
Risk Factors and Predictors for Functional Outcome and Complication Rate in Total Hip Arthroplasty through Minimally Invasive and Conventional Approaches: A Systematic Review and Meta-Regression Analysis of 41 Randomized Controlled Trials
 ,
,
Abstract
1. Introduction
2. Materials and Methods
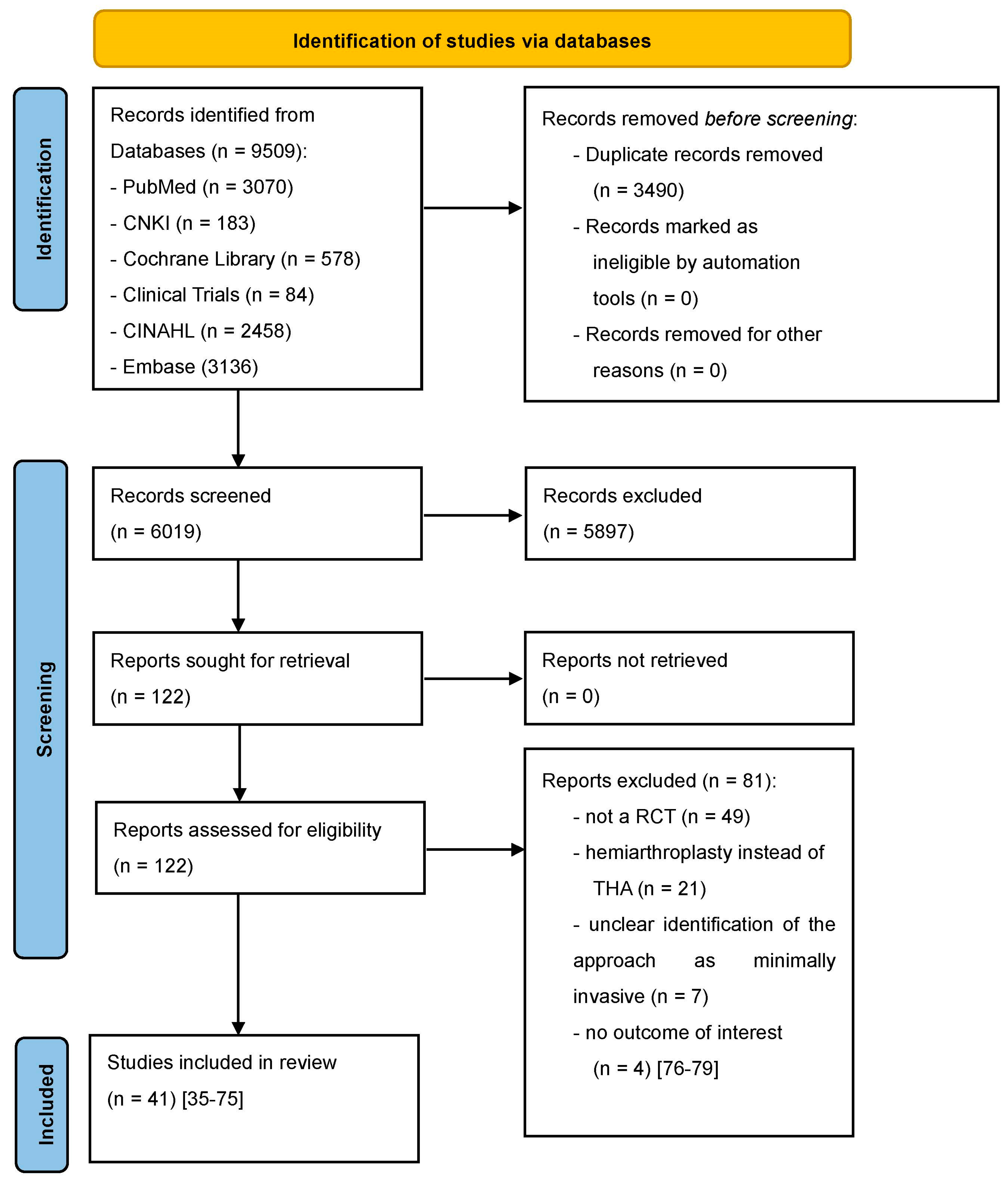
2.1. Search Strategy and Inclusion Criteria
2.2. Data Extraction
2.3. Outcome Parameters
2.4. RCT Quality Assessment
2.5. Data Synthesis and Statistical Analysis

3. Results
3.1. Quality Assessment
3.2. Meta-Analysis
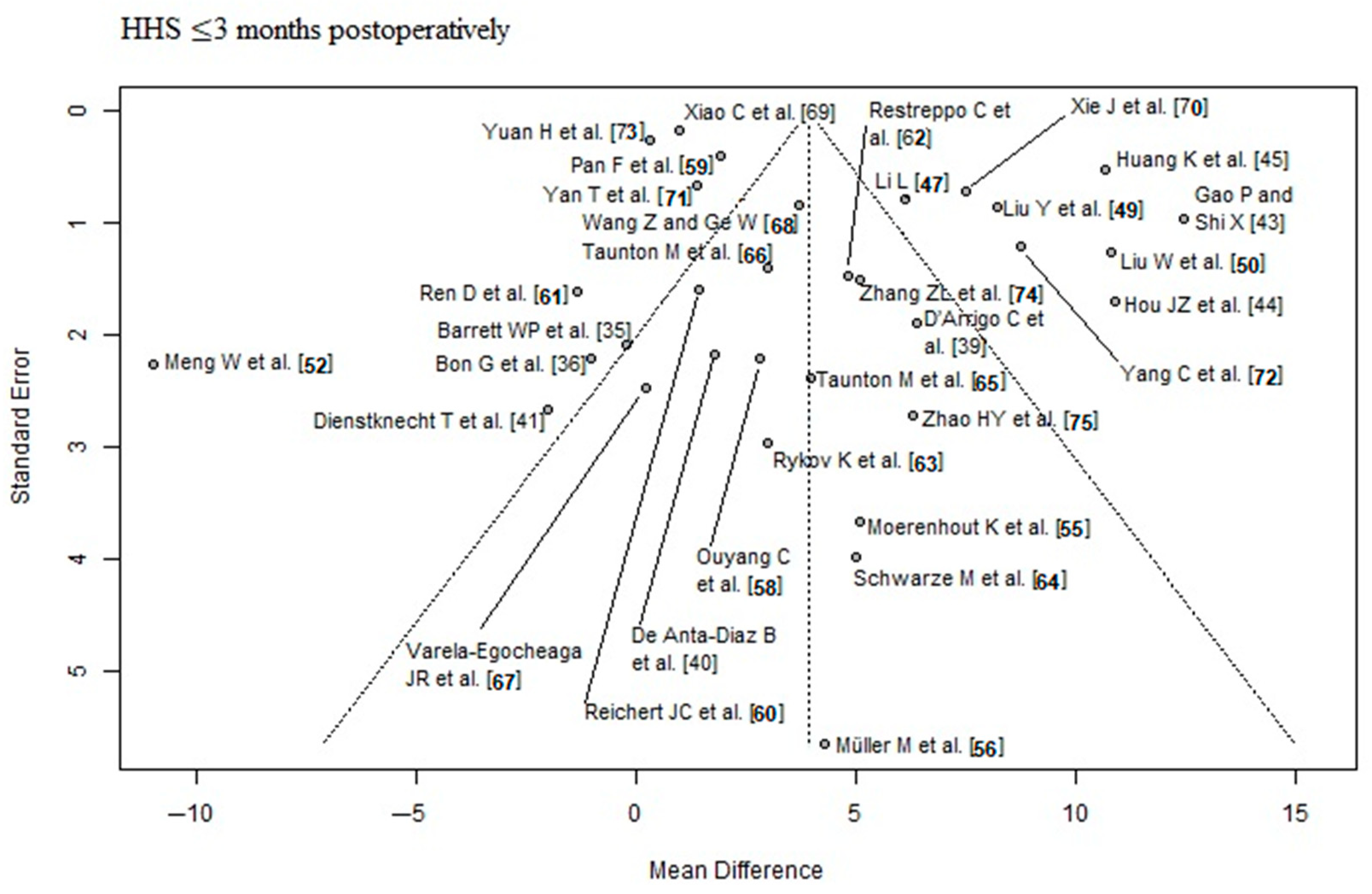
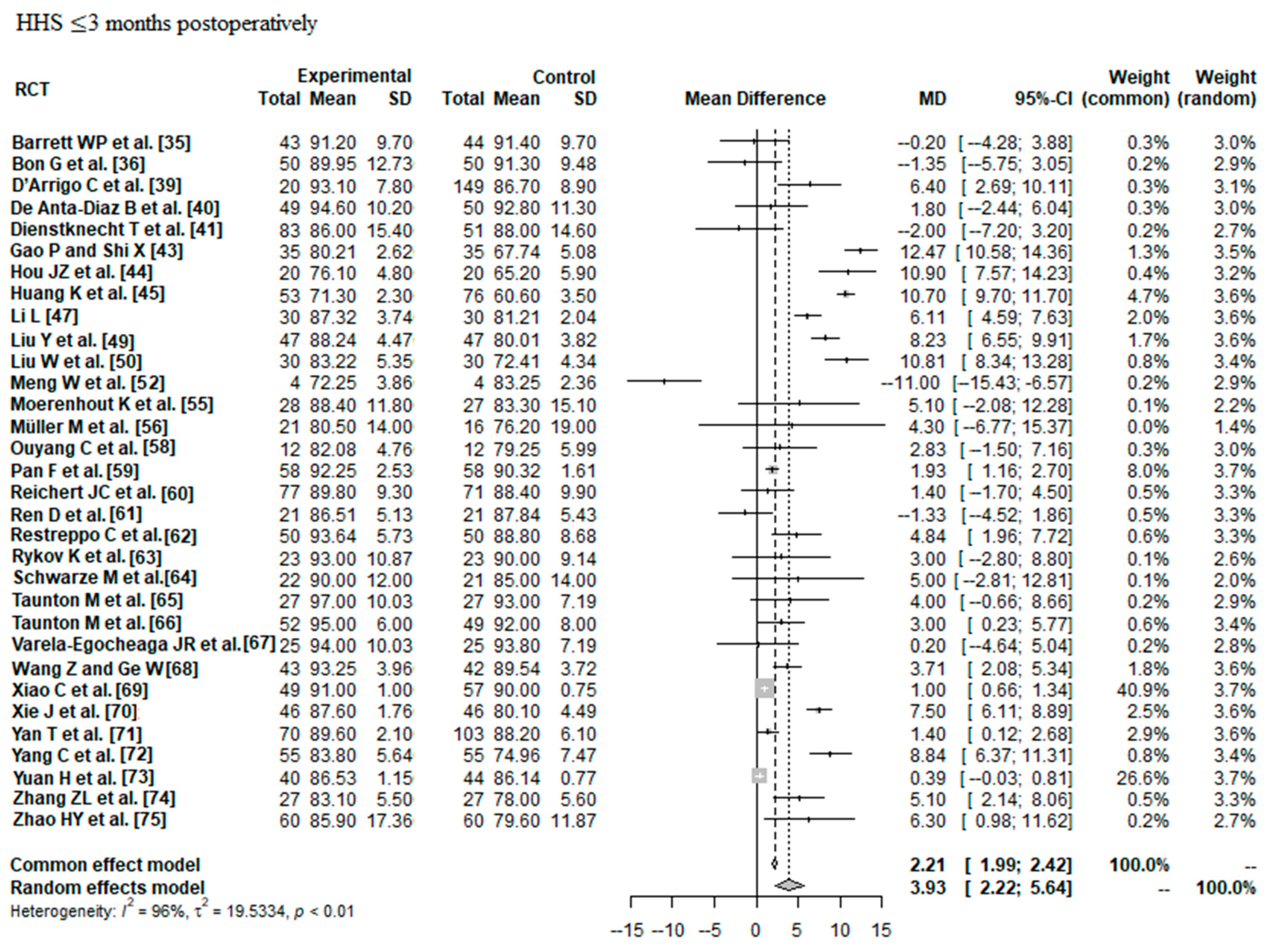
3.2.1. HHS ≤ 3 Months Postoperatively
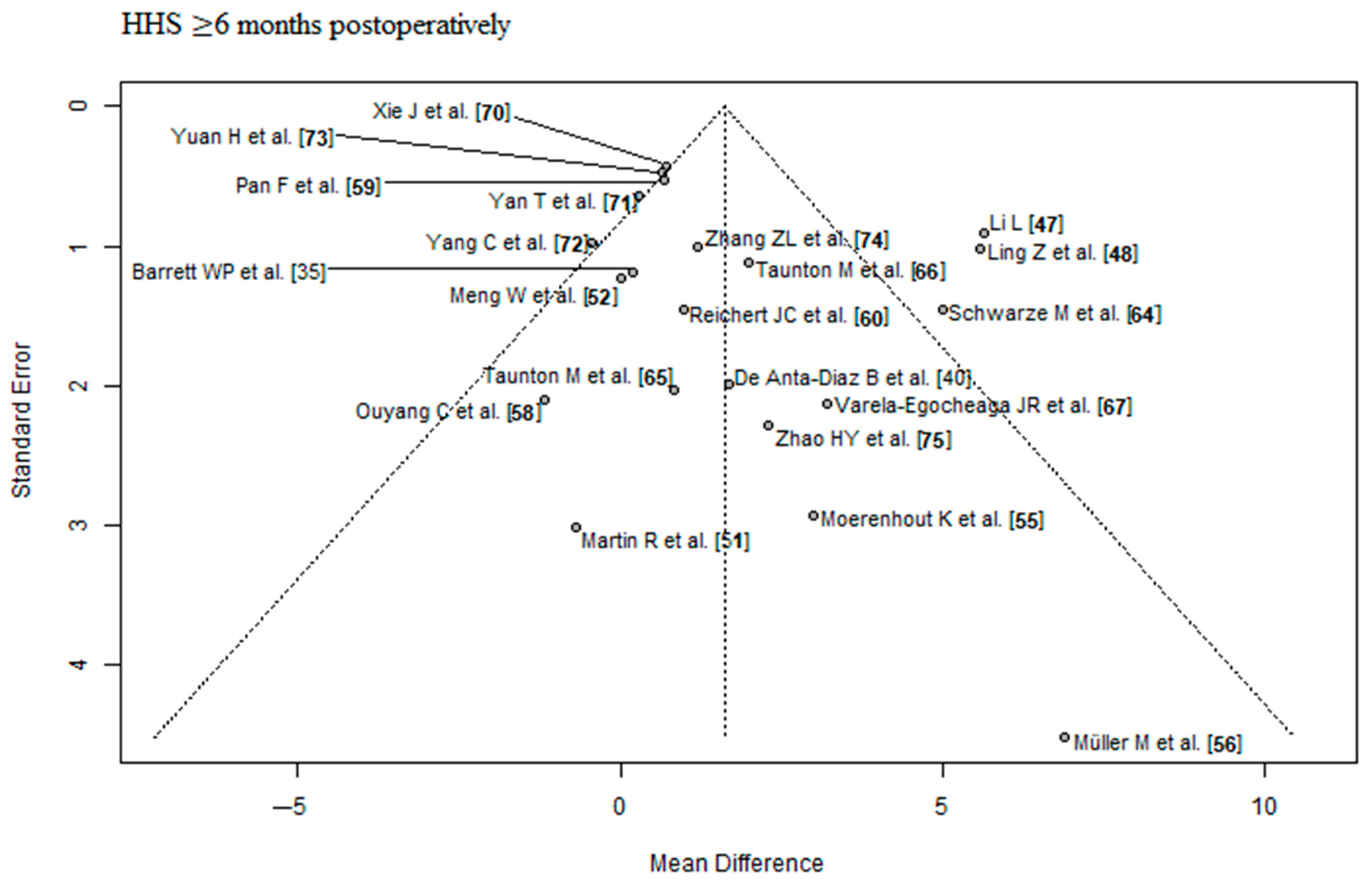
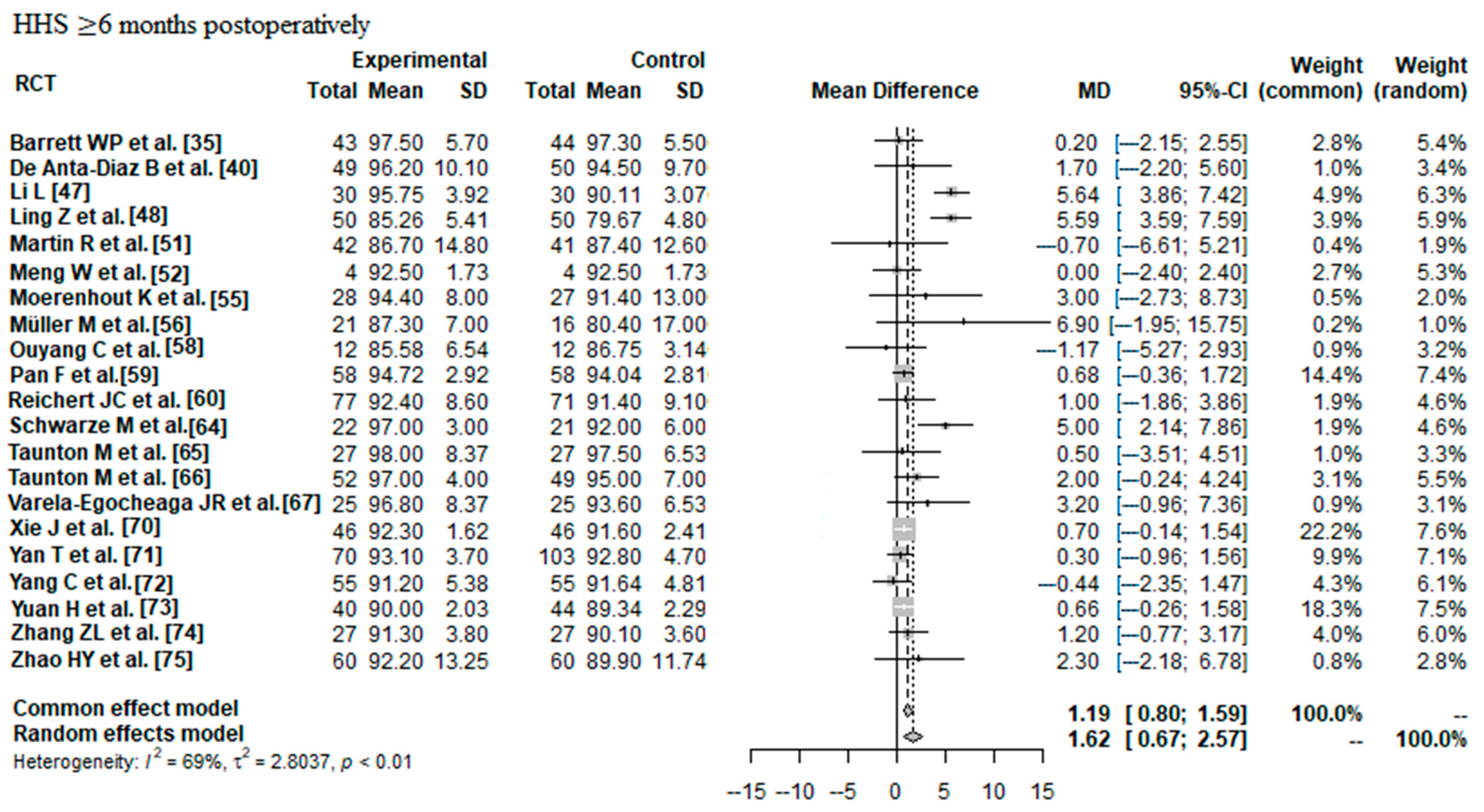
3.2.2. HHS ≥ 6 Months Postoperatively
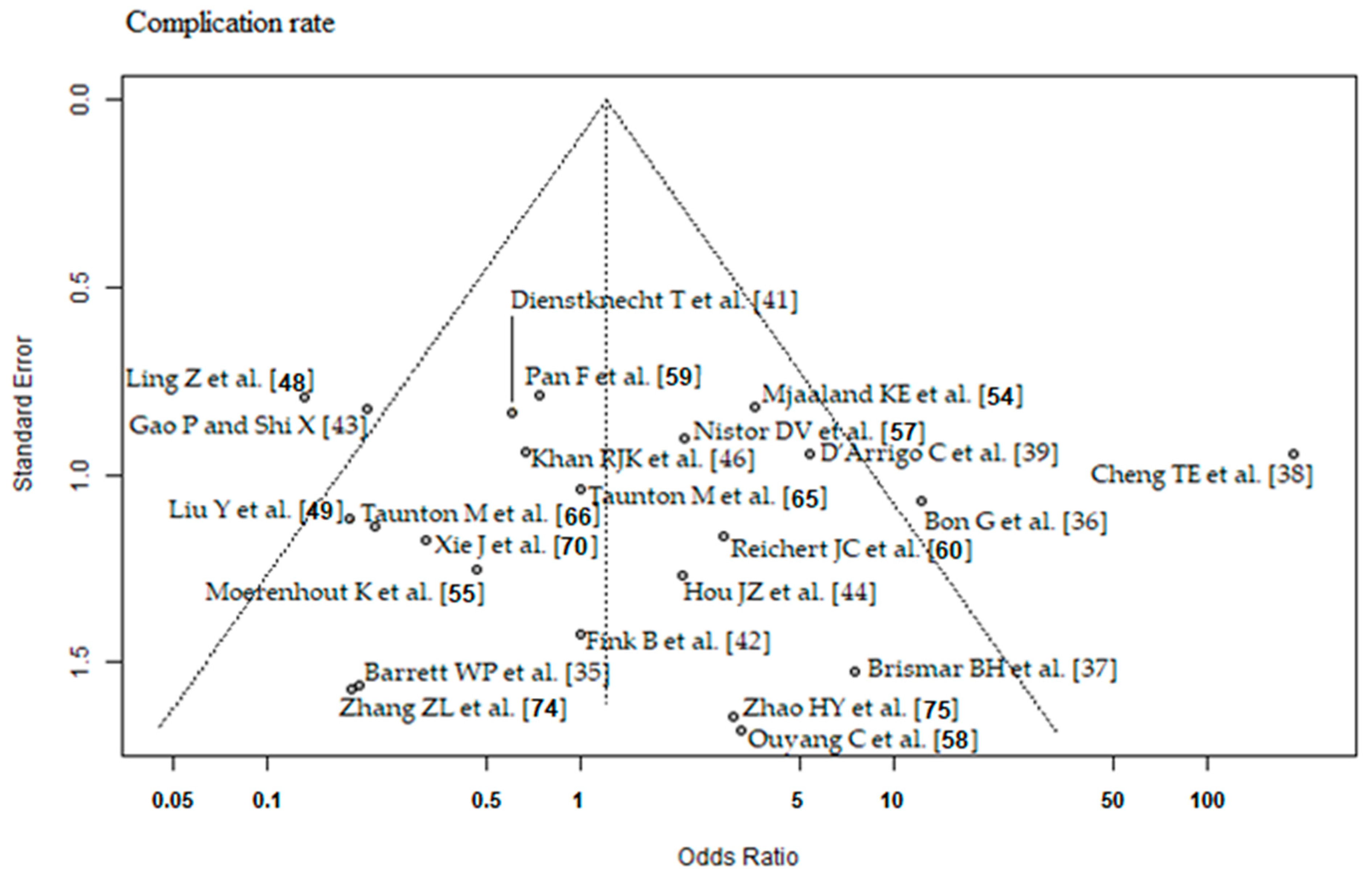
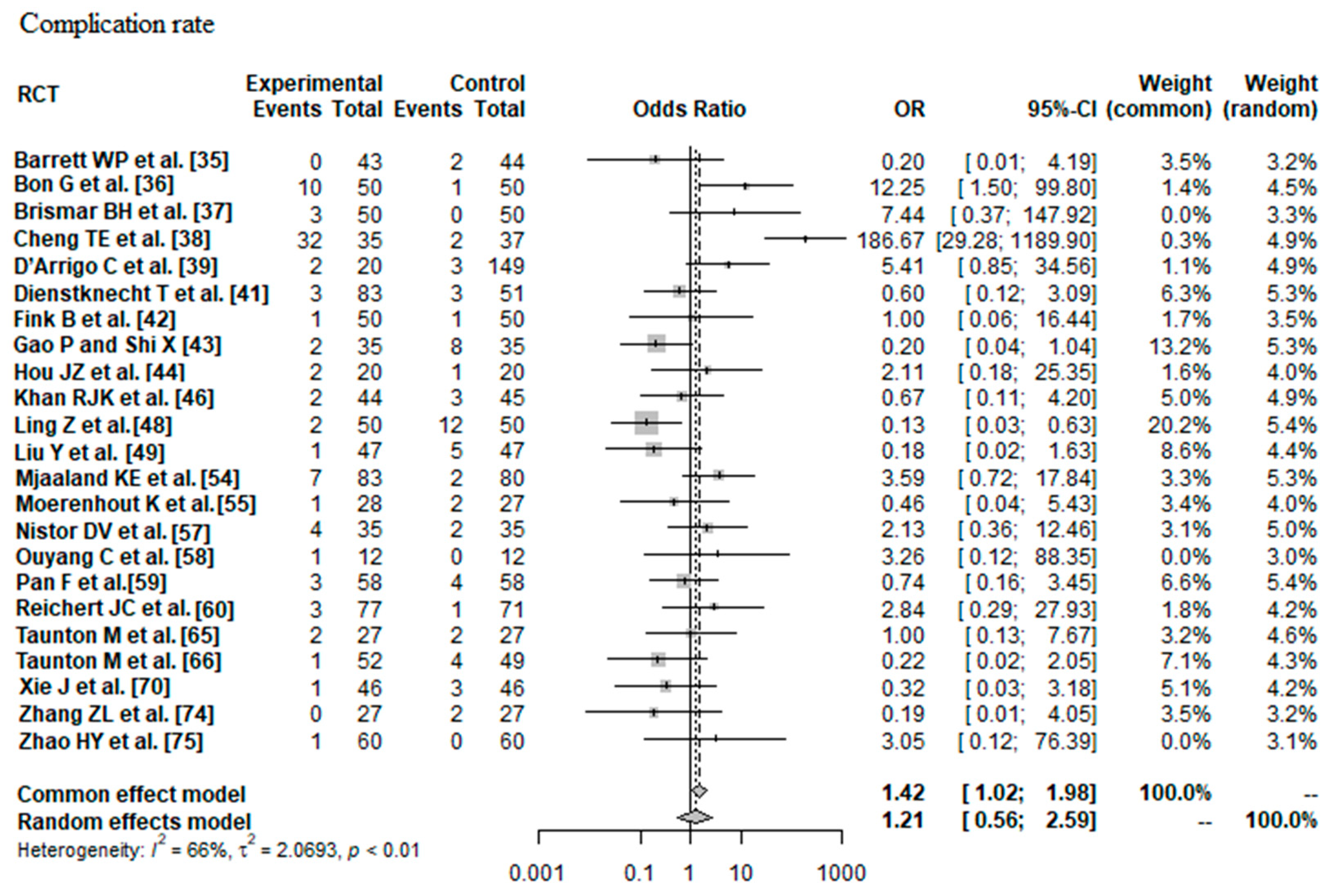
3.2.3. Complication Rate
3.3. Meta-Regression Analysis
3.3.1. Risk Factors and Predictors of HHS ≤ 3 Months Postoperatively
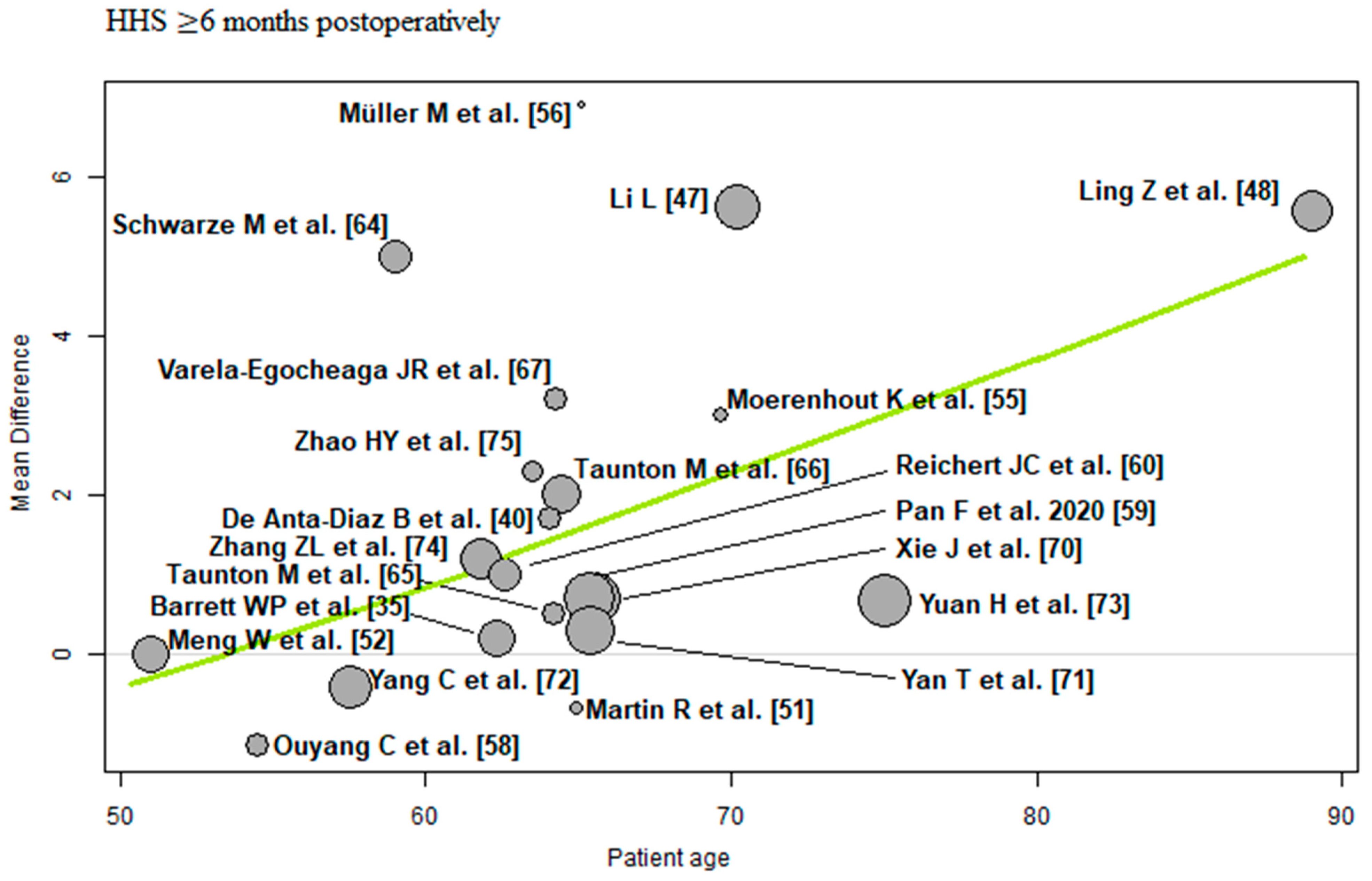
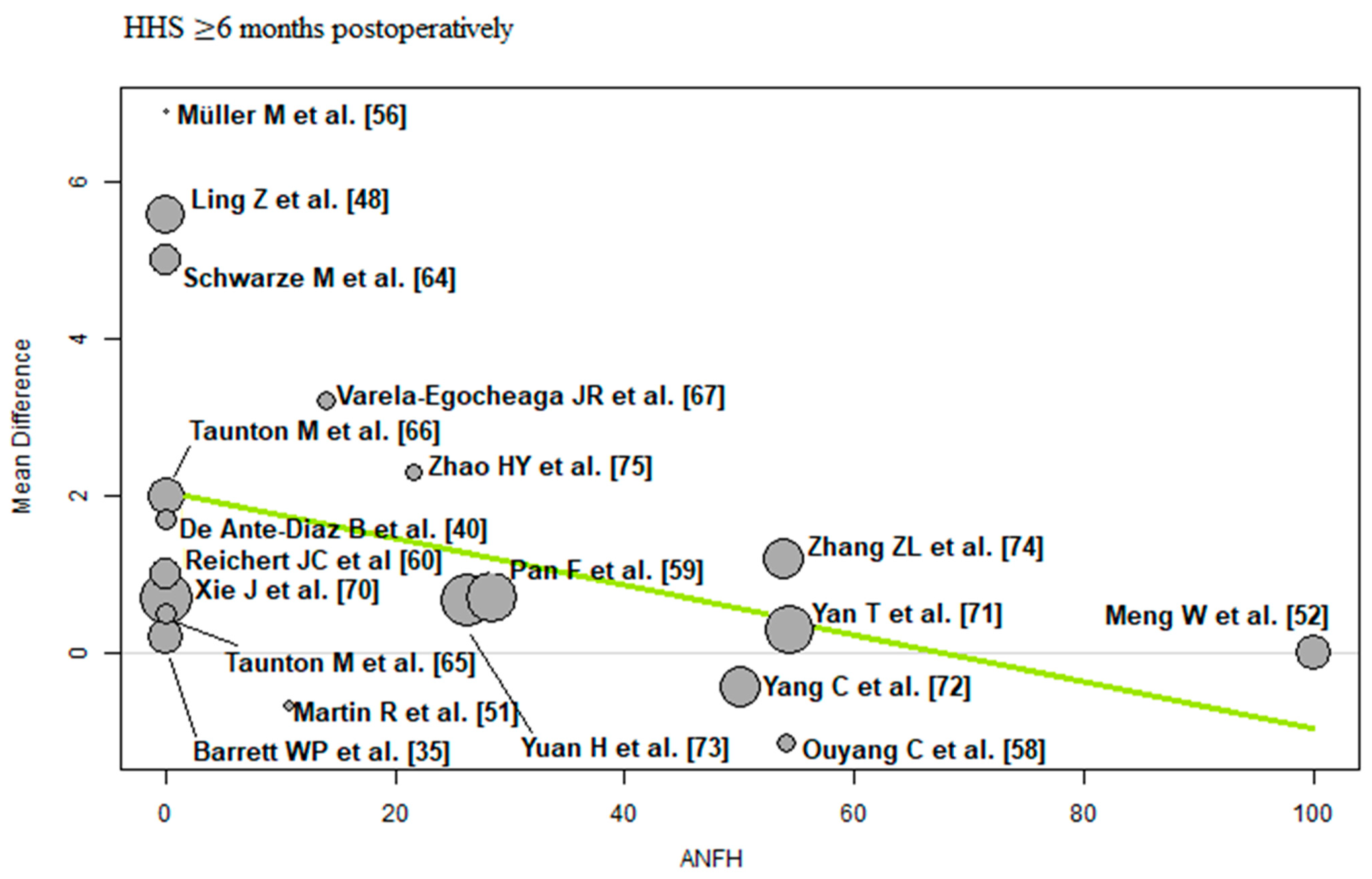
3.3.2. Risk Factors and Predictors of HHS ≥ 6 Months Postoperatively
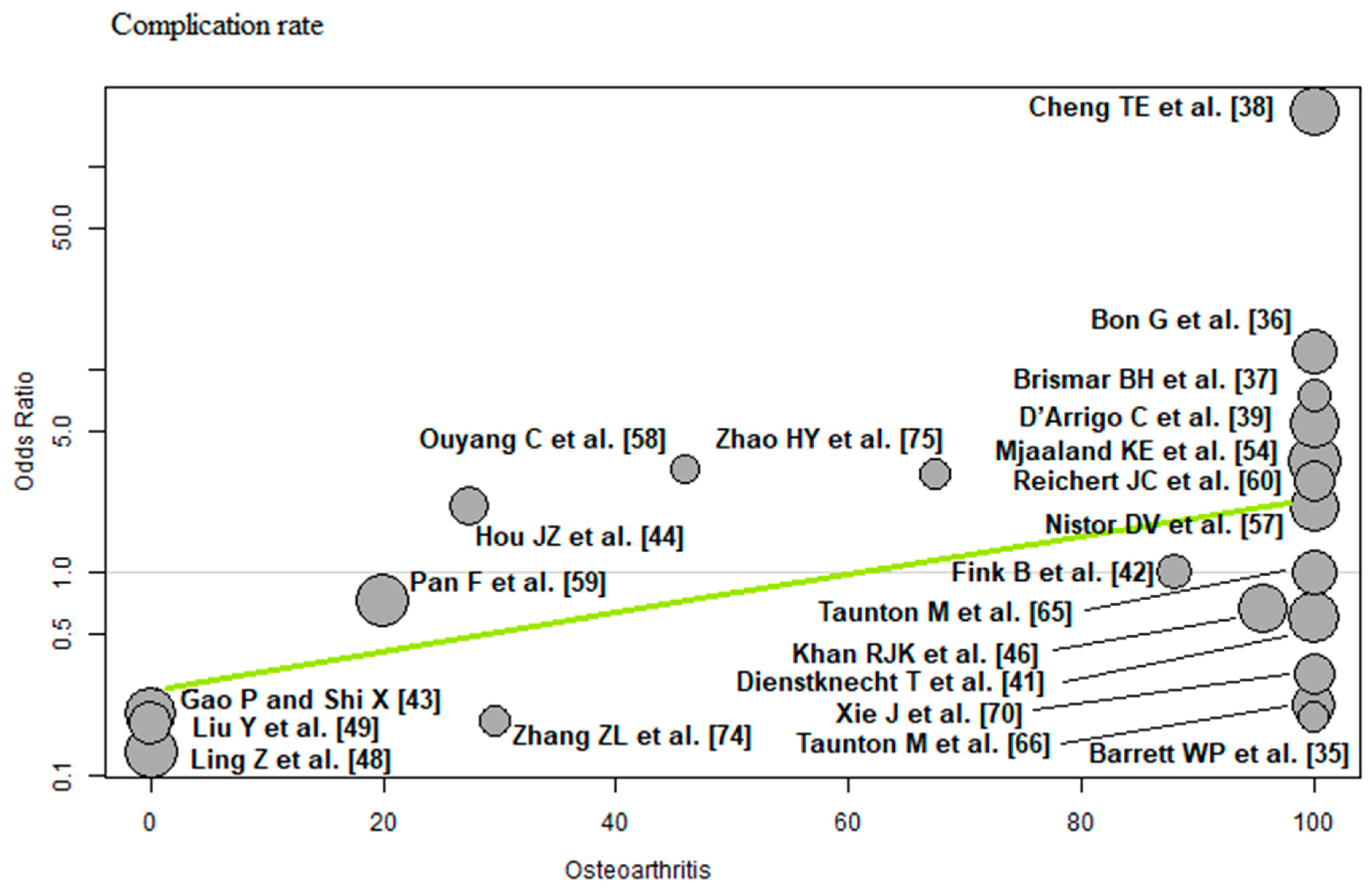
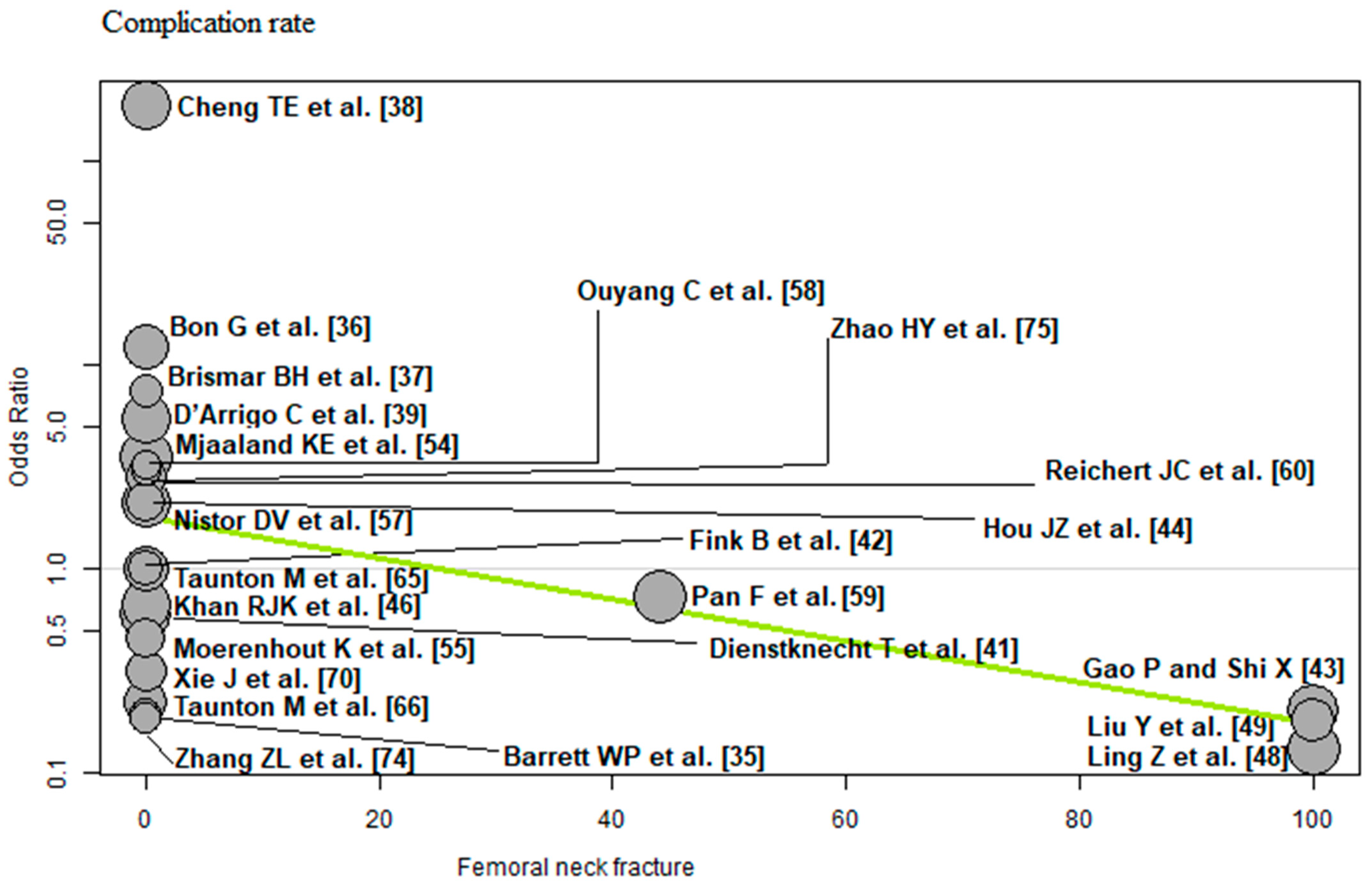
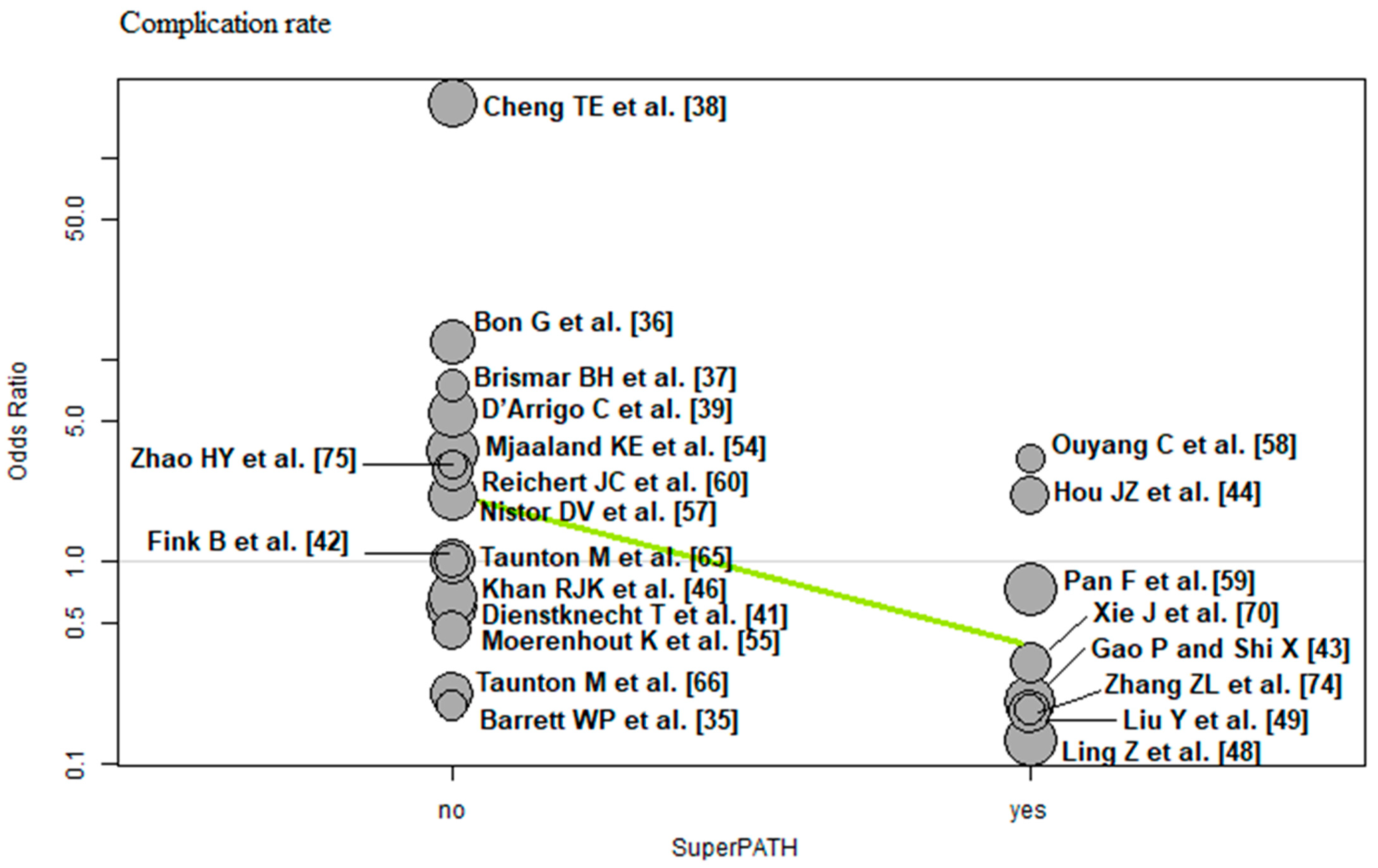
3.3.3. Risk Factors and Predictors of Complication Rate
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANFH | avascular necrosis of the femoral head |
| BMI | body mass index |
| CI | confidence interval |
| CINAHL | Cumulative Index to Nursing and Allied Health Literature |
| CK | creatine kinase |
| CNKI | China National Knowledge Infrastructure |
| CRP | C-reactive protein |
| HHS | Harris Hip Score |
| ITT | intention-to-treat |
| MD | mean difference |
| OR | odds ratio |
| THA | total hip arthroplasty |
References
- Varacallo, M.A.; Herzog, L.; Toossi, N.; Johanson, N.A. Ten-Year Trends and Independent Risk Factors for Unplanned Readmission Following Elective Total Joint Arthroplasty at a Large Urban Academic Hospital. J. Arthroplast. 2017, 32, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jordan, J. Epidemiology of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A. Osteoarthritis is a serious disease. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 120), 3–6. [Google Scholar] [PubMed]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Nelson, A.E.; Abbate, L.M.; et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2009, 36, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Steinbuch, M.; Stevenson, R.; Miday, R.; Watts, N.B. The epidemiology of osteonecrosis: Findings from the GPRD and THIN databases in the UK. Osteoporos. Int. 2010, 21, 569–577. [Google Scholar] [CrossRef]
- Zhao, D.W.; Yu, M.; Hu, K.; Wang, W.; Yang, L.; Wang, B.J.; Gao, X.H.; Guo, Y.M.; Xu, Y.Q.; Wei, Y.S.; et al. Prevalence of Nontraumatic Osteonecrosis of the Femoral Head and its Associated Risk Factors in the Chinese Population: Results from a Nationally Representative Survey. Chin. Med. J. 2015, 128, 2843–2850. [Google Scholar] [CrossRef]
- Rosell, P.A.; Parker, M.J. Functional outcome after hip fracture. A 1-year prospective outcome study of 275 patients. Injury 2003, 34, 529–532. [Google Scholar] [CrossRef]
- Bonnaire, F.; Weber, A. S2e-Leitlinie Schenkelhalsfraktur des Erwachsenen. 2015. Available online: https://www.awmf.org/uploads/tx_szleitlinien/012-001l_S2e_Schenkelhalsfraktur_2015-10_01.pdf (accessed on 1 January 2023).
- Bender, B.; Nogler, M.; Hozack, W.J. Direct anterior approach for total hip arthroplasty. Orthop. Clin. N. Am. 2009, 40, 321e8. [Google Scholar] [CrossRef]
- Graf, R.; Mohajer, M.A. The Stolzalpe technique: A modified Watson-Jones approach. Int. Orthop. 2007, 31 (Suppl. 1), S21e4. [Google Scholar] [CrossRef]
- Berger, R.A. The technique of minimally invasive total hip arthroplasty using the two-incision approach. Instr. Course Lect. 2004, 53, 149e55. [Google Scholar]
- Della Torre, P.K.; Fitch, D.A.; Chow, J.C. Supercapsular percutaneously-assisted total hip arthroplasty: Radiographic outcomes and surgical technique. Ann. Transl. Med. 2015, 3, 180. [Google Scholar] [PubMed]
- Howell, J.R.; Garbuz, D.S.; Duncan, C.P. Minimally invasive hip replacement: Rationale, applied anatomy, and instrumentation. Orthop. Clin. N. Am. 2004, 35, 107e18. [Google Scholar] [CrossRef]
- Berry, D.J.; Berger, R.A.; Callaghan, J.J.; Dorr, L.D.; Duwelius, P.J.; Hartzband, M.A.; Lieberman, J.R.; Mears, D.C. Minimally invasive total hip arthroplasty. Development, early results, and a critical analysis. Presented at the Annual Meeting of the American Orthopaedic Association, Charleston, South Carolina, USA, June 14, 2003. J. Bone Joint Surg. Am. 2003, 85, 2235–2246. [Google Scholar] [CrossRef]
- Cheng, T.; Feng, J.G.; Liu, T.; Zhang, X.L. Minimally invasive total hip arthroplasty: A systematic review. Int. Orthop. 2009, 33, 1473e81. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nilsdotter, A.-K.; Petersson, I.F.; Roos, E.M.; Lohmander, L.S. Predictors of patient relevant outcome after total hip replacement for osteoarthritis: A prospective study. Ann. Rheum. Dis. 2003, 62, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Johanson, N.A.; Abzug, J.M.; Gallus, C.A.; Charlson, M.E. Baseline function and comorbidity predict outcome in total hip arthroplasty. UPOJ 2009, 194, 1–7. [Google Scholar]
- Davis, A.M.; Agnidis, Z.; Bradley, E.; Kiss, A.; Waddell, J.P.; Gross, A.E. Predictors of functional outcome two years following revision hip arthroplasty. J. Bone Joint Surg. Am. 2006, 88-A, 685–691. [Google Scholar]
- Cushnaghan, J.; Coggon, D.; Reading, I.; Croft, P.; Byng, P.; Cox, K.; Dieppe, P.; Cooper, C. Long-term outcome following total hip arthroplasty: A controlled longitudinal study. Arthritis Rheum. 2007, 57, 1375–1380. [Google Scholar] [CrossRef]
- Biring, G.S.; Masri, B.A.; Greidanus, N.V.; Duncan, C.P.; Garbuz, D.S. Predictors of quality of life outcomes after revision total hip replacement. J. Bone Joint Surg. Br. 2007, 89-B, 1446–1451. [Google Scholar] [CrossRef]
- Smith, G.H.; Johnson, S.; Ballantyne, J.A.; Dunstan, E.; Brenkel, I.J. Predictors of excellent early outcome after total hip arthroplasty. J. Orthop. Surg. Res. 2012, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Huddleston, J.I.; Wang, Y.; Uquillas, C.; Herndon, J.H.; Maloney, W.J. Age and obesity are risk factors for adverse events after total hip arthroplasty. Clin. Orthop. Relat. Res. 2012, 470, 490–496. [Google Scholar] [CrossRef]
- Melloh, M.; Eggli, S.; Busato, A.; Roder, C. Predictors of early stem loosening after total hip arthroplasty: A case-control study. J. Orthop. Surg. 2011, 19, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Buirs, L.D.; Van Beers, L.W.; Scholtes, V.A.; Pastoors, T.; Sprague, S.; Poolman, R.W. Predictors of physical functioning after total hip arthroplasty: A systematic review. BMJ Open 2016, 6, e010725. [Google Scholar] [CrossRef] [PubMed]
- Hofstede, S.N.; Gademan, M.G.; Vliet Vlieland, T.P.; Nelissen, R.G.; Marang-van de Mheen, P.J. Preoperative predictors for outcomes after total hip replacement in patients with osteoarthritis: A systematic review. BMC Musculoskelet. Disord. 2016, 17, 212. [Google Scholar] [CrossRef]
- Prokopetz, J.J.; Losina, E.; Bliss, R.L.; Wright, J.; Baron, J.A.; Katz, J.N. Risk factors for revision of primary total hip arthroplasty: A systematic review. BMC Musculoskelet. Disord. 2012, 13, 251. [Google Scholar] [CrossRef]
- Ren, X.; Ling, L.; Qi, L.; Liu, Z.; Zhang, W.; Yang, Z.; Wang, W.; Tu, C.; Li, Z. Patients’ risk factors for periprosthetic joint infection in primary total hip arthroplasty: A meta-analysis of 40 studies. BMC Musculoskelet. Disord. 2021, 22, 776. [Google Scholar] [CrossRef]
- Hewlett-Smith, N.; Pope, R.; Furness, J.; Simas, V.; Hing, W. Prognostic factors for inpatient functional recovery following total hip and knee arthroplasty: A systematic review. Acta Orthop. 2020, 91, 313–318. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Deeks, J.; Altman, D. Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011; Chapter 16. [Google Scholar]
- Harris, W.H. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Joint Surg. Am. 1969, 51, 737–755. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Berkey, C.S.; Hoaglin, D.C.; Antczak-Bouckoms, A.; Mosteller, F.; Colditz, G.A. Meta-analysis of multiple outcomes by regression with random effects. Stat. Med. 1998, 17, 2537–2550. [Google Scholar] [CrossRef]
- Barrett, W.P.; Turner, S.E.; Leopold, J.P. Prospective randomized study of direct anterior vs postero-lateral approach for total hip arthroplasty. J. Arthroplast. 2013, 28, 1634–1638. [Google Scholar] [CrossRef] [PubMed]
- Bon, G.; Kacem, E.B.; Lepretre, P.M.; Weissland, T.; Mertl, P.; Dehl, M.; Gabrion, A. Does the direct anterior approach allow earlier recovery of walking following total hip arthroplasty? A randomized prospective trial using accelerometry. Orthop. Traumatol. Surg. Res. 2019, 105, 445–452. [Google Scholar] [CrossRef]
- Brismar, B.H.; Hallert, O.; Tedhamre, A.; Lindgren, J.U. Early gain in pain reduction and hip function, but more complications following the direct anterior minimally invasive approach for total hip arthroplasty: A randomized trial of 100 patients with 5 years of follow up. Acta Orthop. 2018, 89, 484–489. [Google Scholar] [CrossRef]
- Cheng, T.E.; Wallis, J.A.; Taylor, N.F.; Holden, C.T.; Marks, P.; Smith, C.L.; Armstrong, M.S.; Singh, P.J. A Prospective Randomized Clinical Trial in Total Hip Arthroplasty-Comparing Early Results Between the Direct Anterior Approach and the Posterior Approach. J. Arthroplast. 2017, 32, 883–890. [Google Scholar] [CrossRef]
- D’Arrigo, C.; Speranza, A.; Monaco, E.; Carcangiu, A.; Ferretti, A. Learning curve in tissue sparing total hip replacement: Comparison between different approaches. J. Orthop. Traumatol. 2009, 10, 47–54. [Google Scholar] [CrossRef]
- De Anta-Díaz, B.; Serralta-Gomis, J.; Lizaur-Utrilla, A.; Benavidez, E.; López-Prats, F.A. No differences between direct anterior and lateral approach for primary total hip arthroplasty related to muscle damage or functional outcome. Int. Orthop. 2016, 40, 2025–2030. [Google Scholar] [CrossRef]
- Dienstknecht, T.; Lüring, C.; Tingart, M.; Grifka, J.; Sendtner, E. A minimally invasive approach for total hip arthroplasty does not diminish early post-operative outcome in obese patients: A prospective, randomised trial. Int. Orthop. 2013, 37, 1013–1018. [Google Scholar] [CrossRef]
- Fink, B.; Mittelstaedt, A.; Schulz, M.S.; Sebena, P.; Singer, J. Comparison of a minimally invasive posterior approach and the standard posterior approach for total hip arthroplasty A prospective and comparative study. J. Orthop. Surg. Res. 2010, 5, 46. [Google Scholar] [CrossRef]
- Gao, P.; Shi, X. The effect of total hip replacement with minimally invasive SuperPATH approach in the treatment of femoral neck fractures in the elderly. Hen. Med. Res. 2020, 29, 3715–3717. (In Chinese) [Google Scholar]
- Hou, J.Z.; Bao, H.; Cheng, Y. Early effect observation of total hip arthroplasty by using SuperPATH technique. J. Clin. Orthop. 2017, 20, 50–53. (In Chinese) [Google Scholar]
- Huang, K.; Xie, K.; Shi, Y.; Lu, X.; Chen, J.; Lu, L.; Liu, J.; Lu, M.; Pan, S.; Tang, Y. Analysis of early clinical efficacy of SuperPATH approach and lateral approach for initial total hip arthroplasty. Youjiang Med. J. 2021, 49, 9. [Google Scholar]
- Khan, R.J.; Maor, D.; Hofmann, M.; Haebich, S. A comparison of a less invasive piriformis-sparing approach versus the standard posterior approach to the hip: A randomised controlled trial. J. Bone Joint Surg. Br. 2012, 94, 43–50. [Google Scholar] [CrossRef]
- Li, L. SuperPATH minimally invasive total hip replacement surgery treatment: Analysis of clinical efficacy of aseptic necrosis of femoral head. Chin. J. Mod. Drug Appl. 2020, 14, 84–86. (In Chinese) [Google Scholar]
- Ling, Z.; Zhou, P.; Fu, Y. Analysis of the effect of total hip replacement via SuperPATH approach on the prognosis of elderly patients with femoral neck fracture. Chin. J. Front. Med. Sc. 2020, 12, 66–70. (In Chinese) [Google Scholar]
- Liu, Y.; Hu, P.; Zhu, J.; She, H.; Zhang, Y. Efficacy of minimally invasive total hip arthroplasty in the treatment of elderly femoral neck fractures. Prac. J. Med. Pharm. 2021, 38, 226–231. [Google Scholar]
- Liu, W.; Liu, X.; Gao, H.; Wang, G.; Li, J. Comparison of the curative effect, pain degree, and hip joint function between SuperPATH hip replacement and total hip replacement. Mod. Chin. Docs. 2022, 60, 78–84. [Google Scholar]
- Martin, R.; Clayson, P.E.; Troussel, S.; Fraser, B.P.; Docquier, P.L. Anterolateral minimally invasive total hip arthroplasty: A prospective randomized controlled study with a follow-up of 1 year. J. Arthroplast. 2011, 26, 1362–1372. [Google Scholar] [CrossRef]
- Meng, W.; Huang, Z.; Wang, H.; Wang, D.; Luo, Z.; Bai, Y.; Gao, L.; Wang, G.; Zhou, Z. Supercapsular percutaneously-assisted total hip (SuperPath) versus posterolateral total hip arthroplasty in bilateral osteonecrosis of the femoral head: A pilot clinical trial. BMC Musculoskelet. Disord. 2019, 21, 2. [Google Scholar] [CrossRef]
- Mjaaland, K.E.; Kivle, K.; Svenningsen, S.; Pripp, A.H.; Nordsletten, L. Comparison of markers for muscle damage, inflammation, and pain using minimally invasive direct anterior versus direct lateral approach in total hip arthroplasty: A prospective, randomized, controlled trial. J. Orthop. Res. 2015, 33, 1305–1310. [Google Scholar] [CrossRef]
- Mjaaland, K.E.; Kivle, K.; Svenningsen, S.; Nordsletten, L. Do Postoperative Results Differ in a Randomized Trial Between a Direct Anterior and a Direct Lateral Approach in THA? Clin. Orthop. Relat. Res. 2019, 477, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Moerenhout, K.; Derome, P.; Laflamme, G.Y.; Leduc, S.; Gaspard, H.S.; Benoit, B. Direct anterior versus posterior approach for total hip arthroplasty: A multicentre, prospective, randomized clinical trial. Can. J. Surg. 2020, 63, E412–E417. [Google Scholar] [CrossRef]
- Müller, M.; Tohtz, S.; Springer, I.; Dewey, M.; Perka, C. Randomized controlled trial of abductor muscle damage in relation to the surgical approach for primary total hip replacement: Minimally invasive anterolateral versus modified direct lateral approach. Arch. Orthop. Trauma Surg. 2011, 131, 179–189. [Google Scholar] [CrossRef]
- Nistor, D.V.; Caterev, S.; Bolboacă, S.D.; Cosma, D.; Lucaciu, D.O.G.; Todor, A. Transitioning to the direct anterior approach in total hip arthroplasty. Is it a true muscle sparing approach when performed by a low volume hip replacement surgeon? Int. Orthop. 2017, 41, 2245–2252. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, C.; Wang, H.; Meng, W.; Luo, Z.; Wang, D.; Pei, F.; Zhou, Z. Randomized controlled trial of comparison between the SuperPATH and posterolateral approaches in total hip arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2018, 32, 1500–1506. (In Chinese) [Google Scholar] [PubMed]
- Pan, Y.; Zhang, J.; Yan, X.; Chang, X.; Li, J.; Tang, B. Comparison of SuperPATH and posterolateral total hip replacement. Orthop. J. China 2020, 28, 1176–1180. (In Chinese) [Google Scholar]
- Reichert, J.C.; von Rottkay, E.; Roth, F.; Renz, T.; Hausmann, J.; Kranz, J.; Rackwitz, L.; Nöth, U.; Rudert, M. A prospective randomized comparison of the minimally invasive direct anterior and the transgluteal approach for primary total hip arthroplasty. BMC Musculoskelet. Disord. 2018, 19, 241. [Google Scholar] [CrossRef]
- Ren, D.; Yang, G.; Zhao, H.; Zha, J.; Lu, S.; Xu, Y. Effect of SuperPath minimally invasive incision total hip arthroplasty on femoral head necrosis and the quality of life. J. Hebei Med. Univ. 2016, 37, 1416–1419. (In Chinese) [Google Scholar]
- Restrepo, C.; Parvizi, J.; Pour, A.E.; Hozack, W.J. Prospective randomized study of two surgical approaches for total hip arthroplasty. J. Arthroplast. 2010, 25, 671–679.e1. [Google Scholar] [CrossRef]
- Rykov, K.; Reininga, I.H.F.; Sietsma, M.S.; Knobben, B.A.S.; Ten Have BLEF. Posterolateral vs Direct Anterior Approach in Total Hip Arthroplasty (POLADA Trial): A Randomized Controlled Trial to Assess Differences in Serum Markers. J. Arthroplast. 2017, 32, 3652–3658.e1. [Google Scholar] [CrossRef]
- Schwarze, M.; Budde, S.; von Lewinski, G.; Windhagen, H.; Keller, M.C.; Seehaus, F.; Hurschler, C.; Floerkemeier, T. No effect of conventional vs. minimally invasive surgical approach on clinical outcome and migration of a short stem total hip prosthesis at 2-year follow-up: A randomized controlled study. Clin. Biomech. 2018, 51, 105–112. [Google Scholar] [CrossRef]
- Taunton, M.J.; Mason, J.B.; Odum, S.M.; Springer, B.D. Direct anterior total hip arthroplasty yields more rapid voluntary cessation of all walking aids: A prospective, randomized clinical trial. J. Arthroplast. 2014, 29 (Suppl. 9), 169–172. [Google Scholar] [CrossRef] [PubMed]
- Taunton, M.J.; Trousdale, R.T.; Sierra, R.J.; Kaufman, K.; Pagnano, M.W. John Charnley Award: Randomized Clinical Trial of Direct Anterior and Miniposterior Approach THA: Which Provides Better Functional Recovery? Clin. Orthop. Relat. Res. 2018, 476, 216–229. [Google Scholar] [CrossRef] [PubMed]
- Varela-Egocheaga, J.R.; Suárez-Suárez, M.A.; Fernández-Villán, M.; González-Sastre, V.; Varela-Gómez, J.R.; Murcia-Mazón, A. Minimally invasive hip surgery: The approach did not make the difference. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 47–52. [Google Scholar] [CrossRef]
- Wang, Z.; Ge, W. SuperPATH approach total hip replacement for elderly patients with femoral neck fracture: Impact of hip function. Clin. Med. 2021, 41, 27–29. (In Chinese) [Google Scholar]
- Xiao, C.; Gao, Z.; Zhang, S.; Long, N.; Yao, K.; Cai, P.; He, F.; Liu, L.; Jiang, Y. Comparative prospective randomized study of minimally invasive transpiriformis approach versus conventional posterolateral approach in total hip arthroplasty as measured by biology markers. Int. Orthop. 2021, 45, 1707–1717. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Zhang, H.; Wang, L.; Yao, X.; Pan, Z.; Jiang, Q. Comparison of supercapsular percutaneously assisted approach total hip versus conventional posterior approach for total hip arthroplasty: A prospective, randomized controlled trial. J. Orthop. Surg. Res. 2017, 12, 138. [Google Scholar] [CrossRef]
- Yan, T.; Tian, S.; Wang, Y.; Yang, X.; Li, T.; Liu, J.; Pan, P.; Wang, R.; Wang, D.; Sun, K. Comparison of early effectiveness between SuperPATH approach and Hardinge approach in total hip arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2017, 31, 17–24. (In Chinese) [Google Scholar] [PubMed]
- Yang, C.; Zhu, Q.; Han, Y.; Zhu, J.; Wang, H.; Cong, R.; Zhang, D. Minimally-invasive total hip arthroplasty will improve early postoperative outcomes: A prospective, randomized, controlled trial. Ir. J. Med. Sci. 2010, 179, 285–290. [Google Scholar] [CrossRef]
- Yuan, H.; Zhu, J.; Sun, Z.; Zhang, Z. Comparison of effectiveness between SuperPATH approach and posterolateral approach in total hip arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2018, 32, 14–19. (In Chinese) [Google Scholar] [PubMed]
- Zhang, Z.L.; Lin, J.; Xia, B. Clinical research on joint function and life quality through SuperPath approach in total hip arthroplasty. China J. Integr. Trad. Chin. West. Med. 2019, 25, 709–714. (In Chinese) [Google Scholar]
- Zhao, H.Y.; Kang, P.D.; Xia, Y.Y.; Shi, X.J.; Nie, Y.; Pei, F.X. Comparison of Early Functional Recovery After Total Hip Arthroplasty Using a Direct Anterior or Posterolateral Approach: A Randomized Controlled Trial. J. Arthroplast. 2017, 32, 3421–3428. [Google Scholar] [CrossRef]
- Landgraeber, S.; Quitmann, H.; Güth, S.; Haversath, M.; Kowalczyk, W.; Kecskeméthy, A.; Heep, H.; Jäger, M. A prospective randomized peri- and post-operative comparison of the minimally invasive anterolateral approach versus the lateral approach. Orthop. Rev. 2013, 5, e19. [Google Scholar]
- Li, X.; Ma, L.; Wang, Q.; Rong, K. Comparison of total hip arthroplasty with minimally invasive SuperPath approach vs. conventional posterolateral approach in elderly patients: A one-year follow-up randomized controlled research. Asian J. Surg. 2021, 44, 531–536. [Google Scholar] [CrossRef]
- Parvizi, J.; Restrepo, C.; Maltenfort, M.G. Total Hip Arthroplasty Performed Through Direct Anterior Approach Provides Superior Early Outcome: Results of a Randomized, Prospective Study. Orthop. Clin. N. Am. 2016, 47, 497–504. [Google Scholar] [CrossRef]
- Zhao, S. Minimally invasive SuperPATH approach for hip replacement in elderly patients. Analysis of clinical efficacy in patients with bone neck fractures. Mod. Diagn. Treat. 2021, 32, 3593. [Google Scholar]
- Ramadanov, N. An Updated Meta-Analysis of Randomized Controlled Trials on Total Hip Arthroplasty through SuperPATH versus Conventional Approaches. Orthop. Surg. 2022, 14, 807–823. [Google Scholar] [CrossRef]
- Basile, G.; Gallina, M.; Passeri, A.; Gaudio, R.M.; Castelnuovo, N.; Ferrante, P.; Calori, G.M. Prosthetic joint infections and legal disputes: A threat to the future of prosthetic orthopedics. J. Orthop. Traumatol. 2021, 22, 44. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RCT | Year of Publication, Origin | Patients, N | THAs, N | Sex, Male, N (%) | Approach | Use of Bone Cement, N | Table/ Patient Position | Mean Age, Years, SD | Mean BMI, kg/m2, SD | HHS Preoperatively, Points, SD |
|---|---|---|---|---|---|---|---|---|---|---|
| Barrett WP et al. [35] | 2013, USA | 43 | 43 | 29 (67.44) | MI DAA | 0 | TT | 61.40 ± 9.20 | 30.70 ± 5.40 | 57.60 ± 10.20 |
| 44 | 44 | 19 (43.18) | CA PL | 0 | Lat | 63.20 ± 7.70 | 29.10 ± 5.00 | 55.10 ± 9.10 | ||
| Bon G et al. [36] | 2019, France | 50 | 50 | 21 (42.00) | MI DAA | 7 | TT | 67.26 ± 10.00 | 26.46 ± 3.58 | 54.04 ± 14.94 |
| 50 | 50 | 23 (46.00) | CA P | 7 | NR | 68.98 ± 7.93 | 26.69 ± 3.12 | 52.31 ± 13.06 | ||
| Brismar BH et al. [37] | 2018, Sweden | 50 | 50 | 18 (36.00) | MI DAA | 0 | Supine | 66.00 ± 4.00 | 27.00 ± 1.25 | NR |
| 50 | 50 | 17 (34.00) | CA L | 0 | Lat | 67.00 ± 4.00 | 27.00 ± 1.50 | NR | ||
| Cheng TE et al. [38] | 2016, Australia | 35 | 35 | 15 (42.29) | MI DAA | NR | TT | 59.00 ± 3.75 | 27.70 ± 1.05 | NR |
| 37 | 37 | 18 (48.65) | CA P | NR | Lat | 62.50 ± 3.50 | 28.30 ± 1.57 | NR | ||
| D’Arrigo C et al. [39] | 2009, Italy | 20 | 20 | 12 (60.00) | MI DAA | 0 | NR | 64.00 ± 8.00 | 22.70 ± 1.50 | 37.70 ± 19.00 |
| 149 | 149 | 81 (54.36) | CA L | 0 | NR | 65.00 ± 9.80 | 28.00 ± 1.80 | 39.00 ± 10.20 | ||
| De Anta-Diaz B et al. [40] | 2016, Spain | 49 | 49 | 26 (53.06) | MI DAA | 8 | NR | 64.80 ± 10.10 | 26.60 ± 3.90 | 44.40 ± 13.60 |
| 50 | 50 | 26 (52.00) | CA L | 6 | NR | 63.50 ± 12.50 | 26.90 ± 3.10 | 42.90 ± 15.20 | ||
| Dienstknecht T et al. [41] * | 2013, Germany | 42 | 42 | 14 (33.33) | MI MH | 2 | Lat | 61.00 ± 13.00 | 26.10 ± 3.00 | 48.00 ± 15.00 |
| 36 | 36 | 12 (33.33) | CA L | 1 | NR | 62.00 ± 13.00 | 24.30 ± 3.60 | 46.00 ± 16.00 | ||
| 41 | 41 | 24 (58.54) | MI MH | 3 | Lat | 61.00 ± 11.00 | 34.30 ± 4.40 | 44.00 ± 15.00 | ||
| 15 | 15 | 10 (66.67) | CA L | 0 | NR | 61.00 ± 10.00 | 34.60 ± 4.10 | 46.00 ± 16.00 | ||
| Fink B et al. [42] | 2010, Germany | 50 | 50 | 25 (50.00) | MI P | 50 | NR | 71.90 ± 6.10 | 27.00 ± 4.80 | NR |
| 50 | 50 | 23 (46.00) | CA PL | 50 | NR | 71.50 ± 5.60 | 28.00 ± 3.80 | NR | ||
| Gao P et Shi X [43] | 2020, China | 35 | 35 | 23 (65.71) | MI S | NR | Lat | 69.26 ± 3.28 | 23.09 ± 2.57 | 15.43 ± 2.92 |
| 35 | 35 | 20 (57.14) | CA P | NR | Lat | 68.81 ± 3.45 | 23.21 ± 2.44 | 15.65 ± 2.71 | ||
| Hou JZ et al. [44] | 2017, China | 20 | 20 | 13 (65.00) | MI S | NR | Lat | 54.30 ± 13.70 | 24.50 ± 3.60 | 33.80 ± 5.40 |
| 20 | 20 | 12 (60.00) | CA | NR | Lat | 53.80 ± 12.90 | 23.90 ± 4.10 | 31.90 ± 6.10 | ||
| Huang K et al. [45] ** | 2021, China | 37 | 37 | 31 (83.78) | MI S | NR | Lat | 56.20 ± 11.50 | NR | 47.30 ± 6.10 |
| 58 | 58 | 50 (86.21) | CA L | NR | Lat | 53.00 ± 10.40 | NR | 45.70 ± 8.10 | ||
| 16 | 16 | 2 (12.50) | MI S | NR | Lat | 78.10 ± 7.80 | NR | 40.60 ± 11.50 | ||
| 18 | 18 | 8 (44.44) | CA L | NR | Lat | 77.70 ± 10.10 | NR | 40.90 ± 11.60 | ||
| Khan RJK et al. [46] | 2012, Australia | 44 | 44 | 24 (54.55) | MI P | 44 | Lat | 72.30 ± 1.00 | 28.50 ± 0.70 | NR |
| 45 | 45 | 19 (42.22) | CA P | 45 | Lat | 72.80 ± 1.10 | 28.90 ± 0.60 | NR | ||
| Li L [47] | 2020, China | 30 | 30 | 16 (53.33) | MI S | NR | Lat | 70.35 ± 4.26 | NR | 25.41 ± 2.41 |
| 30 | 30 | 18 (60.00) | CA PL | NR | Lat | 70.12 ± 4.78 | NR | 26.35 ± 2.47 | ||
| Ling Z et al. [48] | 2020, China | 50 | 50 | 31 (62.00) | MI S | NR | NR | 89.14 ± 3.60 | NR | 46.08 ± 3.29 |
| 50 | 50 | 29 (58.00) | CA PL | NR | NR | 88.95 ± 3.71 | NR | 45.88 ± 3.71 | ||
| Liu Y et al. [49] | 2021, China | 47 | 47 | 26 (55.32) | MI S | NR | Lat | 68.27 ± 3.71 | NR | 67.70 ± 7.30 |
| 47 | 47 | 24 (51.06) | CA PL | NR | Lat | 68.55 ± 3.40 | NR | 68.66 ± 6.22 | ||
| Liu W et al. [50] | 2022, China | 30 | 30 | 17 (56.67) | MI S | NR | Lat | 58.59 ± 4.32 | NR | 58.73 ± 4.31 |
| 30 | 30 | 18 (60.00) | CA | NR | Lat | 58.31 ± 4.57 | NR | 58.79 ± 4.33 | ||
| Martin R et al. [51] | 2011, Belgium | 42 | 42 | 12 (28.57) | MI AL | 42 | Lat | 66.70 ± 10.10 | 30.60 ± 6.10 | 37.40 ± 15.50 |
| 41 | 41 | 14 (34.15) | CA L | 41 | NR | 63.10 ± 10.20 | 29.40 ± 5.50 | 40.20 ± 12.90 | ||
| Meng W et al. [52] | 2020, China | 2 | 4 | 2 (100.00) | MI S | NR | Lat | 51.00 ± 4.54 | 21.49 ± 1.73 | 37.86 ± 13.27 |
| 2 | 4 | 2 (100.00) | CA PL | NR | Lat | 51.00 ± 4.54 | 21.49 ± 1.73 | 37.66 ± 7.02 | ||
| Mjaaland KE et al. [53] *** | 2015, Norway | 83 | 83 | 25 (30.12) | MI DAA | 83 | Supine | 67.20 ± 8.60 | 27.70 ± 3.60 | 53.60 ± 13.70 |
| 80 | 80 | 30 (37.50) | CA L | 80 | Lat | 65.60 ± 8.60 | 27.60 ± 3.90 | 56.00 ± 11.20 | ||
| Mjaaland KE et al. [54] *** | 2018, Norway | 83 | 83 | 25 (30.12) | MI DAA | 83 | Supine | 67.20 ± 8.60 | 27.70 ± 3.60 | 53.60 ± 13.70 |
| 80 | 80 | 30 (37.50) | CA L | 80 | Lat | 65.60 ± 8.60 | 27.60 ± 3.90 | 56.00 ± 11.20 | ||
| Moerenhout K et al. [55] | 2019, Canada | 28 | 28 | 11 (39.29) | MI DAA | 0 | TT | 70.40 ± 9.10 | 27.60 ± 4.40 | 52.10 ± 19.70 |
| 27 | 27 | 18 (66.67) | CA P | 0 | Lat | 69.00 ± 8.80 | 26.50 ± 4.30 | 48.20 ± 10.10 | ||
| Müller M et al. [56] | 2010, Germany | 21 | 21 | 12 (57.14) | MI AL | 0 | NR | 66.00 ± 6.75 | 28.00 ± 4.25 | 55.90 ± 8.00 |
| 16 | 16 | 8 (50.00) | CA L | 0 | NR | 64.00 ± 13.75 | 26.00 ± 2.50 | 55.60 ± 12.00 | ||
| Nistor DV et al. [57] | 2017, Romania | 35 | 35 | 26 (74.29) | MI DAA | 0 | Supine | 67.00 ± 4.75 | 27.45 ± 3.76 | NR |
| 35 | 35 | 16 (45.71) | CA L | 0 | Supine | 64.00 ± 3.25 | 28.63 ± 3.12 | NR | ||
| Ouyang C et al. [58] | 2018, China | 12 | 12 | 8 (66.67) | MI S | NR | Lat | 54.00 ± 6.50 | 23.10 ± 2.30 | 45.67 ± 5.93 |
| 12 | 12 | 9 (75.00) | CA PL | NR | Lat | 55.00 ± 5.00 | 23.90 ± 3.38 | 46.92 ± 8.94 | ||
| Pan F et al. [59] | 2020, China | 58 | 58 | 34 (58.62) | MI S | NR | Lat | 65.23 ± 6.84 | 22.24 ± 4.15 | 83.85 ± 2.71 |
| 58 | 58 | 33 (56.90) | CA PL | NR | Lat | 65.62 ± 6.96 | 22.56 ± 4.22 | 84.02 ± 3.15 | ||
| Reichert et al. [60] | 2018, Germany | 77 | 77 | 45 (58.44) | MI DAA | 4 | Supine | 63.20 ± 8.20 | 28.10 ± 3.70 | 54.00 ± 14.20 |
| 71 | 71 | 39 (54.93) | CA L | 5 | Supine | 61.90 ± 7.80 | 28.30 ± 3.40 | 53.00 ± 15.70 | ||
| Ren D et al. [61] | 2016, China | 21 | 21 | 12 (57.14) | MI S | NR | NR | 57.96 ± 6.89 | NR | 35.35 ± 4.85 |
| 21 | 21 | 13 (61.90) | CA | NR | NR | 58.45 ± 6.25 | NR | 36.23 ± 3.54 | ||
| Restreppo C et al. [62] | 2010, USA | 50 | 50 | 17 (34.00) | MI DAA | 0 | Supine | 62.02 ± 12.38 | 25.18 ± 11.1 | 51.86 ± 7.88 |
| 50 | 50 | 22 (44.00) | CA L | 0 | Supine | 59.91 ± 9.00 | 25.17 ± 2.48 | 54.95 ± 5.53 | ||
| Rykov K et al. [63] | 2017, Netherlands | 23 | 23 | 8 (34.78) | MI DAA | 23 | Supine | 62.80 ± 6.10 | 29.00 ± 5.60 | 52.00 ± 6.67 |
| 23 | 23 | 11 (47.83) | CA PL | 23 | Lat | 60.20 ± 8.10 | 29.30 ± 4.80 | 51.00 ± 8.95 | ||
| Schwarze M et al. [64] | 2017, Germany | 22 | 22 | 13 (59.09) | MI AL | 0 | Supine | 59.00 ± 9.00 | 26.70 ± 4.20 | 53.00 ± 12.00 |
| 21 | 21 | 13 (61.90) | CA L | 0 | Supine | 59.00 ± 9.00 | 26.70 ± 4.20 | 59.00 ± 15.00 | ||
| Taunton M et al. [65] | 2014, USA | 27 | NR | 12 (44.44) | MI DAA | NR | Supine | 62.05 ± NR | 27.70 ± NR | 55.00 ± 4.25 |
| 27 | NR | 13 (48.15) | CA P | NR | Lat | 66.40 ± NR | 29.20 ± NR | 51.00 ± 6.00 | ||
| Taunton M et al. [66] | 2018, USA | 52 | 52 | 27 (51.92) | MI DAA | 0 | NR | 65.00 ± 10.00 | 29.00 ± 2.20 | 57.00 ± 13.00 |
| 49 | 49 | 25 (51.02) | CA P | 0 | NR | 64.00 ± 11.00 | 30.00 ± 4.00 | 56.00 ± 12.00 | ||
| Varela-Egocheaga JR et al. [67] | 2013, Spain | 25 | 25 | 12 (48.00) | MI L | 0 | NR | 64.80 ± 10.45 | 28.27 ± 3.67 | 52.70 ± 12.90 |
| 25 | 25 | 12 (48.00) | CA L | 0 | NR | 63.80 ± 9.70 | 27.78 ± 3.24 | 51.30 ± 14.90 | ||
| Wang Z et Ge W [68] | 2021, China | 43 | 43 | 26 (60.47) | MI S | NR | Supine | 71.53 ± 3.76 | 22.47 ± 1.12 | 62.18 ± 5.23 |
| 42 | 42 | 24 (57.14) | CA PL | NR | Lat | 71.58 ± 3.79 | 22.51 ± 1.15 | 62.65 ± 6.59 | ||
| Xiao C et al. [69] | 2021, China | 49 | 49 | 16 (32.65) | MI P | 0 | Lat | 71.06 ± 10.87 | 26.73 ± 4.18 | NR |
| 57 | 57 | 26 (45.61) | CA PL | 0 | Lat | 73.93 ± 10.02 | 26.39 ± 4.64 | NR | ||
| Xie J et al. [70] | 2017, China | 46 | 46 | 12 (26.09) | MI S | 0 | Lat | 66.60 ± 11.88 | 23.62 ± 1.63 | 28.90 ± 11.32 |
| 46 | 46 | 19 (41.30) | CA P | 0 | Lat | 64.47 ± 12.09 | 24.06 ± 2.72 | 29.30 ± 17.40 | ||
| Yan T et al. [71] | 2017, China | 64 | 70 | 29 (45.21) | MI S | NR | NR | 66.00 ± 4.00 | 24.50 ± 3.45 | 33.50 ± 5.30 |
| 90 | 103 | 42 (46.67) | CA L | NR | NR | 65.00 ± 6.50 | 23.60 ± 3.58 | 30.70 ± 7.60 | ||
| Yang C et al. [72] | 2010, China | 55 | 55 | 26 (47.27) | MI AL | 0 | Lat | 59.47 ± 13.24 | 23.12 ± 3.23 | 25.93 ± 11.30 |
| 55 | 55 | 30 (54.55) | CA PL | 0 | Lat | 55.82 ± 13.91 | 22.42 ± 3.95 | 28.18 ± 13.73 | ||
| Yuan H et al. [73] | 2018, China | 40 | 40 | 24 (60.00) | MI S | 0 | Lat | 74.30 ± 3.00 | 22.73 ± 1.71 | 33.00 ± 1.89 |
| 44 | 44 | 21 (47.72) | CA PL | 0 | Lat | 75.70 ± 3.25 | 22.36 ± 2.72 | 32.70 ± 1.32 | ||
| Zhang ZL et al. [74] | 2019, China | 27 | 27 | 10 (37.04) | MI S | NR | NR | 62.41 ± 6.44 | 24.53 ± 5.31 | 35.60 ± 8.80 |
| 27 | 27 | 12 (44.44) | CA PL | NR | NR | 61.28 ± 6.70 | 23.93 ± 4.89 | 36.20 ± 9.20 | ||
| Zhao HY et al. [75] | 2017, China | 60 | 60 | 24 (40.00) | MI DAA | NR | Supine | 64.88 ± 12.13 | 24.35 ± 3.10 | 40.19 ± 9.23 |
| 60 | 60 | 22 (36.67) | CA PL | NR | Lat | 62.18 ± 14.72 | 25.58 ± 2.83 | 43.11 ± 15.59 |
| RCT | Osteoarthritis, N | Femoral Neck Fracture, N | Dysplasia, N | ANFH, N | Operation Time, min., SD | Incision Length, cm, SD | Intraoperative Blood Loss, mL, SD | Acetabular Cup Inclination Angle, Degree, SD | CRP 1–3 Days Postoperatively, mg/L, SD | CK 1–3 Days Postoperatively, U/L, SD |
|---|---|---|---|---|---|---|---|---|---|---|
| Barrett WP et al. [35] | 43 | 0 | 0 | 0 | 84.30 ± 12.40 | 13.70 ± 0.90 | 391.00 ± 206.00 | 47.10 ± 6.10 | NR | NR |
| 44 | 0 | 0 | 0 | 60.50 ± 12.40 | 12.70 ± 1.30 | 191.00 ± 107.00 | 42.40 ± 7.60 | NR | NR | |
| Bon G et al. [36] | 50 | 0 | 0 | 0 | 70.10 ± 11.00 | NR | NR | 37.74 ± 4.20 | NR | NR |
| 50 | 0 | 0 | 0 | 56.70 ± 11.79 | NR | NR | 39.60 ± 6.87 | NR | NR | |
| Brismar BH et al. [37] | 50 | 0 | 0 | 0 | 101.00 ± NR | NR | 325.00 ± NR | NR | NR | NR |
| 50 | 0 | 0 | 0 | 80.00 ± NR | NR | 300.00 ± NR | NR | NR | NR | |
| Cheng TE et al. [38] | 35 | 0 | 0 | 0 | 125.00 ± NR | 10.70 ± 8.00 | NR | 46.20 ± NR | NR | NR |
| 37 | 0 | 0 | 0 | 100.00 ± NR | 13.50 ± 7.00 | NR | 45.90 ± NR | NR | NR | |
| D’Arrigo C et al. [39] | 20 | 0 | 0 | 0 | 121.00 ± 23.60 | NR | 1344.00 ± 710.00 | NR | NR | NR |
| 149 | 0 | 0 | 0 | 77.00 ± 15.10 | NR | 1644.00 ± 757.70 | NR | NR | NR | |
| De Anta-Diaz B et al. [40] | 49 | 0 | 0 | 0 | 78.20 ± 16.20 | 10.40 ± 0.90 | NR | NR | 11.40 ± 5.20 | 203.20 ± 53.70 |
| 50 | 0 | 0 | 0 | 82.20 ± 15.20 | 11.50 ± 0.70 | NR | NR | 14.40 ± 9.10 | 387.00 ± 174.00 | |
| Dienstknecht T et al. [41] * | 42 | 0 | 0 | 0 | 66.00 ± 27.00 | 13.00 ± 2.00 | 440.00 ± 821.00 | 49.20 ± 7.00 | 142.00 ± 56.00 | NR |
| 36 | 0 | 0 | 0 | 58.00 ± 15.00 | 9.00 ± 1.00 | 346.00 ± 170.00 | 48.20 ± 6.10 | 118.00 ± 53.00 | NR | |
| 41 | 0 | 0 | 0 | 70.00 ± 28.00 | 14.00 ± 3.00 | 383.00 ± 265.00 | 50.10 ± 5.00 | 149.00 ± 62.00 | NR | |
| 15 | 0 | 0 | 0 | 60.00 ± 9.00 | 9.00 ± 1.00 | 302.00 ± 138.00 | 48.10 ± 6.00 | 178.00 ± 115.00 | NR | |
| Fink B et al. [42] | 44 | 0 | 1 | 5 | 51.90 ± 11.40 | NR | 262.70 ± 149.70 | 43.70 ± 5.90 | NR | NR |
| 44 | 0 | 1 | 5 | 50.90 ± 10.20 | NR | 382.00 ± 179.90 | 42.80 ± 6.60 | NR | NR | |
| Gao P et Shi X [43] | 0 | 35 | 0 | 0 | 68.59 ± 5.37 | 7.41 ± 0.85 | 88.68 ± 6.04 | NR | NR | NR |
| 0 | 35 | 0 | 0 | 61.56 ± 6.02 | 14.55 ± 1.86 | 208.52 ± 4.61 | NR | NR | NR | |
| Hou JZ et al. [44] | 6 | 0 | 0 | 14 | 115.00 ± 10.09 | 7.20 ± 0.50 | 315.00 ± 116.00 | 43.90 ± 2.90 | NR | NR |
| 5 | 0 | 0 | 15 | 105.00 ± 15.40 | 15.00 ± 1.60 | 470.00 ± 127.10 | 44.70 ± 3.10 | NR | NR | |
| Huang K et al. [45] ** | 0 | 0 | 0 | 37 | 82.80 ± 14.30 | 7.62 ± 1.11 | 71.90 ± 17.90 | NR | NR | NR |
| 0 | 0 | 0 | 58 | 73.50 ± 23.20 | 10.64 ± 1.16 | 174.70 ± 50.50 | NR | NR | NR | |
| 0 | 16 | 0 | 0 | 83.70 ± 27.00 | 7.63 ± 1.20 | 72.50 ± 16.90 | NR | NR | NR | |
| 0 | 18 | 0 | 0 | 75.10 ± 19.80 | 10.33 ± 1.08 | 162.80 ± 48.50 | NR | NR | NR | |
| Khan RJK et al. [46] | 42 | 0 | 0 | 2 | 87.00 ± 2.97 | 12.60 ± 0.72 | NR | 41.80 ± 1.02 | 98.20 ± 53.50 | NR |
| 43 | 0 | 0 | 2 | 90.00 ± 2.12 | 19.30 ± 0.37 | NR | 45.30 ± 0.98 | 92.00 ± 47.25 | NR | |
| Li L [47] | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | |
| Ling Z et al. [48] | 0 | 50 | 0 | 0 | 118.25 ± 16.95 | 7.06 ± 0.99 | 185.47 ± 20.23 | NR | NR | NR |
| 0 | 50 | 0 | 0 | 68.81 ± 10.37 | 9.13 ± 1.18 | 388.95 ± 47.71 | NR | NR | NR | |
| Liu Y et al. [49] | 0 | 47 | 0 | 0 | NR | 7.32 ± 1.30 | 92.43 ± 7.14 | NR | NR | NR |
| 0 | 47 | 0 | 0 | NR | 13.30 ± 2.46 | 195.83 ± 18.99 | NR | NR | NR | |
| Liu W et al. [50] | 3 | 13 | 0 | 14 | 88.83 ± 7.36 | 7.83 ± 0.36 | 203.03 ± 23.14 | NR | NR | NR |
| 6 | 9 | 0 | 15 | 90.29 ± 7.27 | 12.29 ± 1.27 | 387.49 ± 24.25 | NR | NR | NR | |
| Martin R et al. [51] | 37 | 0 | 0 | 5 | 114.12 ± 21.47 | 9.50 ± 1.40 | NR | NR | 14.20 ± 7.40 | NR |
| 37 | 0 | 0 | 4 | 95.78 ± 18.53 | 14.80 ± 3.30 | NR | NR | 13.80 ± 5.70 | NR | |
| Meng W et al. [52] | 0 | 0 | 0 | 4 | 103.25 ± 12.41 | 7.62 ± 0.97 | 1108.50 ± 163.63 | 38.75 ± 8.21 | NR | NR |
| 0 | 0 | 0 | 4 | 66.50 ± 13.79 | 11.12 ± 1.21 | 843.50 ± 111.60 | 44.50 ± 3.64 | NR | NR | |
| Mjaaland KE et al. [53] *** | 83 | 0 | 0 | 0 | 77.00 ± 21.00 | 9.50 ± 1.25 | NR | NR | 47.50 ± 39.30 | 989.50 ± 446.70 |
| 80 | 0 | 0 | 0 | 62.00 ± 10.75 | 13.50 ± 1.25 | NR | NR | 50.00 ± 41.50 | 965.80 ± 467.80 | |
| Mjaaland KE et al. [54] *** | 83 | 0 | 0 | 0 | NR | NR | NR | NR | NR | NR |
| 80 | 0 | 0 | 0 | NR | NR | NR | NR | NR | NR | |
| Moerenhout K et al. [55] | NR | 0 | 0 | NR | 59.90 ± 12.70 | NR | NR | 43.30 ± 8.40 | NR | NR |
| NR | 0 | 0 | NR | 45.70 ± 17.90 | NR | NR | 39.80 ± 5.40 | NR | NR | |
| Müller M et al. [56] | 21 | 0 | 0 | 0 | 51.00 ± 6.80 | 8.00 ± 1.60 | NR | NR | NR | NR |
| 16 | 0 | 0 | 0 | 50.00 ± 7.40 | 10.40 ± 2.00 | NR | NR | NR | NR | |
| Nistor DV et al. [57] | 35 | 0 | 0 | 0 | 70.00 ± 1.25 | 12.18 ± 1.91 | NR | 36.97 ± 1.85 | NR | 469.00 ± 83.00 |
| 35 | 0 | 0 | 0 | 70.00 ± 3.75 | 14.79 ± 2.25 | NR | 39.63 ± 2.88 | NR | 357.00 ± 56.25 | |
| Ouyang C et al. [58] | 5 | 0 | 0 | 7 | 109.60 ± 28.30 | 10.40 ± 3.00 | 138.33 ± 42.82 | 37.08 ± 6.53 | 63.27 ± 49.43 | 661.75 ± 261.01 |
| 6 | 0 | 0 | 6 | 67.50 ± 16.20 | 12.50 ± 1.40 | 141.67 ± 35.89 | 39.67 ± 6.95 | 87.55 ± 38.94 | 1035.25 ± 540.62 | |
| Pan F et al. [59] | 12 | 26 | NR | 15 | 92.58 ± 12.35 | 7.51 ± 0.82 | NR | NR | NR | NR |
| 11 | 25 | NR | 18 | 125.32 ± 12.63 | 15.23 ± 2.14 | NR | NR | NR | NR | |
| Reichert et al. [60] | 77 | 0 | 0 | 0 | NR | NR | NR | 38.60 ± 5.70 | NR | NR |
| 71 | 0 | 0 | 0 | NR | NR | NR | 40.28 ± 6.20 | NR | NR | |
| Ren D et al. [61] | 0 | 0 | 0 | 21 | NR | NR | NR | NR | NR | NR |
| 0 | 0 | 0 | 21 | NR | NR | NR | NR | NR | NR | |
| Restreppo C et al. [62] | 50 | 0 | 0 | 0 | 56.42 ± 13.75 | NR | 172.50 ± 137.50 | NR | NR | NR |
| 50 | 0 | 0 | 0 | 54.88 ± 16.00 | NR | 170.00 ± 112.50 | NR | NR | NR | |
| Rykov K et al. [63] | 23 | 0 | 0 | 0 | 71.00 ± 7.00 | NR | 325.70 ± 99.74 | NR | NR | NR |
| 23 | 0 | 0 | 0 | 62.00 ± 7.00 | NR | 273.70 ± 181.00 | NR | NR | NR | |
| Schwarze M et al. [64] | 22 | 0 | 0 | 0 | 70.00 ± 20.00 | NR | NR | NR | NR | NR |
| 21 | 0 | 0 | 0 | 67.00 ± 18.00 | NR | NR | NR | NR | NR | |
| Taunton M et al. [65] | 27 | 0 | 0 | 0 | NR | NR | NR | 38.00 ± 1.25 | NR | NR |
| 27 | 0 | 0 | 0 | NR | NR | NR | 40.00 ± 1.50 | NR | NR | |
| Taunton M et al. [66] | 52 | 0 | 0 | 0 | NR | NR | NR | 37.00 ± 5.00 | NR | NR |
| 49 | 0 | 0 | 0 | NR | NR | NR | 39.00 ± 6.00 | NR | NR | |
| Varela-Egocheaga JR et al. [67] | 21 | 0 | 0 | 4 | 62.04 ± NR | NR | NR | 43.70 ± NR | NR | NR |
| 22 | 0 | 0 | 3 | 60.60 ± NR | NR | NR | 45.30 ± NR | NR | NR | |
| Wang Z et Ge W [68] | 0 | 43 | 0 | 0 | 105.79 ± 18.75 | 8.26 ± 1.02 | 89.47 ± 9.32 | NR | NR | NR |
| 0 | 42 | 0 | 0 | 73.16 ± 9.82 | 11.19 ± 0.93 | 253.86 ± 42.58 | NR | NR | NR | |
| Xiao C et al. [69] | 0 | 49 | 0 | 0 | 84.47 ± 19.37 | 9.10 ± 0.94 | NR | NR | 97.21 ± 39.27 | 370.23 ± 249.37 |
| 0 | 57 | 0 | 0 | 105.44 ± 10.50 | 15.56 ± 1.20 | NR | NR | 113.29 ± 4.98 | 504.62 ± 21.88 | |
| Xie J et al. [70] | 46 | 0 | 0 | 0 | 103.60 ± 11.80 | 7.40 ± 1.06 | 303.60 ± 106.30 | 43.60 ± 6.80 | NR | NR |
| 46 | 0 | 0 | 0 | 106.50 ± 16.50 | 14.50 ± 2.38 | 326.40 ± 127.20 | 44.50 ± 6.50 | NR | NR | |
| Yan T et al. [71] | 14 | 11 | 0 | 39 | 52.00 ± 5.00 | 5.80 ± 0.60 | 349.00 ± 28.00 | 38.90 ± 2.60 | NR | NR |
| 12 | 23 | 0 | 55 | 36.00 ± 15.00 | 14.30 ± 1.20 | 165.00 ± 70.00 | 39.50 ± 0.40 | NR | NR | |
| Yang C et al. [72] | 12 | 11 | 0 | 32 | 77.55 ± 13.39 | 7.49 ± 0.86 | 376.18 ± 168.30 | 48.30 ± 5.30 | NR | NR |
| 19 | 13 | 0 | 23 | 73.67 ± 14.51 | 15.19 ± 1.82 | 605.00 ± 225.12 | 48.90 ± 6.60 | NR | NR | |
| Yuan H et al. [73] | 5 | 21 | 4 | 10 | 57.50 ± 5.66 | 7.50 ± 1.13 | 175.00 ± 11.32 | NR | NR | NR |
| 6 | 24 | 2 | 12 | 63.64 ± 6.50 | 10.73 ± 1.30 | 209.09 ± 16.96 | NR | NR | NR | |
| Zhang ZL et al. [74] | 7 | 0 | 5 | 15 | NR | NR | NR | NR | NR | NR |
| 9 | 0 | 4 | 14 | NR | NR | NR | NR | NR | NR | |
| Zhao HY et al. [75] | 41 | 0 | 6 | 13 | 83.26 ± 6.69 | 9.09 ± 0.45 | 165.89 ± 42.60 | 40.30 ± 2.80 | NR | NR |
| 40 | 0 | 7 | 13 | 65.48 ± 13.32 | 13.14 ± 0.31 | 123.84 ± 56.83 | 41.80 ± 3.40 | NR | NR |
| RCT | Bias Arising from the Randomization Process | Bias Due to Deviation from Intended Interventions | Bias Due to Missing Outcome Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Result | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Barrett WP et al. [35] | + | − | ? | ? | + | − |
| Bon G et al. [36] | + | + | + | + | + | + |
| Brismar BH et al. [37] | + | + | − | + | + | − |
| Cheng TE et al. [38] | + | + | − | + | + | − |
| D’Arrigo C et al. [39] | + | + | + | + | + | + |
| De Anta-Diaz B et al. [40] | − | + | + | + | + | − |
| Dienstknecht T et al. [41] | − | + | + | + | + | − |
| Fink B et al. [42] | + | + | + | + | + | + |
| Gao P and Shi X [43] | + | ? | − | + | + | − |
| Hou JZ et al. [44] | + | ? | + | + | + | ? |
| Huang K et al. [45] | − | ? | + | + | + | − |
| Khan RJK et al. [46] | + | + | + | + | + | + |
| Li L [47] | + | ? | − | − | + | − |
| Ling Z et al. [48] | ? | + | − | + | + | − |
| Liu Y et al. [49] | + | + | − | + | + | − |
| Liu W et al. [50] | + | + | + | + | + | + |
| Martin R et al. [51] | ? | ? | + | + | ? | ? |
| Meng W et al. [52] | + | + | + | + | + | + |
| Mjaaland KE et al. [53] | + | + | + | + | + | + |
| Mjaaland KE et al. [54] | + | + | + | + | + | + |
| Moerenhout K et al. [55] | + | + | + | + | + | + |
| Müller M et al. [56] | + | + | ? | ? | + | ? |
| Nistor DV et al. [57] | − | + | + | + | + | − |
| Ouyang C et al. [58] | + | + | + | + | + | + |
| Pan F et al. 2020 [59] | + | ? | − | + | + | − |
| Reichert JC et al. [60] | − | + | + | + | + | − |
| Ren D et al. [61] | + | ? | − | ? | ? | − |
| Restreppo C et al. [62] | + | + | + | + | + | + |
| Rykov K et al. [63] | + | + | − | + | + | − |
| Schwarze M et al. [64] | ? | ? | − | − | + | − |
| Taunton M et al. [65] | + | + | ? | + | + | ? |
| Taunton M et al. [66] | + | + | ? | + | + | ? |
| Varela-Egocheaga JR et al. [67] | − | − | + | + | + | − |
| Wang Z and Ge W [68] | + | ? | − | + | + | − |
| Xiao C et al. [69] | ? | + | + | + | + | ? |
| Xie J et al. [70] | + | + | + | + | + | + |
| Yan T et al. [71] | + | ? | ? | + | + | ? |
| Yang C et al. [72] | + | + | + | + | + | + |
| Yuan H et al. [73] | + | ? | − | + | + | − |
| Zhang ZL et al. [74] | + | + | ? | + | + | ? |
| Zhao HY et al. [75] | + | + | + | + | + | + |
| Number of RCTs | Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Quality of Evidence |
|---|---|---|---|---|---|---|---|
| HHS ≤ 3 months postoperatively | |||||||
| 32 | RCT | Serious | Serious | No serious indirectness | Serious | In some cases, SD was calculated via imputation | Low |
| HHS ≥ 6 months postoperatively | |||||||
| 21 | RCT | Serious | No serious inconsistency | No serious indirectness | No serious imprecision | - | Moderate |
| Complication rate | |||||||
| 23 | RCT | Serious | Serious | No serious indirectness | No serious imprecision | - | Low |
| Outcome | Predictor | Number of RCTs | Number of THAs | I2 | Tau2 | QE.p.val | Predictor.Estimate | Predictor.p.val |
|---|---|---|---|---|---|---|---|---|
| HHS ≤ 3 months postoperatively | Patient age | 32 | 2690 | 97.16 | 19.69 | <0.01 | 0.06 | 0.71 |
| BMI | 27 | 2305 | 95.47 | 17.40 | <0.01 | −0.22 | 0.54 | |
| Preoperative HHS | 31 | 2584 | 95.14 | 19.56 | <0.01 | −0.06 | 0.33 | |
| Sex | 32 | 2690 | 96.54 | 18.51 | <0.01 | 0.13 | 0.16 | |
| Osteoarthritis | 30 | 2575 | 97.54 | 20.72 | <0.01 | −0.02 | 0.46 | |
| Femoral neck fracture | 31 | 2630 | 96.61 | 18.97 | <0.01 | 0.03 | 0.16 | |
| Dysplasia | 12 | 820 | 79.58 | 4.12 | <0.01 | 0.05 | 0.75 | |
| ANFH | 30 | 2575 | 97.24 | 20.91 | <0.01 | −0.02 | 0.59 | |
| Surgical approach | 32 | 2690 | 96.09 | 19.02 | <0.01 | 1.86 | 0.27 | |
| Operation time | 25 | 2137 | 97.43 | 23.12 | <0.01 | 0.05 | 0.40 | |
| Incision length | 19 | 1668 | 98.20 | 31.16 | <0.01 | −0.34 | 0.79 | |
| Intraoperative blood loss | 18 | 1625 | 97.70 | 29.86 | <0.01 | −0.01 | 0.31 | |
| Cup inclination | 15 | 1296 | 91.17 | 25.12 | <0.01 | 0.27 | 0.52 | |
| CRP 1–3 days postoperatively | 4 | 363 | 30.24 | 1.22 | 0.53 | −0.02 | 0.35 | |
| CK 1–3 days postoperatively | 3 | 229 | 8.63 | 0.17 | 0.53 | 0.01 | 0.49 | |
| Use of bone cement | 17 | 1561 | 94.47 | 7.59 | <0.01 | −0.01 | 0.74 | |
| HHS ≥ 6 months postoperatively | Patient age | 21 | 1698 | 70.57 | 2.31 | <0.01 | 0.14 | 0.01 * |
| BMI | 19 | 1538 | 60.08 | 1.42 | 0.57 | 0.19 | 0.12 | |
| Preoperative HHS | 21 | 1698 | 75.37 | 3.20 | <0.01 | 0.01 | 0.91 | |
| Sex | 21 | 1698 | 73.45 | 2.95 | <0.01 | 0.07 | 0.18 | |
| Osteoarthritis | 19 | 1583 | 71.71 | 2.57 | 0.01 | 0.01 | 0.69 | |
| Femoral neck fracture | 20 | 1638 | 68.33 | 2.22 | 0.01 | 0.02 | 0.13 | |
| Dysplasia | 12 | 814 | 71.47 | 3.12 | 0.01 | −0.10 | 0.40 | |
| ANFH | 19 | 1583 | 68.11 | 2.02 | 0.01 | −0.03 | 0.04 * | |
| Surgical approach | 21 | 1698 | 77.47 | 3.21 | <0.01 | −0.09 | 0.93 | |
| Operation time | 16 | 1281 | 76.57 | 3.29 | 0.01 | −0.01 | 0.75 | |
| Incision length | 13 | 1133 | 70.34 | 1.86 | 0.03 | −0.82 | 0.03 * | |
| Intraoperative blood loss | 9 | 798 | 83.27 | 3.08 | 0.01 | −0.01 | 0.63 | |
| Cup inclination | 12 | 1022 | 32.72 | 0.63 | 0.79 | −0.08 | 0.39 | |
| CRP 1–3 days postoperatively | 3 | 206 | 7.65 | 0.54 | 0.51 | −0.03 | 0.44 | |
| CK 1–3 days postoperatively | 2 | 123 | N/A ** | N/A ** | N/A ** | N/A ** | N/A ** | |
| Use of bone cement | 12 | 989 | 69.44 | 2.22 | 0.12 | −0.02 | 0.48 | |
| Complication rate | Patient age | 23 | 2152 | 62.37 | 1.90 | 0.01 | −0.10 | 0.06 |
| BMI | 21 | 1958 | 63.03 | 2.02 | 0.01 | 0.12 | 0.50 | |
| Preoperative HHS | 18 | 1721 | 52.28 | 1.27 | 0.02 | 0.01 | 0.74 | |
| Sex | 23 | 2152 | 65.41 | 2.14 | <0.01 | −0.04 | 0.32 | |
| Osteoarthritis | 22 | 2097 | 61.38 | 1.79 | 0.01 | 0.02 | 0.02 * | |
| Femoral neck fracture | 23 | 2152 | 59.92 | 1.71 | 0.01 | −0.02 | 0.02 * | |
| Dysplasia | 11 | 859 | 32.41 | 0.60 | 0.38 | −0.01 | 0.97 | |
| ANFH | 22 | 2097 | 68.06 | 2.34 | <0.01 | −0.01 | 0.98 | |
| Surgical approach | 23 | 2152 | 60.78 | 1.76 | 0.01 | −1.72 | 0.02 * | |
| Operation time | 17 | 1538 | 68.71 | 2.46 | <0.01 | 0.02 | 0.31 | |
| Incision length | 13 | 1108 | 73.49 | 2.95 | <0.01 | 0.27 | 0.39 | |
| Intraoperative blood loss | 12 | 1130 | 43.77 | 1.02 | 0.30 | 0.01 | 0.08 | |
| Cup inclination | 15 | 1286 | 63.82 | 2.35 | 0.01 | 0.01 | 0.94 | |
| CRP 1–3 days postoperatively | 3 | 247 | 12.64 | 0.21 | 0.48 | −0.01 | 0.55 | |
| CK 1–3 days postoperatively | 2 | 94 | N/A ** | N/A ** | N/A ** | N/A ** | N/A ** | |
| Use of bone cement | 13 | 1408 | 49.33 | 1.15 | 0.10 | 0.01 | 0.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramadanov, N.; Ostojic, M.; Lazaru, P.; Liu, K.; Hable, R.; Marinova-Kichikova, P.; Dimitrov, D.; Becker, R. Risk Factors and Predictors for Functional Outcome and Complication Rate in Total Hip Arthroplasty through Minimally Invasive and Conventional Approaches: A Systematic Review and Meta-Regression Analysis of 41 Randomized Controlled Trials. J. Clin. Med. 2023, 12, 5895. https://doi.org/10.3390/jcm12185895
Ramadanov N, Ostojic M, Lazaru P, Liu K, Hable R, Marinova-Kichikova P, Dimitrov D, Becker R. Risk Factors and Predictors for Functional Outcome and Complication Rate in Total Hip Arthroplasty through Minimally Invasive and Conventional Approaches: A Systematic Review and Meta-Regression Analysis of 41 Randomized Controlled Trials. Journal of Clinical Medicine. 2023; 12(18):5895. https://doi.org/10.3390/jcm12185895
Chicago/Turabian StyleRamadanov, Nikolai, Marko Ostojic, Philip Lazaru, Kuiliang Liu, Robert Hable, Polina Marinova-Kichikova, Dobromir Dimitrov, and Roland Becker. 2023. "Risk Factors and Predictors for Functional Outcome and Complication Rate in Total Hip Arthroplasty through Minimally Invasive and Conventional Approaches: A Systematic Review and Meta-Regression Analysis of 41 Randomized Controlled Trials" Journal of Clinical Medicine 12, no. 18: 5895. https://doi.org/10.3390/jcm12185895
APA StyleRamadanov, N., Ostojic, M., Lazaru, P., Liu, K., Hable, R., Marinova-Kichikova, P., Dimitrov, D., & Becker, R. (2023). Risk Factors and Predictors for Functional Outcome and Complication Rate in Total Hip Arthroplasty through Minimally Invasive and Conventional Approaches: A Systematic Review and Meta-Regression Analysis of 41 Randomized Controlled Trials. Journal of Clinical Medicine, 12(18), 5895. https://doi.org/10.3390/jcm12185895