
Are Thiols Useful Biomarkers for Coronary Collateral Circulation in Patients with Stable Coronary Artery Disease?

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Method
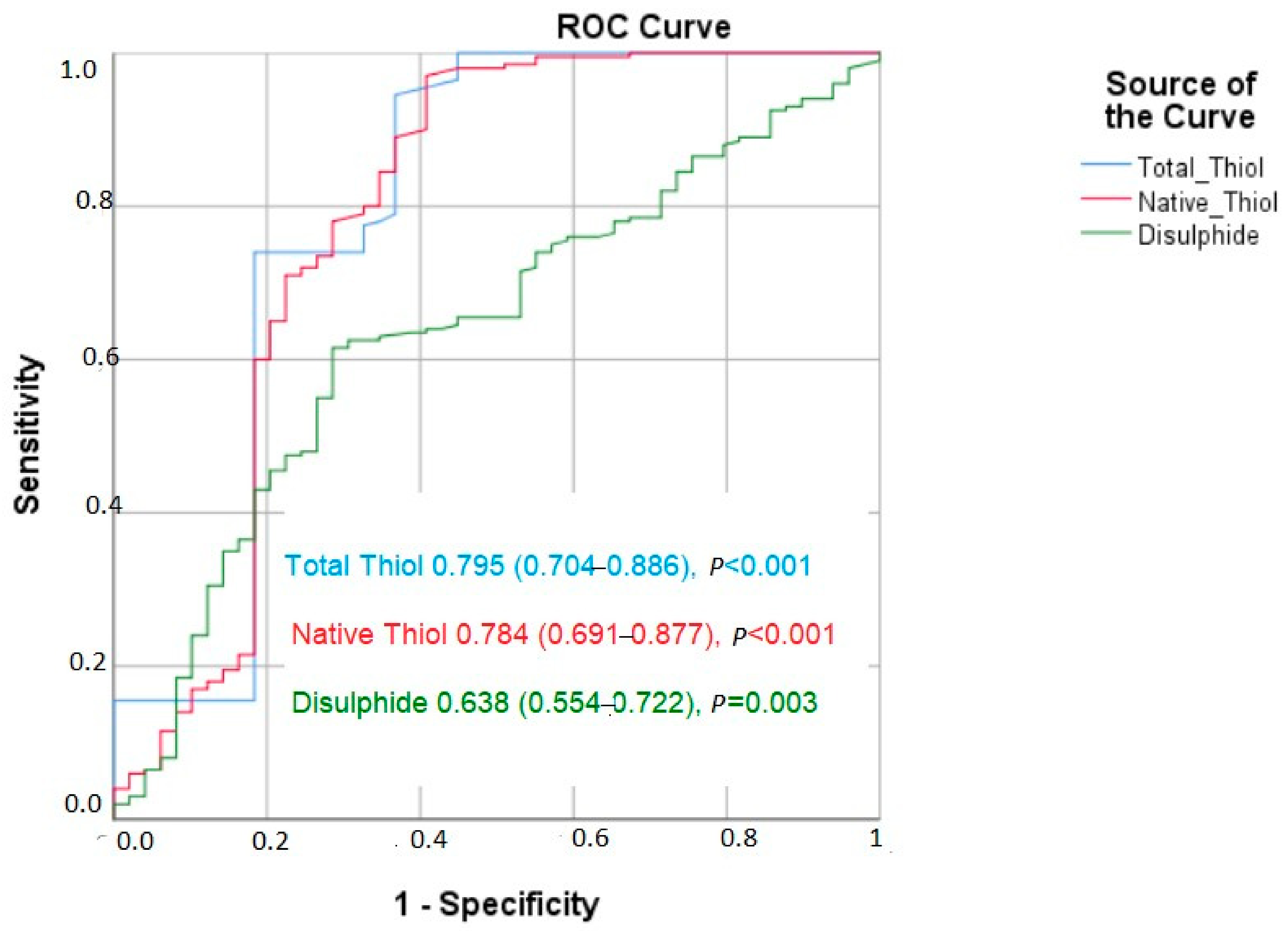
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meier, P.; Schirmer, S.H.; Lansky, A.J.; Timmis, A.; Pitt, B.; Seiler, C. The collateral circulation of the heart. BMC Med. 2013, 11, 143. [Google Scholar] [CrossRef]
- Cui, K.; Lyu, S.; Song, X.; Yuan, F.; Xu, F.; Zhang, M.; Zhang, M.; Wang, W.; Zhang, D.; Tian, J. Effect of Coronary Collaterals on Prognosis in Patients Undergoing Primary Percutaneous Coronary Intervention for Acute ST-Segment Elevation Myocardial Infarction: A Meta-Analysis. Angiology 2018, 69, 803–811. [Google Scholar] [CrossRef]
- Seiler, C.; Stoller, M.; Pitt, B.; Meier, P. The human coronary collateral circulation: Development and clinical importance. Eur. Heart J. 2013, 34, 2674–2682. [Google Scholar] [CrossRef]
- Li, S.H.; He, Z.X. Preserved Myocardial Viability in patients with Chronic Total Occlusion of a Single Coronary Artery with and without Collateral Circulation. J. Nucl. Med. 2018, 59, 1537. [Google Scholar]
- Kilian, J.G.; Keech, A.; Adams, M.R.; Celermajer, D.S. Coronary collateralization: Determinants of adequate distal vessel filling after arterial occlusion. Coron. Artery Dis. 2002, 13, 155–159. [Google Scholar] [CrossRef]
- Pourati, I.; Kimmelstiel, C.; Rand, W.; Karas, R.H. Statin use is associated with enhanced collateralization of severely diseased coronary arteries. Am. Heart J. 2003, 146, 876–881. [Google Scholar] [CrossRef]
- Boodhwani, M.; Sodha, N.R.; Mieno, S.; Xu, S.H.; Feng, J.; Ramlawi, B.; Clements, R.T.; Sellke, F.W. Functional, cellular, and molecular characterization of the angiogenic response to chronic myocardial ischemia in diabetes. Circulation 2007, 116, I31–I37. [Google Scholar] [CrossRef]
- Harrison, D.G.; Sellke, F.W.; Quillen, J.E. Neurohumoral regulation of coronary collateral vasomotor tone. Basic Res. Cardiol. 1990, 85, 121–129. [Google Scholar] [CrossRef]
- Solorio, S.; Murillo-Ortíz, B.; Hernández-González, M.; Guillén-Contreras, J.; Arenas-Aranda, D.; Solorzano-Zepeda, F.J.; Ruiz-Avila, R.; Mora-Villalpando, C.; de la Roca-Chiapas, J.M.; Malacara-Hernández, J.M. Association between telomere length and C-reactive protein and the development of coronary collateral circulation in patients with coronary artery disease. Angiology 2011, 62, 467–472. [Google Scholar] [CrossRef]
- Aras, D.; Geyik, B.; Topaloglu, S.; Ergun, K.; Ayaz, S.; Maden, O.; Yildiz, A.; Balci, M.; Ozeke, O.; Korkmaz, S. Serum level of lipoprotein (a) is inversely associated with the development of coronary collateral circulation. Coron. Artery Dis. 2006, 17, 159–163. [Google Scholar] [CrossRef]
- Guray, U.; Erbay, A.R.; Guray, Y.; Yilmaz, M.B.; Boyaci, A.A.; Sasmaz, H.; Korkmaz, S.; Kutuk, E. Poor coronary collateral circulation is associated with higher concentrations of soluble adhesion molecules in patients with single-vessel disease. Coron. Artery Dis. 2004, 15, 413–417. [Google Scholar] [CrossRef]
- Seiler, C.; Pohl, T.; Billinger, M.; Meier, B. Tumour necrosis factor alpha concentration and collateral flow in patients with coronary artery disease and normal systolic left ventricular function. Heart 2003, 89, 96–97. [Google Scholar] [CrossRef]
- Demirbag, R.; Gur, M.; Yilmaz, R.; Kunt, A.S.; Erel, O.; Andac, M.H. Influence of oxidative stress on the development of collateral circulation in total coronary occlusions. Int. J. Cardiol. 2007, 116, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Nickenig, G.; Harrison, D.G. The AT(1)-type angiotensin receptor in oxidative stress and atherogenesis: Part I: Oxidative stress and atherogenesis. Circulation 2002, 105, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Ray, R.; Shah, A.M. NADPH oxidase and endothelial cell function. Clin. Sci. 2005, 109, 217–226. [Google Scholar] [CrossRef]
- Griendling, K.K.; Fitzgerald, G.A. Oxidative stress and cardiovascular injury: Part I: Basic mechanisms and in vivo monitoring of ROS. Circulation 2003, 108, 1912–1916. [Google Scholar] [CrossRef]
- Leopold, J.A.; Loscalzo, J. Oxidative risk for atherothrombotic cardiovascular disease. Free Radic. Biol. Med. 2009, 47, 1673–1706. [Google Scholar] [CrossRef] [PubMed]
- Lubos, E.; Loscalzo, J.; Handy, D.E. Glutathione peroxidase-1 in health and disease: From molecular mechanisms to therapeutic opportunities. Antioxid. Redox Signal. 2011, 15, 1957–1997. [Google Scholar] [CrossRef] [PubMed]
- Erel, Ö.; Erdoğan, S. Thiol-disulfide homeostasis: An integrated approach with biochemical and clinical aspects. Turk. J. Med. Sci. 2020, 50, 1728–1738. [Google Scholar] [CrossRef] [PubMed]
- Altıparmak, I.H.; Erkuş, M.E.; Sezen, H.; Demirbag, R.; Gunebakmaz, O.; Kaya, Z.; Sezen, Y.; Asoglu, R.; Dedeoglu, I.H.; Neselioglu, S.; et al. The relation of serum thiol levels and thiol/disulphide homeostasis with the severity of coronary artery disease. Kardiol. Pol. 2016, 74, 1346–1353. [Google Scholar] [CrossRef]
- Kiziltunc, E.; Gok, M.; Kundi, H.; Cetin, M.; Topcuoglu, C.; Gulkan, B.; Cicekcioglu, H.; Ornek, E. Plasma thiols and thiol-disulfide homeostasis in patients with isolated coronary artery ectasia. Atherosclerosis 2016, 253, 209–213. [Google Scholar] [CrossRef]
- Cremers, C.M.; Jakob, U. Oxidant sensing by reversible disulfide bond formation. J. Biol. Chem. 2013, 288, 26489–26496. [Google Scholar] [CrossRef] [PubMed]
- Kalkan, M.; Sahin, M.; Kalkan, A.; Güler, A.; Taş, M.; Bulut, M.; Demir, S.; Acar, R.; Arslantaş, U.; Oztürkeri, B.; et al. The relationship between the neutrophil-lymphocyte ratio and the coronary collateral circulation in patients with chronic total occlusion. Perfusion 2014, 29, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Açar, G.; Kalkan, M.E.; Avci, A.; Alizade, E.; Tabakci, M.M.; Toprak, C.; Özkan, B.; Alici, G.; Esen, A.M. The relation of platelet-lymphocyte ratio and coronary collateral circulation in patients with stable angina pectoris and chronic total occlusion. Clin. Appl. Thromb. Hemost. 2015, 21, 462–468. [Google Scholar] [CrossRef]
- Ambrosio, G.; Mugelli, A.; Lopez-Sendón, J.; Tamargo, J.; Camm, J. Management of stable angina: A commentary on the European Society of Cardiology guidelines. Eur. J. Prev. Cardiol. 2016, 23, 1401–1412. [Google Scholar] [CrossRef]
- Erel, O.; Neselioglu, S. A novel and automated assay for thiol/disulphide homeostasis. Clin. Biochem. 2014, 47, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Rentrop, K.P.; Cohen, M.; Blanke, H.; Phillips, R.A. Changes in collateral channel filling immediately after controlled coronary artery occlusion by an angioplasty balloon in human subjects. J. Am. Coll. Cardiol. 1985, 5, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://syntaxscore.org (accessed on 16 August 2023).
- Ergün, G.; Yılmaz, Y. Which is more important for development coronary collateral circulation in chronic coronary syndromes; inflammation or oxidative stress? Anatol. J. Cardiol. 2022, 26 (Suppl. S1), S1–S177. [Google Scholar] [CrossRef]
- Seiler, C. The human coronary collateral circulation. Heart 2003, 89, 1352–1357. [Google Scholar] [CrossRef]
- Gök, M.; Kundi, H.; Kızıltunç, E.; Topcuoglu, C.; Ornek, E. The relationship between ischaemia-modified albumin and good coronary collateral circulation. Kardiol. Pol. 2018, 76, 370–375. [Google Scholar] [CrossRef]
- Sivri, F.; Öztürk Ceyhan, B. Increased Plasma Non-High-Density Lipoprotein Levels and Poor Coronary Collateral Circulation in Patients With Stable Coronary Artery Disease. Tex. Heart Inst. J. 2023, 50, e227934. [Google Scholar] [CrossRef] [PubMed]
- Kelesoglu, S.; Yilmaz, Y.; Elcık, D.; Kalay, N. Systemic immune inflammation index: A novel predictor for coronary collateral circulation. Perfusion 2022, 37, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Kelesoglu, S.; Yilmaz, Y.; Elcık, D. Relationship between C-Reactive Protein to Albumin Ratio and Coronary Collateral Circulation in Patients With Stable Coronary Artery Disease. Angiology 2021, 72, 829–835. [Google Scholar] [CrossRef]
- Sasayama, S.; Fujita, M. Recent insights into coronary collateral circulation. Circulation 1992, 85, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Sabia, P.J.; Powers, E.R.; Ragosta, M.; Sarembock, I.J.; Burwell, L.R.; Kaul, S. An association between collateral blood flow and myocardial viability in patients with recent myocardial infarction. N. Engl. J. Med. 1992, 327, 1825–1831. [Google Scholar] [CrossRef] [PubMed]
- Kaya, M.G.; Akpek, M.; Lam, Y.Y.; Yarlioglues, M.; Celik, T.; Gunebakmaz, O.; Duran, M.; Ulucan, S.; Keser, A.; Oguzhan, A.; et al. Prognostic value of neutrophil/lymphocyte ratio in patients with ST-elevated myocardial infarction undergoing primary coronary intervention: A prospective, multicenter study. Int. J. Cardiol. 2013, 168, 1154–1159. [Google Scholar] [CrossRef]
- Kundi, H.; Gok, M.; Kiziltunc, E.; Cetin, M.; Ornek, E. Association of IGF-1 with coronary collateral circulation in stable coronary artery disease. Biomark. Med. 2017, 11, 527–534. [Google Scholar] [CrossRef]
- Leopold, J.A. Antioxidants and coronary artery disease: From pathophysiology to preventive therapy. Coron. Artery Dis. 2015, 26, 176–183. [Google Scholar] [CrossRef]
- Arai, M.; Alpert, N.R.; MacLennan, D.H.; Barton, P.; Periasamy, M. Alterations in sarcoplasmic reticulum gene expression in human heart failure. A possible mechanism for alterations in systolic and diastolic properties of the failing myocardium. Circ. Res. 1993, 72, 463–469. [Google Scholar] [CrossRef]
- Zhao, M.; Zhu, P.; Fujino, M.; Zhuang, J.; Guo, H.; Sheikh, I.; Zhao, L.; Li, X.K. Oxidative Stress in Hypoxic-Ischemic Encephalopathy: Molecular Mechanisms and Therapeutic Strategies. Int. J. Mol. Sci. 2016, 17, 2078. [Google Scholar] [CrossRef]
- Sinha, N.; Dabla, P.K. Oxidative stress and antioxidants in hypertension-a current review. Curr. Hypertens. Rev. 2015, 11, 132–142. [Google Scholar] [CrossRef]
- Tuttle, J.L.; Sanders, B.M.; Burkhart, H.M.; Fath, S.W.; Kerr, K.A.; Watson, W.C.; Herring, B.P.; Dalsing, M.C.; Unthank, J.L. Impaired collateral artery development in spontaneously hypertensive rats. Microcirculation 2002, 9, 343–351. [Google Scholar] [CrossRef]
- Allahwala, U.K.; Khachigian, L.M.; Nour, D.; Ridiandres, A.; Billah, M.; Ward, M.; Weaver, J.; Bhindi, R. Recruitment and maturation of the coronary collateral circulation: Current understanding and perspectives in arteriogenesis. Microvasc. Res. 2020, 132, 104058. [Google Scholar] [CrossRef]
- Rocic, P.; Kolz, C.; Reed, R.; Potter, B.; Chilian, W.M. Optimal reactive oxygen species concentration and p38 MAP kinase are required for coronary collateral growth. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H2729–H2736. [Google Scholar] [CrossRef]
- Reed, R.; Kolz, C.; Potter, B.; Rocic, P. The mechanistic basis for the disparate effects of angiotensin II on coronary collateral growth. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 61–67. [Google Scholar] [CrossRef]
- Kundi, H.; Ates, I.; Kiziltunc, E.; Cetin, M.; Cicekcioglu, H.; Neselioglu, S.; Erel, O.; Ornek, E. A novel oxidative stress marker in acute myocardial infarction; thiol/disulphide homeostasis. Am. J. Emerg. Med. 2015, 33, 1567–1571. [Google Scholar] [CrossRef] [PubMed]
- Altiparmak, I.H.; Erkus, M.E.; Sezen, H.; Demirbag, R.; Kaya, Z.; Sezen, Y.; Gunebakmaz, O.; Asoglu, R.; Besli, F.; Neselioglu, S.; et al. Evaluation of thiol levels, thiol/disulfide homeostasis and their relation with inflammation in cardiac syndrome X. Coron. Artery Dis. 2016, 27, 295–301. [Google Scholar] [CrossRef]
- Kundi, H.; Gok, M.; Cetin, M.; Kiziltunç, E.; Topcuoglu, C.; Neşelioğlu, S.; Erel, O.; Ulusoy, F.V. Association of thiol disulfide homeostasis with slow coronary flow. Scand. Cardiovasc. J. 2016, 50, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Maulik, N. Reactive oxygen species drives myocardial angiogenesis? Antioxid. Redox Signal. 2006, 8, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- Fass, D. Disulfide bonding in protein biophysics. Annu. Rev. Biophys. 2012, 41, 63–79. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Coronary Collateral Circulation | ||
|---|---|---|---|
| Poor (n = 49) | Good (n = 200) | p Value | |
| Age (years) | 67 (60–74) | 62.5 (55–70) | 0.015 |
| Male gender (n, %) | 37 (75.5) | 144 (72) | 0.621 |
| DM (n, %) | 20 (40.8) | 42 (21) | 0.004 |
| HT (n, %) | 27 (55.1) | 105 (52.5) | 0.744 |
| Dyslipidemia (n, %) | 17 (34.6) | 71 (35.5) | 0.916 |
| Smoking (n, %) | 25 (%51) | 97 (49.5) | 0.957 |
| BMI (kg/m2) | 27.4 ± 3.8 | 26.9 ± 2.9 | 0.639 |
| Systolic blood pressure (mmHg) | 126.8 ± 14,6 | 125.9 ± 16.3 | 0.721 |
| Diastolic blood pressure (mmHg) | 73.9 ± 18.5 | 74.6 ± 17.6 | 0.859 |
| HR | 77.3 ± 8.8 | 75.6 ± 9.2 | 0.231 |
| LVEF (%) | 55.4 ± 7.6 | 56.1 ± 9.1 | 0.551 |
| Previous medications, n (%) | |||
| Aspirin | 14 (%28.6) | 55 (%27.5) | 0.912 |
| ΒB | 11 (%22.4) | 46 (%23) | 0.932 |
| Angiotensin–aldosterone antagonists | 9 (%18.3) | 36 (%18) | 0.923 |
| Statin | 11 (%22.4) | 40 (%21) | 0.813 |
| Clopidogrel | 3 (%6.1) | 12 (%6) | 0.894 |
| Number of Patients | Coronary Collateral Circulation | ||
|---|---|---|---|
| Poor (n = 49) | Good (n = 200) | p Value | |
| Glucose (mg/dL) | 127.1 ± 85.2 | 109.2 ± 73.3 | 0.125 |
| Creatinine (mg/dL) | 0.91 ± 0.2 | 0.86 ± 0.2 | 0.153 |
| ALT (U/L) | 24.5 ± 11.2 | 27.2 ± 12.1 | 0.454 |
| AST (U/L) | 30.3 ± 8.8 | 35.5 ± 9.6 | 0.346 |
| Total cholesterol (mg/dL) | 189 (164–231) | 186 (164–219) | 0.701 |
| High density lipoprotein cholesterol (mg/dL) | 45 (35–53) | 41 (35–47) | 0.662 |
| Low density lipoprotein cholesterol (mg/dL) | 123 (87–145) | 115 (93–137) | 0.059 |
| Triglyceride (mg/dL) | 143 (106–204) | 150 (105–215) | 0.513 |
| Hb (mg/dL) | 14 (12.5–15) | 14 (13–15) | 0.816 |
| PLT (103/µL) | 267 (232–323) | 248 (209–291) | 0.027 |
| White blood cells (103/µL) | 9.3 (7.9–11.2) | 8.9 (7.2–11.3) | 0.331 |
| hs-CRP (mg/L) | 3.4 ± 2.9 | 2.6 ± 1.8 | 0.012 |
| Neutrophil (103/µL) | 6.5 (5.5–8.5) | 5.4 (3.4–6.4) | <0.001 |
| Lymphocyte (103/µL) | 2 (1.5–3) | 2 (2–3) | 0.975 |
| Neutrophil/Lymphocyte ratio (NLR) | 3.2 (1.8–6.3) | 2.7 (1.7–3.7) | 0.008 |
| Platelets/Lymphocyte ratio (PLR) | 124 (97–186) | 119 (94–116) | 0.204 |
| Total thiol (μmol/L) | 278 (236–387) | 432.2 (356.4–534.8) | <0.001 |
| Native thiol (μmol/L) | 258 (214–344) | 384.6 (334.6–462.8) | <0.001 |
| Disulfide (μmol/L) | 16.2 (10.3–23.7) | 22.3 (13.6–33.6) | 0.003 |
| Rentrop Collateral Grades: | Coronary Collateral Circulation | ||
|---|---|---|---|
| Poor (n = 49) | Good (n = 200) | p Value | |
| 0 | 24 | ||
| 1 | 25 | ||
| 2 | 137 | ||
| 3 | 63 | ||
| Position of chronic total occlusion | |||
| Left anterior descending coronary artery | 23 (%46.9) | 98 (%49) | 0.765 |
| Left circumflex coronary artery | 11 (%22.4) | 45 (%22.5) | 0.952 |
| Right coronary artery | 15 (%30.7) | 57 (%28.5) | 0.736 |
| Number of diseased coronary artery | |||
| One-vessel disease | 14 (%28.6) | 59 (%29.5) | 0.811 |
| Two-vessel disease | 18 (%36.7) | 68 (%34) | 0.797 |
| Three-vessel disease | 17 (%34.7) | 73 (%36,5) | 0.812 |
| SYNTAX score | 19.7 ± 4.5 | 20.3 ± 5.3 | 0.645 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value | |
| DM | 2.594 | 1.336–5.038 | 0.005 | 2.671 | 1.238–5.761 | 0.012 |
| Age | 1.039 | 1.007–1.073 | 0.018 | |||
| PLT | 1.003 | 0.999–1.000 | 0.097 | |||
| Hs CRP | 1.182 | 1.033–1.351 | 0.015 | |||
| NLR | 1.081 | 1.002–1.166 | 0.045 | |||
| Total Thyol | 1.011 | 1.007–1.015 | <0.001 | 1.012 | 1.008–1.017 | <0.001 |
| Disulfide | 0.961 | 0.935–0.989 | 0.006 | 1.022 | 1.000–1.044 | 0.044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doğan, Y.; Yilmaz, Y.; Kelesoğlu, S.; Calapkorur, B.; Neşelioglu, S.; Erel, Ö.; Kalay, N. Are Thiols Useful Biomarkers for Coronary Collateral Circulation in Patients with Stable Coronary Artery Disease? J. Clin. Med. 2023, 12, 6361. https://doi.org/10.3390/jcm12196361
Doğan Y, Yilmaz Y, Kelesoğlu S, Calapkorur B, Neşelioglu S, Erel Ö, Kalay N. Are Thiols Useful Biomarkers for Coronary Collateral Circulation in Patients with Stable Coronary Artery Disease? Journal of Clinical Medicine. 2023; 12(19):6361. https://doi.org/10.3390/jcm12196361
Chicago/Turabian StyleDoğan, Yasemin, Yücel Yilmaz, Saban Kelesoğlu, Bekir Calapkorur, Salim Neşelioglu, Özcan Erel, and Nihat Kalay. 2023. "Are Thiols Useful Biomarkers for Coronary Collateral Circulation in Patients with Stable Coronary Artery Disease?" Journal of Clinical Medicine 12, no. 19: 6361. https://doi.org/10.3390/jcm12196361
APA StyleDoğan, Y., Yilmaz, Y., Kelesoğlu, S., Calapkorur, B., Neşelioglu, S., Erel, Ö., & Kalay, N. (2023). Are Thiols Useful Biomarkers for Coronary Collateral Circulation in Patients with Stable Coronary Artery Disease? Journal of Clinical Medicine, 12(19), 6361. https://doi.org/10.3390/jcm12196361