Transcultural Adaptation and Psychometric Validation of the Spanish Version of the Pain Attitudes and Beliefs Scale for Physiotherapists

 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
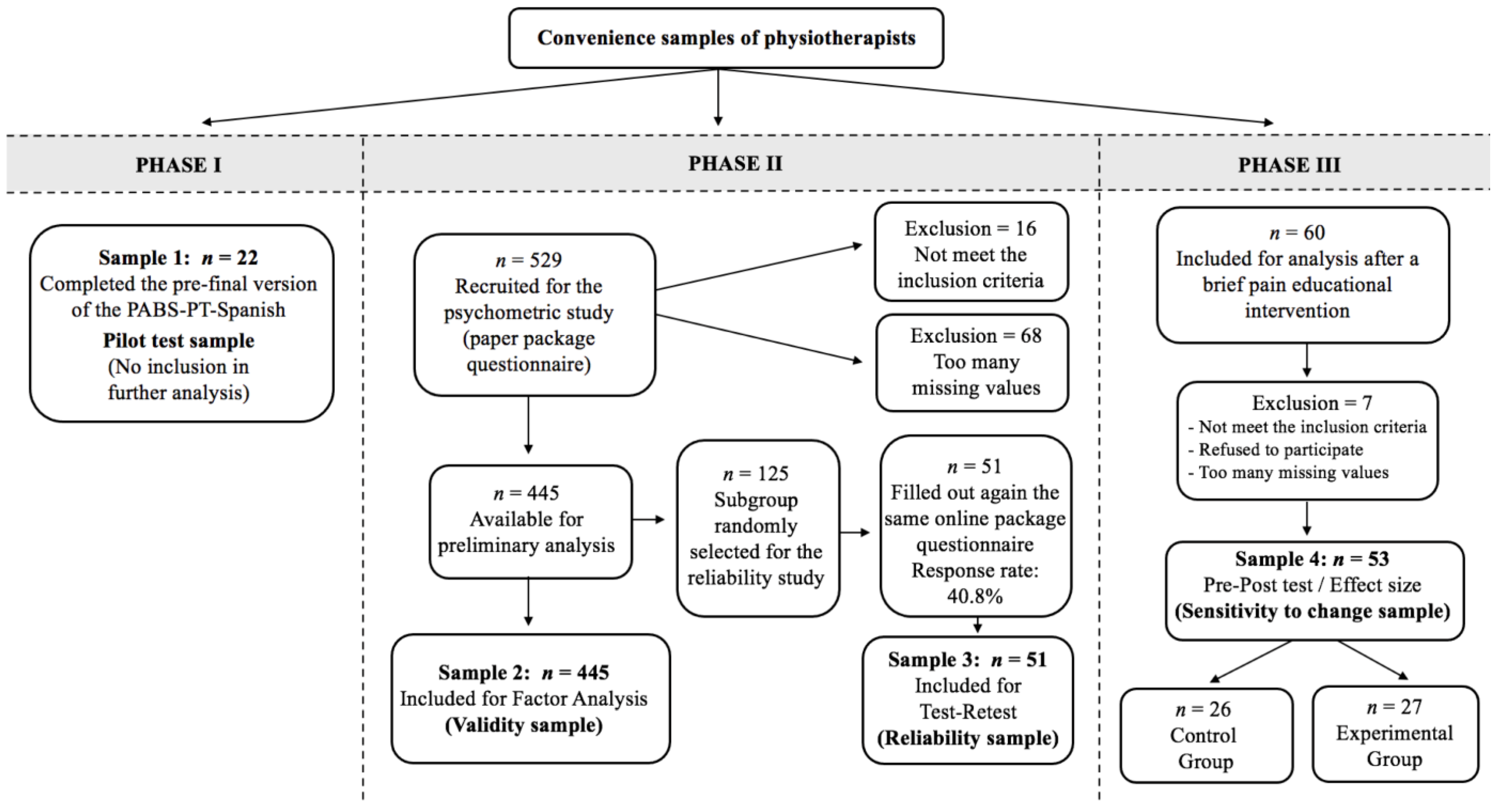
2.1. Participants and Design
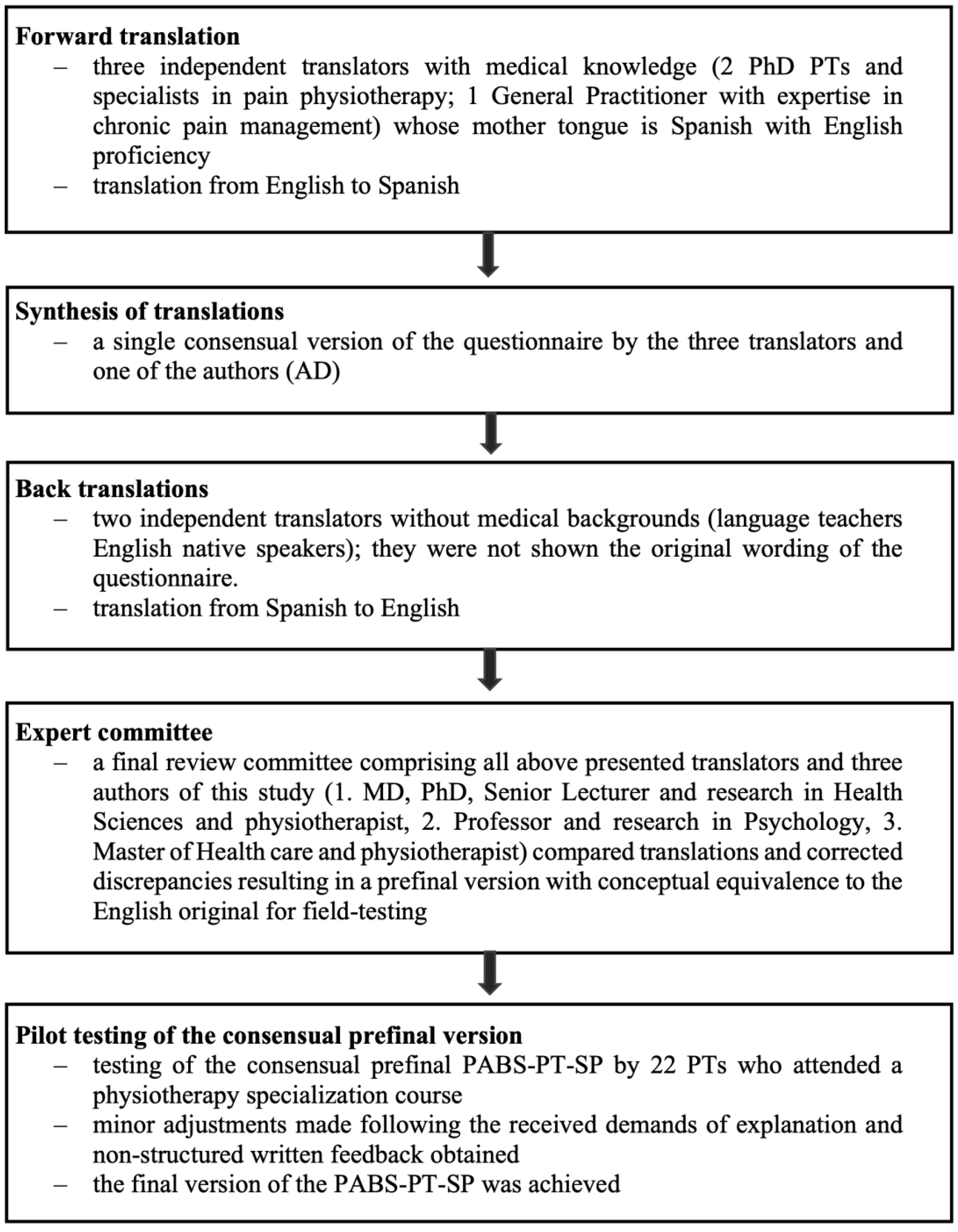
2.1.1. Phase I: Translation and Cross-Cultural Adaptation
2.1.2. Phase II: Investigation of Psychometric Properties
2.1.3. Phase III: Investigation of Sensitivity to Change
2.2. Outcome Measures
2.2.1. Sociodemographic Data
2.2.2. Pain Attitudes and Beliefs Scale for Physiotherapists
2.2.3. Health Care Providers’ Pain and Impairment Relationship Scale
2.2.4. Revised Neurophysiology Pain Questionnaire (R-NPQ)
2.3. Statistical Analyses
3. Results
3.1. Demographic Characteristics and Responses of the Instruments
3.2. Translation and Cultural Adaptation
3.3. Construct Validity
3.4. Internal Consistency
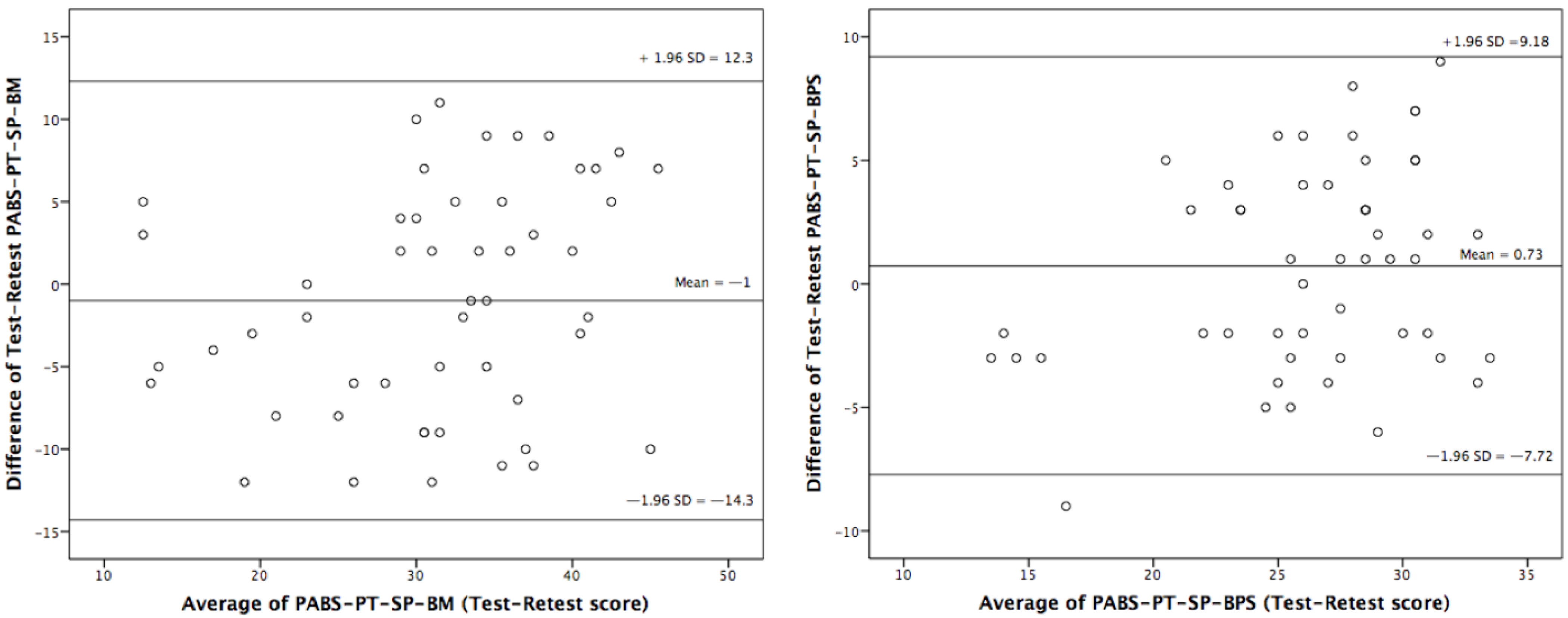
3.5. Test–Retest Reliability and Interpretability
3.6. Concurrent Validity
3.7. Discriminative Ability (Known Groups Validity)
3.8. Sensitivity to Change and Responsiveness
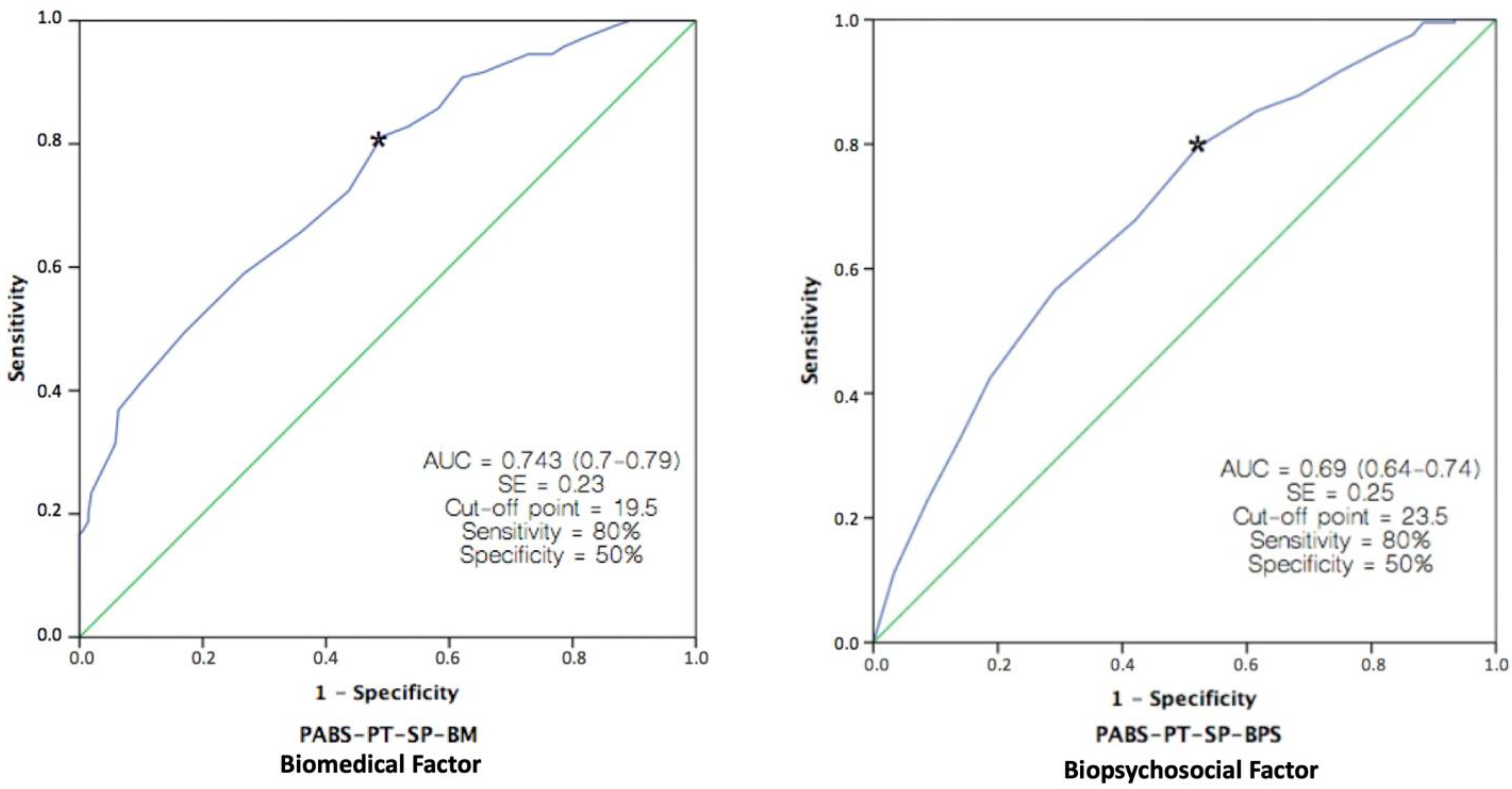
3.9. Predictive Ability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maniadakis, N.; Gray, A. The Economic Burden of Back Pain in the UK. Pain 2000, 84, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, S.; Caro, J.; Haldeman, S. A Systematic Review of Low Back Pain Cost of Illness Studies in the United States and Internationally. Spine J. 2008, 8, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of Low Back Pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, W.; Sato, M.; Nagasaka, Y.; Vietri, J. The Economic and Humanistic Costs of Chronic Lower back pain in Japan. Clin. Outcomes Res. 2017, 9, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 Study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Mattiuzzi, C.; Lippi, G.; Bovo, C. Current Epidemiology of Low Back Pain. J. Hosp. Manag. Health Policy 2020, 4. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Hernández-Barrera, V.; Alonso-Blanco, C.; Palacios-Ceña, D.; Carrasco-Garrido, P.; Jiménez-Sánchez, S.; Jiménez-García, R. Prevalence of Neck and Low Back Pain in Community-Dwelling Adults in Spain: A Population-Based National Study. Spine 2011, 36, E213–E219. [Google Scholar] [CrossRef]
- Wang, L.; Ye, H.; Li, Z.; Lu, C.; Ye, J.; Liao, M.; Chen, X. Epidemiological Trends of Low Back Pain at the Global, Regional, and National Levels. Eur. Spine J. 2022, 31, 953–962. [Google Scholar] [CrossRef]
- Waddell, G. The Back Pain Revolution, 2nd ed.; Churchill Livingstone: Edinburgh, UK, 2004. [Google Scholar]
- Hill, J.C.; Fritz, J.M. Psychosocial Influences on Low Back Pain, Disability, and Response to Treatment. Phys. Ther. 2011, 91, 712–721. [Google Scholar] [CrossRef]
- Andronis, L.; Kinghorn, P.; Qiao, S.; Whitehurst, D.G.T.; Durrell, S.; McLeod, H. Cost-Effectiveness of Non-Invasive and Non-Pharmacological Interventions for Low Back Pain: A Systematic Literature Review. Appl. Health Econ. Health Policy 2017, 15, 173–201. [Google Scholar] [CrossRef]
- Roe, C. Attitude and Belief of Pain-Therapists Are Important When Trying to Help Chronic Pain Patients: The Norwegian Version of the Pain Attitudes and Beliefs Scale (PABS) Improved by Rasch Analysis. Scand. J. Pain 2016, 13, 140–141. [Google Scholar] [CrossRef] [PubMed]
- Zusman, M. Belief Reinforcement: One Reason Why Costs for Low Back Pain Have Not Decreased. J. Multidiscip. Healthc. 2013, 6, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Richmond, H.; Hall, A.M.; Copsey, B.; Hansen, Z.; Williamson, E.; Hoxey-Thomas, N.; Cooper, Z.; Lamb, S.E. The Effectiveness of Cognitive Behavioural Treatment for Non-Specific Low Back Pain: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0134192. [Google Scholar] [CrossRef]
- Magalhaes, M.O.; Costa, L.O.P.; Ferreira, M.L.; Machado, L.A.C. Clinimetric Testing of Two Instruments That Measure Attitudes and Beliefs of Health Care Providers about Chronic Low Back Pain. Rev. Bras. Fisioter 2011, 15, 249–256. [Google Scholar] [PubMed]
- Rainville, J.; Bagnall, D.; Phalen, L. Health Care Providers’ Attitudes and Beliefs about Functional Impairments and Chronic Back Pain. Clin. J. Pain 1995, 11, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Darlow, B.; Fullen, B.M.; Dean, S.; Hurley, D.A.; Baxter, G.D.; Dowell, A. The Association between Health Care Professional Attitudes and Beliefs and the Attitudes and Beliefs, Clinical Management, and Outcomes of Patients with Low Back Pain: A Systematic Review. Eur. J. Pain 2012, 16, 3–17. [Google Scholar] [CrossRef]
- Simmonds, M.J.; Derghazarian, T.; Vlaeyen, J.W.S. Physiotherapists’ Knowledge, Attitudes, and Intolerance of Uncertainty Influence Decision Making in Low Back Pain. Clin. J. Pain 2012, 28, 467–474. [Google Scholar] [CrossRef]
- Linton, S.J.; Maher, C.G.; Van Zundert, J. Low Back Pain: Basic Mechanisms, Treatment, and Management. In Pain 2012 Refresher Courses 14th World Congress on Pain; Tracey, I., Ed.; IASP Press: Seattle, WA, USA, 2012; pp. 195–206. [Google Scholar]
- Houben, R.M.A.; Gijsen, A.; Peterson, J.; de Jong, P.J.; Vlaeyen, J.W.S. Do Health Care Providers’ Attitudes towards Back Pain Predict Their Treatment Recommendations? Differential Predictive Validity of Implicit and Explicit Attitude Measures. Pain 2005, 114, 491–498. [Google Scholar] [CrossRef]
- Bishop, A.; Foster, N.E.; Thomas, E.; Hay, E.M. How Does the Self-Reported Clinical Management of Patients with Low Back Pain Relate to the Attitudes and Beliefs of Health Care Practitioners? A Survey of UK General Practitioners and Physiotherapists. Pain 2008, 135, 187–195. [Google Scholar] [CrossRef]
- Ostelo, R.W.J.G.; Vlaeyen, J.W.S. Attitudes and Beliefs of Health Care Providers: Extending the Fear-Avoidance Model. Pain 2008, 135, 3–4. [Google Scholar] [CrossRef]
- Domenech, J.; Sanchez-Zuriaga, D.; Segura-Orti, E.; Espejo-Tort, B.; Lison, J.F. Impact of Biomedical and Biopsychosocial Training Sessions on the Attitudes, Beliefs, and Recommendations of Health Care Providers about Low Back Pain: A Randomised Clinical Trial. Pain 2011, 152, 2557–2563. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Linton, S.J. Are We “Fear-Avoidant”? Pain 2006, 124, 240–241. [Google Scholar] [CrossRef] [PubMed]
- Von Korff, M.; Barlow, W.; Cherkin, D.; Deyo, R.A. Effects of Practice Style in Managing Back Pain. Ann. Intern. Med. 1994, 121, 187–195. [Google Scholar] [CrossRef]
- Beales, D.; Kendell, M.; Chang, R.P.; Håmsø, M.; Gregory, L.; Richardson, K.; O’Sullivan, P. Association between the 10 Item Örebro Musculoskeletal Pain Screening Questionnaire and Physiotherapists’ Perception of the Contribution of Biopsychosocial Factors in Patients with Musculoskeletal Pain. Man. Ther. 2016, 23, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Ostelo, R.W.J.G.; Stomp-van den Berg, S.G.M.; Vlaeyen, J.W.S.; Wolters, P.M.J.C.; de Vet, H.C.W. Health Care Provider’s Attitudes and Beliefs towards Chronic Low Back Pain: The Development of a Questionnaire. Man. Ther. 2003, 8, 214–222. [Google Scholar] [CrossRef]
- Bishop, A.; Thomas, E.; Foster, N.E. Health Care Practitioners’ Attitudes and Beliefs about Low Back Pain: A Systematic Search and Critical Review of Available Measurement Tools. Pain 2007, 132, 91–101. [Google Scholar] [CrossRef]
- Brunner, E.; Meichtry, A.; Kieran, O.; Baldew, S.; Dankaerts, W.; Probst, M. Factor Structure of the German Version of the Pain Attitudes and Beliefs Scale for Physiotherapists. Physiother. Theory Pr. 2018, 35, 995–1003. [Google Scholar] [CrossRef]
- Houben, R.M.A.; Ostelo, R.W.J.G.; Vlaeyen, J.W.S.; Wolters, P.M.J.C.; Peters, M.; Stomp-van den Berg, S.G.M. Health Care Providers’ Orientations towards Common Low Back Pain Predict Perceived Harmfulness of Physical Activities and Recommendations Regarding Return to Normal Activity. Eur. J. Pain 2005, 9, 173–183. [Google Scholar] [CrossRef]
- Laekeman, M.-A.; Sitter, H.; Basler, H.D. The Pain Attitudes and Beliefs Scale for Physiotherapists: Psychometric Properties of the German Version. Clin. Rehabil. 2008, 22, 564–575. [Google Scholar] [CrossRef]
- Dalkilinc, M.; Cirak, Y.; Yilmaz, G.D.; Parlak Demir, Y. Validity and Reliability of Turkish Version of the Pain Attitudes and Beliefs Scale for Physiotherapists. Physiother. Theory Pr. 2015, 31, 186–193. [Google Scholar] [CrossRef]
- Eland, N.D.; Kvale, A.; Ostelo, R.W.J.G.; Strand, L.I. The Pain Attitudes and Beliefs Scale for Physiotherapists: Dimensionality and Internal Consistency of the Norwegian Version. Physiother. Res. Int. 2017, 22, e1670. [Google Scholar] [CrossRef]
- Watson, P.J.; Bowey, J.; Purcell-Jones, G.; Gales, T. General Practitioner Sickness Absence Certification for Low Back Pain Is Not Directly Associated with Beliefs about Back Pain. Eur. J. Pain 2008, 12, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Fullen, B.M.; Baxter, G.D.; Doody, C.; Daly, L.E.; Hurley, D.A. General Practitioners’ Attitudes and Beliefs Regarding the Management of Chronic Low Back Pain in Ireland: A Cross-Sectional National Survey. Clin. J. Pain 2011, 27, 542–549. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Prisen, C.A.; Patrick, D.L.; Aloso, J.; Bouter, L.M.; de Vet, H.C.; Terwee, C.B. COSMIN Study Design Checklist for Patient-Reported Outcome Measurement Instruments. Qual Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Lai, J.; Mokkink, L.B.; Terwee, C.B. COSMIN Reporting Guideline for Studies on Measurement Properties of Patient-Reported Outcome Measures. Qual. Life Res. 2021, 30, 2197–2218. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Catley, M.J.; O’Connell, N.E.; Moseley, G.L. How Good Is the Neurophysiology of Pain Questionnaire? A Rasch Analysis of Psychometric Properties. J. Pain 2013, 14, 818–827. [Google Scholar] [CrossRef]
- Mutsaers, J.-H.A.M.; Pool-Goudzwaard, A.L.; Ostelo, R.W.J.G.; Peters, R.; Koes, B.W.; Verhagen, A.P. The Psychometric Properties of the PABS-PT in Neck Pain Patients: A Validation Study. Man. Ther. 2014, 19, 208–214. [Google Scholar] [CrossRef]
- Clarke, C.L.; Ryan, C.G.; Martin, D.J. Pain Neurophysiology Education for the Management of Individuals with Chronic Low Back Pain: Systematic Review and Meta-Analysis. Man. Ther. 2011, 16, 544–549. [Google Scholar] [CrossRef]
- Mutsaers, J.-H.A.M.; Peters, R.; Pool-Goudzwaard, A.L.; Koes, B.W.; Verhagen, A.P. Psychometric Properties of the Pain Attitudes and Beliefs Scale for Physiotherapists: A Systematic Review. Man. Ther. 2016, 17, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Houben, R.M.A.; Vlaeyen, J.W.S.; Peters, M.; Ostelo, R.W.J.G.; Wolters, P.M.J.C.; Stomp-van den Berg, S.G.M. Health Care Providers’ Attitudes and Beliefs towards Common Low Back Pain: Factor Structure and Psychometric Properties of the HC-PAIRS. Clin. J. Pain 2004, 20, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Domenech, J.; Segura-Orti, E.; Lison, J.F.; Espejo-Tort, B.; Sanchez-Zuriaga, D. Psychometric Properties and Factor Structure of the Spanish Version of the HC-PAIRS Questionnaire. Eur. Spine J. 2013, 22, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Moseley, L. Unraveling the Barriers to Reconceptualization of the Problem in Chronic Pain: The Actual and Perceived Ability of Patients and Health Professionals to Understand the Neurophysiology. J. Pain Off. J. Am. Pain Soc. 2003, 4, 184–189. [Google Scholar] [CrossRef]
- Moseley, G.L. Evidence for a Direct Relationship between Cognitive and Physical Change during an Education Intervention in People with Chronic Low Back Pain. Eur. J. Pain 2004, 8, 39–45. [Google Scholar] [CrossRef]
- Meeus, M.; Nijs, J.; Van Oosterwijck, J.; Van Alsenoy, V.; Truijen, S. Pain Physiology Education Improves Pain Beliefs in Patients with Chronic Fatigue Syndrome Compared with Pacing and Self-Management Education: A Double-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2010, 91, 1153–1159. [Google Scholar] [CrossRef]
- Louw, A.; Puentedura, E.J. Therapeutic Neuroscience Education, Pain, Physiotherapy and the Pain Neuromatrix. Int. J. Health Sci. (IJHS) 2014, 2, 33–45. [Google Scholar] [CrossRef]
- Lee, H.; McAuley, J.H.; Hubscher, M.; Kamper, S.J.; Traeger, A.C.; Moseley, G.L. Does Changing Pain-Related Knowledge Reduce Pain and Improve Function through Changes in Catastrophizing? Pain 2016, 157, 922–930. [Google Scholar] [CrossRef]
- Torres-Lacomba, M.; Navarro-Brazález, B.; Bailón-Cerezo, J.; Vergara-Pérez, F.; de la Rosa-Díaz, I.; Prieto-Gómez, V. Assessment Tools of Patient Competences: The Spanish Version of the R-NPQ and Three Practical Cases in Women with Breast Cancer and Persistent Pain. Int. J. Environ. Res. Public Health 2021, 18, 4463. [Google Scholar] [CrossRef]
- de Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011; ISBN 9780521118200. [Google Scholar]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 2015; ISBN 9780199685219. [Google Scholar]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 2nd ed.; Prentice Hall Health: Upper Saddle River, NJ, USA, 2015. [Google Scholar]
- Weir, J.P. Quantifying Test-Retest Reliability Using the Intraclass Correlation Coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Haley, S.M.; Fragala-Pinkham, M.A. Interpreting Change Scores of Tests and Measures Used in Physical Therapy. Phys. Ther. 2006, 86, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN Checklist for Assessing the Methodological Quality of Studies on Measurement Properties of Health Status Measurement Instruments: An International Delphi Study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN Study Reached International Consensus on Taxonomy, Terminology, and Definitions of Measurement Properties for Health-Related Patient-Reported Outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Prinsen, C.A.C.; Bouter, L.M.; de Vet, H.C.W.; Terwee, C.B. The COnsensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN) and How to Select an Outcome Measurement Instrument. Braz J. Phys. Ther. 2016, 20, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.B.; Adachi, J.D.; Beattie, K.A.; Lau, A.; MacDermid, J.C. Determining Known-Group Validity and Test-Retest Reliability in the PEQ (Personalized Exercise Questionnaire). BMC Musculoskelet. Disord. 2019, 20, 373. [Google Scholar] [CrossRef]
- Mikamo, Y.; Takasaki, H. Pain Neurophysiology Knowledge Enhances Attitudes toward Biopsychosocial Management of Low Back Pain among Japanese Physical Therapists. Prog. Rehabil. Med. 2021, 6, 20210039. [Google Scholar] [CrossRef]
- Rufa, A.; Dolphin, M.; Adams, K.; Brooks, G. Factors Associated with the Low Back Pain-Related Attitudes and Beliefs of Physical Therapists. Musculoskelet. Sci. Pr. 2022, 58, 102518. [Google Scholar] [CrossRef]
- Brydges, C.R. Effect Size Guidelines, Sample Size Calculations, and Statistical Power in Gerontology. Innov. Aging 2019, 3, igz036. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The Efficacy of Pain Neuroscience Education on Musculoskeletal Pain: A Systematic Review of the Literature. Physiother. Theory Pr. 2016, 32, 332–355. [Google Scholar] [CrossRef] [PubMed]
- Jho, H.J.; Myung, S.-K.; Chang, Y.-J.; Kim, D.-H.; Ko, D.H. Efficacy of Pain Education in Cancer Patients: A Meta-Analysis of Randomized Controlled Trials. Support. Care Cancer 2013, 21, 1963–1971. [Google Scholar] [CrossRef]
- Davidson, M.; Keating, J. Patient-Reported Outcome Measures (PROMs): How Should I Interpret Reports of Measurement Properties? A Practical Guide for Clinicians and Researchers Who Are Not Biostatisticians. Br. J. Sports Med. 2014, 48, 792–796. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Zweig, M.H.; Campbell, G. Receiver-Operating Characteristic (ROC) Plots: A Fundamental Evaluation Tool in Clinical Medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- Gacto-Sánchez, M.; Lozano-Meca, J.A.; Montilla-Herrador, J. The Pain Attitudes and Beliefs Scale for Physiotherapists: Development and Psychometric Assessment of the Spanish Version among Physiotherapy Students. Physiother. Theory Pr. 2023, 39, 561–577. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández-Baeza, A.; Tomás-Marco, I. El Análisis Factorial Exploratorio de Los Ítems: Una Guía Práctica, Revisada y Actualizada. An. Psicol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- McDonald, R.P. Test Theory: A Unified Treatment; Erlbaum: Mahwah, NJ, USA, 1999; ISBN 0805830758. [Google Scholar]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, K.; O’Sullivan, P.; O’Sullivan, L.; Dankaerts, W. Back Pain Beliefs among Physiotherapists Are More Positive after Biopsychosocially Orientated Workshops. Physiother. Pr. Res. 2013, 34, 37–45. [Google Scholar] [CrossRef]
- Eland, N.D.; Kvåle, A.; Ostelo, R.W.J.G.; de Vet, H.C.W.; Strand, L.I. Discriminative Validity of the Pain Attitudes and Beliefs Scale for Physical Therapists. Phys. Ther. 2019, 99, 339–353. [Google Scholar] [CrossRef]
- Overmeer, T.; Boersma, K.; Main, C.J.; Linton, S.J. Do Physical Therapists Change Their Beliefs, Attitudes, Knowledge, Skills and Behaviour after a Biopsychosocially Orientated University Course? J. Eval. Clin. Pr. 2009, 15, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Vonk, F.; Pool, J.J.M.; Ostelo, R.W.J.G.; Verhagen, A.P. Physiotherapists’ Treatment Approach towards Neck Pain and the Influence of a Behavioural Graded Activity Training: An Exploratory Study. Man. Ther. 2009, 14, 131–137. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Values |
|---|---|
| Female, n (%) | 267 (60) |
| Age (years), mean (SD, range) | 30.1 (6.7, 21–56) |
| Years of experience, mean (SD, range) | 7.2 (6.5, 1–33) |
| Clinical practice situation, n (%) | |
| Public | 85 (19.1) |
| Private | 234 (52.6) |
| Freelance | 105 (23.6) |
| Unemployed | 21 (4.7) |
| Clinical experience on LBP in the last six months, n (%) | |
| Frequently | 265 (59.5) |
| Occasionally | 180 (42.5) |
| Specific pain education, n (%) | 189 (42.4) |
| HC-PAIRS, mean (SD) | 57.5 (12.1) |
| PABS-PT-SP-BM, mean (SD) | 21.6 (7.1) |
| PABS-PT-SP-BPS, mean (SD) | 24.1 (4.4) |
| R-NPQ, mean (SD) | 6.8 (2.6) |
| N° | Item | Mean (SD) | Factor | F1 | F2 |
|---|---|---|---|---|---|
| 1 | Back pain sufferers should refrain from all physical activity in order to avoid injury. | 1.9 (1.2) | E (B) | ||
| 2 | Good posture prevents back pain. | 4.2 (1.2) | E (B) | ||
| 3 | Knowledge of the tissue damage is not necessary for effective therapy. | 2.5 (1.4) | E (B) | ||
| 4 | Reduction of daily physical exertion is a significant factor in treating back pain. | 2.9 (1.4) | E (B) | ||
| 5 | Not enough effort is made to find the underlying organic causes of back pain. | 4.2 (1.3) | E (B) | ||
| 6 | Mental stress can cause back pain even in the absence of tissue damage. | 4.8 (1.4) | 2 | 0.771 | |
| 7 | The cause of back pain is unknown. | 3.4 (1.4) | E (B) | ||
| 8 | Unilateral physical stress is not a cause of back pain. | 3.2 (0.9) | E (B) | ||
| 9 | Patients who have suffered chronic low back pain should avoid activities that stress the back. | 3.7 (1.5) | 1 | 0.614 | |
| 10 | Pain is a nociceptive stimulus, indicating tissue damage. | 3.3 (1.6) | 1 | 0.621 | |
| 11 | A patient suffering from severe low back pain will benefit from physical exercise. | 4.8 (1.1) | 2 | 0.701 | |
| 12 | Functional limitations associated with back pain are the result of psychosocial factors. | 3.8 (1.1) | E (C) | ||
| 13 | The best advice for low back pain is: ‘Take car’ and ‘Make no unnecessary movements’. | 2.6 (1.5) | 1 | 0.772 | |
| 14 | Patients with back pain should preferably practice only pain-free movements. | 3.5 (1.3) | E (B) | ||
| 15 | Back pain indicates that there is something dangerously wrong with the back. | 3.0 (1.4) | E (C) | ||
| 16 | The way patients view their pain influences the progress of the symptoms. | 4.7 (1.3) | 2 | 0.529 | |
| 17 | Therapy may have been successful even if the pain remains. | 3.5 (1.4) | E (B) | ||
| 18 | Therapy can completely alleviate the functional symptoms caused by back pain. | 4.1 (1.3) | E (B) | ||
| 19 | If ADL activities cause more back pain, this is not dangerous. | 2.4 (1.1) | E (B) | ||
| 20 | Low back pain indicates the presence of organic injury. | 2.8 (1.4) | 1 | 0.738 | |
| 21 | Sports should not be recommended for patients with back pain. | 2.1 (1.2) | E (A) | ||
| 22 | If back pain increases in severity, I immediately adjust the intensity of my treatment accordingly. | 4.2 (1.4) | E (B) | ||
| 23 | If therapy does not result in a reduction in back pain, there is a high risk of severe restrictions in the long term. | 3.5 (1.3) | E (B) | ||
| 24 | Pain reduction is a precondition for the restoration of normal functioning. | 5.0 (1.2) | E (A) | ||
| 25 | Increased pain indicates new tissue damage or the spread of existing damage. | 2.9 (1.2) | 1 | 0.677 | |
| 26 | It is the task of the physiotherapist to remove the cause of back pain. | 3.8 (1.4) | 1 | 0.519 | |
| 27 | There is no effective treatment to eliminate back pain. | 3.0 (1.3) | E (B) | ||
| 28 | TENS and/or back braces support functional recovery. | 3.5 (1.3) | E (B) | ||
| 29 | Even if the pain has worsened, the intensity of the next treatment can be increased. | 2.7 (1.1) | E (B) | ||
| 30 | If patients complain of pain during exercise, I worry that damage is being caused. | 3.3 (1.4) | 1 | 0.661 | |
| 31 | The severity of tissue damage determines the level of pain. | 3.3 (1.4) | 1 | 0.731 | |
| 32 | A rapid resumption of daily activities is an important goal of the treatment. | 5.0 (0.8) | E (A) | ||
| 33 | Learning to cope with stress promotes recovery from low back pain. | 4.8 (1.0) | 2 | 0.649 | |
| 34 | Exercises that may be back straining should not be avoided during the treatment. | 4.4 (1.3) | 2 | 0.547 | |
| 35 | In the long run, patients with back pain have a higher risk of developing spinal impairments. | 3.1 (1.3) | E (B) | ||
| 36 | In back pain, imaging tests are unnecessary. | 3.4 (0.9) | E (B) |
| t-Test Paired | SRM [95% CI] | r | R2 | ||||
|---|---|---|---|---|---|---|---|
| Control group (n = 26) | BM factor | No statistical significance | — | Correlation between BM factor ---- BPS factor | Time 1 (BASELINE) | −0.47 * | 0.22 |
| BPS factor | No statistical significance | — | Time 2 (POST-INTERVENTION) | −0.45 * | 0.20 | ||
| Experimental group (n = 27) | BM factor | t = 3.231; df = 26 p-value < 0.05 * | 0.53 [0.22, 0.73] | Time 1 (BASELINE) | −0.44 * | 0.19 | |
| BPS factor | t = −3.567; df = 26 p-value < 0.001 ** | 0.76 [0.39, 0.98] | Time 2 (POST-INTERVENTION) | −0.68 ** | 0.46 |
| Factor 1 (Biomedical) | Factor 2 (Biopsychosocial) | |||||
|---|---|---|---|---|---|---|
| Number of Items | Cronbach’s Alpha | Variance Explained (%) | Number of Items | Cronbach’s Alpha | Variance Explained (%) | |
| Ostelo et al., 2003 [27] | 14 | 0.84 | 25.2 | 6 | 0.54 | 8.2 |
| Houben et al., 2005 [30] | 10 | 0.73 | 23.4 | 9 | 0.68 | 10 |
| Laekeman et al., 2008 [31] | 10 | 0.77 | 21.5 | 4 | 0.58 | 3.6 |
| Watson et al., 2008 * [34] | 12 | 0,.79 | - | 5 | 0.60 | - |
| Magalhaes et al., 2011 [15] | 10 | 0.74 | - | 9 | 0.67 | - |
| Dalkilinc et al., 2014 [32] | 7 | 0.72 | 24.5 | 6 | 0.59 | 14 |
| Mutsaers et al., 2014 ** [41] | 7 | 0.75 | - | 8 | 0.73 | - |
| Eland et al., 2016 [33] | 13 | 0.79 | 18.1 | 6 | 0.57 | 7.1 |
| Gacto-Sánchez et al., 2023 *** [72] | 9 | 0.72 | 49.3 | 7 | 0.71 | 26.5 |
| this work | 8 | 0.86 | 39.4 | 5 | 0.77 | 13.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-Fernández, Á.; Ortega-Martínez, A.R.; Cortés-Pérez, I.; Ibáñez-Vera, A.J.; Obrero-Gaitán, E.; Lomas-Vega, R. Transcultural Adaptation and Psychometric Validation of the Spanish Version of the Pain Attitudes and Beliefs Scale for Physiotherapists. J. Clin. Med. 2023, 12, 6045. https://doi.org/10.3390/jcm12186045
Díaz-Fernández Á, Ortega-Martínez AR, Cortés-Pérez I, Ibáñez-Vera AJ, Obrero-Gaitán E, Lomas-Vega R. Transcultural Adaptation and Psychometric Validation of the Spanish Version of the Pain Attitudes and Beliefs Scale for Physiotherapists. Journal of Clinical Medicine. 2023; 12(18):6045. https://doi.org/10.3390/jcm12186045
Chicago/Turabian StyleDíaz-Fernández, Ángeles, Ana Raquel Ortega-Martínez, Irene Cortés-Pérez, Alfonso Javier Ibáñez-Vera, Esteban Obrero-Gaitán, and Rafael Lomas-Vega. 2023. "Transcultural Adaptation and Psychometric Validation of the Spanish Version of the Pain Attitudes and Beliefs Scale for Physiotherapists" Journal of Clinical Medicine 12, no. 18: 6045. https://doi.org/10.3390/jcm12186045
APA StyleDíaz-Fernández, Á., Ortega-Martínez, A. R., Cortés-Pérez, I., Ibáñez-Vera, A. J., Obrero-Gaitán, E., & Lomas-Vega, R. (2023). Transcultural Adaptation and Psychometric Validation of the Spanish Version of the Pain Attitudes and Beliefs Scale for Physiotherapists. Journal of Clinical Medicine, 12(18), 6045. https://doi.org/10.3390/jcm12186045