
Delirium Screening and Pharmacotherapy in the ICU: The Patients Are Not the Only Ones Confused

 ,
, 
Abstract
1. Introduction
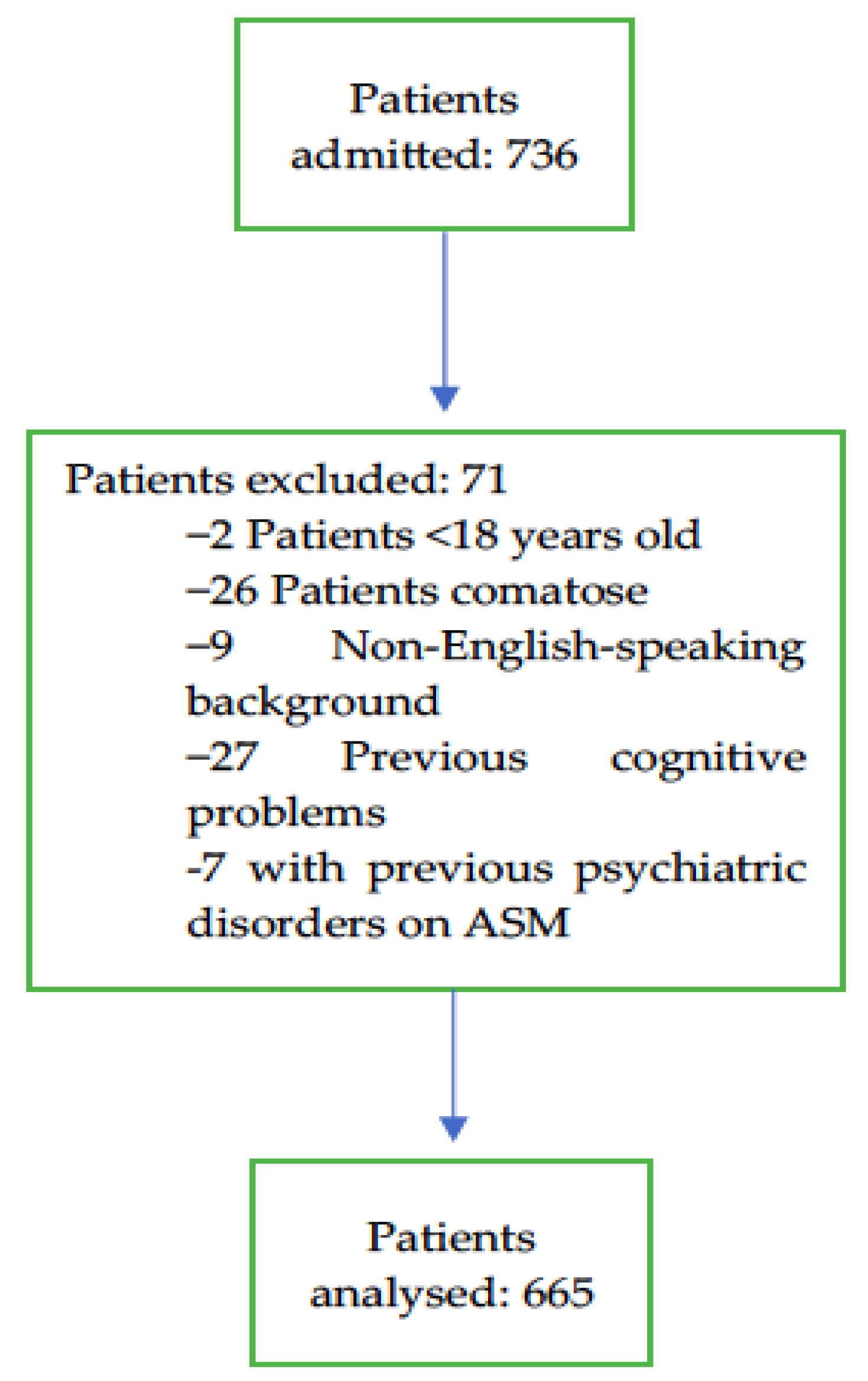
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2013; Available online: http://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596 (accessed on 25 June 2016).
- Fiest, K.M.; Soo, A.; Hee Lee, C.; Niven, D.J.; Ely, E.W.; Doig, C.J.; Stelfox, H.T. Long-Term Outcomes in ICU Patients with Delirium: A Population-based Cohort Study. Am. J. Respir. Crit. Care Med. 2021, 204, 412–420. [Google Scholar] [CrossRef] [PubMed]
- WHO|ICD-10 Online Versions. Available online: http://www.who.int/classifications/icd/icdonlineversions/en/ (accessed on 17 April 2020).
- Wolters, A.E.; van Dijk, D.; Pasma, W.; Cremer, O.L.; Looije, M.F.; de Lange, D.W.; Veldhuijzen, D.S.; Slooter, A.J. Long-term outcome of delirium during intensive care unit stay in survivors of critical illness: A prospective cohort study. Crit. Care 2014, 18, R125. [Google Scholar] [CrossRef] [PubMed]
- De, J.; Wand, A.P. Delirium Screening: A Systematic Review of Delirium Screening Tools in Hospitalized Patients. Gerontologist 2015, 55, 1079–1099. [Google Scholar] [CrossRef]
- Monitoring Delirium in the ICU. Available online: https://www.icudelirium.org/medical-professionals/delirium/monitoring-delirium-in-the-icu (accessed on 13 March 2023).
- Barman, A.; Pradhan, D.; Bhattacharyya, P.; Dey, S.; Bhattacharjee, A.; Tesia, S.S.; Mitra, J.K. Diagnostic accuracy of delirium assessment methods in critical care patients. J. Crit. Care 2018, 44, 82–86. [Google Scholar] [CrossRef]
- Riekerk, B.; Pen, E.J.; Hofhuis, J.G.M.; Rommes, J.H.; Schultz, M.J.; Spronk, P.E. Limitations and practicalities of CAM-ICU implementation, a delirium scoring system, in a Dutch intensive care unit. Intensive Crit. Care Nurs. 2009, 25, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Burry, L.; Hutton, B.; Williamson, D.R.; Mehta, S.; Adhikari, N.K.; Cheng, W.; Ely, E.W.; Egerod, I.; Fergusson, D.A.; Rose, L. Pharmacological interventions for the treatment of delirium in critically ill adults. Cochrane Database Syst. Rev. 2019, 2019, CD011749. [Google Scholar] [CrossRef] [PubMed]
- Girard, T.D.; Exline, M.C.; Carson, S.S.; Hough, C.L.; Rock, P.; Gong, M.N.; Douglas, I.S.; Malhotra, A.; Owens, R.L.; Feinstein, D.J.; et al. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness. N. Engl. J. Med. 2018, 379, 2506–2516. [Google Scholar] [CrossRef]
- Andersen-Ranberg, N.C.; Poulsen, L.M.; Perner, A.; Wetterslev, J.; Estrup, S.; Hästbacka, J.; Morgan, M.; Citerio, G.; Caballero, J.; Lange, T.; et al. Haloperidol for the Treatment of Delirium in ICU Patients. N. Engl. J. Med. 2022, 387, 2425–2435. [Google Scholar] [CrossRef]
- American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults. American Geriatrics Society abstracted clinical practice guideline for postoperative delirium in older adults. J. Am. Geriatr. Soc. 2015, 63, 142–150. [Google Scholar] [CrossRef]
- Markowitz, J.D.; Narasimhan, M. Delirium and Antipsychotics: A Systematic Review of Epidemiology and Somatic Treatment Options. Psychiatry 2008, 5, 29–36. [Google Scholar]
- Haloperidol—Australian Medicines Handbook. Available online: https://amhonline.amh.net.au.acs.hcn.com.au/chapters/psychotropic-drugs/antipsychotics/haloperidol?menu=hints (accessed on 27 June 2023).
- ANZICS. CORE Reports. Available online: https://www.anzics.com.au/annual-reports/ (accessed on 14 March 2023).
- Wang, C.; Qin, Y.; Wan, X.; Song, L.; Li, Z.; Li, H. Incidence and risk factors of postoperative delirium in the elderly patients with hip fracture. J. Orthop. Surg. 2018, 13, 186. [Google Scholar] [CrossRef] [PubMed]
- van den Boogaard, M.; Schoonhoven, L.; van der Hoeven, J.G.; van Achterberg, T.; Pickkers, P. Incidence and short-term consequences of delirium in critically ill patients: A prospective observational cohort study. Int. J. Nurs. Stud. 2012, 49, 775–783. [Google Scholar] [CrossRef]
- Williams, E.C.; Estime, S.; Kuza, C.M. Delirium in trauma ICUs: A review of incidence, risk factors, outcomes, and management. Curr. Opin. Anesthesiol. 2023, 36, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Vasilevskis, E.E.; Han, J.H.; Hughes, C.G.; Ely, E.W. Epidemiology and risk factors for delirium across hospital settings. Best Pract. Res. Clin. Anaesthesiol. 2012, 26, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Watt, C.L.; Momoli, F.; Ansari, M.T.; Sikora, L.; Bush, S.H.; Hosie, A.; Kabir, M.; Rosenberg, E.; Kanji, S.; Lawlor, P.G. The incidence and prevalence of delirium across palliative care settings: A systematic review. Palliat. Med. 2019, 33, 865–877. [Google Scholar] [CrossRef]
- Martinez, F.E.; Ho, V.W.; Brogan, G.; Pickering, C.; Leung, G.; Parrey, J.; Charlton, A. Period-Prevalence and Risk Factors for Delirium in a Tertiary Referral ICU: A prospective cohort study. Acute Med. 2021, 20, 168–173. [Google Scholar] [CrossRef]
- Taran, Z.; Namadian, M.; Faghihzadeh, S.; Naghibi, T. The Effect of Sedation Protocol Using Richmond Agitation-Sedation Scale (RASS) on Some Clinical Outcomes of Mechanically Ventilated Patients in Intensive Care Units: A Randomized Clinical Trial. J. Caring Sci. 2019, 8, 199–206. [Google Scholar] [CrossRef]
- DeGrado, J.R.; Anger, K.E.; Szumita, P.M.; Pierce, C.D.; Massaro, A.F. Evaluation of a local ICU sedation guideline on goal-directed administration of sedatives and analgesics. J. Pain Res. 2011, 4, 127–134. [Google Scholar] [CrossRef][Green Version]
- Pandharipande, P.; Shintani, A.; Peterson, J.; Pun, B.T.; Wilkinson, G.R.; Dittus, R.S.; Bernard, G.R.; Ely, E.W. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 2006, 104, 21–26. [Google Scholar] [CrossRef]
- Shehabi, Y.; Howe, B.D.; Bellomo, R.; Arabi, Y.M.; Bailey, M.; Bass, F.E.; Bin Kadiman, S.; McArthur, C.J.; Murray, L.; Reade, M.C.; et al. Early Sedation with Dexmedetomidine in Critically Ill Patients. N. Engl. J. Med. 2019, 380, 2506–2517. [Google Scholar] [CrossRef]
- Riker, R.R.; Shehabi, Y.; Bokesch, P.M.; Ceraso, D.; Wisemandle, W.; Koura, F.; Whitten, P.; Margolis, B.D.; Byrne, D.W.; Ely, E.W.; et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: A randomized trial. JAMA 2009, 301, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.P.; Pun, B.T.; Herr, D.L.; Maze, M.; Girard, T.D.; Miller, R.R.; Shintani, A.K.; Thompson, J.L.; Jackson, J.C.; Deppen, S.A.; et al. Effect of Sedation With Dexmedetomidine vs Lorazepam on Acute Brain Dysfunction in Mechanically Ventilated Patients: The MENDS Randomized Controlled Trial. JAMA 2007, 298, 2644–2653. [Google Scholar] [CrossRef] [PubMed]
- Zaal, I.J.; Devlin, J.W.; Peelen, L.M.; Slooter, A.J.C. A Systematic Review of Risk Factors for Delirium in the ICU. Crit. Care Med. 2015, 43, 40–47. [Google Scholar] [CrossRef]
- Park, Y.; Bateman, B.T.; Kim, D.H.; Hernandez-Diaz, S.; Patorno, E.; Glynn, R.J.; Mogun, H.; Huybrechts, K.F. Use of haloperidol versus atypical antipsychotics and risk of in-hospital death in patients with acute myocardial infarction: Cohort study. BMJ 2018, 360, k1218. [Google Scholar] [CrossRef] [PubMed]
- Huhn, M.; Nikolakopoulou, A.; Schneider-Thoma, J.; Krause, M.; Samara, M.; Peter, N.; Arndt, T.; Bäckers, L.; Rothe, P.; Cipriani, A.; et al. Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: A systematic review and network meta-analysis. Lancet 2019, 394, 939–951. [Google Scholar] [CrossRef]
- McGinn, K.; Davis, S.N.; Terrry, E.; Simmons, J.; Brevard, S. Elimination of Routine Benzodiazepine Administration for Nonprocedural Sedation in a Trauma Intensive Care Unit is Feasible. Am. Surg. 2018, 84, 947–951. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | N = 665 |
|---|---|
| Age | |
| Median (IQR) | 64 (53–74) |
| Mean (SD) | 61 (17) |
| Sex (male) | 62.6% (417/665) |
| APACHE-III scores | |
| Median (IQR) | 55 (40–75.5) |
| Mean (SD) | 59 (26) |
| Admission type | |
| Medical | 48.6% (323/665) |
| Surgical | 51.4% (342/665) |
| ICU LOS (days) | |
| Median (IQR) | 1.9 (1–3.6) |
| Mean (SD) | 3.2 (5) |
| ICU LOS (hours) | |
| Median (IQR) | 46 (24–86) |
| Mean (SD) | 76.2 (120) |
| Received IMV at one point during ICU admission | |
| Yes | 55.9% (372/665) |
| No | 44.2% (293/665) |
| Sedative, any | 57.1% (380/665) |
| Benzodiazepine | 43% (286/665) |
| Alpha-2 agonist | 16.7% (111/665) |
| Opioid | 74% (492/665) |
| ICU mortality | 10.5% (70/665) |
| Primary Outcome | |
| Incidence, or rate, of patients who were found to have delirium at least once during their admission. | 11.3% (75/665) |
| Secondary Outcomes of screening | |
| Total RASSs performed | 17,273 |
| Number of RASSs performed per patient per day (average number of RASSs/average ICU LOS) | 8.2 |
| Number of RASSs completed per patient during their ICU stays | |
| Median (IQR) | 12 (5–27) |
| Mean (SD) | 26 (52) |
| Time between RASS score evaluation (Average number of RASSs/24 h) | 2.9 h |
| Number of patients who were not assessed with RASS at any time during their ICU stays | 8.4% (56/665) |
| RASS score value | |
| Median (IQR) | −0.2 (−1.2 to 0.0) |
| Mean (SD) | −0.55 (1.5) |
| Number of patients with a mean RASS score < −3 (cannot be assessed with CAM-ICU) | 6.2% (41/665) |
| Total CAM-ICUs performed | 1248 |
| Number of CAM-ICUs performed per patient per day (Average number of CAM-ICUs/average ICU LOS) | 0.6 |
| Number of CAM-ICUs completed per patient during their ICU stays | |
| Median (IQR) | 1 (0–2) |
| Mean (SD) | 1.9 (3.1) |
| Time between CAM-ICU evaluation (Average number of CAM-ICUs/24 h) | 40 h |
| Number of patients who were | |
| assessed with CAM-ICU at least once while in the ICU | 59.4%(395/665) |
| not assessed with CAM-ICU at any time while in the ICU | 40.6% (270/665) |
| Rate of delirium based on assessments (Positive CAM-ICU results/Total CAM-ICU results) | 14.8% (185/1248) |
| Rate of patients who had at least one positive CAM-ICU result out of those who were assessed with CAM-ICU | 19% (75/395) |
| n = 665 | |
|---|---|
| APM prescribed | 17% (113/665) |
| Patients who received APMs | |
| After being screened for delirium | 63.7% (72/113) |
| After not being screened for delirium | 36.3% (41/113) |
| Patients who were screened for delirium who received APMs | |
| with a positive CAM-ICU result | 57.3% (43/75) |
| with a negative CAM-ICU result | 9.1% (29/320) |
| Patients that received | |
| one agent | 12.6% (84/665) |
| two agents | 3.5% (23/665) |
| three agents | 0.9% (6/665) |
| Most used APM | |
| Quetiapine | 6% (40/665) |
| Haloperidol | 4.5% (30/665) |
| Olanzepine | 3.3% (22/665) |
| Droperidol | 2.6% (17/665) |
| Risperidone | 0.5% (3/665) |
| Other | 0.2% (1/665) |
| Patients who received non-APM treatment with a benzodiazepine | |
| with a positive CAM-ICU result | 68% (51/75) |
| with a negative CAM-ICU result | 35% (114/320) |
| Patients who received non-APM treatment with an alpha-2 agonist | |
| with a positive CAM-ICU result | 45.3% (34/75) |
| with a negative CAM-ICU result | 13.4% (43/320) |
| Variable | Odds Ratio | 95% CI (Profile Likelihood) |
|---|---|---|
| Intercept (Delirium) | 0.012 | 0.002217 to 0.05621 |
| Gender | 1.119 | 0.5980 to 2.132 |
| Age | 1.003 | 0.9832 to 1.024 |
| ICU LOS in hours | 1.006 | 1.003 to 1.009 |
| Admission type (surgical, medical) | 0.8267 | 0.4034 to 1.683 |
| APACHE-III score | 1.027 | 1.013 to 1.041 |
| Intubated | 0.9344 | 0.4105 to 2.157 |
| New sedative prescribed | 1.385 | 0.4597 to 4.087 |
| New benzo prescribed | 2.007 | 0.8929 to 4.778 |
| Alpha-2 agonist prescribed | 2.760 | 1.302 to 5.919 |
| New opioid prescribed | 0.6006 | 0.2525 to 1.418 |
| Variable | Odds Ratio | 95% CI (Profile Likelihood) |
|---|---|---|
| Intercept (APM use) | 0.08668 | 0.02639 to 0.2658 |
| Gender | 1.055 | 0.6059 to 1.865 |
| Age | 0.9856 | 0.9696 to 1.002 |
| ICU LOS in hours | 1.003 | 1.001 to 1.006 |
| Admission type (surgical, medical) | 1.503 | 0.8428 to 2.712 |
| APACHE-III score | 1.002 | 0.9906 to 1.014 |
| Intubated | 0.6482 | 0.3438 to 1.196 |
| Alpha-2 agonist (clonidine/dexmed) prescribed | 7.615 | 4.182 to 14.04 |
| Delirium | 3.537 | 1.747 to 7.066 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez, F.E.; Tee, R.; Poulter, A.-L.; Jordan, L.; Bell, L.; Balogh, Z.J. Delirium Screening and Pharmacotherapy in the ICU: The Patients Are Not the Only Ones Confused. J. Clin. Med. 2023, 12, 5671. https://doi.org/10.3390/jcm12175671
Martinez FE, Tee R, Poulter A-L, Jordan L, Bell L, Balogh ZJ. Delirium Screening and Pharmacotherapy in the ICU: The Patients Are Not the Only Ones Confused. Journal of Clinical Medicine. 2023; 12(17):5671. https://doi.org/10.3390/jcm12175671
Chicago/Turabian StyleMartinez, F. Eduardo, Rebecca Tee, Amber-Louise Poulter, Leah Jordan, Liam Bell, and Zsolt J. Balogh. 2023. "Delirium Screening and Pharmacotherapy in the ICU: The Patients Are Not the Only Ones Confused" Journal of Clinical Medicine 12, no. 17: 5671. https://doi.org/10.3390/jcm12175671
APA StyleMartinez, F. E., Tee, R., Poulter, A.-L., Jordan, L., Bell, L., & Balogh, Z. J. (2023). Delirium Screening and Pharmacotherapy in the ICU: The Patients Are Not the Only Ones Confused. Journal of Clinical Medicine, 12(17), 5671. https://doi.org/10.3390/jcm12175671