
The Mechanism of Effort Intolerance in Patients with Peripheral Arterial Disease: A Combined Stress Echocardiography and Cardiopulmonary Exercise Test
 , , , ,
, , , , 

Abstract
:1. Introduction
2. Methods
2.1. Study Cohort
2.2. Study Protocol
2.3. Cardiopulmonary Exercise Test
2.4. Stress Echocardiography
3. Statistical Analysis
4. Results
5. Discussion
5.1. Diastolic Dysfunction
5.2. Peripheral Oxygen Extraction
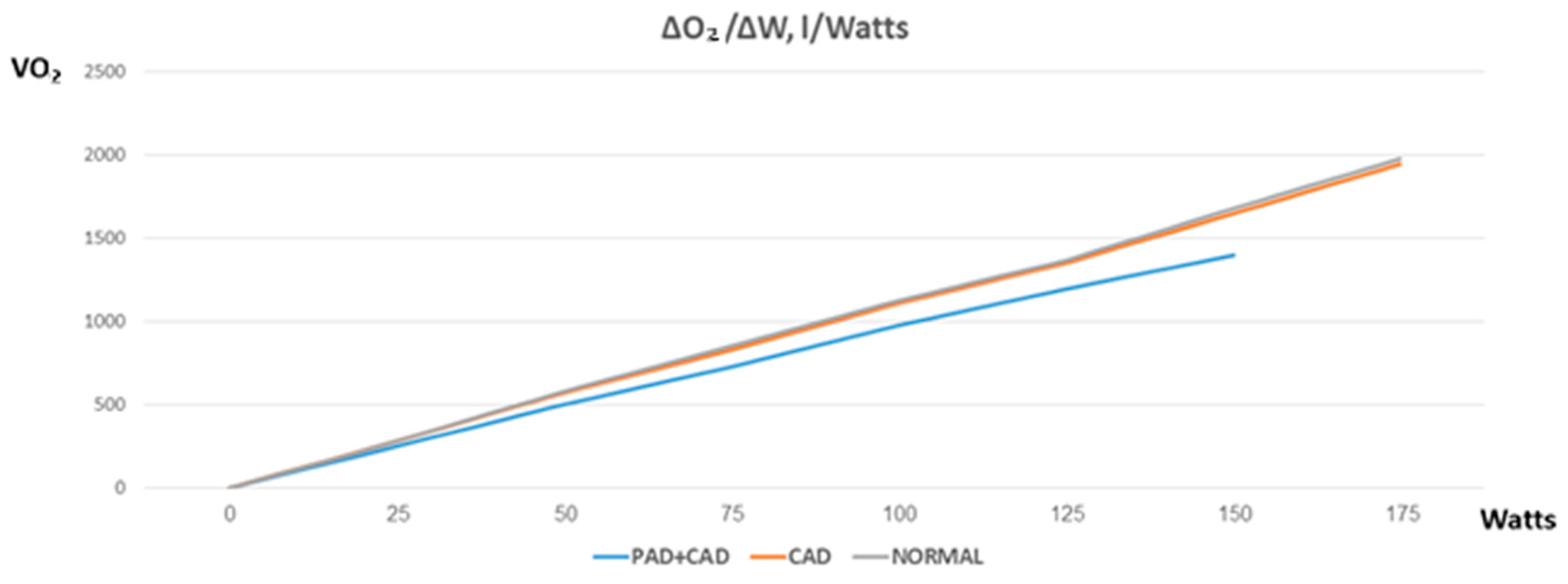
5.3. Mechanical Efficiency
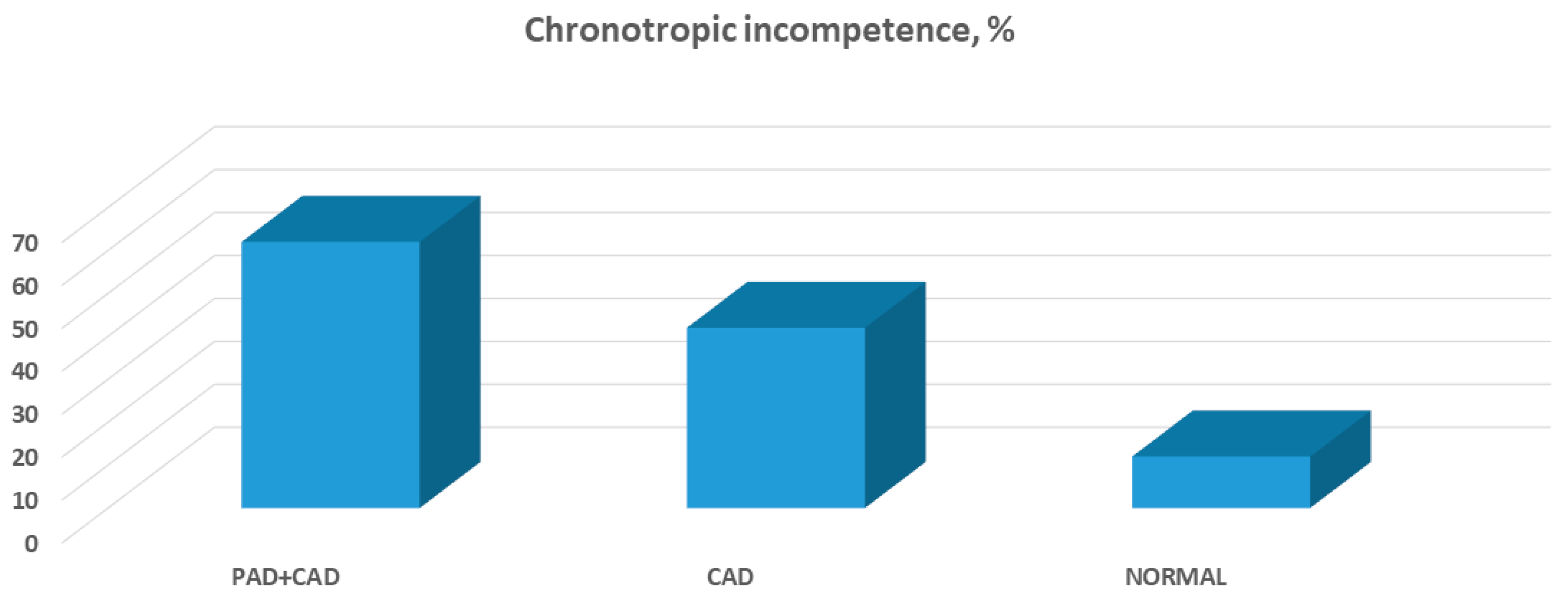
5.4. Chronotropic Incompetence
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar]
- Calvet, D.; Touze, E.; Varenne, O.; Sablayrolles, J.L.; Weber, S.; Mas, J.L. Prevalence of asymptomatic coronary artery disease in ischemic stroke patients: The PRECORIS study. Circulation 2010, 121, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Vidakovic, R.; Schouten, O.; Kuiper, R.; Hoeks, S.E.; Flu, W.J.; van Kuijk, J.P.; Goei, D.; Verhagen, H.J.; Neskovic, A.N.; Poldermans, D. The prevalence of polyvascular disease in patients referred for peripheral arterial disease. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 435–440. [Google Scholar] [CrossRef]
- Belardinelli, R.; Lacalaprice, F.; Carle, F.; Minnucci, A.; Cianci, G.; Perna, G.; D’Eusanio, G. Exercise-induced myocardial ischaemia detected by cardiopulmonary exercise testing. Eur. Heart J. 2003, 24, 1304–1313. [Google Scholar] [CrossRef]
- Coeckelberghs, E.; Buys, R.; Goetschalckx, K.; Cornelissen, V.A.; Vanhees, L. Prognostic value of the oxygen uptake efficiency slope and other exercise variables in patients with coronary artery disease. Eur. J. Prev. Cardiol. 2016, 23, 237–244. [Google Scholar] [CrossRef]
- Shimiaie, J.; Sherez, J.; Aviram, G.; Megidish, R.; Viskin, S.; Halkin, A.; Ingbir, M.; Nesher, N.; Biner, S.; Keren, G.; et al. Determinants of Effort Intolerance in Patients With Heart Failure: Combined Echocardiography and Cardiopulmonary Stress Protocol. JACC Heart Fail. 2015, 3, 803–814. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. European Association for Cardiovascular P, Rehabilitation and American Heart A. EACPR/AHA Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef] [PubMed]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic incompetence: Causes, consequences, and management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef]
- Haykowsky, M.J.; Brubaker, P.H.; Stewart, K.P.; Morgan, T.M.; Eggebeen, J.; Kitzman, D.W. Effect of endurance training on the determinants of peak exercise oxygen consumption in elderly patients with stable compensated heart failure and preserved ejection fraction. J. Am. Coll Cardiol. 2012, 60, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Momsen, A.H.; Jensen, M.B.; Norager, C.B.; Madsen, M.R.; Vestersgaard-Andersen, T.; Lindholt, J.S. Drug therapy for improving walking distance in intermittent claudication: A systematic review and meta-analysis of robust randomised controlled studies. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Al-Jundi, W.; Madbak, K.; Beard, J.D.; Nawaz, S.; Tew, G.A. Systematic review of home-based exercise programmes for individuals with intermittent claudication. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 690–706. [Google Scholar] [CrossRef] [PubMed]
- Lane, R.; Ellis, B.; Watson, L.; Leng, G.C. Exercise for intermittent claudication. Cochrane Database Syst. Rev. 2014, CD000990. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, R.; Kypta, A.; Steinwender, C.; Kerschner, K.; Grund, M.; Leisch, F. Coronary angiography in patients undergoing carotid artery stenting shows a high incidence of significant coronary artery disease. Heart 2005, 91, 1438–1441. [Google Scholar] [CrossRef]
- Yamasaki, S.; Izawa, A.; Shiba, Y.; Tomita, T.; Miyashita, Y.; Koyama, J.; Ikeda, U. Presence of diastolic dysfunction in patients with peripheral artery disease. Angiology 2013, 64, 540–543. [Google Scholar] [CrossRef]
- Obokata, M.; Kane, G.C.; Reddy, Y.N.; Olson, T.P.; Melenovsky, V.; Borlaug, B.A. Role of Diastolic Stress Testing in the Evaluation for Heart Failure with Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study. Circulation 2017, 135, 825–838. [Google Scholar] [CrossRef]
- Taqueti, V.R.; Solomon, S.D.; Shah, A.M.; Desai, A.S.; Groarke, J.D.; Osborne, M.T.; Hainer, J.; Bibbo, C.F.; Dorbala, S.; Blankstein, R.; et al. Coronary microvascular dysfunction and future risk of heart failure with preserved ejection fraction. Eur. Heart J. 2018, 39, 840–849. [Google Scholar] [CrossRef]
- Tanabe, Y.; Nakagawa, I.; Ito, E.; Suzuki, K. Hemodynamic basis of the reduced oxygen uptake relative to work rate during incremental exercise in patients with chronic heart failure. Int. J. Cardiol. 2002, 83, 57–62. [Google Scholar] [CrossRef]
- McDermott, M.M.; Ferrucci, L.; Gonzalez-Freire, M.; Kosmac, K.; Leeuwenburgh, C.; Peterson, C.A.; Saini, S.; Sufit, R. Skeletal Muscle Pathology in Peripheral Artery Disease: A Brief Review. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2577–2585. [Google Scholar] [CrossRef]
- Beckman, J.A.; Duncan, M.S.; Damrauer, S.M.; Wells, Q.S.; Barnett, J.V.; Wasserman, D.H.; Bedimo, R.J.; Butt, A.A.; Marconi, V.C.; Sico, J.J.; et al. Microvascular Disease, Peripheral Artery Disease, and Amputation. Circulation 2019, 140, 449–458. [Google Scholar] [CrossRef]
- Rossi, M.; Carpi, A. Skin microcirculation in peripheral arterial obliterative disease. Biomed. Pharmacother. 2004, 58, 427–431. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Hoff, F.; Ferrucci, L.; Pearce, W.H.; Guralnik, J.M.; Tian, L.; Liu, K.; Schneider, J.R.; Sharma, L.; Tan, J.; et al. Lower extremity ischemia, calf skeletal muscle characteristics, and functional impairment in peripheral arterial disease. J. Am. Geriatr. Soc. 2007, 55, 400–406. [Google Scholar] [CrossRef]
- Kosmac, K.; Gonzalez-Freire, M.; McDermott, M.M.; White, S.H.; Walton, R.G.; Sufit, R.L.; Tian, L.; Li, L.; Kibbe, M.R.; Criqui, M.H.; et al. Correlations of Calf Muscle Macrophage Content with Muscle Properties and Walking Performance in Peripheral Artery Disease. J. Am. Heart Assoc. 2020, 9, e015929. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Chuang, W.Y.; Wei, F.C.; Yeh, C.H.; Tinhofer, I.; Al Deek, N.F.; Fu, T.C.; Ng, S.C.; Chang, T.C.; Cheung, Y.C.; et al. Peripheral arterial disease: The role of extracellular volume measurements in lower limb muscles with MRI. Eur. Radiol. 2020, 30, 3943–3950. [Google Scholar] [CrossRef] [PubMed]
- Pipinos, I.I.; Shepard, A.D.; Anagnostopoulos, P.V.; Katsamouris, A.; Boska, M.D. Phosphorus 31 nuclear magnetic resonance spectroscopy suggests a mitochondrial defect in claudicating skeletal muscle. J. Vasc. Surg. 2000, 31, 944–952. [Google Scholar] [CrossRef]
- Zweerink, A.; van der Lingen, A.C.J.; Handoko, M.L.; van Rossum, A.C.; Allaart, C.P. Chronotropic Incompetence in Chronic Heart Failure. Circ. Heart Fail. 2018, 11, e004969. [Google Scholar] [CrossRef]
- Topilsky, Y.; Rozenbaum, Z.; Khoury, S.; Pressman, G.S.; Gura, Y.; Sherez, J.; Man, A.; Shimiaie, J.; Edwards, S.; Berookhim, J.; et al. Mechanisms of Effort Intolerance in Patients with Heart Failure and Borderline Ejection Fraction. Am. J. Cardiol. 2017, 119, 416–422. [Google Scholar] [CrossRef]
- Haykowsky, M.J.; Brubaker, P.H.; John, J.M.; Stewart, K.P.; Morgan, T.M.; Kitzman, D.W. Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction. J. Am. Coll Cardiol. 2011, 58, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Melenovsky, V.; Russell, S.D.; Kessler, K.; Pacak, K.; Becker, L.C.; Kass, D.A. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 2006, 114, 2138–2147. [Google Scholar] [CrossRef]
- Stone, A.J.; Kaufman, M.P. The exercise pressor reflex and peripheral artery disease. Auton. Neurosci. 2015, 188, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xing, J. Muscle afferent receptors engaged in augmented sympathetic responsiveness in peripheral artery disease. Front. Physiol. 2012, 3, 247. [Google Scholar] [CrossRef] [PubMed]
- Lane, R.; Harwood, A.; Watson, L.; Leng, G.C. Exercise for intermittent claudication. Cochrane Database Syst. Rev. 2017, 12, CD000990. [Google Scholar] [CrossRef] [PubMed]
- Harwood, A.E.; Smith, G.E.; Cayton, T.; Broadbent, E.; Chetter, I.C. A Systematic Review of the Uptake and Adherence Rates to Supervised Exercise Programs in Patients with Intermittent Claudication. Ann. Vasc. Surg. 2016, 34, 280–289. [Google Scholar] [CrossRef]
- Pymer, S.; Harwood, A.; Ibeggazene, S.; McGregor, G.; Huang, C.; Twiddy, M.; Nicholls, A.R.; Ingle, L.; Carroll, S.; Long, J.; et al. High INtensity Interval Training In pATiEnts with intermittent claudication (INITIATE): Protocol for a multicentre, proof-of-concept, prospective interventional study. BMJ Open 2020, 10, e038825. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N. Engl. J. Med. 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Godo, S.; Suda, A.; Takahashi, J.; Yasuda, S.; Shimokawa, H. Coronary Microvascular Dysfunction. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1625–1637. [Google Scholar] [CrossRef]
- Bairey Merz, C.N.; Pepine, C.J.; Shimokawa, H.; Berry, C. Treatment of coronary microvascular dysfunction. Cardiovasc. Res. 2020, 116, 856–870. [Google Scholar] [CrossRef]
- de Borba, A.T.; Jost, R.T.; Gass, R.; Nedel, F.B.; Cardoso, D.M.; Pohl, H.H.; Reckziegel, M.B.; Corbellini, V.A.; Paiva, D.N. The influence of active and passive smoking on the cardiorespiratory fitness of adults. Multidiscip. Respir. Med. 2014, 9, 34. [Google Scholar] [CrossRef]
- Lauria, V.T.; Sperandio, E.F.; de Sousa, T.L.W.; de Oliveira Vieira, W.; Romiti, M.; de Toledo Gagliardi, A.R.; Arantes, R.L.; Dourado, V.Z. Evaluation of dose–response relationship between smoking load and cardiopulmonary fitness in adult smokers: A cross-sectional study. Pulmonology 2017, 23, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Adatia, A.; Wahab, M.; Shahid, I.; Moinuddin, A.; Killian, K.J.; Satia, I. Effects of cigarette smoke exposure on pulmonary physiology, muscle strength and exercise capacity in a retrospective cohort with 30,000 subjects. PLoS ONE 2021, 16, e0250957. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| PAD + CAD n = 23 | CAD n = 24 | Normal Controls n = 15 | p Value PAD + CAD vs. CAD | p Value PAD + CAD vs. Normal | |
|---|---|---|---|---|---|
| Age, years | 74.5 ± 7.1 | 72.9 ± 6.8 | 74 ± 7.7 | 0.21 | 0.86 |
| Male, % | 82 | 83 | 75 | 0.77 | 0.19 |
| PAD involvement, %: | |||||
| CAS | 26 | NA | NA | NA | NA |
| AAA | 13 | ||||
| Ilio-femoral Rev. | 48 | ||||
| Low ABI | 74 | ||||
| Extent of CAD, %: | NA | 0.11 | NA | ||
| 1-vessel disease | 26 | 25 | |||
| 2-vessel disease | 61 | 69 | |||
| LM or 3-vessel disease | 13 | 6 | |||
| SBP, mmHg | 141 ± 8 | 138 ± 8 | 133 ± 11 | 0.26 | 0.03 |
| Heart rate, bpm | 71.1 ± 4.3 | 72.5 ± 5 | 78.7 ± 7.2 | 0.82 | 0.10 |
| BMI, kg/m2 | 27.8 ± 5.2 | 27.3 ± 5.1 | 28.8 | 0.47 | 0.31 |
| Current smoker, % | 31 | 14 | 17 | 0.01 | 0.042 |
| Past smoker, % | 61 | 17 | 19 | <0.001 | <0.001 |
| Hypertension, % | 71 | 74 | 65 | 0.56 | 0.33 |
| Diabetes mellitus, % | 31 | 28 | 22 | 0.33 | 0.06 |
| Hyperlipidemia, % | 85 | 87 | 47 | 0.78 | 0.012 |
| Atrial fibrillation, % | 21 | 14 | 15 | 0.11 | 0.085 |
| Creatinine, mg/dL | 1.23 ± 0.46 | 1.07 ± 0.27 | 1.13 ± 0.39 | 0.29 | 0.2 |
| Hemoglobin, g/dL | 15.1 ± 2.1 | 14.7 ± 1.8 | 14.1 ± 2.7 | 0.29 | 0.31 |
| Beta-blockers, % | 76 | 68 | 26 | 0.22 | 0.0014 |
| ACEI, % | 60 | 65 | 68 | 0.2 | 0.26 |
| Antiplatelet, % | 88 | 92 | 12 | 0.6 | <0.001 |
| Statins, % | 92 | 97 | 40 | 0.73 | <0.001 |
| EDV index, mL/m2 | 68 ± 9 | 67.1 ± 10.6 | 67.5 ± 11.5 | 0.54 | 0.71 |
| ESV index, mL/m2 | 26 ± 8.4 | 25.2 ± 8.7 | 24.9 ± 8.9 | 0.81 | 0.63 |
| Stroke volume, mL | 73.3 ± 8.1 | 71.5 ± 8.5 | 74.3 ± 10.7 | 0.36 | 0.74 |
| Cardiac output, L/min | 5.4 ± 0.9 | 5.2 ± 0.85 | 5.4 ± 1.05 | 0.29 | 0.9 |
| LVEF, % | 55.1 ± 6.3 | 58.3 ± 4.5 | 62.1 ± 4.1 | 0.17 | 0.041 |
| LVMI, g/m2 | 97.8 ± 26.1 | 94.9 ± 24.7 | 94.3 ± 27 | 0.43 | 0.71 |
| LAVI, mL/m2 | 24.3 ± 6.8 | 21.2 ± 5.9 | 20.6 ± 5.1 | 0.15 | 0.11 |
| E wave, m/s | 0.64 ± 0.13 | 0.53 ± 0.1 | 0.57 ± 0.16 | 0.08 | 0.46 |
| A wave, m/s | 0.66 ± 0.06 | 0.61 ± 0.13 | 0.55 ± 0.1 | 0.19 | 0.04 |
| E wave DT, m/s | 204 ± 50 | 199 ± 47 | 201 ± 58 | 0.58 | 0.62 |
| Averaged E′ cm/s | 7.5 ± 2.3 | 9.0 ± 2.1 | 9.7 ± 3.1 | 0.17 | 0.07 |
| E/E′ ratio | 12.1 ± 2.7 | 10.2 ± 2.4 | 8.3 ± 3.1 | 0.18 | 0.013 |
| S’, cm/s | 8.2 ± 1.8 | 9.4 ± 1.9 | 9.4 ± 2 | 0.11 | 0.24 |
| SPAP, mmHg | 25.2 ± 4.2 | 24.6 ± 4.4 | 23.7 ± 4.9 | 0.51 | 0.31 |
| FVC, L | 3.2 ± 1.4 | 3.4 ± 1.1 | 3.4 ± 1 | 0.39 | 0.75 |
| FVC, % predicted | 103 ± 16.0 | 92.1 ± 14.5 | 94.5 ± 17 | 0.09 | 0.32 |
| FEV1, L/s | 2.6 ± 0.9 | 3.1 ± 1.1 | 3.1 ± 1.1 | 0.12 | 0.15 |
| FEV1, % predicted | 79.1 ± 16.8 | 94 ± 15 | 96.2 ± 17.7 | 0.05 | 0.03 |
| FEV1/FVC | 77 ± 8.1 | 92.1 ± 6.1 | 92.2 ± 6.3 | 0.01 | 0.01 |
| VO2/kg/min | 3.6 ± 0.8 | 3.6 ± 0.8 | 3.6 ± 0.85 | 1 | 0.96 |
| RER | 0.78 ± 0.07 | 0.79 ± 0.07 | 0.78 ± 0.08 | 0.91 | 0.93 |
| AV difference, L/L | 0.06 ± 0.02 | 0.06 ± 0.02 | 0.06 ± 0.02 | 1 | 1 |
| Baseline | Unloaded | AT | Peak | p Value within Group | p Value PAD + CAD vs. CAD | p Value PAD + CAD vs. Normal | |
|---|---|---|---|---|---|---|---|
| EDV index, mL/m2 PAD + CAD CAD Normal | 68 ± 9.4 67.1 ± 10.6 67.5 ± 11.5 | 76 ± 9.5 80.2 ± 10 80.7 ± 11.7 | 76.1 ± 9.5 86.6 ± 9.8 88. ± 12 | 75.3 ± 9.8 86.2 ± 10.2 85.9 ± 11.6 | 0.036 <0.001 <0.001 | 0.015 | 0.029 |
| ESV index, mL/m2 PAD + CAD CAD Normal | 26.3 ± 8.4 25.2 ± 8.7 24.9 ± 8.9 | 26 ± 9 24.5 ± 8.1 21.3 ± 9.6 | 24.3 ± 8.6 24.2 ± 9.5 23 ± 9.2 | 23.8 ± 8.1 21.1 ± 8.8 20.5 ± 9.7 | 0.36 0.17 0.27 | 0.44 | 0.39 |
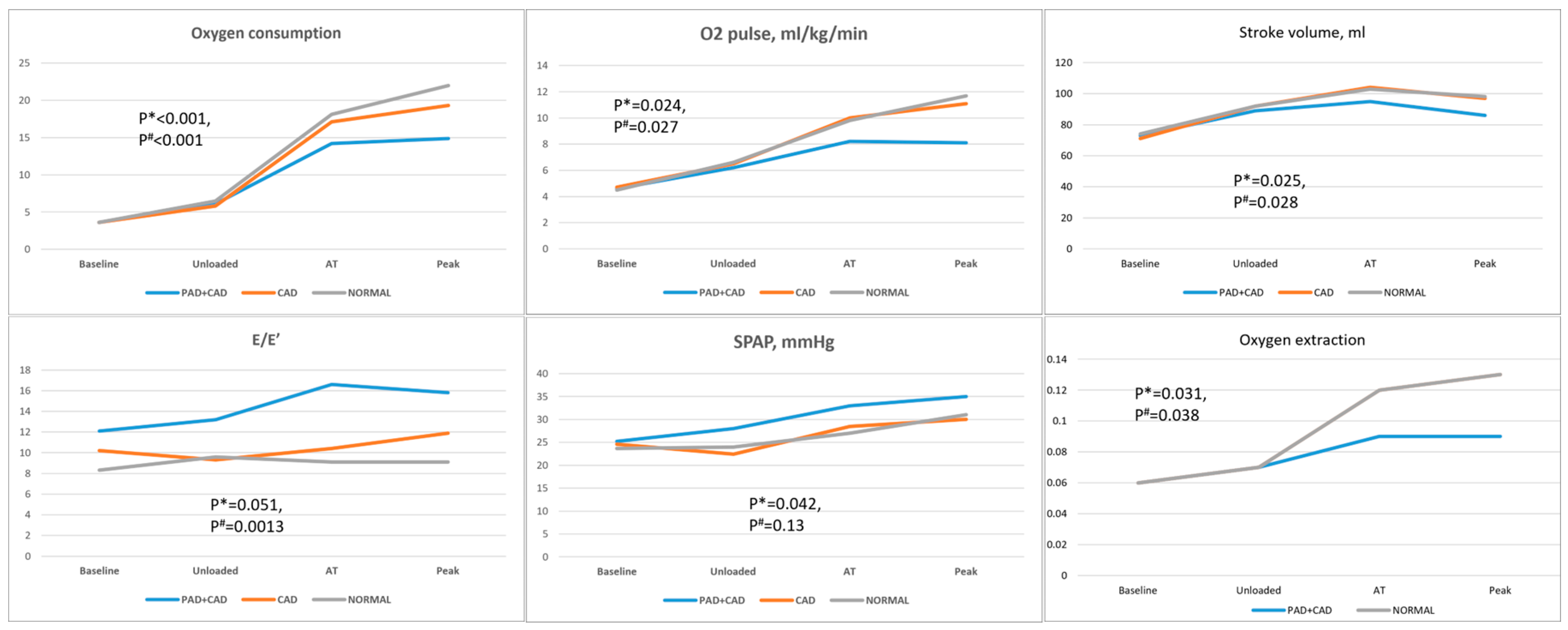
| Stroke volume, mL PAD + CAD CAD Normal | 73.3 ± 8.1 71.5 ± 8.5 74.3 ± 10.7 | 89 ± 11 92 ± 11 92 ± 13 | 95 ± 10 104 ± 9 103 ± 11 | 86 ± 10 97 ± 10 98 ± 11 | 0.0014 <0.001 <0.001 | 0.025 | 0.028 |
| HR, bpm PAD + CAD CAD Normal | 71.1 ± 4.3 72.5 ± 5 78.7 ± 7.2 | 82 ± 12.6 86.3 ± 13.2 88.1 ± 14 | 97.3 ± 14.1 99.6 ± 13.3 116.7 ± 15 | 107.7 ± 17.2 119.8 ± 14.4 138.5 ± 18.9 | <0.001 <0.001 <0.001 | 0.036 | <0.001 |
| CO, L/min PAD + CAD CAD Normal | 5.4 ± 0.9 5.2 ± 0.85 5.4 ± 1.05 | 7.4 ± 2 7.5 ± 2.1 7.8 ± 3 | 9.3 ± 2.7 10.3 ± 2.4 11.9 ± 2.8 | 10.5 ± 2.9 12.7 ± 2.2 13.2 ± 3 | <0.001 <0.001 <0.001 | 0.029 | 0.017 |
| E/E′ ratio PAD + CAD CAD Normal | 12.1 ± 2.7 10.2 ± 2.4 8.3 ± 3.1 | 13.2 ± 3.1 9.3 ± 2.4 9.6 ± 4 | 16.6 ± 4.3 10.4 ± 2.5 9.1 ± 3.8 | 15.8 ± 4 11.9 ± 2.9 9.1 ± 4.1 | 0.034 0.42 0.61 | 0.051 | 0.0013 |
| S′, cm/s PAD + CAD CAD Normal | 8.2 ± 1.8 9.4 ± 1.9 9.4 ± 2 | 8.1 ± 2 10.1 ± 2.1 9.7 ± 1.5 | 8.6 ± 1.6 9.6 ± 1.8 9.1 ± 1.8 | 8.8 ± 1.9 9.7 ± 2 9.6 ± 2.1 | 0.66 0.71 0.6 | 0.33 | 0.41 |
| SPAP, mmHg PAD + CAD CAD Normal | 25.2 ± 4.2 24.6 ± 4.4 23.7 ± 4.9 | 28.1 ± 4.9 24.2 ± 4.8 22.6 ± 5.2 | 32.9 ± 4.4 28.6 ± 3.8 27.1 ± 4.6 | 35 ± 5.1 30.2 ± 4 31.6 ± 6.3 | <0.001 0.11 0.018 | 0.042 | 0.13 |
| VO2, mL/kg/min PAD + CAD CAD Normal | 3.6 ± 0.8 3.6 ± 0.8 3.6 ± 0.85 | 6.1 ± 1.4 5.8 ± 1.9 6.5 ± 2.5 | 14.2 ± 1.8 17.1 ± 2.9 18.1 ± 3.3 | 14.9 ± 2 19.3 ± 2.5 22 ± 3.6 | <0.001 <0.001 <0.001 | <0.001 | <0.001 |
| O2 pulse, mL/kg/min PAD + CAD CAD Normal | 4.6 ± 1.3 4.7 ± 1.1 4.5 ± 1.3 | 6.2 ± 1.9 6.5 ± 2 6.6 ± 2.3 | 8.2 ± 1.8 10 ± 2.4 9.8 ± 2.3 | 8.1 ± 2.2 11.1 ± 2 11.7 ± 2.6 | <0.001 <0.001 <0.001 | 0.0024 | 0.0027 |
| AV difference, L/L PAD + CAD CAD Normal | 0.06 ± 0.02 0.06 ± 0.02 0.06 ± 0.02 | 0.06 ± 0.03 0.07 ± 0.03 0.07 ± 0.03 | 0.09 ± 0.0 0.12 ± 0.0 0.12 ± 0.03 | 0.09 ± 0.0 0.13 ± 0.0 0.13 ± 0.03 | 0.043 <0.001 <0.001 | 0.031 | 0.038 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghantous, E.; Shetrit, A.; Erez, Y.; Noam, N.; Zamanzadeh, R.S.; Zahler, D.; Granot, Y.; Levi, E.; Perl, M.L.; Banai, S.; et al. The Mechanism of Effort Intolerance in Patients with Peripheral Arterial Disease: A Combined Stress Echocardiography and Cardiopulmonary Exercise Test. J. Clin. Med. 2023, 12, 5817. https://doi.org/10.3390/jcm12185817
Ghantous E, Shetrit A, Erez Y, Noam N, Zamanzadeh RS, Zahler D, Granot Y, Levi E, Perl ML, Banai S, et al. The Mechanism of Effort Intolerance in Patients with Peripheral Arterial Disease: A Combined Stress Echocardiography and Cardiopulmonary Exercise Test. Journal of Clinical Medicine. 2023; 12(18):5817. https://doi.org/10.3390/jcm12185817
Chicago/Turabian StyleGhantous, Eihab, Aviel Shetrit, Yonatan Erez, Natalie Noam, Ryan S. Zamanzadeh, David Zahler, Yoav Granot, Erez Levi, Michal Laufer Perl, Shmuel Banai, and et al. 2023. "The Mechanism of Effort Intolerance in Patients with Peripheral Arterial Disease: A Combined Stress Echocardiography and Cardiopulmonary Exercise Test" Journal of Clinical Medicine 12, no. 18: 5817. https://doi.org/10.3390/jcm12185817
APA StyleGhantous, E., Shetrit, A., Erez, Y., Noam, N., Zamanzadeh, R. S., Zahler, D., Granot, Y., Levi, E., Perl, M. L., Banai, S., Topilsky, Y., & Havakuk, O. (2023). The Mechanism of Effort Intolerance in Patients with Peripheral Arterial Disease: A Combined Stress Echocardiography and Cardiopulmonary Exercise Test. Journal of Clinical Medicine, 12(18), 5817. https://doi.org/10.3390/jcm12185817