
Preventing Rejection of the Kidney Transplant

Abstract
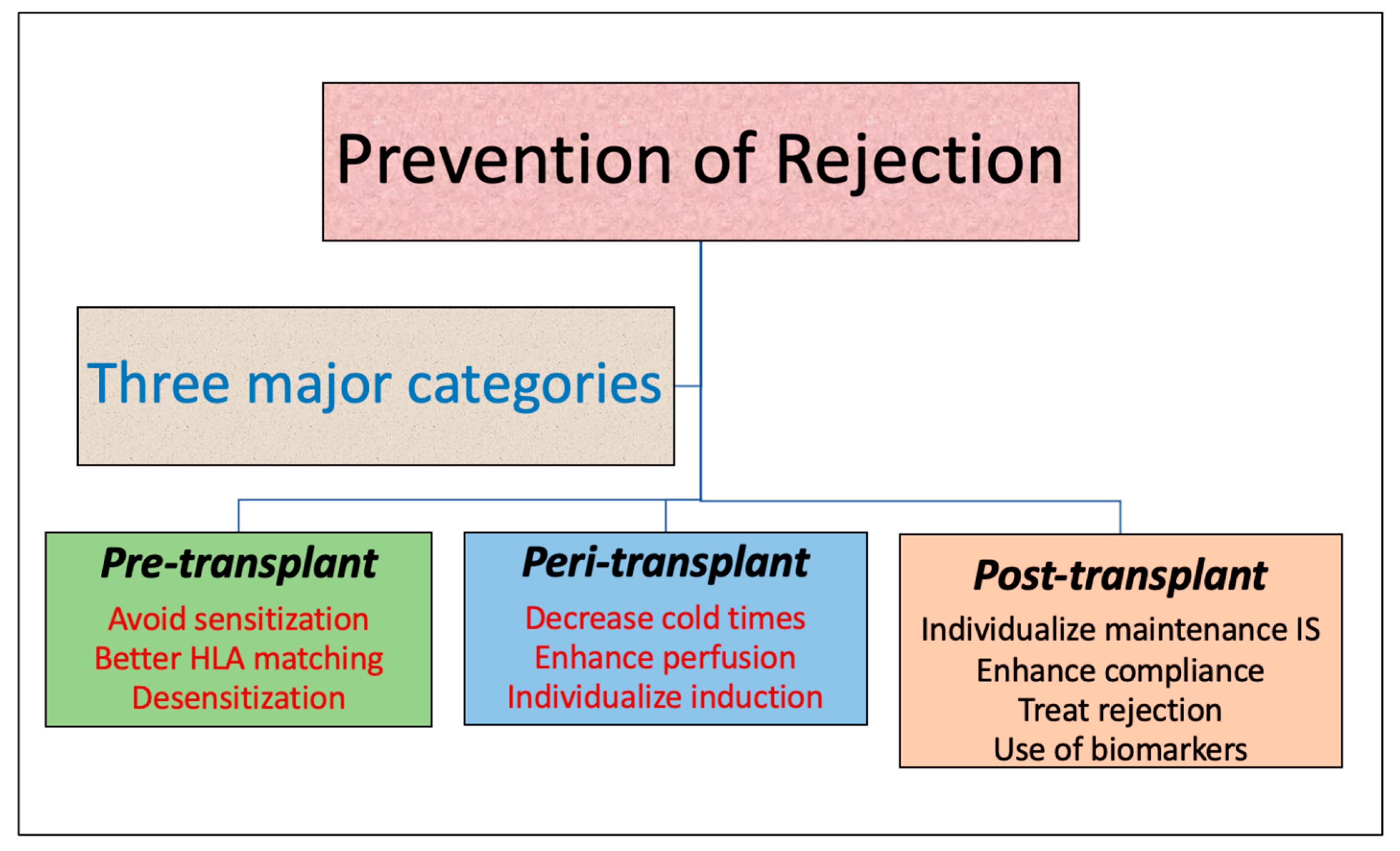
:1. Introduction
2. Pre-Transplant Measures
2.1. Optimization of Donor-Recipient Compatibility: HLA Matching
2.2. Desensitization in HLA-Incompatible Kidney Transplantation
2.3. Role of Non-HLA Mismatches in Transplant Rejection
|
3. Peri-Transplant Measures
3.1. Minimizing Cold-Ischemia Time/Optimizing Perfusion
3.2. Individualizing Induction Immunosuppression
|
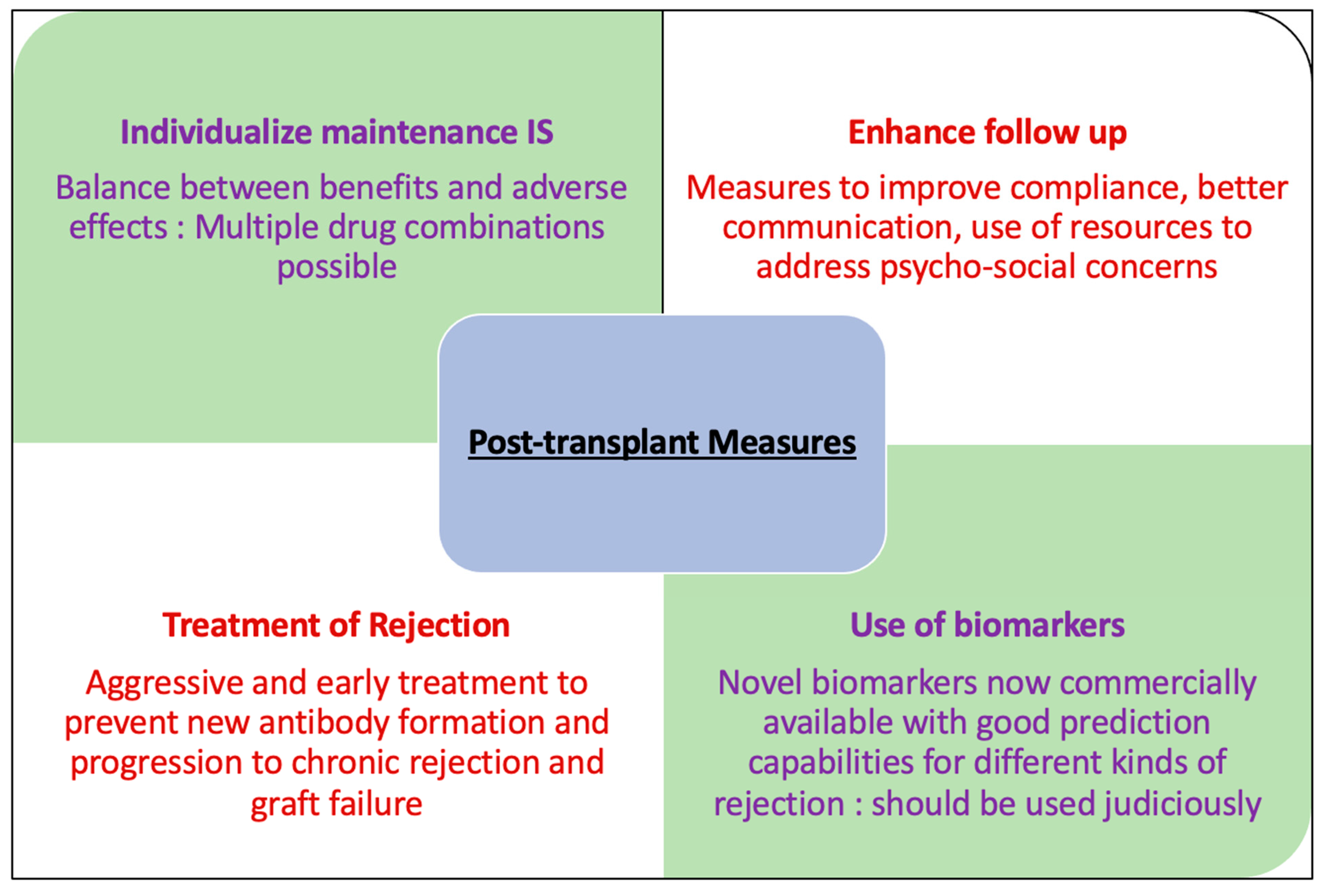
4. Post-Transplant Measures to Prevent Rejection
4.1. Prevention of Cell Mediated Rejection
CNI Free Regimens
4.2. Prevention of Antibody Mediated Rejection
4.3. Minimizing Non-Compliance
4.4. Treatment of Rejection
4.5. Role of Biomarkers
4.6. Emerging Therapies
|
5. Financial Impact, Practical Considerations and Real-World Challenges
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Voronoy, U. Blocking the reticuloendothelial system in man in some forms of mercuric chloride intoxication and the transplantation of the cadaver kidney as a method of treatment for the anuria resulting from the intoxication. Siglo Med. 1937, 97, 296. [Google Scholar]
- Poggio, E.D.; Augustine, J.J.; Arrigain, S.; Brennan, D.C.; Schold, J.D. Long-term kidney transplant graft survival-Making progress when most needed. Am. J. Transplant. 2021, 21, 2824–2832. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Smith, J.M.; Hart, A.; Miller, J.; Skeans, M.A.; Larkin, L.; Robinson, A.; Gauntt, K.; Israni, A.K.; Hirose, R.; et al. OPTN/SRTR 2020 Annual Data Report: Kidney. Am. J. Transplant. 2022, 22 (Suppl. S2), 21–136. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Gheorghian, A.; Axelrod, D.; Kalsekar, A.; L’Italien, G.; Schnitzler, M.A. The implications of acute rejection for allograft survival in contemporary U.S. kidney transplantation. Transplantation 2012, 94, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Chen, J.; Wang, Y.; Zhang, J.; Zhu, Z.; Shou, Z.; Wang, S.; Zhang, P.; Huang, H.; He, Q. Impact of acute rejection episodes on long-term renal allograft survival. Chin. Med. J. 2003, 116, 1741–1745. [Google Scholar]
- Cole, E.H.; Johnston, O.; Rose, C.L.; Gill, J.S. Impact of acute rejection and new-onset diabetes on long-term transplant graft and patient survival. Clin. J. Am. Soc. Nephrol. 2008, 3, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.M.; Mandia-Sampaio, E.L.; de Sandes-Freitas, T.V.; Felipe, C.R.; Park, S.I.; Pinheiro-Machado, P.G.; Garcia, R.; Tedesco-Silva, H., Jr.; Medina-Pestana, J.O. Risk factors associated with graft loss and patient survival after kidney transplantation. Transplant. Proc. 2009, 41, 3667–3670. [Google Scholar] [CrossRef]
- Jalalzadeh, M.; Mousavinasab, N.; Peyrovi, S.; Ghadiani, M.H. The impact of acute rejection in kidney transplantation on long-term allograft and patient outcome. Nephrourol. Mon. 2015, 7, e24439. [Google Scholar] [CrossRef]
- Meier-Kriesche, H.U.; Ojo, A.O.; Hanson, J.A.; Cibrik, D.M.; Punch, J.D.; Leichtman, A.B.; Kaplan, B. Increased impact of acute rejection on chronic allograft failure in recent era. Transplantation 2000, 70, 1098–1100. [Google Scholar] [CrossRef]
- Pallardó Mateu, L.M.; Sancho Calabuig, A.; Capdevila Plaza, L.; Franco Esteve, A. Acute rejection and late renal transplant failure: Risk factors and prognosis. Nephrol. Dial. Transplant. 2004, 19 (Suppl. S3), iii38–iii42. [Google Scholar] [CrossRef]
- Almond, P.S.; Matas, A.; Gillingham, K.; Dunn, D.L.; Payne, W.D.; Gores, P.; Gruessner, R.; Najarian, J.S. Risk factors for chronic rejection in renal allograft recipients. Transplantation 1993, 55, 752–756; Discussion 756–757. [Google Scholar] [CrossRef] [PubMed]
- Basadonna, G.P.; Matas, A.J.; Gillingham, K.J.; Payne, W.D.; Dunn, D.L.; Sutherland, D.E.; Gores, P.F.; Gruessner, R.W.; Najarian, J.S. Early versus late acute renal allograft rejection: Impact on chronic rejection. Transplantation 1993, 55, 993–995. [Google Scholar] [CrossRef] [PubMed]
- Choo, S.Y. The HLA system: Genetics, immunology, clinical testing, and clinical implications. Yonsei Med. J. 2007, 48, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.H.; Chadban, S.J.; Clayton, P.; Budgeon, C.A.; Murray, K.; Campbell, S.B.; Cohney, S.; Russ, G.R.; McDonald, S.P. Human leukocyte antigen mismatches associated with increased risk of rejection, graft failure, and death independent of initial immunosuppression in renal transplant recipients. Clin. Transplant. 2012, 26, E428–E437. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.C.; Opelz, G.; McGarvey, C.J.; Weil, E.J.; Chakkera, H.A. The Risk of Transplant Failure with HLA Mismatch in First Adult Kidney Allografts from Deceased Donors. Transplantation 2016, 100, 1094–1102. [Google Scholar] [CrossRef]
- Lim, W.H.; Chapman, J.R.; Coates, P.T.; Lewis, J.R.; Russ, G.R.; Watson, N.; Holdsworth, R.; Wong, G. HLA-DQ Mismatches and Rejection in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2016, 11, 875–883. [Google Scholar] [CrossRef]
- Kumru Sahin, G.; Unterrainer, C.; Süsal, C. Critical evaluation of a possible role of HLA epitope matching in kidney transplantation. Transplant. Rev. 2020, 34, 100533. [Google Scholar] [CrossRef]
- Senev, A.; Coemans, M.; Lerut, E.; Van Sandt, V.; Kerkhofs, J.; Daniëls, L.; Driessche, M.V.; Compernolle, V.; Sprangers, B.; Van Loon, E.; et al. Eplet Mismatch Load and De Novo Occurrence of Donor-Specific Anti-HLA Antibodies, Rejection, and Graft Failure after Kidney Transplantation: An Observational Cohort Study. J. Am. Soc. Nephrol. 2020, 31, 2193–2204. [Google Scholar] [CrossRef]
- Do Nguyen, H.T.; Wong, G.; Chapman, J.R.; McDonald, S.P.; Coates, P.T.; Watson, N.; Russ, G.R.; D’Orsogna, L.; Lim, W.H. The Association between Broad Antigen HLA Mismatches, Eplet HLA Mismatches and Acute Rejection after Kidney Transplantation. Transplant. Direct 2016, 2, e120. [Google Scholar] [CrossRef]
- Duquesnoy, R.J. HLAMatchmaker: A molecularly based algorithm for histocompatibility determination. I. Description of the algorithm. Hum. Immunol. 2002, 63, 339–352. [Google Scholar] [CrossRef]
- Chipman, V.; Cooper, M.; Thomas, A.G.; Ronin, M.; Lee, B.; Flechner, S.; Leeser, D.; Segev, D.L.; Mandelbrot, D.A.; Lunow-Luke, T.; et al. Motivations and outcomes of compatible living donor-recipient pairs in paired exchange. Am. J. Transplant. 2022, 22, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Tafulo, S.; Malheiro, J.; Dias, L.; Lobato, L.; Ramalhete, L.; Martinho, A.; Bolotinha, C.; Costa, R.; Ivo, M. Improving HLA matching in living donor kidney transplantation using kidney paired exchange program. Transpl. Immunol. 2020, 62, 101317. [Google Scholar] [CrossRef] [PubMed]
- Abbes, S.; Metjian, A.; Gray, A.; Martinu, T.; Snyder, L.; Chen, D.-F.; Ellis, M.; Arepally, G.M.; Onwuemene, O. Human Leukocyte Antigen Sensitization in Solid Organ Transplantation: A Primer on Terminology, Testing, and Clinical Significance for the Apheresis Practitioner. Ther. Apher. Dial. 2017, 21, 441–450. [Google Scholar] [CrossRef]
- Mohan, S.; Palanisamy, A.; Tsapepas, D.; Tanriover, B.; Crew, R.J.; Dube, G.; Ratner, L.E.; Cohen, D.J.; Radhakrishnan, J. Donor-specific antibodies adversely affect kidney allograft outcomes. J. Am. Soc. Nephrol. 2012, 23, 2061–2071. [Google Scholar] [CrossRef] [PubMed]
- Alachkar, N.; Lonze, B.E.; Zachary, A.A.; Holechek, M.J.; Schillinger, K.; Cameron, A.M.; Desai, N.M.; Dagher, N.N.; Segev, D.L.; Montgomery, R.A.; et al. Infusion of high-dose intravenous immunoglobulin fails to lower the strength of human leukocyte antigen antibodies in highly sensitized patients. Transplantation 2012, 94, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Vo, A.A.; Petrozzino, J.; Yeung, K.; Sinha, A.; Kahwaji, J.; Peng, A.; Villicana, R.; Mackowiak, J.; Jordan, S.C. Efficacy, outcomes, and cost-effectiveness of desensitization using IVIG and rituximab. Transplantation 2013, 95, 852–858. [Google Scholar] [CrossRef]
- Magee, C.C.; Felgueiras, J.; Tinckam, K.; Malek, S.; Mah, H.; Tullius, S. Renal transplantation in patients with positive lymphocytotoxicity crossmatches: One center’s experience. Transplantation 2008, 86, 96–103. [Google Scholar] [CrossRef]
- Loupy, A.; Suberbielle-Boissel, C.; Zuber, J.; Anglicheau, D.; Timsit, M.O.; Martinez, F.; Thervet, E.; Bruneval, P.; Charron, D.; Hill, G.S.; et al. Combined posttransplant prophylactic IVIg/anti-CD 20/plasmapheresis in kidney recipients with preformed donor-specific antibodies: A pilot study. Transplantation 2010, 89, 1403–1410. [Google Scholar] [CrossRef]
- Amrouche, L.; Aubert, O.; Suberbielle, C.; Rabant, M.; Van Huyen, J.D.; Martinez, F.; Sberro-Soussan, R.; Scemla, A.; Tinel, C.; Snanoudj, R.; et al. Long-term Outcomes of Kidney Transplantation in Patients with High Levels of Preformed DSA: The Necker High-Risk Transplant Program. Transplantation 2017, 101, 2440–2448. [Google Scholar] [CrossRef]
- Lorenz, M.; Regele, H.; Schillinger, M.; Kletzmayr, J.; Haidbauer, B.; Derfler, K.; Druml, W.; Böhmig, G.A. Peritransplant immunoadsorption: A strategy enabling transplantation in highly sensitized crossmatch-positive cadaveric kidney allograft recipients. Transplantation 2005, 79, 696–701. [Google Scholar] [CrossRef]
- Bagnasco, S.M.; Zachary, A.A.; Racusen, L.C.; Arend, L.J.; Carter-Monroe, N.; Alachkar, N.; Nazarian, S.M.; Lonze, B.E.; Montgomery, R.A.; Kraus, E.S. Time course of pathologic changes in kidney allografts of positive crossmatch HLA-incompatible transplant recipients. Transplantation 2014, 97, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Orandi, B.J.; Luo, X.; Massie, A.B.; Garonzik-Wang, J.M.; Lonze, B.E.; Ahmed, R.; Van Arendonk, K.J.; Stegall, M.D.; Jordan, S.C.; Oberholzer, J.; et al. Survival Benefit with Kidney Transplants from HLA-Incompatible Live Donors. N. Engl. J. Med. 2016, 374, 940–950. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C.; Tyan, D.; Stablein, D.; McIntosh, M.; Rose, S.; Vo, A.; Toyoda, M.; Davis, C.; Shapiro, R.; Adey, D.; et al. Evaluation of intravenous immunoglobulin as an agent to lower allosensitization and improve transplantation in highly sensitized adult patients with end-stage renal disease: Report of the NIH IG02 trial. J. Am. Soc. Nephrol. 2004, 15, 3256–3262. [Google Scholar] [CrossRef] [PubMed]
- Marks, W.H.; Mamode, N.; Montgomery, R.A.; Stegall, M.D.; Ratner, L.E.; Cornell, L.D.; Rowshani, A.T.; Colvin, R.B.; Dain, B.; Boice, J.A.; et al. Safety and efficacy of eculizumab in the prevention of antibody-mediated rejection in living-donor kidney transplant recipients requiring desensitization therapy: A randomized trial. Am. J. Transplant. 2019, 19, 2876–2888. [Google Scholar] [CrossRef]
- Jouve, T.; Daligault, M.; Noble, J.; Terrec, F.; Imerzoukene, F.; Dard, C.; Bardy, B.; Malvezzi, P.; Rostaing, L. Tocilizumab Evaluation in HLA-Desensitization before Kidney Transplantation as an Add-On Therapy to Apheresis: The TETRA Study. J. Clin. Med. 2023, 12, 424. [Google Scholar] [CrossRef]
- Jethwani, P.; Rao, A.; Bow, L.; Menon, M.C. Donor-Recipient Non-HLA Variants, Mismatches and Renal Allograft Outcomes: Evolving Paradigms. Front. Immunol. 2022, 13, 822353. [Google Scholar] [CrossRef]
- Postalcioglu, M.; Kaze, A.D.; Byun, B.C.; Siedlecki, A.; Tullius, S.G.; Milford, E.L.; Paik, J.M.; Abdi, R. Association of Cold Ischemia Time with Acute Renal Transplant Rejection. Transplantation 2018, 102, 1188–1194. [Google Scholar] [CrossRef]
- Sampaio, M.S.; Chopra, B.; Tang, A.; Sureshkumar, K.K. Impact of cold ischemia time on the outcomes of kidneys with Kidney Donor Profile Index ≥85%: Mate kidney analysis—A retrospective study. Transpl. Int. 2018, 31, 729–738. [Google Scholar] [CrossRef]
- Moers, C.; Smits, J.M.; Maathuis, M.-H.J.; Treckmann, J.; van Gelder, F.; Napieralski, B.P.; van Kasterop-Kutz, M.; van der Heide, J.J.H.; Squifflet, J.-P.; van Heurn, E.; et al. Machine perfusion or cold storage in deceased-donor kidney transplantation. N. Engl. J. Med. 2009, 360, 7–19. [Google Scholar] [CrossRef]
- Watson, C.J.E.; Wells, A.C.; Roberts, R.J.; Akoh, J.A.; Friend, P.J.; Akyol, M.; Calder, F.R.; Allen, J.E.; Jones, M.N.; Collett, D.; et al. Cold machine perfusion versus static cold storage of kidneys donated after cardiac death: A UK multicenter randomized controlled trial. Am. J. Transplant. 2010, 10, 1991–1999. [Google Scholar] [CrossRef]
- Helio Tedesco-Silva, J.; Offerni, J.C.M.; Carneiro, V.A.; de Paula, M.I.; Neto, E.D.; Lemos, F.B.C.; Moura, L.R.R.; e Silva Filho, A.P.; de Morais Cunha, M.D.F.; da Silva, E.F.; et al. Randomized Trial of Machine Perfusion Versus Cold Storage in Recipients of Deceased Donor Kidney Transplants with High Incidence of Delayed Graft Function. Transplant. Direct 2017, 3, e155. [Google Scholar] [CrossRef] [PubMed]
- Tingle, S.J.; Figueiredo, R.S.; Moir, J.A.; Goodfellow, M.; Thompson, E.R.; Ibrahim, I.K.; Bates, L.; Talbot, D.; Wilson, C.H. Hypothermic machine perfusion is superior to static cold storage in deceased donor kidney transplantation: A meta-analysis. Clin. Transplant. 2020, 34, e13814. [Google Scholar] [CrossRef] [PubMed]
- Szczech, L.A.; Berlin, J.A.; Aradhye, S.; Grossman, R.A.; Feldman, H.I. Effect of anti-lymphocyte induction therapy on renal allograft survival: A meta-analysis. J. Am. Soc. Nephrol. 1997, 8, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Mourad, G.; Morelon, E.; Noël, C.; Glotz, D.; Lebranchu, Y. The role of Thymoglobulin induction in kidney transplantation: An update. Clin. Transplant. 2012, 26, E450–E464. [Google Scholar] [CrossRef] [PubMed]
- Brennan, D.C.; Daller, J.A.; Lake, K.D.; Cibrik, D.; Del Castillo, D. Rabbit antithymocyte globulin versus basiliximab in renal transplantation. N. Engl. J. Med. 2006, 355, 1967–1977. [Google Scholar] [CrossRef]
- Lü, T.M.; Yang, S.L.; Wu, W.Z.; Tan, J.M. Alemtuzumab induction therapy in highly sensitized kidney transplant recipients. Chin. Med. J. 2011, 124, 664–668. [Google Scholar]
- Thomas, P.G.; Woodside, K.J.; Lappin, J.A.; Vaidya, S.; Rajaraman, S.; Gugliuzza, K.K. Alemtuzumab (Campath 1H) induction with tacrolimus monotherapy is safe for high immunological risk renal transplantation. Transplantation 2007, 83, 1509–1512. [Google Scholar] [CrossRef]
- Hanaway, M.J.; Woodle, E.S.; Mulgaonkar, S.; Peddi, V.R.; Kaufman, D.B.; First, M.R.; Croy, R.; Holman, J. Alemtuzumab induction in renal transplantation. N. Engl. J. Med. 2011, 364, 1909–1919. [Google Scholar] [CrossRef]
- Wang, K.; Xu, X.; Fan, M. Induction therapy of basiliximab versus antithymocyte globulin in renal allograft: A systematic review and meta-analysis. Clin. Exp. Nephrol. 2018, 22, 684–693. [Google Scholar] [CrossRef]
- Hwang, S.D.; Lee, J.H.; Lee, S.W.; Park, K.M.; Kim, J.K.; Kim, M.J.; Song, J.H. Efficacy and Safety of Induction Therapy in Kidney Transplantation: A Network Meta-Analysis. Transplant. Proc. 2018, 50, 987–992. [Google Scholar] [CrossRef]
- Marin, E.P.; Cohen, E.; Malhotra, D. Chapter 2: Immunosuppressive Therapy for Solid Organ Transplantation. In Dermatology and Solid Organ Transplantation, 1st ed.; Zeitouni, N.C., Samie, F.H., Eds.; CRC Press: Boca Raton, FL, USA, 2021; Volume 1, pp. 23–35. [Google Scholar]
- Lentine, K.L.; Smith, J.M.; Miller, J.M.; Bradbrook, K.; Larkin, L.; Weiss, S.; Handarova, D.K.; Temple, K.; Israni, A.K.; Snyder, J.J. OPTN/SRTR 2021 Annual Data Report: Kidney. Am. J. Transplant. 2023, 23, S21–S120. [Google Scholar] [CrossRef]
- Kamal, J.; Doyle, A. Immunosuppression and Kidney Transplantation. Handb. Exp. Pharmacol. 2022, 272, 165–179. [Google Scholar] [PubMed]
- Wang, D.; Matsumoto, R.; You, Y.; Che, T.; Lin, X.Y.; Gaffen, S.L.; Lin, X. CD3/CD28 costimulation-induced NF-kappaB activation is mediated by recruitment of protein kinase C-theta, Bcl10, and IkappaB kinase beta to the immunological synapse through CARMA1. Mol. Cell. Biol. 2004, 24, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Arriens, C.; Polyakova, S.; Adzerikho, I.; Randhawa, S.; Solomons, N. OP0277 Aurora Phase 3 Study demonstrates Voclosporin statistical superiority over standard of care in Lupus Nephritis (LN). Ann. Rheum. Dis. 2020, 79, 172–173. [Google Scholar] [CrossRef]
- Webster, A.C.; Woodroffe, R.C.; Taylor, R.S.; Chapman, J.R.; Craig, J.C. Tacrolimus versus ciclosporin as primary immunosuppression for kidney transplant recipients: Meta-analysis and meta-regression of randomized trial data. BMJ 2005, 331, 810. [Google Scholar] [CrossRef]
- Halloran, P.; Mathew, T.; Tomlanovich, S.; Groth, C.; Hooftman, L.; Barker, C. Mycophenolate mofetil in renal allograft recipients: A pooled efficacy analysis of three randomized, double-blind, clinical studies in prevention of rejection. The International Mycophenolate Mofetil Renal Transplant Study Groups. Transplantation 1997, 63, 39–47; Erratum in Transplantation 1997, 63, 618. [Google Scholar]
- Wagner, M.; Earley, A.K.; Webster, A.C.; Schmid, C.H.; Balk, E.M.; Uhlig, K. Mycophenolic acid versus azathioprine as primary immunosuppression for kidney transplant recipients. Cochrane Database Syst. Rev. 2015, 12, CD007746. [Google Scholar] [CrossRef]
- Vincenti, F.; Rostaing, L.; Grinyo, J.; Rice, K.; Steinberg, S.; Gaite, L.; Moal, M.-C.; Mondragon-Ramirez, G.A.; Kothari, J.; Polinsky, M.S.; et al. Belatacept and Long-Term Outcomes in Kidney Transplantation. N. Engl. J. Med. 2016, 374, 333–343, Erratum in N. Engl. J. Med. 2016, 374, 698. [Google Scholar] [CrossRef]
- Durrbach, A.; Pestana, J.M.; Florman, S.; Del Carmen Rial, M.; Rostaing, L.; Kuypers, D.; Matas, A.; Wekerle, T.; Polinsky, M.; Meier-Kriesche, H.U.; et al. Long-Term Outcomes in Belatacept- Versus Cyclosporine-Treated Recipients of Extended Criteria Donor Kidneys: Final Results from BENEFIT-EXT, a Phase III Randomized Study. Am. J. Transplant. 2016, 16, 3192–3201. [Google Scholar] [CrossRef]
- Masson, P.; Henderson, L.; Chapman, J.R.; Craig, J.C.; Webster, A.C. Belatacept for kidney transplant recipients. Cochrane Database Syst. Rev. 2014, 2014, CD010699. [Google Scholar] [CrossRef]
- Rostaing, L.; Massari, P.; Garcia, V.D.; Mancilla-Urrea, E.; Nainan, G.; del Carmen Rial, M.; Steinberg, S.; Vincenti, F.; Shi, R.; Di Russo, G.; et al. Switching from calcineurin inhibitor-based regimens to a belatacept-based regimen in renal transplant recipients: A randomized phase II study. Clin. J. Am. Soc. Nephrol. 2011, 6, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Hahn, D.; Hodson, E.M.; A Hamiwka, L.; Lee, V.W.; Chapman, J.R.; Craig, J.C.; Webster, A.C. Target of rapamycin inhibitors (TOR-I; sirolimus and everolimus) for primary immunosuppression in kidney transplant recipients. Cochrane Database Syst. Rev. 2019, 12, CD004290. [Google Scholar] [CrossRef] [PubMed]
- Chehade Hassib, M.D.; Pascual Manuel, M.D. The Challenge of Acute Antibody-Mediated Rejection in Kidney Transplantation. Transplantation 2016, 100, 264–265. [Google Scholar] [CrossRef] [PubMed]
- Süsal, C.; Döhler, B.; Opelz, G. Presensitized kidney graft recipients with HLA class I and II antibodies are at increased risk for graft failure: A Collaborative Transplant Study report. Hum. Immunol. 2009, 70, 569. [Google Scholar] [CrossRef]
- Lachmann, N.; Terasaki, P.I.; Budde, K.; Liefeldt, L.; Kahl, A.; Reinke, P.; Pratschke, J.; Rudolph, B.; Schmidt, D.; Salama, A.; et al. Anti-human leukocyte antigen and donor-specific antibodies detected by luminex posttransplant serve as biomarkers for chronic rejection of renal allografts. Transplantation 2009, 87, 1505–1513. [Google Scholar] [CrossRef]
- Hidalgo, L.G.; Campbell, P.M.; Sis, B.; Einecke, G.; Mengel, M.; Chang, J.; Sellares, J.; Reeve, J.; Halloran, P.F. De novo donor-specific antibody at the time of kidney transplant biopsy associates with microvascular pathology and late graft failure. Am. J. Transplant. 2009, 9, 2532–2541. [Google Scholar] [CrossRef]
- Davis, S.; Wiebe, C.; Campbell, K.; Anobile, C.; Aubrey, M.; Stites, E.; Grafals, M.; Pomfret, E.; Nickerson, P.; Cooper, J.E. Adequate tacrolimus exposure modulates the impact of HLA class II molecular mismatch: A validation study in an American cohort. Am. J. Transplant. 2020, 21, 322–328. [Google Scholar] [CrossRef]
- Lederer, S.R.; Friedrich, N.; Banas, B.; von Welser, G.; Albert, E.D.; Sitter, T. Effects of mycophenolate mofetil on donor-specific antibody formation in renal transplantation. Clin. Transplant. 2005, 19, 168–174. [Google Scholar] [CrossRef]
- Budde, K.; Prashar, R.; Haller, H.; Rial, M.C.; Kamar, N.; Agarwal, A.; de Fijter, J.W.; Rostaing, L.; Berger, S.P.; Djamali, A.; et al. Conversion from Calcineurin Inhibitor- to Belatacept-Based Maintenance Immunosuppression in Renal Transplant Recipients: A Randomized Phase 3b Trial. J. Am. Soc. Nephrol. 2021, 32, 3252–3264. [Google Scholar] [CrossRef]
- Bray, R.A.; Gebel, H.M.; Townsend, R.; Roberts, M.E.; Polinsky, M.; Yang, L.; Meier-Kriesche, H.-U.; Larsen, C.P. Posttransplant reduction in preexisting donor-specific antibody levels after belatacept- versus cyclosporine-based immunosuppression: Post hoc analyses of BENEFIT and BENEFIT-EXT. Am. J. Transplant. 2018, 18, 1774–1782. [Google Scholar] [CrossRef]
- Morath, C.; Opelz, G.; Zeier, M.; Süsal, C. Prevention of antibody-mediated kidney transplant rejection. Transplant. Int. 2009, 25, 633–645. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, C.; Gibson, I.W.; Blydt-Hansen, T.D.; Karpinski, M.; Ho, J.; Storsley, L.J.; Goldberg, A.; Birk, P.E.; Rush, D.N.; Nickerson, P.W. Evolution and clinical pathologic correlations of de novo donor-specific HLA antibody post kidney transplant. Am. J. Transplant. 2012, 12, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Sellarés, J.; De Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Stringer, D.; Gardner, L.; Shaw, O.; Clarke, B.; Briggs, D.; Worthington, J.; Buckland, M.; Danzi, G.; Hilton, R.; Picton, M.; et al. Optimized immunosuppression to prevent graft failure in renal transplant recipients with HLA antibodies (OuTSMART): A randomized controlled trial. eClinicalMedicine 2022, 56, 101819. [Google Scholar] [CrossRef] [PubMed]
- Machado, S.; Agarwal, G.; Ahmed, F.; Julian, B.; Mannon, R.; Mehta, S.; Kumar, V.; Ong, S.; Thaduri, S.; Towns, G.; et al. Immunosurveillance with Donor Derived Cellular Free DNA Assay Plus Donor Specific Antibody, an Alternative to Renal Allograft Biopsy. Am. J. Transplant. 2020, 20, 686. [Google Scholar]
- Bloom, R.D.; Bromberg, J.S.; Poggio, E.D.; Bunnapradist, S.; Langone, A.J.; Sood, P.; Matas, A.J.; Mehta, S.; Mannon, R.B.; Sharfuddin, A.; et al. Cell-Free DNA and Active Rejection in Kidney Allografts. J. Am. Soc. Nephrol. 2017, 28, 2221–2232. [Google Scholar] [CrossRef]
- Sigdel, T.K.; Archila, F.A.; Constantin, T.; Prins, S.A.; Liberto, J.; Damm, I.; Towfighi, P.; Navarro, S.; Kirkizlar, E.; Demko, Z.P.; et al. Optimizing Detection of Kidney Transplant Injury by Assessment of Donor-Derived Cell-Free DNA via Massively Multiplex PCR. J. Clin. Med. 2019, 8, 19. [Google Scholar] [CrossRef]
- Friedewald, J.J.; Kurian, S.M.; Heilman, R.L.; Whisenant, T.C.; Poggio, E.D.; Marsh, C.; Baliga, P.; Odim, J.; Brown, M.M.; Ikle, D.N.; et al. Development and clinical validity of a novel blood-based molecular biomarker for subclinical acute rejection following kidney transplant. Am. J. Transplant. 2019, 19, 98–109. [Google Scholar] [CrossRef]
- Swanson, K.J.; Aziz, F.; Garg, N.; Mohamed, M.; Mandelbrot, D.; Djamali, A.; Parajuli, S. Role of novel biomarkers in kidney transplantation. World J. Transplant. 2020, 10, 230–255. [Google Scholar] [CrossRef]
- ClinicalTrials.gov Identifier: NCT0366335.
- Doberer, K.; Duerr, M.; Halloran, P.F.; Eskandary, F.; Budde, K.; Regele, H.; Reeve, J.; Borski, A.; Kozakowski, N.; Reindl-Schwaighofer, R.; et al. A Randomized Clinical Trial of Anti-IL-6 Antibody Clazakizumab in Late Antibody-Mediated Kidney Transplant Rejection. J. Am. Soc. Nephrol. 2021, 32, 708–722. [Google Scholar] [CrossRef]
- Nickerson, P.W.; Böhmig, G.A.; Chadban, S.; Kumar, D.; Mannon, R.B.; van Gelder, T.; Lee, J.C.; Adler, S.; Chong, E.; Djamali, A. Clazakizumab for the treatment of chronic active antibody-mediated rejection (AMR) in kidney transplant recipients: Phase 3 IMAGINE study rationale and design. Trials 2022, 23, 1042. [Google Scholar] [CrossRef] [PubMed]
- Daligault, M.; Bardy, B.; Noble, J.; Bourdin, A.R.; Masson, D.; Bennani, H.N.; Bugnazet, M.B.; Malvezzi, P.; Rostaing, L.; Jouve, T. Marginal Impact of Tocilizumab Monotherapy on Anti-HLA Alloantibodies in Highly Sensitized Kidney Transplant Candidates. Transplant. Direct 2021, 7, e690. [Google Scholar] [CrossRef] [PubMed]
- Vo, A.A.; Choi, J.; Kim, I.; Louie, S.; Cisneros, K.; Kahwaji, J.; Toyoda, M.; Ge, S.; Haas, M.; Puliyanda, D.; et al. A Phase I/II Trial of the Interleukin-6 Receptor-Specific Humanized Monoclonal (Tocilizumab) + Intravenous Immunoglobulin in Difficult to Desensitize Patients. Transplantation 2015, 99, 2356–2363. [Google Scholar] [CrossRef]
- Jordan, S.C.; Vescio, R.; Toyoda, M.; Ammerman, N.; Huang, E.; Peng, A.; Sethi, S.; Najjar, R.; Lim, K.; Vo, A. Daratumumab for Treatment of Antibody-Mediated Rejection in a Kidney Transplant Recipient [abstract]. Am. J. Transplant. 2019, 19 (Suppl. S3), 1062. [Google Scholar]
- Spica, D.; Junker, T.; Dickenmann, M.; Schaub, S.; Steiger, J.; Rüfli, T.; Halter, J.; Hopfer, H.; Holbro, A.; Hirt-Minkowski, P. Daratumumab for Treatment of Antibody-Mediated Rejection after ABO-Incompatible Kidney Transplantation. Case Rep. Nephrol. Dial. 2019, 9, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Banham, G.D.; Flint, S.M.; Torpey, N.; Lyons, P.; Shanahan, D.N.; Gibson, A.; Watson, C.; O’Sullivan, A.-M.; A Chadwick, J.; E Foster, K.; et al. Belimumab in kidney transplantation: An experimental medicine, randomized, placebo-controlled phase 2 trial. Lancet 2018, 391, 2619–2630. [Google Scholar] [CrossRef]
- Winstedt, L.; Järnum, S.; Nordahl, E.A.; Olsson, A.; Runström, A.; Bockermann, R.; Karlsson, C.; Malmström, J.; Palmgren, G.S.; Malmqvist, U.; et al. Complete Removal of Extracellular IgG Antibodies in a Randomized Dose-Escalation Phase I Study with the Bacterial Enzyme IdeS—A Novel Therapeutic Opportunity. PLoS ONE 2015, 10, e0132011. [Google Scholar] [CrossRef]
- Jordan, S.C.; Lorant, T.; Choi, J.; Kjellman, C.; Winstedt, L.; Bengtsson, M.; Zhang, X.; Eich, T.; Toyoda, M.; Eriksson, B.M.; et al. IgG Endopeptidase in Highly Sensitized Patients Undergoing Transplantation. N. Engl. J. Med. 2017, 377, 442–453. [Google Scholar] [CrossRef]
- Jordan, S.C.; Legendre, C.; Desai, N.M.; Lorant, T.; Bengtsson, M.; Lonze, B.E.; Vo, A.A.; Runström, A.M.; Laxmyr, L.; Sjöholm, K.; et al. Imlifidase Desensitization in Crossmatch-positive, Highly Sensitized Kidney Transplant Recipients: Results of an International Phase 2 Trial (Highdes). Transplantation 2021, 105, 1808–1817. [Google Scholar] [CrossRef]
- Viglietti, D.; Gosset, C.; Loupy, A.; Deville, L.; Verine, J.; Zeevi, A.; Glotz, D.; Lefaucheur, C. C1 Inhibitor in Acute Antibody-Mediated Rejection Nonresponsive to Conventional Therapy in Kidney Transplant Recipients: A Pilot Study. Am. J. Transplant. 2016, 16, 1596–1603. [Google Scholar] [CrossRef]
- Montgomery, R.A.; Orandi, B.J.; Racusen, L.; Jackson, A.M.; Garonzik-Wang, J.M.; Shah, T.; Woodle, E.S.; Sommerer, C.; Fitts, D.; Rockich, K.; et al. Plasma-Derived C1 Esterase Inhibitor for Acute Antibody-Mediated Rejection Following Kidney Transplantation: Results of a Randomized Double-Blind Placebo-Controlled Pilot Study. Am. J. Transplant. 2016, 16, 3468–3478. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, D.A.; Schnitzler, M.A.; Xiao, H.; Irish, W.; Tuttle-Newhall, E.; Chang, S.-H.; Kasiske, B.L.; Alhamad, T.; Lentine, K.L. An economic assessment of contemporary kidney transplant practice. Am. J. Transplant. 2018, 18, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Fu, R.M.; Sekercioglu, N.; Berta, W.; Coyte, P.C. Cost-effectiveness of Deceased-donor Renal Transplant Versus Dialysis to Treat End-stage Renal Disease: A Systematic Review. Transplant. Direct 2020, 6, e522. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Pre-transplant |
| Avoiding sensitization |
| HLA matching including eplet matching |
| Desensitization |
| Peri-transplant |
| Minimizing cold ischemia time/Optimizing perfusion |
| Individualizing induction immunosuppression |
| HLA matching including eplet matching |
| Post-transplant |
| Individualizing maintenance immunosuppression |
| Minimizing non-compliance |
| DSA monitoring |
| Treatment of acute rejection |
| Role of novel biomarkers |
| Agent | Class | Mechanism of Action | Adverse Effects |
|---|---|---|---|
| Basiliximab | Lymphocyte Non-depleting | Blocks IL-2 receptor | Minimal |
| Rabbit anti-thymocyte globulin | Lymphocyte depleting | Polyclonal rabbit antisera; destroys T lymphocytes by targeting multiple antigens | Infections, Bone marrow suppression, infusion reactions |
| Alemtuzumab | Lymphocyte depleting | Humanized rat monoclonal antibody; destroys T lymphocytes and other immune cells by targeting CD-52 | Infections, Bone marrow suppression |
| Drug | Class/Mechanism | Use | Adverse Effects | Practical Considerations |
|---|---|---|---|---|
| Tacrolimus | CNI | Used in a vast majority of combination regimens for maintenance immunosuppression | Neurotoxicity which includes tremor, AMS and memory loss, nephrotoxicity, increased incidence of DM, Hair loss | Component of >90% regimens in the US. Also available as a long-acting formulation called Envarsus |
| Cyclosporine | CNI | Limited use in current regimens for maintenance immunosuppression | Hirsutism, gingival enlargement, nephrotoxicity | Was approved more than a decade before tacrolimus but is now primarily used in patients who are intolerant of tacrolimus |
| Mycophenolic Acid | Antimetabolite | In combination with tacrolimus makes up more than 90% of maintenance immunosuppression regimens | GI side effects including nausea, vomiting and diarrhea; bone marrow suppression | Contraindicated in pregnancy |
| Azathioprine | Antimetabolite | Used in combination with CNI/Belatacept/mTORi rarely | Bone marrow suppression, hepatotoxicity | Useful in pregnancy and in case of intolerable side effects to MPA. Genetic polymorphisms exist that alter metabolism |
| Prednisone | Corticosteroid | Used in about 70% of maintenance immunosuppression regimens | Metabolic side effects, osteoporosis, weight gain | Can be used as part of induction, maintenance, and rejection treatment regimens |
| Sirolimus/ Everolimus | mTOR inhibitor | Used rarely either in combination with CNI or other agents | Hyperlipidemia, lymphedema, bone marrow suppression, lung injury, oral ulcers, proteinuria, impaired wound healing | Useful in special circumstances like skin cancer and certain viral infections like BK and CMV |
| Belatacept | CTLA-4 Ig fusion; works as co-stimulation blockade to selectively halt T-cell activation | Used as part of maintenance immunosuppression in patients who cannot tolerate CNI; de novo use is rare | Infusion reactions, bone marrow suppression, diarrhea | Black box warning in EBV-seronegative patients: increased risk of PTLD. Use is increasing because of less nephrotoxicity. Cost remains a major issue |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malhotra, D.; Jethwani, P. Preventing Rejection of the Kidney Transplant. J. Clin. Med. 2023, 12, 5938. https://doi.org/10.3390/jcm12185938
Malhotra D, Jethwani P. Preventing Rejection of the Kidney Transplant. Journal of Clinical Medicine. 2023; 12(18):5938. https://doi.org/10.3390/jcm12185938
Chicago/Turabian StyleMalhotra, Divyanshu, and Priyanka Jethwani. 2023. "Preventing Rejection of the Kidney Transplant" Journal of Clinical Medicine 12, no. 18: 5938. https://doi.org/10.3390/jcm12185938
APA StyleMalhotra, D., & Jethwani, P. (2023). Preventing Rejection of the Kidney Transplant. Journal of Clinical Medicine, 12(18), 5938. https://doi.org/10.3390/jcm12185938