
Perineural Invasion Predicts Local Recurrence and Poor Survival in Laryngeal Cancer
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics and Surgical Parameters
3.2. Tumor Characteristics
3.3. Risk Factors for 5-Year Overall Survival
3.4. Risk Factors for 5-Year Disease-Free Survival
3.5. Patterns of Recurrence According to PNI Status
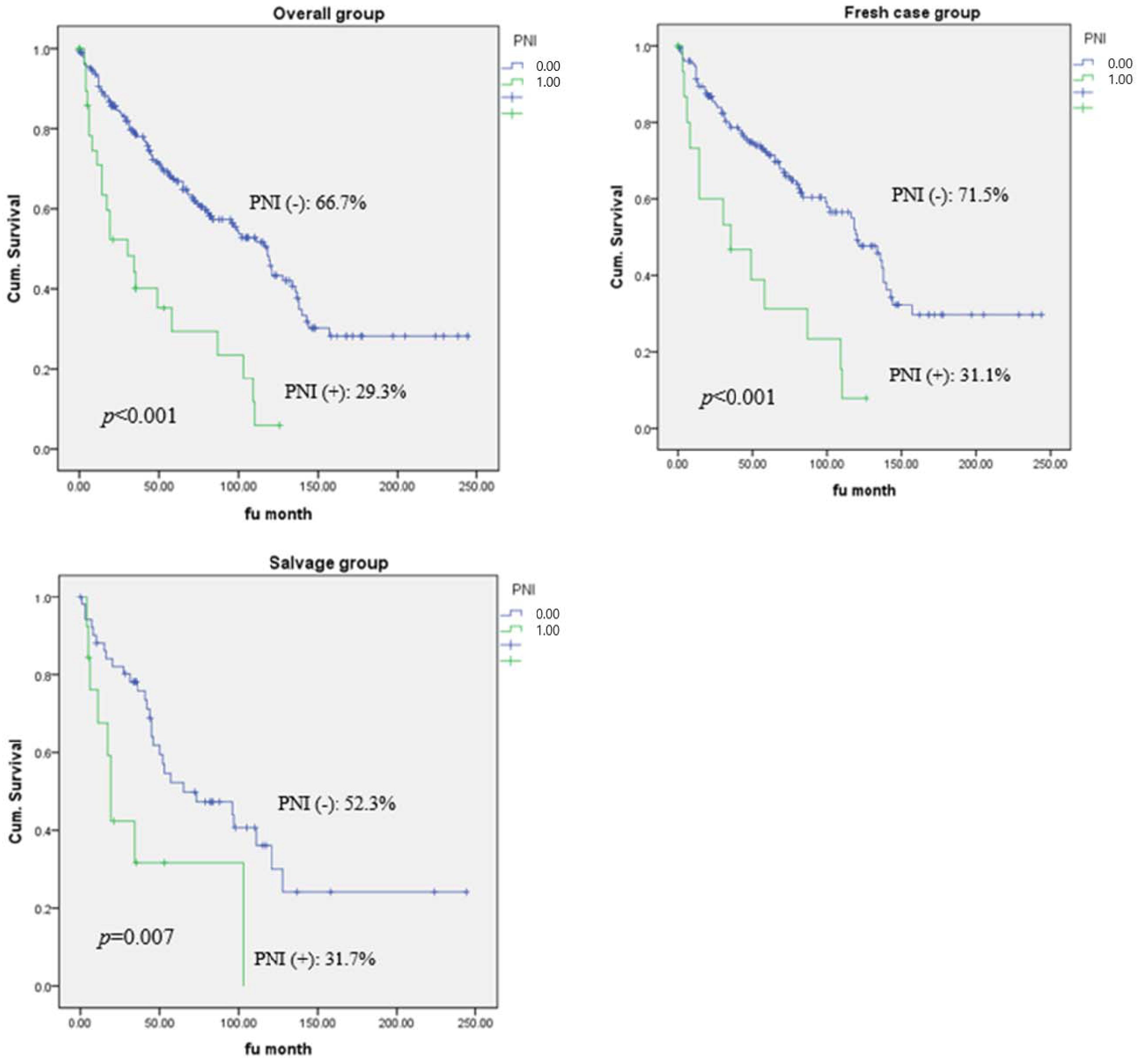
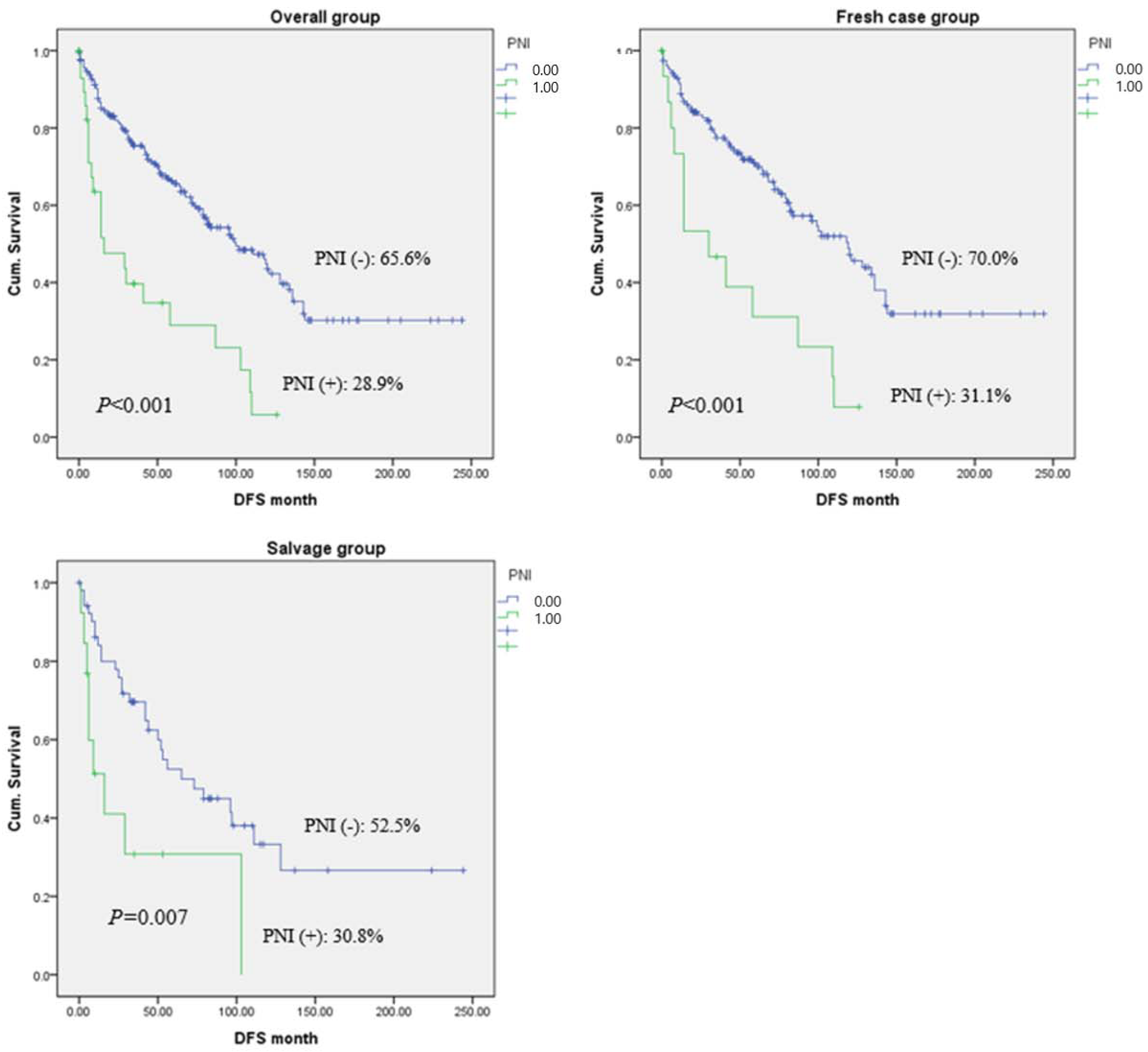
3.6. Survival Analysis According to PNI Status and Treatment History
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnes, L.; Eveson, J.W.; Sidransky, D.; Reichart, P. Pathology and Genetics of Head and Neck Tumours; IARC: Lyon, France, 2005. [Google Scholar]
- Jemal, A.; Siegel, R.; Ward, E.; Murray, T.; Xu, J.; Thun, M.J. CA: A cancer journal for clinicians. Cancer Stat. 2007, 57, 43–66. [Google Scholar]
- Kwabi-Addo, B.; Lindstrom, T.L. Cancer Causes and Controversies: Understanding Risk Reduction and Prevention: Understanding Risk Reduction and Prevention; ABC-CLIO: Santa Barbara, CA, USA, 2011. [Google Scholar]
- Zhu, X.; Duan, F.; Zhu, Y.; Shi, X.; Sun, S.; Cheng, Y.; Chen, X. Perineural Invasion as a Prognostic Factor in Laryngeal Squamous Cell Cancer: A Matched-Pair Survival Analysis. Cancer Investig. 2021, 39, 734–740. [Google Scholar] [CrossRef]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: A review of the literature. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2009, 115, 3379–3391. [Google Scholar] [CrossRef] [PubMed]
- Batsakis, J.G. Nerves and neurotropic carcinomas. Ann. Otol. Rhinol. Laryngol. 1985, 94, 426–427. [Google Scholar] [CrossRef] [PubMed]
- Fagan, J.J.; Collins, B.; Barnes, L.; D’Amico, F.; Myers, E.N.; Johnson, J.T. Perineural Invasion in Squamous Cell Carcinoma of the Head and Neck. Arch. Otolaryngol. Neck Surg. 1998, 124, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, T.; Hosal, A.S.; Gedikoǧlu, G.; Önerci, M.; Grsel, B. Prognostic significance of vascular and perineura invasion in cancer of the larynx. Am. J. Otolaryngol. 1998, 19, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Vural, E.; Fan, C.Y.; Spring, P.; Stack, B.C., Jr.; Kokoska, M.S.; Hanna, E.Y.; Suen, J.Y. Evaluation of the inferior and superior laryngeal nerve stumps for perineural spread in laryngeal cancer. Otolaryngol. Head Neck Surg. 2007, 137, 889–892. [Google Scholar] [CrossRef]
- Bova, R.; Goh, R.; Poulson, M.; Coman, W.B. Total Pharyngolaryngectomy for Squamous Cell Carcinoma of the Hypopharynx: A Review. Laryngoscope 2005, 115, 864–869. [Google Scholar] [CrossRef]
- Chirilă, M.; Bolboacă, S.D.; Cosgarea, M.; Tomescu, E.; Mureşan, M. Perineural invasion of the major and minor nerves in laryngeal and hypopharyngeal cancer. Otolaryngol. Head Neck Surg. 2009, 140, 65–69. [Google Scholar] [CrossRef]
- Soo, K.-C.; Carter, R.L.; O’Brien, C.J.; Barr, L.; Bliss, J.M.; Shaw, H.J. Prognostic implications of perineural spread in squamous carcinomas of the head and neck. Laryngoscope 1986, 96, 1145–1148. [Google Scholar] [CrossRef]
- Barrett, A.W.; Pratt, M.K.; Sassoon, I.; Bisase, B.S.; Newman, L.; Tighe, J.V.; Norris, P.M.; Dhanda, J.; Gulati, A. Perineural and lymphovascular invasion in squamous cell carcinoma of the tongue. J. Oral. Pathol. Med. 2021, 50, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, K.T.; Gal, T.J.; Ebelhar, A.J.; Valentino, J.; Brill, Y.M.; Dressler, E.; Aouad, R.K. Prognostic indicators and survival in salvage surgery for laryngeal cancer. Head Neck 2017, 39, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.T.; Chang, J.T.; Wang, H.M.; Ng, S.H.; Hsueh, C.; Lee, L.Y.; Lin, C.H.; Chen, I.H.; Huang, S.F.; Cheng, A.J.; et al. Does adjuvant radiation therapy improve outcomes in pT1-3N0 oral cavity cancer with tumor-free margins and perineural invasion? Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-C.; Wang, C.-P.; Ko, J.-Y.; Yang, T.-L.; Hsu, C.-W.; Yeh, K.-A.; Chang, Y.-L.; Lou, P.-J. The Impact of Perineural Invasion and/or Lymphovascular Invasion on the Survival of Early-Stage Oral Squamous Cell Carcinoma Patients. Ann. Surg. Oncol. 2013, 20, 2388–2395. [Google Scholar] [CrossRef]
- Department of Veterans Affairs Laryngeal Cancer Study Group; Wolf, G.T.; Fisher, S.G.; Hong, W.K.; Hillman, R.; Spaulding, M.; Laramore, G.E.; Endicott, J.W.; McClatchey, K.; Henderson, W.G. Induction Chemotherapy plus Radiation Compared with Surgery plus Radiation in Patients with Advanced Laryngeal Cancer. N. Engl. J. Med. 1991, 324, 1685–1690. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent Chemotherapy and Radiotherapy for Organ Preservation in Advanced Laryngeal Cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef]
- Markou, K.; Goudakos, J.; Triaridis, S.; Konstantinidis, J.; Vital, V.; Nikolaou, A. The role of tumor size and patient’s age as prognostic factors in laryngeal cancer. Hippokratia 2011, 15, 75–80. [Google Scholar]
- Morales-Angulo, C.; Val-Bernal, F.; Buelta, L.; Fernandez, F.; García-Castrillo, L.; Rama, J. Prognostic factors in supraglottic laryngeal carcinoma. Otolaryngol. Head Neck Surg. 1998, 119, 548–553. [Google Scholar]
- Pulkkinen, J.O.; Klemi, P.; Martikainen, P.; Grénman, R. Apoptosis in situ, p53, bcl-2 and AgNOR counts as prognostic factors in laryngeal carcinoma. Anticancer Res. 1999, 19, 703–707. [Google Scholar]
- Meulemans, J.; Debacker, J.; Demarsin, H.; Vanclooster, C.; Neyt, P.; Mennes, T.; Vauterin, T.; Huvenne, W.; Laenen, A.; Delaere, P.; et al. Oncologic Outcomes After Salvage Laryngectomy for Squamous Cell Carcinoma of the Larynx and Hypopharynx: A Multicenter Retrospective Cohort Study. Ann. Surg. Oncol. 2020, 28, 1751–1761. [Google Scholar] [CrossRef]
- Ballantyne, A.; McCarten, A.B.; Ibanez, M.L. The extension of cancer of the head and neck through peripheral nerves. Am. J. Surg. 1963, 106, 651–667. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, P.; Welz, C.; Jacobi, C.; Reiter, M. Is Perineural Invasion of Head and Neck Squamous Cell Carcinomas Linked to Tobacco Consumption? Otolaryngol. Head Neck Surg. 2018, 158, 878–881. [Google Scholar] [CrossRef] [PubMed]
- Hinerman, R.W.; Mendenhall, W.M.; Ms, C.G.M.; Amdur, R.J.; Werning, J.W.; Villaret, D.B. Postoperative irradiation for squamous cell carcinoma of the oral cavity: 35-year experience. Head Neck 2004, 26, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, K.A.; Hoffman, H.T.; Zimmerman, M.B.; Robinson, R.A. Perineural and vascular invasion in oral cavity squamous carcinoma: Increased incidence on re-review of slides and by using immunohistochemical enhancement. Arch. Pathol. Lab. Med. 2005, 129, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Rahima, B.; Shingaki, S.; Nagata, M.; Saito, C. Prognostic significance of perineural invasion in oral and oropharyngeal carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2004, 97, 423–431. [Google Scholar] [CrossRef]
- Ozaki, H.; Hiraoka, T.; Mizumoto, R.; Matsuno, S.; Matsumoto, Y.; Nakayama, T.; Tsunoda, T.; Suzuki, T.; Monden, M.; Saitoh, Y.; et al. The prognostic significance of lymph node metastasis and intrapancreatic perineural invasion in pancreatic cancer after curative resection. Surg. Today 1999, 29, 16–22. [Google Scholar] [CrossRef]
- Law, W.L.; Chu, K.W. Anterior resection for rectal cancer with mesorectal excision: A prospective evaluation of 622 patients. Ann. Surg. 2004, 240, 260–268. [Google Scholar] [CrossRef]
- Beard, C.; Chen, M.; Cote, K.; Loffredo, M.; Renshaw, A.; Hurwitz, M.; D’Amico, A. Perineural invasion is associated with increased relapse after external beam radiotherapy for men with low-risk prostate cancer and may be a marker for occult, high-grade cancer. Int. J. Radiat. Oncol. 2004, 58, 19–24. [Google Scholar] [CrossRef]
- Su, C.-H.; Tsay, S.-H.; Wu, C.-C.; Shyr, Y.-M.; King, K.-L.; Lee, C.-H.; Lui, W.-Y.; Liu, T.-J.; P’Eng, F.-K. Factors Influencing Postoperative Morbidity, Mortality, and Survival after Resection for Hilar Cholangiocarcinoma. Ann. Surg. 1996, 223, 384–394. [Google Scholar] [CrossRef]
- Duraker, N.; Şişman, S.; Can, G. The Significance of Perineural Invasion as a Prognostic Factor in Patients with Gastric Carcinoma. Surg. Today 2003, 33, 95–100. [Google Scholar] [CrossRef]
- Maddox, W.A. Vicissitudes of head and neck cancer. Am. J. Surg. 1984, 148, 428–432. [Google Scholar] [CrossRef] [PubMed]
- McGavran, M.H.; Bauer, W.C.; Ogura, J.H. The incidence of cervical lymph node metastases from epidermoid carcinoma of the larynx and their relationship to certain characteristics of the primary tumor.A study based on the clinical and pathological findings for 96 patients treated by primary en bloc laryngectomy and radical neck dissection. Cancer 1961, 14, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.; Barnes, L.; Mazariegos, J.; Taylor, F.; Johnson, J.; Bs, R.L.W. Prognostic factors in mobile tongue and floor of mouth carcinoma. Cancer 1989, 64, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.O.; Maksem, J. The prostatic perineural space and its relation to tumor spread: An ultrastructural study. Am. J. Surg. Pathol. 1980, 4, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Bakst, R.L.; Wong, R.J. Mechanisms of Perineural Invasion. J. Neurol. Surg. Part B: Skull Base 2016, 77, 96–106. [Google Scholar] [CrossRef]
- Gil, Z.; Cavel, O.; Kelly, K.; Brader, P.; Rein, A.; Gao, S.P.; Carlson, D.L.; Shah, J.; Fong, Y.; Wong, R.J. Paracrine Regulation of Pancreatic Cancer Cell Invasion by Peripheral Nerves. Gynecol. Oncol. 2010, 102, 107–118. [Google Scholar] [CrossRef]
- Ayala, G.E.; Wheeler, T.M.; Shine, H.D.; Schmelz, M.; Frolov, A.; Chakraborty, S.; Rowley, D. In vitro dorsal root ganglia and human prostate cell line interaction: Redefining perineural invasion in prostate cancer. Prostate 2001, 49, 213–223. [Google Scholar] [CrossRef]
- Cornell, R.J.; Rowley, D.; Wheeler, T.; Ali, N.; Ayala, G. Neuroepithelial interactions in prostate cancer are enhanced in the presence ofprostatic stroma. Urology 2003, 61, 870–875. [Google Scholar] [CrossRef]
- Chilton, J.K. Molecular mechanisms of axon guidance. Dev. Biol. 2006, 292, 13–24. [Google Scholar] [CrossRef]
- Chédotal, A.; Kerjan, G.; Moreau-Fauvarque, C. The brain within the tumor: New roles for axon guidance molecules in cancers. Cell Death Differ. 2005, 12, 1044–1056. [Google Scholar] [CrossRef]
- Boyd, J.G.; Gordon, T. Neurotrophic Factors and Their Receptors in Axonal Regeneration and Functional Recovery after Peripheral Nerve Injury. Mol. Neurobiol. 2003, 27, 277–324. [Google Scholar] [CrossRef] [PubMed]
- Ketterer, K.; Rao, S.; Friess, H.; Weiss, J.; Büchler, M.W.; Korc, M. Reverse transcription-PCR analysis of laser-captured cells points to potential paracrine and autocrine actions of neurotrophins in pancreatic cancer. Clin. Cancer Res. 2003, 9, 5127–5136. [Google Scholar] [PubMed]
- Okada, Y.; Eibl, G.; Guha, S.; Duffy, J.P.; Reber, H.A.; Hines, O.J. Nerve growth factor stimulates MMP-2 expression and activity and increases invasion by human pancreatic cancer cells. Clin. Exp. Metastasis 2004, 21, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Lanzer, M.; Gander, T.; Kruse, A.; Luebbers, H.; Reinisch, S. Influence of histopathologic factors on pattern of metastasis in squamous cell carcinoma of the head and neck. Laryngoscope 2013, 124, E160–E166. [Google Scholar] [CrossRef]
- Aivazian, K.; Ebrahimi, A.; Low, T.-H.H.; Gao, K.; Clifford, A.; Shannon, K.; Clark, J.R.; Gupta, R. Perineural invasion in oral squamous cell carcinoma: Quantitative subcategorisation of perineural invasion and prognostication. J. Surg. Oncol. 2014, 111, 352–358. [Google Scholar] [CrossRef]
- Brandwein-Gensler, M.; Smith, R.V.; Wang, B.; Penner, C.; Theilken, A.; Broughel, D.; Schiff, B.; Owen, R.P.; Smith, J.; Sarta, C.; et al. Validation of the Histologic Risk Model in a New Cohort of Patients with Head and Neck Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2010, 34, 676–688. [Google Scholar] [CrossRef]
- Bur, A.; Lin, A.; Weinstein, G.S. Adjuvant radiotherapy for early head and neck squamous cell carcinoma with perineural invasion: A systematic review. Head Neck 2015, 38, E2350–E2357. [Google Scholar] [CrossRef]
- Carter, J.B.; Johnson, M.M.; Chua, T.L.; Karia, P.S.; Schmults, C.D. Outcomes of primary cutaneous squamous cell carcinoma with perineural invasion: An 11-year cohort study. JAMA Dermatol. 2013, 149, 35–41. [Google Scholar] [CrossRef]
- Chatzistefanou, I.; Lubek, J.; Markou, K.; Ord, R.A. The role of perineural invasion in treatment decisions for oral cancer patients: A review of the literature. J. Cranio-Maxillofac. Surg. 2017, 45, 821–825. [Google Scholar] [CrossRef]
- Miller, M.E.; Palla, B.; Chen, Q.; Elashoff, D.A.; Abemayor, E.; John, M.A.S.; Lai, C.K. A novel classification system for perineural invasion in noncutaneous head and neck squamous cell carcinoma: Histologic subcategories and patient outcomes. Am. J. Otolaryngol. 2012, 33, 212–215. [Google Scholar] [CrossRef]
- Tai, S.-K.; Li, W.-Y.; Yang, M.-H.; Chang, S.-Y.; Chu, P.-Y.; Tsai, T.-L.; Wang, Y.-F.; Chang, P.M.-H. Treatment for T1-2 Oral Squamous Cell Carcinoma with or without Perineural Invasion: Neck Dissection and Postoperative Adjuvant Therapy. Ann. Surg. Oncol. 2011, 19, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Chi, A.C.; Katabi, N.; Chen, H.-S.; Cheng, Y.-S.L. Interobserver Variation Among Pathologists in Evaluating Perineural Invasion for Oral Squamous Cell Carcinoma. Head Neck Pathol. 2016, 10, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Santos, T.S.; Estêvão, R.; Antunes, L.; Certal, V.; Silva, J.C.; Monteiro, E. Clinical and histopathological prognostic factors in locoregional advanced laryngeal cancer. J. Laryngol. Otol. 2016, 130, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Langendijk, J.A.; Slotman, B.; Van Der Waal, V.; Doornaert, P.; Berkof, J.; Leemans, C.R. Risk-group definition by recursive partitioning analysis of patients with squamous cell head and neck carcinoma treated with surgery and postoperative radiotherapy. Cancer 2005, 104, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefèbvre, J.-L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. European Organization for Research and Treatment of Cancer Trial 22931. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck Cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef]
- Bradford, C.R.; Wolf, G.T.; Fisher, S.G.; McClatchey, K.D. Prognostic importance of surgical margins in advanced laryngeal squamous carcinoma. Head Neck 1996, 18, 11–16. [Google Scholar] [CrossRef]
- Manni, J.J.; Terhaard, C.H.; de Boer, M.F.; Croll, G.A.; Hilgers, F.J.; Annyas, A.A.; van der Meij, A.G.; Hordijk, G.J. Prognostic factors for survival in patients with T3 laryngeal carcinoma. Am. J. Surg. 1992, 164, 682–687. [Google Scholar] [CrossRef]
- Saraniti, C.; Speciale, R.; Gallina, S.; Salvago, P. Prognostic role of resection margin in open oncologic laryngeal surgery: Survival analysis of a cohort of 139 patients affected by squamous cell carcinoma. Braz. J. Otorhinolaryngol. 2019, 85, 603–610. [Google Scholar] [CrossRef]
- Zhou, J.; Zhou, L.; Tao, L.; Zhang, M.; Wu, H.; Chen, X.; Li, X.; Li, C.; Gong, H. Oncologic outcomes of surgical treatment for T3 glottic laryngeal squamous cell carcinoma. Head Neck 2018, 40, 1734–1742. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | N (%) |
|---|---|
| Sex (male:female) | 218:22 |
| Age (years old, mean ± SD) | 64.82 ± 9.63 |
| Smoking | |
| 40 pack years | 97 (40.4%) |
| Less than 40 pack years | 120 (50%) |
| Primary Site | |
| Glottis | 66 (27.5%) |
| Supraglottis | 64 (26.6%) |
| Transglottis | 110 (45.8%) |
| Previous treatment status | |
| None (fresh case) | 175 (72.9%) |
| RT failure | 38 (15.8%) |
| Surgery failure | 27 (11.2%) |
| Type of surgery | |
| Total laryngectomy | 81 (33.7%) |
| Vertical partial hemilaryngectomy | 21 (8.7%) |
| Supraglottic partial laryngectomy | 33 (13.7%) |
| Supracricoid partial laryngectomy | 105 (43.7%) |
| TN stage (pathologic) | |
| T1 | 23 (9.5%) |
| T2 | 67 (27.9%) |
| T3 | 84 (35%) |
| T4 | 66 (27.5%) |
| N0 | 165 (68.7%) |
| N1 | 18 (7.5%) |
| N2 | 36 (15%) |
| N3 | 21 (8.7%) |
| Postoperative adjuvant therapy | |
| RT | 49 (20.4%) |
| CCRT | 48 (20%) |
| None | 143 (59.5%) |
| Parameters | N (%) |
|---|---|
| Differentiation (1: WD, 2: PD) | 66:18 (27.5%:7.5%) |
| Longest dimension (mm; mean ± SD) | 25.96 ± 13.34 |
| Depth of invasion (mm; mean ± SD) | 10.37 ± 7.12 |
| Margin status (clear:close:positive) | 149:54:37 (62%:22.5%:15.4%) |
| Paraglottic space invasion | 117 (48.7%) |
| Preepiglottic space invasion | 43 (17.9%) |
| Lymphatic invasion | 60 (25.0%) |
| Vascular invasion | 13 (5.4%) |
| Perineural invasion | 30 (12.5%) |
| Parameters | Fresh Cases (n = 175) | Salvage Cases (n = 65) | Overall (n = 240) |
|---|---|---|---|
| HR (p, 95% CI) | HR (p, 95% CI) | HR (p, 95% CI) | |
| Margin positive (ref. margin negative) | 1.25 (0.46, 0.68–2.28) | 1.96 (0.14, 0.78–4.90) | 1.36 (0.22, 0.82–2.25) |
| Paraglottic space invasion | 1.47 (0.07, 0.95–2.28) | 1.59 (0.15, 0.83–3.03) | 1.49 (0.02, 1.04–2.14) |
| Preepiglottic space invasion | 2.23 (0.01, 1.36–3.66) | 1.16 (0.75, 0.45–2.98) | 1.87 (0.04, 1.21–2.88) |
| Lymphatic invasion | 1.67 (0.03, 1.04–2.68) | 1.74 (0.13, 0.84–3.60) | 1.80 (0.02, 1.23–2.62) |
| Vascular invasion | 0.87 (0.78, 0.34–2.22) | 3.87 (0.07, 0.88–17.04) | 1.41 (0.37, 0.65–3.04) |
| Perineural invasion | 2.73 (0.01, 1.47–5.09) | 2.80 (0.01, 1.28–6.12) | 3.19 (0.01, 1.99–5.12) |
| Parameters | Fresh Cases (n = 175) | Salvage Cases (n = 65) | Overall (n = 240) |
|---|---|---|---|
| HR (p, 95% CI) | HR (p, 95% CI) | HR (p, 95% CI) | |
| Margin positive (ref. margin negative) | 1.14 (0.66, 0.62–2.08) | 1.96 (0.14, 0.78–4.89) | 1.26 (0.35, 0.76–2.08) |
| Paraglottic space invasion | 1.43 (0.10, 0.92–2.21) | 1.51 (0.20, 0.79–2.87) | 1.42 (0.05, 0.99–2.03) |
| Preepiglottic space invasion | 2.37 (0.01, 1.45–3.88) | 1.20 (0.67, 0.47–3.09) | 1.92 (0.03, 1.25–2.96) |
| Lymphatic invasion | 1.80 (0.09, 1.15–2.83) | 1.84 (0.09, 0.89–3.79) | 1.74 (0.04, 1.19–2.54) |
| Vein invasion | 1.21 (0.68, 0.48–2.99) | 2.89 (0.15, 0.67–12.51) | 1.40 (0.38, 0.65–3.02) |
| Perineural invasion | 2.96 (0.01, 1.62–2.96) | 2.74 (0.01, 1.26–5.92) | 3.05 (0.01, 1.90–4.88) |
| Parameters | PNI (+), n = 30 | PNI (−), n = 210 | HR (p, 95%CI) |
|---|---|---|---|
| Local recurrence | 3 (10%) | 8 (3.8%) | 5.02 (0.02, 1.28–9.66) |
| Regional recurrence | 2 (6.0%) | 9 (4.29%) | 1.25 (0.19, 0.15–2.36) |
| Distant metastasis | 3 (10.0%) | 19 (9.0%) | 0.67 (0.23, 0.61–7.17) |
| Total recurrence | 8 (26.7%) | 36 (17.1%) | 3.06 (0.04, 1.57–6.00) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H.-I.; Bang, J.-I.; Kim, G.-J.; Sun, D.-I.; Kim, S.-Y. Perineural Invasion Predicts Local Recurrence and Poor Survival in Laryngeal Cancer. J. Clin. Med. 2023, 12, 449. https://doi.org/10.3390/jcm12020449
Shin H-I, Bang J-I, Kim G-J, Sun D-I, Kim S-Y. Perineural Invasion Predicts Local Recurrence and Poor Survival in Laryngeal Cancer. Journal of Clinical Medicine. 2023; 12(2):449. https://doi.org/10.3390/jcm12020449
Chicago/Turabian StyleShin, Hyun-Il, Joo-In Bang, Geun-Jeon Kim, Dong-Il Sun, and Sang-Yeon Kim. 2023. "Perineural Invasion Predicts Local Recurrence and Poor Survival in Laryngeal Cancer" Journal of Clinical Medicine 12, no. 2: 449. https://doi.org/10.3390/jcm12020449
APA StyleShin, H.-I., Bang, J.-I., Kim, G.-J., Sun, D.-I., & Kim, S.-Y. (2023). Perineural Invasion Predicts Local Recurrence and Poor Survival in Laryngeal Cancer. Journal of Clinical Medicine, 12(2), 449. https://doi.org/10.3390/jcm12020449