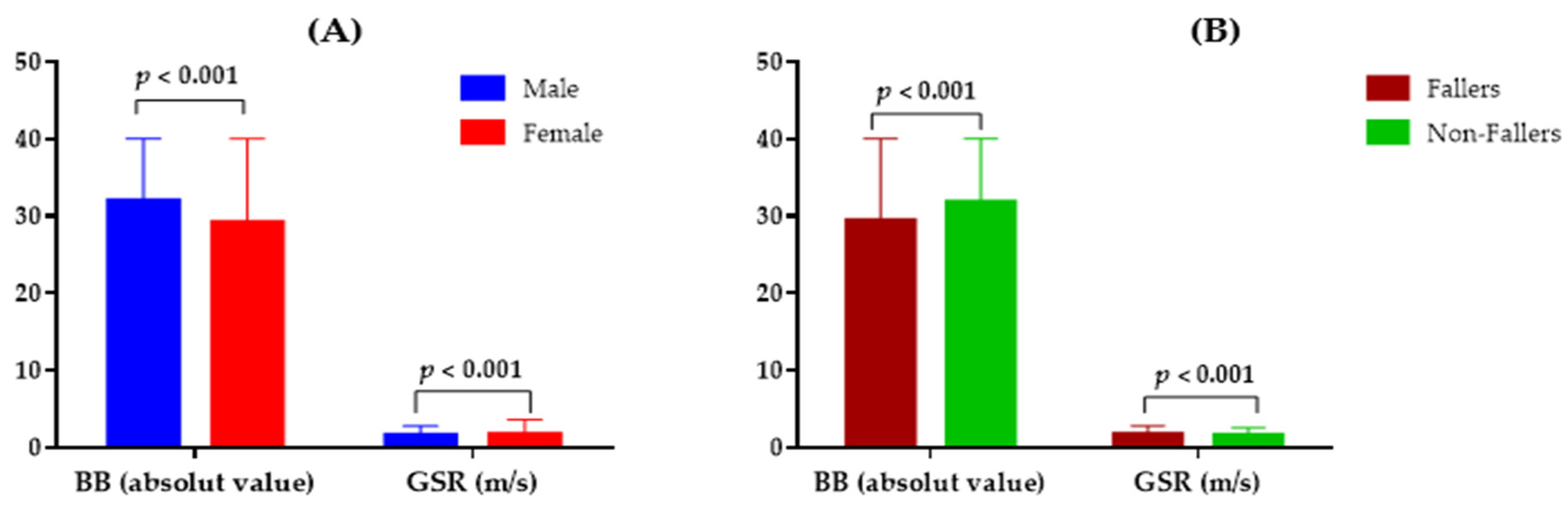
3.2. GSR and BB Performance According to Sex and History of Falls
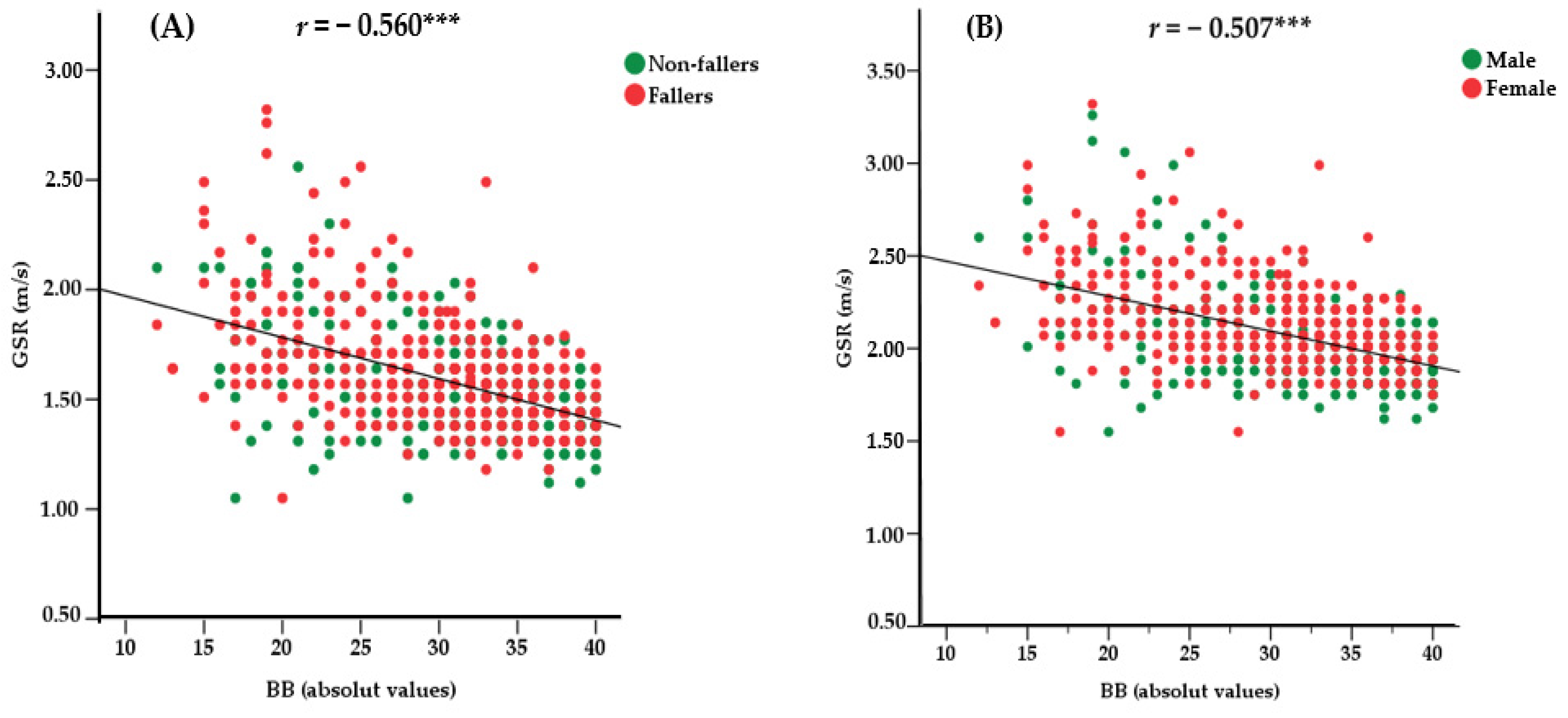
3.3. Results of the Correlation Coefficients between GSR and BB According to the History of Falls and Sex
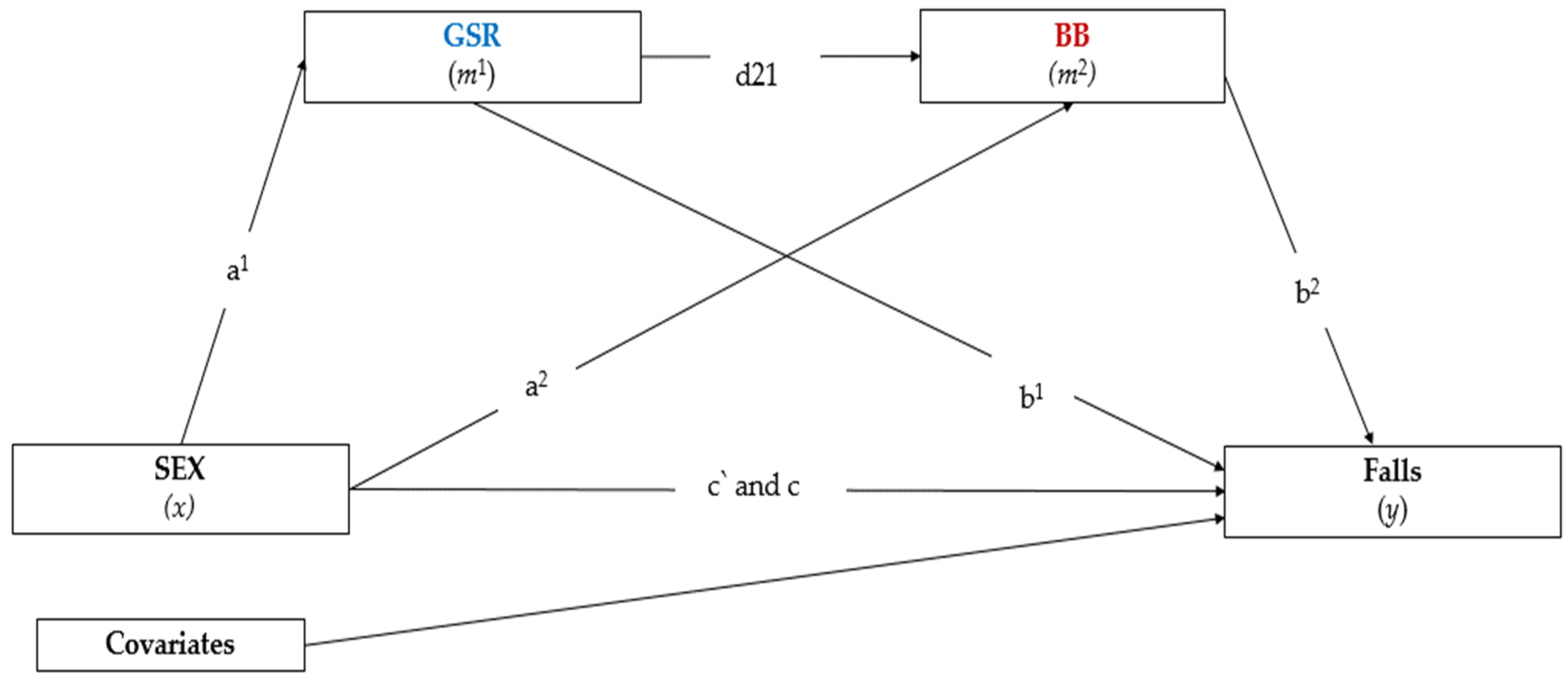
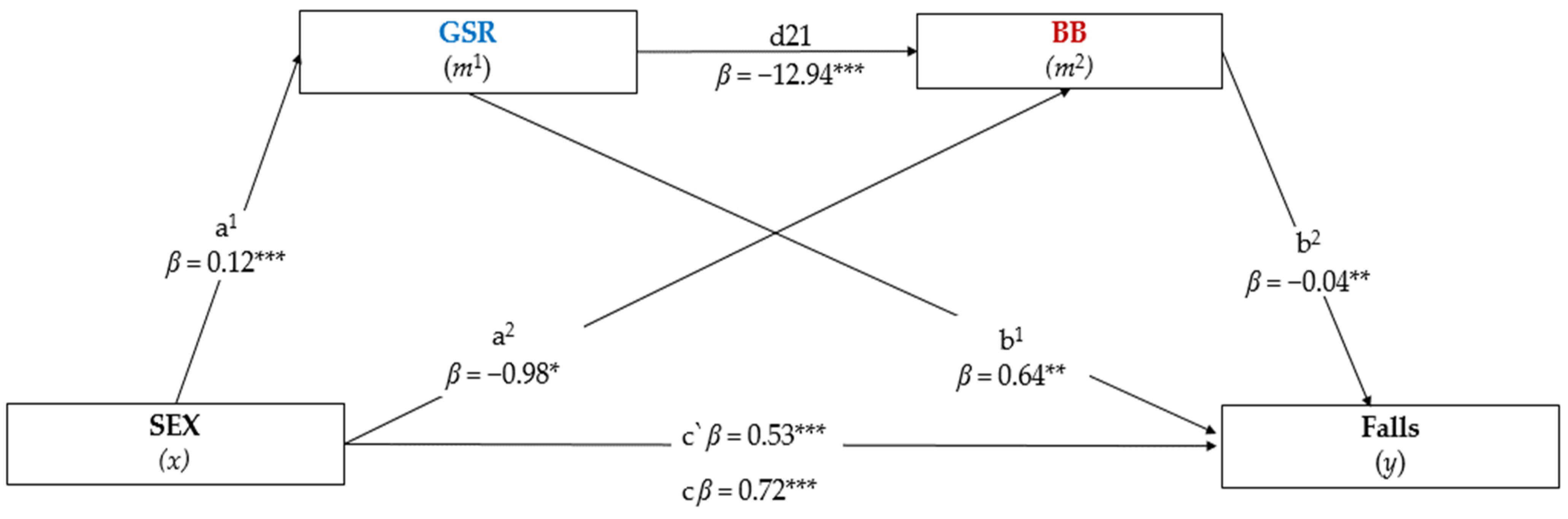
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yoshida, S. A Global Report on Falls Prevention: Epidemiology of Falls; WHO: Geneva, Switzerland, 2007; Volume 1. [Google Scholar]
- Guirguis-Blake, J.M.; Michael, Y.L.; Perdue, L.A.; Coppola, E.L.; Beil, T.L. Interventions to Prevent Falls in Older Adults. JAMA 2018, 319, 1705. [Google Scholar] [CrossRef] [PubMed]
- Terroso, M.; Rosa, N.; Torres Marques, A.; Simoes, R. Physical consequences of falls in the elderly: A literature review from 1995 to 2010. Eur. Rev. Aging Phys. Act. 2014, 11, 51–59. [Google Scholar] [CrossRef]
- Khow, K.S.; Visvanathan, R. Falls in the Aging Population. Clin. Geriatr. Med. 2017, 33, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Cooper, C.; Aihie Sayer, A. Prevalence and risk factors for falls in older men and women: The English Longitudinal Study of Ageing. Age Ageing 2016, 45, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Berková, M.; Berka, Z. Falls: A significant cause of morbidity and mortality in elderly people. Vnitr. Lek. 2018, 64, 1076–1083. [Google Scholar] [CrossRef]
- Burns, E.; Kakara, R. Deaths from Falls Among Persons Aged ≥65 Years—United States, 2007–2016. Morb. Mortal. Wkly. Rep. 2018, 67, 509–514. [Google Scholar] [CrossRef]
- Verma, S.K.; Willetts, J.L.; Corns, H.L.; Marucci-Wellman, H.R.; Lombardi, D.A.; Courtney, T.K. Falls and Fall-Related Injuries among Community-Dwelling Adults in the United States. PLoS ONE 2016, 11, e0150939. [Google Scholar] [CrossRef]
- Ganz, D.A.; Latham, N.K. Prevention of Falls in Community-Dwelling Older Adults. N. Engl. J. Med. 2020, 382, 734–743. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Falls Prevention in Older Age; WHO: Geneva, Switzerland, 2007.
- Bohl, A.A.; Phelan, E.A.; Fishman, P.A.; Harris, J.R. How Are the Costs of Care for Medical Falls Distributed? The Costs of Medical Falls by Component of Cost, Timing, and Injury Severity. Gerontologist 2012, 52, 664–675. [Google Scholar]
- Stevens, J.A.; Corso, P.S.; Finkelstein, E.A.; Miller, T.R. The costs of fatal and non-fatal falls among older adults. Inj. Prev. 2006, 12, 290–295. [Google Scholar] [CrossRef]
- Enderlin, C.; Rooker, J.; Ball, S.; Hippensteel, D.; Alderman, J.; Fisher, S.J.; McLeskey, N.; Jordan, K. Summary of factors contributing to falls in older adults and nursing implications. Geriatr. Nurs. 2015, 36, 397–406. [Google Scholar] [CrossRef]
- Hamacher, D.; Liebl, D.; Hödl, C.; Heßler, V.; Kniewasser, C.K.; Thönnessen, T.; Zech, A. Gait Stability and Its Influencing Factors in Older Adults. Front. Physiol. 2019, 9, 1955. [Google Scholar] [CrossRef]
- Pauelsen, M.; Nyberg, L.; Röijezon, U.; Vikman, I. Both psychological factors and physical performance are associated with fall-related concerns. Aging Clin. Exp. Res. 2018, 30, 1079–1085. [Google Scholar] [CrossRef]
- Sotoudeh, G.R.; Mohammadi, R.; Mosallanezhad, Z.; Viitasara, E.; Soares, J.J.F. The prevalence, circumstances and consequences of unintentional falls among elderly Iranians: A population study. Arch. Gerontol. Geriatr. 2018, 79, 123–130. [Google Scholar] [CrossRef]
- Chang, V.C.; Do, M.T. Risk Factors for Falls Among Seniors: Implications of Gender. Am. J. Epidemiol. 2015, 181, 521–531. [Google Scholar] [CrossRef]
- Cameron, E.J.; Bowles, S.K.; Marshall, E.G.; Andrew, M.K. Falls and long-term care: A report from the care by design observational cohort study. BMC Fam. Pract. 2018, 19, 73. [Google Scholar] [CrossRef]
- De Sousa, J.A.V.; Stremel, A.I.F.; Grden, C.R.B.; Borges, P.K.D.O.; Reche, P.M.; Silva, J.H.D.O. da Risk of falls and associated factors in institutionalized elderly. Rev. Rede Enferm. Nord. 2016, 17, 416. [Google Scholar]
- Bor, A.; Matuz, M.; Csatordai, M.; Szalai, G.; Bálint, A.; Benkő, R.; Soós, G.; Doró, P. Medication use and risk of falls among nursing home residents: A retrospective cohort study. Int. J. Clin. Pharm. 2017, 39, 408–415. [Google Scholar] [CrossRef]
- Patton, S.; Vincenzo, J.; Lefler, L. Gender Differences in Older Adults’ Perceptions of Falls and Fall Prevention. Health Promot. Pract. 2021, 23, 785–792. [Google Scholar] [CrossRef]
- Papalia, G.F.; Papalia, R.; Diaz Balzani, L.A.; Torre, G.; Zampogna, B.; Vasta, S.; Fossati, C.; Alifano, A.M.; Denaro, V. The Effects of Physical Exercise on Balance and Prevention of Falls in Older People: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2595. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Lusardi, M.M.; Fritz, S.; Middleton, A.; Allison, L.; Wingood, M.; Phillips, E.; Criss, M.; Verma, S.; Osborne, J.; Chui, K.K. Determining Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta-analysis Using Posttest Probability. J. Geriatr. Phys. Ther. 2017, 40, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Plotnik, M.; Bove, F.; Berardelli, A. The neurobiology of falls. Neurol. Sci. 2012, 33, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Brach, J.S.; Perera, S.; VanSwearingen, J.M.; Hile, E.S.; Wert, D.M.; Studenski, S.A. Challenging Gait Conditions Predict 1-Year Decline in Gait Speed in Older Adults With Apparently Normal Gait. Phys. Ther. 2011, 91, 1857–1864. [Google Scholar] [CrossRef]
- Verghese, J.; LeValley, A.; Hall, C.B.; Katz, M.J.; Ambrose, A.F.; Lipton, R.B. Epidemiology of Gait Disorders in Community-Residing Older Adults. J. Am. Geriatr. Soc. 2006, 54, 255–261. [Google Scholar] [CrossRef]
- Lord, S.R.; Sturnieks, D.L. The physiology of falling: Assessment and prevention strategies for older people. J. Sci. Med. Sport 2005, 8, 35–42. [Google Scholar] [CrossRef]
- Sturnieks, D.L.; St. George, R.R.; Lord, S. Balance disorders in the elderly. Neurophysiol. Clin. Neurophysiol. 2008, 38, 467–478. [Google Scholar] [CrossRef]
- Melzer, I.; Benjuya, N.; Kaplanski, J. Postural stability in the elderly: A comparison between fallers and non-fallers. Age Ageing 2004, 33, 602–607. [Google Scholar] [CrossRef]
- Crenshaw, J.R.; Bernhardt, K.A.; Achenbach, S.J.; Atkinson, E.J.; Khosla, S.; Kaufman, K.R.; Amin, S. The circumstances, orientations, and impact locations of falls in community-dwelling older women. Arch. Gerontol. Geriatr. 2017, 73, 240–247. [Google Scholar] [CrossRef]
- Nair, K.S. Aging muscle. Am. J. Clin. Nutr. 2005, 81, 953–963. [Google Scholar] [CrossRef]
- Lacroix, A.; Kressig, R.W.; Muehlbauer, T.; Gschwind, Y.J.; Pfenninger, B.; Bruegger, O.; Granacher, U. Effects of a Supervised versus an Unsupervised Combined Balance and Strength Training Program on Balance and Muscle Power in Healthy Older Adults: A Randomized Controlled Trial. Gerontology 2016, 62, 275–288. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Andrews, A.W.; Thomas, M.W. Walking Speed: Reference Values and Correlates for Older Adults. J. Orthop. Sports Phys. Ther. 1996, 24, 86–90. [Google Scholar] [CrossRef]
- Ayoubi, F.; Launay, C.P.; Annweiler, C.; Beauchet, O. Fear of Falling and Gait Variability in Older Adults: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2015, 16, 14–19. [Google Scholar] [CrossRef]
- Cromwell, R.L.; Newton, R.A. Relationship between Balance and Gait Stability in Healthy Older Adults. J. Aging Phys. Act. 2004, 12, 90–100. [Google Scholar] [CrossRef]
- Nascimento, M.D.M.; Gouveia, É.R.; Gouveia, B.R.; Marques, A.; Martins, F.; Przednowek, K.; França, C.; Peralta, M.; Ihle, A. Associations of Gait Speed, Cadence, Gait Stability Ratio, and Body Balance with Falls in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 13926. [Google Scholar] [CrossRef]
- De Maio Nascimento, M.; Gouveia, B.R.; Gouveia, É.R.; Campos, P.; Marques, A.; Ihle, A. Muscle Strength and Balance as Mediators in the Association between Physical Activity and Health-Related Quality of Life in Community-Dwelling Older Adults. J. Clin. Med. 2022, 11, 4857. [Google Scholar] [CrossRef]
- Tseng, J. Sex, Gender, and Why the Differences Matter. AMA J. Ethics 2008, 10, 427–428. [Google Scholar]
- Diamond, M. IV. Sex and Gender: Same or Different? Fem. Psychol. 2000, 10, 46–54. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Lippincott Williams Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Marfell-Jones, M.; Olds, T.; Stew, A.; Carter, L. International standards for anthropometric assessment. In International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2012. [Google Scholar]
- Rose, D.J. Fallproof!: A Comprehensive Balance and Mobility Training Program; Human Kinetics: Champaign, IL, USA, 2010; ISBN 978-0-7360-6747-8. [Google Scholar]
- Mirmoezzi, M.; Namazizadeh, M.; Sadeghi, H.; Mohammadi, F. Effect of Different Cognitive Loads on Gait Stability in Younger and Older Adults. Phys. Treat. Specif. Phys. Ther. J. 2019, 9, 69–76. [Google Scholar] [CrossRef]
- Rogers, H.L.; Cromwell, R.L.; Grady, J.L. Adaptive Changes in Gait of Older and Younger Adults as Responses to Challenges to Dynamic Balance. J. Aging Phys. Act. 2008, 16, 85–96. [Google Scholar] [CrossRef]
- Rose, D.J.; Lucchese, N.; Wiersma, L.D. Development of a Multidimensional Balance Scale for Use with Functionally Independent Older Adults. Arch. Phys. Med. Rehabil. 2006, 87, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, B.R.; Jardim, H.G.; Martins, M.M.; Gouveia, É.R.; de Freitas, D.L.; Maia, J.A.; Rose, D.J. An evaluation of a nurse-led rehabilitation programme (the ProBalance Programme) to improve balance and reduce fall risk of community-dwelling older people: A randomised controlled trial. Int. J. Nurs. Stud. 2016, 56, 1–8. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hernandez, D.; Rose, D.J. Predicting Which Older Adults Will or Will Not Fall Using the Fullerton Advanced Balance Scale. Arch. Phys. Med. Rehabil. 2008, 89, 2309–2315. [Google Scholar] [CrossRef] [PubMed]
- Gamwell, H.E.; Wait, S.O.; Royster, J.T.; Ritch, B.L.; Powell, S.C.; Skinner, J.W. Aging and Gait Function: Examination of Multiple Factors that Influence Gait Variability. Gerontol. Geriatr. Med. 2022, 8, 233372142210803. [Google Scholar] [CrossRef] [PubMed]
- Harridge, S.D.R.; Lazarus, N.R. Physical Activity, Aging, and Physiological Function. Physiology 2017, 32, 152–161. [Google Scholar] [CrossRef]
- Cohen, J. Set correlation and contingency tables. Appl. Psychol. Meas. 1988, 12, 425–434. [Google Scholar] [CrossRef]
- Uyanık, G.K.; Güler, N. A Study on Multiple Linear Regression Analysis. Procedia-Soc. Behav. Sci. 2013, 106, 234–240. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Basead Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018; Volume 7, ISBN 978146253454. [Google Scholar]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Stevens, J.A.; Sogolow, E.D. Gender differences for non-fatal unintentional fall related injuries among older adults. Inj. Prev. 2005, 11, 115–119. [Google Scholar] [CrossRef]
- Niederer, D.; Engeroff, T.; Fleckenstein, J.; Vogel, O.; Vogt, L. The age-related decline in spatiotemporal gait characteristics is moderated by concerns of falling, history of falls & diseases, and sociodemographic-anthropometric characteristics in 60–94 years old adults. Eur. Rev. Aging Phys. Act. 2021, 18, 19. [Google Scholar]
- Gouveia, É.R.; Gouveia, B.R.; Ihle, A.; Kliegel, M.; Marques, A.; Freitas, D.L. Balance and mobility relationships in older adults: A representative population-based cross-sectional study in Madeira, Portugal. Arch. Gerontol. Geriatr. 2019, 80, 65–69. [Google Scholar] [CrossRef]
- Espy, D.D.; Yang, F.; Bhatt, T.; Pai, Y.-C. Independent influence of gait speed and step length on stability and fall risk. Gait Posture 2010, 32, 378–382. [Google Scholar] [CrossRef]
- Kaczmarczyk, K.; Błażkiewicz, M.; Wiszomirska, I.; Pietrasik, K.; Zdrodowska, A.; Wit, A.; Barton, G.; Skarżyński, H. Assessing Gait Stability before and after Cochlear Implantation. Biomed Res. Int. 2019, 2019, 2474273. [Google Scholar] [CrossRef]
- Brach, J.S.; Studenski, S.A.; Perera, S.; VanSwearingen, J.M.; Newman, A.B. Gait variability and the risk of incident mobility disability in community-dwelling older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 983–988. [Google Scholar] [CrossRef]
- Verghese, J.; Holtzer, R.; Lipton, R.B.; Wang, C. Quantitative Gait Markers and Incident Fall Risk in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64A, 896–901. [Google Scholar] [CrossRef]
- Resnick, B.; Boltz, M.; Galik, E.; Holmes, S.; Fix, S.; Zhu, S. Gender Differences in Function, Physical Activity, Falls, Medication Use, and Life Satisfaction Among Residents in Assisted Living Settings. Res. Gerontol. Nurs. 2020, 13, 31–40. [Google Scholar] [CrossRef]
- Stevens, J.A.; Mahoney, J.E.; Ehrenreich, H. Circumstances and outcomes of falls among high risk community-dwelling older adults. Inj. Epidemiol. 2014, 1, 5. [Google Scholar] [CrossRef]
- Duckham, R.L.; Procter-Gray, E.; Hannan, M.T.; Leveille, S.G.; Lipsitz, L.A.; Li, W. Sex differences in circumstances and consequences of outdoor and indoor falls in older adults in the MOBILIZE Boston cohort study. BMC Geriatr. 2013, 13, 133. [Google Scholar] [CrossRef]
- Slade, S.C.; Carey, D.L.; Hill, A.M.; Morris, M.E. Effects of falls prevention interventions on falls outcomes for hospitalised adults: Protocol for a systematic review with meta-analysis. BMJ Open 2017, 7, e017864. [Google Scholar] [CrossRef]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef]
- Rosano, C.; Aizenstein, H.; Brach, J.; Longenberger, A.; Studenski, S.; Newman, A.B. Gait Measures Indicate Underlying Focal Gray Matter Atrophy in the Brain of Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 1380–1388. [Google Scholar] [CrossRef]
- Verghese, J.; Wang, C.; Lipton, R.B.; Holtzer, R.; Xue, X. Quantitative gait dysfunction and risk of cognitive decline and dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 929–935. [Google Scholar] [CrossRef]
- Montero-Odasso, M. Gait as a biomarker of cognitive impairment and dementia syndromes. Quo vadis? Eur. J. Neurol. 2016, 23, 437–438. [Google Scholar] [CrossRef] [PubMed]
- Toots, A.T.M.; Taylor, M.E.; Lord, S.R.; Close, J.C.T. Associations Between Gait Speed and Cognitive Domains in Older People with Cognitive Impairment. J. Alzheimer’s Dis. 2019, 71, S15–S21. [Google Scholar] [CrossRef] [PubMed]
- Plummer, P.; Zukowski, L.A.; Giuliani, C.; Hall, A.M.; Zurakowski, D. Effects of Physical Exercise Interventions on Gait-Related Dual-Task Interference in Older Adults: A Systematic Review and Meta-Analysis. Gerontology 2015, 62, 94–117. [Google Scholar] [CrossRef] [PubMed]
- Teraz, K.; Šlosar, L.; Paravlić, A.H.; de Bruin, E.D.; Marusic, U. Impact of Motor-Cognitive Interventions on Selected Gait and Balance Outcomes in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Psychol. 2022, 13, 837710. [Google Scholar] [CrossRef] [PubMed]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef]
- Van Abbema, R.; de Greef, M.; Crajé, C.; Krijnen, W.; Hobbelen, H.; van der Schans, C. What type, or combination of exercise can improve preferred gait speed in older adults? A meta-analysis. BMC Geriatr. 2015, 15, 72. [Google Scholar] [CrossRef]
- Wollesen, B.; Wildbredt, A.; van Schooten, K.S.; Lim, M.L.; Delbaere, K. The effects of cognitive-motor training interventions on executive functions in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 9. [Google Scholar] [CrossRef]
- Varela-Vásquez, L.A.; Minobes-Molina, E.; Jerez-Roig, J. Dual-task exercises in older adults: A structured review of current literature. J. Frailty Sarcopenia Falls 2020, 5, 31–37. [Google Scholar] [CrossRef]
- Scheffer, A.C.; Schuurmans, M.J.; van dijk, N.; van der Hooft, T.; de Rooij, S.E. Fear of falling: Measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing 2008, 37, 19–24. [Google Scholar] [CrossRef]
- Friedman, S.M.; Munoz, B.; West, S.K.; Ruben, G.S.; Fried, L.P. Falls and fear of falling: Which comes first? A longitudinal secondary prevention. J. Am. Geriatr. Soc. 2002, 50, 1329–1335. [Google Scholar] [CrossRef]
- VanderWeele, T.J. Mediation Analysis: A Practitioner’s Guide. Annu. Rev. Public Health 2016, 37, 17–32. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation Analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef]
- Fradelos, E.; Papathanasiou, I.; Mitsi, D.; Tsaras, K.; Kleisiaris, C.; Kourkouta, L. Health Based Geographic Information Systems (GIS) and their Applications. Acta Inform. Med. 2014, 22, 402. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Full Sample (n = 619) | Female (n = 314) | Male (n = 305) | p Value |
|---|---|---|---|---|
| Age (years) | 69.50 ± 5.62 | 69.49 ± 5.57 | 69.51 ± 5.70 | 0.960 |
| Age group n (%) | 0.842 | |||
| 60–69 years | 294 (47.5) | 145 (46.2) | 149 (48.8) | |
| 70–79 years | 303 (48.9) | 158 (50.3) | 145 (47.5) | |
| 80–89 years | 22 (3.5) | 11 (3.5) | 11 (3.6) | |
| Falls (%) | <0.001 | |||
| Yes | 225 (36.3) | 153 (48.7) | 72 (23.6) | |
| No | 394 (63.7) | 152 (48.4) | 242 (79.3) | |
| Number of falls (n) | <0.001 | |||
| 1–2 | 164 (72.9) | 104 (33.1) | 60 (19.7) | |
| 3–4 | 38 (16.9) | 31 (9.8) | 7 (2.2) | |
| 5–6 | 15 (6.7) | 13 (4.1) | 2 (0.6) | |
| 7–10 | 8 (3.6) | 5 (1.6) | 3 (0.9) | |
| Fear of falling (n) | 2.21 ± 0.50 | 2.44 ± 0.84 | 2.48 ± 0.72 | 0.202 |
| Medication (n) | 3.85 ± 1.97 | 4.10 ± 1.32 | 4.71 ± 1.01 | 0.048 |
| Height (cm) | 159.05 ± 8.69 | 152.94 ± 5.72 | 165.64 ± 5.73 | <0.001 |
| Weight (kg) | 74.77 ± 13.06 | 70.92 ± 12.14 | 79.22 ± 12.45 | <0.001 |
| BMI (kg/m2) | 29.51 ± 4.34 | 30.28 ± 4.73 | 28.80 ± 3.86 | <0.001 |
| Hypertension | 308 (49.7) | 162 (51.6) | 146 (47.8) | 0.041 |
| Diabetes | 148 (23.9) | 56 (17.8) | 92 (30.1) | 0.028 |
| Visual impairment | 378 (61.0) | 284 (90.4) | 202 (66.2) | 0.032 |
| Hearing problems | 191 (30.8) | 89 (28.3) | 107 (35.0) | 0.029 |
| Musculoarticular problems | 46 (5.7) | 24 (7.6) | 22 (7.2) | 0.049 |
| GS (sec.) | 1.26 ± 0.25 | 1.22 ± 0.24 | 1.29 ± 0.24 | <0.001 |
| CAD (sec.) | 1.91 ± 0.22 | 1.94 ± 0.22 | 1.89 ± 0.22 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, M.d.M.; Gouveia, É.R.; Gouveia, B.R.; Marques, A.; França, C.; Marconcin, P.; Freitas, D.L.; Ihle, A. Sex Differences in Falls: The Mediating Role of Gait Stability Ratio and Body Balance in Vulnerable Older Adults. J. Clin. Med. 2023, 12, 450. https://doi.org/10.3390/jcm12020450
Nascimento MdM, Gouveia ÉR, Gouveia BR, Marques A, França C, Marconcin P, Freitas DL, Ihle A. Sex Differences in Falls: The Mediating Role of Gait Stability Ratio and Body Balance in Vulnerable Older Adults. Journal of Clinical Medicine. 2023; 12(2):450. https://doi.org/10.3390/jcm12020450
Chicago/Turabian StyleNascimento, Marcelo de Maio, Élvio Rúbio Gouveia, Bruna R. Gouveia, Adilson Marques, Cíntia França, Priscila Marconcin, Duarte L. Freitas, and Andreas Ihle. 2023. "Sex Differences in Falls: The Mediating Role of Gait Stability Ratio and Body Balance in Vulnerable Older Adults" Journal of Clinical Medicine 12, no. 2: 450. https://doi.org/10.3390/jcm12020450
APA StyleNascimento, M. d. M., Gouveia, É. R., Gouveia, B. R., Marques, A., França, C., Marconcin, P., Freitas, D. L., & Ihle, A. (2023). Sex Differences in Falls: The Mediating Role of Gait Stability Ratio and Body Balance in Vulnerable Older Adults. Journal of Clinical Medicine, 12(2), 450. https://doi.org/10.3390/jcm12020450